Abstract
Background: Research has shown that Adverse Childhood Experiences (ACEs) are prevalent and are associated with psychological distress. Some studies indicate facing these adversities can lead to post-traumatic growth. This study aims to assess the impact of ACEs on psychological distress and post-traumatic growth and to determine the mediating effect of post-traumatic growth between ACEs and psychological distress, in a sample of adults. Methods: In this study, there were 521 participants (mean = 31.32, SD = 12.28), who answered the following surveys online: a sociodemographic questionnaire, the Family ACE Questionnaire, the Kessler Psychological Distress Scale (K10) and the Post-Traumatic Growth Inventory (PTGI). Results: ACEs were positive and significant predictors of psychological distress, and the “Change in the perception of the self and life in general” factor of post-traumatic growth was the strongest predictor of lower perceived psychological distress. Post-traumatic growth did not mediate the relationship between ACEs and psychological distress. Conclusions: These findings contribute to the improvement of clinical practice and health policies and highlight the need for a more in-depth understanding of the impact of ACEs on mental health.
1. Introduction
Adverse Childhood Experiences (ACEs) are stressful events of a traumatic nature that occur in the first 18 years of an individual’s life, which contribute to the absence of secure and stable family relationships (APA 2023), as well to the negative impact on the physical and mental health of the individuals who experience them (Felitti et al. 1998). These experiences and their repercussions on adult health were described for the first time in a study by Felitti and collaborators (1998) and are considered risk factors for morbidity and mortality (Jones et al. 2020; Ramiro et al. 2010). ACEs include types of abuse (emotional, physical, and sexual), exposure to domestic violence, substance abuse in the family environment, divorce or parental separation, imprisonment of a family member and mental illness or suicide, and neglect (emotional and physical) (Silva and Maia 2008).
ACEs are some of the most common and profound sources of stress in early life (Boullier and Blair 2018; WHO 2020) and can lead to the disruption of the child’s physical and psychological health (Kalmakis and Chandler 2014). However, they may not only negatively affect health and well-being at the time they occur, but also later in life (Soares et al. 2016), which will be discussed later.
Many studies show that more than half of individuals have experienced at least one ACE (Esaki and Larkin 2013; Felitti et al. 1998; Hales et al. 2023; Manyema et al. 2018; Merrick et al. 2017; Nevárez-Mendoza and Ochoa-Meza 2022; Soares et al. 2022). The most common types of ACEs are emotional abuse (67–82.9%) (Amaranggani and Dewi 2022; Goodman et al. 2022), emotional neglect (60–82.2%) (AlHemyari et al. 2022; Craig et al. 2023), parental separation or divorce (42–77.6%) (Martin et al. 2022; Soares et al. 2016), and substance abuse in the household (25.6–31.6%) (Felitti et al. 1998, Nevárez-Mendoza and Ochoa-Meza 2022). The least common are sexual abuse (1.4–4%) (Manyema et al. 2018; Soares et al. 2016), the incarceration of a family member (3.4–5%) (Babad et al. 2022; Craig et al. 2023) and physical neglect (4.1–4.6) (Nevárez-Mendoza and Ochoa-Meza 2022; Soares et al. 2016).
1.1. Sociodemographic Disparities in ACEs
A considerable body of research has studied differences in ACEs by demographic variables. Regarding gender, some studies found that women experience more ACEs (AlHemyari et al. 2022; Campbell et al. 2016; Giano et al. 2020; Soares et al. 2016; Wong et al. 2019), while others indicate that the prevalence of ACEs is higher in men (Almuneef et al. 2017; Giovanelli et al. 2016; Hales et al. 2023). However, there seems to be a consensus on the higher prevalence of sexual abuse (Martin et al. 2022; Sánchez-Jáuregui et al. 2023; Soares et al. 2016), emotional neglect (AlHemyari et al. 2022; Martin et al. 2022; Soares et al. 2016; Yuan et al. 2021) and exposure to domestic violence (AlHemyari et al. 2022; Soares et al. 2016) in women. As for men, they seem to experience more physical abuse (Almuneef et al. 2017; Yuan et al. 2021) and exposure to substance abuse (Almuneef et al. 2017; Nevárez-Mendoza and Ochoa-Meza 2022).
Regarding age, younger individuals present a greater number of ACEs compared to older people (Campbell et al. 2016; Felitti et al. 1998; Nevárez-Mendoza and Ochoa-Meza 2022; Riedl et al. 2020) who exhibit better mental health (Nurius et al. 2015). However, although younger people report more experiences of emotional abuse, older people have greater experiences of physical neglect (Novais et al. 2021; Riedl et al. 2020). Freed et al. (2018) found that most adult individuals perceive a deterioration in the well-being of children today compared to when they were children. In addition, the findings of a study by Hughes et al. (2017) indicate that Millennials, Generation Z, and Generation X are more likely to experience a high number of ACEs compared to Baby Boomers, suggesting greater health risks associated with ACEs for younger generations.
When it comes to ethnic and racial minorities (non-Caucasian individuals), they display a higher number of ACEs (Giano et al. 2020; Hales et al. 2023), as do sexual minorities (non-heterosexual people) (Giano et al. 2020), people with lower incomes (Campbell et al. 2016; Giano et al. 2020) and those who have lower levels of education (Campbell et al. 2016; Giano et al. 2020; Wong et al. 2019).
1.2. The Long-Term Impact of ACEs
ACEs can be a contributing factor to the occurrence of risk behaviors, such as exposure to risky sexual behaviors—early sex life (Novais et al. 2021), multiple sexual partners, sexually transmitted diseases (Felitti et al. 1998; Novais et al. 2021) and unwanted pregnancy (Ramiro et al. 2010)-, smoking (Felitti et al. 1998; Hughes et al. 2017; Novais et al. 2021; Ramiro et al. 2010), alcohol use (Felitti et al. 1998; Hughes et al. 2017; Merrick et al. 2017; Ramiro et al. 2010), drug use (Felitti et al. 1998; Merrick et al. 2017), self-harm behaviors (Novais et al. 2021) and suicide attempts (Felitti et al. 1998; Lu et al. 2008; Merrick et al. 2017; Silveira and Pereira 2023; Thompson et al. 2019).
As for physical health, ACEs are known to contribute to high blood pressure (AlHemyari et al. 2022), obesity (AlHemyari et al. 2022; Felitti et al. 1998; Nevárez-Mendoza and Ochoa-Meza 2022), diabetes (Campbell et al. 2016; Monnat and Chandler 2015; Novais et al. 2021), heart problems (Felitti et al. 1998; Monnat and Chandler 2015; Ramiro et al. 2010), and chronic diseases (Boullier and Blair 2018; Jones et al. 2020).
There is also an association between ACEs and psychosocial problems, such as difficulties in controlling anger (Anda et al. 2006), sleep disturbance (Anda et al. 2006), loneliness (Agbaje et al. 2021; Babad et al. 2022; Wong et al. 2019), panic attacks (Anda et al. 2006), PTSD (Brockie et al. 2015; Lu et al. 2008) and suicidal thoughts or suicidal ideation (Thompson et al. 2019; Thai et al. 2020; Wong et al. 2019).
1.3. The Relationship between ACEs and Psychological Distress
Recent studies have also found an association between ACEs and psychological distress (PD) (Agbaje et al. 2021; Jones et al. 2022; Manyema et al. 2018; Thai et al. 2020). Psychological distress is the result of physical and psychological symptoms experienced by the individual (Varela et al. 2017) that are based on emotional suffering such as depression (Agbaje et al. 2021; Belay et al. 2021, Serviço Nacional de Saúde 2018; Varela et al. 2017), anxiety (Agbaje et al. 2021; Belay et al. 2021; Serviço Nacional de Saúde 2018; Varela et al. 2017), stress (Agbaje et al. 2021), and somatic symptoms (Serviço Nacional de Saúde 2018). Research suggests that ACEs are related to depression and anxiety (Watt et al. 2019; Qu et al. 2022; Riedl et al. 2020; Silveira and Pereira 2023). However, a study by Elmore and Crouch (2020) found that ACEs have a greater impact on depression, with emotional abuse (Chapman et al. 2004; Qu et al. 2022; Silveira and Pereira 2023; Qu et al. 2022) and a family history of mental illness (Giano et al. 2021; Pinto et al. 2015) being significant risk factors when it comes to the occurrence of this mood disorder. At the same time, PD is linked to sadness and low self-esteem (Agbaje et al. 2021; Varela et al. 2017), aggression (Agbaje et al. 2021), unhappiness, loss of interest and excessive tiredness (Belay et al. 2021), hopelessness (Belay et al. 2021; Varela et al. 2017), and tension and agitation (Belay et al. 2021; Varela et al. 2017).
1.4. Post-Traumatic Growth
Despite the negative implications of stressful or traumatic life events, they can be a catalyst for posttraumatic growth (PTG), which is the positive psychological change experienced by people after being confronted with a traumatic event, adversity, or complicated life circumstances (Calhoun and Tedeschi 1999, p. 11; Jayawickreme et al. 2020; Tedeschi and Calhoun 1996; Tedeschi and Calhoun 2004). PTG may occur simultaneously with PD, which is the product of attempts to adapt to adverse events (Tedeschi and Calhoun 2004). PTG is not about ending suffering (Kaye-Tzadok and Icekton 2022), nor about accepting the traumatic event itself, but rather about accepting the processes by which people assimilate and accommodate the contrast generated by the ACEs by re-establishing the perceptions that individuals have about themselves, and perceptions of the outside world, which results in a positive change (Quan et al. 2022). PTG has been reported by people who have lived through adverse experiences such as illness (Devine et al. 2010), childhood maltreatment (Mohr and Rosén 2017), breast cancer (Campos et al. 2021), natural disasters (Jin et al. 2014), and bereavement (Stein et al. 2018). The psychological changes reported by individuals are based on three domains: greater openness to new possibilities and greater involvement in interpersonal relationships, change in perception of self and life in general, and spiritual change (Resende et al. 2008).
1.5. Portuguese Context
According to a report from the Portuguese Association for Victim Support (2023), in Portugal, the profile of the victim in children and young people is predominantly female (60%), with an average age of ten (14.1%), and commonly is the child of the perpetrator (31.6%), with 2595 victims in 2022. The second most reported crime in that year was sexual crimes against children and young people (4.9%). According to the annual report of the National Commission for the Promotion of the Rights and Protection of Children and Young People (2023), the most frequent occurrence in 2022 was neglect (30.5%). There was also sexual abuse and emotional abuse, with a higher prevalence in females (76%). Emotional abuse and physical abuse were found mainly in children and young people between the ages of 11 (33.5%) and 14 (31.6%).
Some Portuguese studies have explored the prevalence of ACEs, such as Soares et al. (2022), who conducted a study in a Portuguese sample in which 96.2% of the children had at least one ACE domain. Also, a study from Silva and Maia (2010) based on an adult sample showed that 88% of the participants claimed to have experienced at least one ACE category. Furthermore, research from Pinto et al. (2015) revealed that almost 96,0% of women reported being exposed to at least one ACE domain during childhood and adolescence with physical abuse (46.2%) and emotional abuse (33.8%) being the most prevalent. Lastly, a study conducted by Alves et al. (2022) with inmate women showed that 83.5% reported having experienced some type of ACE, particularly physical abuse (42%) and sexual abuse (42%).
Previous investigations have revealed the negative long-term impact of these experiences on the mental health of individuals, such as Maia et al. (2006), who found an association between adverse experiences and present-day symptomatology. Moreover, Silva and Maia (2010) showed that adversity in childhood was linked with an increased risk for suicide attempts, and Pinto et al. (2015) showed a relationship between ACE exposure, depressive symptoms, and suicide attempts. In addition, Novais et al. (2021) showed higher scores of anxiety for individuals who experienced ACEs However, there is no substantial theoretical evidence to support the mediating effect of post-traumatic growth on the relationship between ACEs and psychological distress in a sample of adults. Therefore, this study aims to assess the impact of ACEs on psychological distress and PTG to determine the mediating effect of PTG between ACEs and psychological distress, as well as to explore the mutual influence of these variables, based on an adult sample. This will lead to a richer and deeper understanding of a scarce and developing area of study.
2. Materials and Methods
2.1. Participants
This study’s sample consisted of 521 participants aged between 18 and 80 (Mean = 31.32; SD = 12.28), of whom 345 (66.2%) identified themselves as women, 166 (31.9%) as men, and 10 (1.9%) as other. Most participants are European/white (94%), have Portuguese nationality (95%), live in Portugal (96.1%), live in a small town (44.5%), are employees (47.2%), have an average socio-economic status (53.9%), and are heterosexual (84.4%). Table 1 shows the sociodemographic characteristics of the sample in greater detail.

Table 1.
Sociodemographic characteristics (n = 521, Mage = 31.32, SDage = 12.28).
2.2. Instruments
The questionnaires were selected to gather information according to the variables and goals of the present study. A Sociodemographic Questionnaire, the Portuguese-language version of the Family Adverse Childhood Experiences Questionnaire, was used to assess the report of ACEs, the Kessler Psychological Distress Scale (K10) was used to assess anxiety and depressive symptoms, and the Post-Traumatic Growth Inventory (PTGI) was used to assess the perception of positive psychological changes after facing adversity.
The Sociodemographic Questionnaire was used to collect data on age, gender, nationality, sexual orientation, marital status, living situation, place of residence, socioeconomic statuse, education, professional status, and ethnic/racial group.
The Portuguese-language version of the Family Adverse Childhood Experiences Questionnaire (Silva and Maia 2008) was used to assess the report of ACEs and consists of the following domains: emotional abuse, physical abuse, sexual abuse, exposure to domestic violence, substance abuse in the family environment, divorce or parental separation, imprisonment of a family member, mental illness or suicide, physical neglect, and emotional neglect. These domains are assessed through 10 items, adapted from the original 77 items (Felitti et al. 1998), and the participant’s responses were evaluated on a Likert scale from 1 (Never) to 5 (Many Times). In the present study, Cronbach’s alpha was 0.81, showing a good internal consistency.
The Kessler Psychological Distress Scale (K10) (Pereira et al. 2019) was used to assess levels of psychological distress, keeping the original items (Kessler et al. 2003). It is based on questions related to depressive symptomatology (items 1, 4, 7, 8, 9, and 10) and anxious symptomatology (items 2, 3, 5, and 6) over the last month. The participants’ answers were given on a Likert scale from 1 (Never) to 5 (Always). The Cronbach’s alpha for the instrument Portuguese population was 0.91. For this study, Cronbach’s alpha was calculated for the total scale and the two sub-scales, obtaining results of 0.94, 0.93, and 0.89 for the total scale, depression, and anxiety, respectively. Thus, the instrument showed good internal consistency.
The Post-traumatic Growth Inventory for the Portuguese Population (Resende et al. 2008), adapted from the original version of the Post-traumatic Growth Inventory (PTGI) by Tedeschi and Calhoun (1996), was used to assess the positive psychological changes reported by individuals who had experienced adverse life events. PTG is assessed based on three factors: (1) Greater openness to new possibilities and greater involvement in interpersonal relationships (items 3, 6, 7, 8, 9, 11, 15, 16, 17, 20, and 21), (2) Change in perception of self and life in general (items 1, 2, 4, 10, 12, 13 and 19), and (3) Spiritual change (items 5 and 18). These factors were assessed using the 21 original items, and the respondent’s answers were given on a Likert scale from 1 (Nothing) to 5 (A lot) considering that the participants’ opinion corresponds to the degree to which they consider themselves to have changed because of a particular trauma. The Post-traumatic Growth Inventory for the Portuguese Population (Resende et al. 2008) showed an alpha of 0.95 for the total scale, an alpha of 0.94 for the greater openness to new possibilities and greater involvement in interpersonal relationships factor, an alpha of 0.84 for the change in perception of self and life in general factor, and finally, an alpha of 0.64 for the spiritual change factor. In this study, the Cronbach’s alpha values for the total scale were 0.96, for the the factor “greater openness to new possibilities and greater involvement in interpersonal relationships” was 0.93, for the factor “change in perception of self and life in general” was 0.91, and for the factor “spiritual change” was 0.48. The instrument showed good internal consistency.
2.3. Procedures
The present study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the University of Beira Interior, Portugal, for studies involving humans (CE-UBI-Pj-2021-047), ensuring all subjects gave their informed consent for inclusion before they participated in the study. This study ensures the principles of informed consent, guaranteeing the confidentiality and anonymity of the data, beneficence, and respect for the integrity of the participants, who were informed about the purpose of the study and the voluntary nature of their participation in the research.
For the investigation, a website was designed to disseminate the online survey on the Microsoft Forms platform via social networks and mailing lists from September to November 2023. Following data collection, a database was built in IBM SPSS Statistics (version 29, Armonk, NY, USA), in which the information was encrypted so that access to the participant’s identification was impossible.
To establish associations between ACEs and PTG, all participants who did not report ACEs but experienced PTG were eliminated, going from 749 respondents to 521 as the final sample.
2.4. Data Analysis
The gathered data were submitted to several statistical analyses according to the goals established for this investigation. Descriptive statistics (mean, standard deviation, percentages, and frequencies) were conducted to describe the prevalence and levels of Total ACEs and domains, levels of PD and subscales of anxiety and depression, as well as Total PTG and its factors, (1) greater openness to new possibilities and greater involvement in interpersonal relationships, (2) change in perception of self and life in general, and (3) spiritual change, in the general sample. Also, three-sample student t-tests were used to compare differences in means of Total ACES and domains, Total PD, anxiety, depression, and Total PTG and its factors, by gender, age group, and sexual orientation. To assess the strength and direction of possible associations between age, Total ACEs, the ten domains of childhood adversity, Total DP and its subscales—anxiety, depression, Total PTG and its factors, Pearson’s correlations were calculated. Additionally, one multiple linear hierarchical regression was performed to assess the predictive power of Total ACEs, ACE domains, sociodemographic variables, and Total PTG and its factors on Total PD. Finally, computer software by Hayes (2012 v4.2 was used to assess whether the relationship between Total ACEs and Total PD is mediated by the Total PTG. For all analyses, a p-value of <0.05 was considered statistically significant. Since this was a cross-sectional, descriptive, inferential, correlational, predictive, and mediational study and not an experimental or quasi-experimental one, we did not apply any treatment, and no control group was needed.
3. Results
Table 2 shows the prevalence of Total ACEs and domains in the overall sample. In this sample, 100% of participants reported at least one ACE. Emotional abuse was the most reported domain (59.7%), followed by emotional neglect (52.1%) and mental illness or suicide of a family member (51.4%). Other categories of ACEs and their respective prevalence can be found in more detail in Table 2.
Table 2.
ACEs prevalence.
Table 3 shows the descriptive statistics for Total ACEs and ACE domains as well as Total PTG and its factors—Factor 1 and seven items for Factor 2—on top of PD and its respective subscales—anxiety and depression. In the general sample, the mean of Total ACEs is 1.66 (SD = 0.61) with a sum of 16.56, the mean of Total PTG is 3.18 (SD = 0.86) with a sum of 66.34, and the mean of Total PD is 2.51 (SD = 0.83) with a sum of 25.05. All descriptive statistics can be found in more detail in Table 3.
Table 3.
Levels of ACEs, PTG, and PD.
Table 4 describes the average levels of the 10 items assessing ACEs, including Total ACEs and its domains, the 10 items assessing PD including Total PD and its subscales—4 items for anxiety and 6 items for depression—and the 21 items assessing PTG including Total PTG and its factors—11 items for Factor 1, 7 items for Factor 2, and 2 items for Factor 3, by age group.
Table 4.
Prevalence of ACEs, PTG, and PD by gender.
Statistically significant differences were found in Total ACEs (t (511) = 3.321; p < 0.001), with women scoring higher when compared to men (M = 1.71, SD = 0.62). Concerning Total PD, we also found statistically significant differences (t(511) = 5.356; p < 0.001), with women also reporting greater scores (M = 2.62, SD = 0.83). No statistically significant differences were found in Total PTG (t(511) = 1.831; p = 0.068). The results can be found in more detail in Table 4.
Table 5 describes the average levels of the 10 items assessing ACEs, including Total ACEs and its domains, the 10 items assessing PD including Total PD and its subscales—4 items for anxiety and 6 items for depression—and the 21 items assessing PTG including Total PTG and its factors—11 items for Factor 1, 7 items for Factor 2, and 2 items for Factor 3 by age group.
Table 5.
Prevalence of ACEs, PTG and PD, by age group.
The results indicate that concerning Total PD, there are statistically significant differences (t(501) = 4.284; p =< 0.001), with younger people showing higher levels (M = 2.65, SD = 0.82). As far as Total PTG, there are statistically significant differences (t(501) = −4.390; p =< 0.001), with older people showing higher levels (M = 3.36, SD = 0.84). As far as Total PTG, there are statistically significant differences (t(501) = −4.390; p =< 0.001), with older people showing higher levels (M = 3.36, SD = 0.84). No statistically significant differences were found in Total ACEs (t(501) = 626; p = 0.532). The results can be found in more detail in Table 5.
Table 6 describes the average levels of the 10 items assessing ACEs, including Total ACEs and its domains, the 10 items assessing PD including Total PD and its subscales—4 for anxiety and 6 for depression—and the 21 items assessing PTG and its factors—11 items for Factor 1, 7 items for Factor 2, and 2 items for Factor 3by sexual orientation.
Table 6.
Prevalence of ACEs, PTG, and PD by sexual orientation.
There were statistically significant differences regarding Total ACEs (t(519) = −3.298; p =< 0.001), with non-heterosexual people reporting greater levels (M = 1.86, SD = 0.70). Also, there were statistically significant differences regarding Total PD (t(519) = −4.296; p =< 0.001), with non-heterosexual individuals showing higher levels (M = 2.86, SD = 0.82). In addition, there were statistically significant differences regarding Total PTG (t(519) = 2.213; p =< 0.05), with heterosexual individuals reporting higher levels (M = 3.21, SD = 0.85). Results can be found in more detail in Table 6.
Table 7 shows the correlations between the following variables: age, Total ACEs, ACEs domains, Total PTG, PTG factors—Factor 1, Factor 2, and Factor 3, and Total PD and its subscales—anxiety and depression. The results show that almost all ACE categories correlate with each other in a significant way (p < 0.001; p < 0.05), with emotional abuse and physical abuse showing the strongest correlation (r = 591). Also, we observed that Total ACEs showed a positive and strong correlation with depression (r = 315). Furthermore, depression showed a stronger correlation with emotional neglect (r = 0.249) when compared to other ACE domains. Moreover, depression was strongly correlated with anxiety (r = 769). All the correlations can be seen in more detail in Table 7.
Table 7.
Results for the correlation values between variables.
To assess the contribution of sociodemographic variables, Total ACEs, and PTG factors on Total PD, a hierarchical multiple linear regression was conducted (see Table 8). The third model, where the three factors relating to PTG were added, increased the variance from 16.8% to 20.6%, which highlights the importance of PTG in the decrease in PD. Out of the three PTG factors, factor 2 was the strongest predictor of a lower perceived Total PD (β = −0.337; p =< 0.001). The results can be seen in more detail in Table 8.
Table 8.
Hierarchical multiple linear regression models.
To determine whether the relationship between Total ACEs and Total PD is mediated by Total PTG, the computer software by Hayes (2012) was used. Regarding Total ACEs direct effect on Total PD, we observed that Total ACEs are a positive and significant predictor of Total PD (β = 0.293, SE = 0.058, p < 0.001). The results can be seen in more detail in Table 9. The simple mediation model for PTG in the form of a statistics diagram can be seen in more detail in Figure 1.
Table 9.
Model coefficients for PTG.
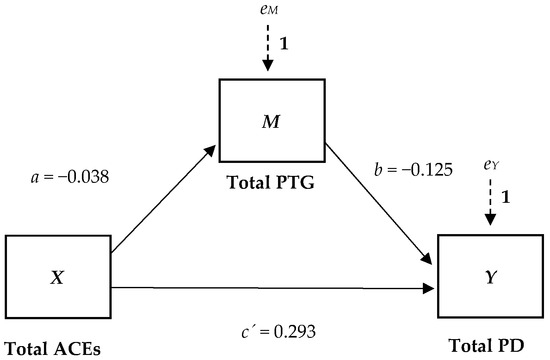
Figure 1.
A simple mediation model for PTG in the form of a statistics diagram.
Table 10 shows the Total Effect and the Indirect Effect of Total ACEs on Total PD. With the inclusion of the mediator, the indirect effect of Total ACEs on Total PD (ab = −0.038 (−0.125) = 0.005) is not statistically different from zero, as evidenced by a confidence interval that is not entirely above zero (−0.012 to 0.023), meaning that Total PTG does not mediate the relationship between Total ACEs and Total PD.
Table 10.
Total and indirect effects of ACEs on PD.
4. Discussion
The main purpose of this study was to assess the impact of ACEs on PD and PTG, as well as to determine the mediating effect of PTG on the relationship between ACEs and PD and to explore the mutual influence of these variables in a sample of adults.
The results show a high prevalence of ACEs ranging from 10.8% (physical neglect) to 59.7% (emotional abuse), with emotional abuse being the most reported category of ACEs. These results are like those found by other studies (Silva and Maia 2008; Silveira and Pereira 2023; Riedl et al. 2020), which suggest that ACEs represent an alarming phenomenon with a significant impact in various cultural contexts. These findings can be associated with the relationship between ACEs and some risk factors that may influence parenting practices, including high parental stress related especially to lower-income situations (Crouch et al. 2019), the lack of parenting skills such as little knowledge about child development (Stith et al. 2009), and the repetition of dysfunctional family patterns, where parents who experienced ACEs in their childhood may be more likely to expose their children to the same experiences (Schickedanz et al. 2021).
As far as Total PD, anxiety and depression are concerned, since the sample is not a clinical sample but a community sample and was not collected probabilistically, the absence of clinical traits was to be expected. Nevertheless, it has been found that Total ACEs are an indicator of the occurrence of Total PD symptomatology in the future (Jones et al. 2022; Thai et al. 2020). The relationship between the occurrence of ACEs and PD can be attributed to how ACEs can create situations of lack of acceptance and support, and in the face of adversity, people react in different ways. For some people, these experiences can result in long-term effects such as feelings of little validation and/or importance, reacting based on response models that are based on depression or anxiety symptoms (Watt et al. 2019), which can be crystallized and maintained over time.
No significant levels of Total PTG were observed. This topic has been the subject of some controversy in the literature (Infurna and Jajawickreme 2019; Jayawickreme and Blackie 2014) regarding the transformative role of adverse experiences in people’s growth (Tedeschi and Calhoun 2004). Some studies show reports of PTG following different traumas (Jin et al. 2014; Stein et al. 2018) and exposure to ACEs (Woodward and Joseph 2003; Schaefer et al. 2018). Research shows that early intervention reinforces protective factors among young individuals who experience sexual and physical childhood victimization (Schaefer et al. 2018) and that childhood abuse can lead to changes associated with philosophical approaches to life, to the self, and within relationships (Woodward and Joseph 2003). However, the perception of positive psychological changes following adverse experiences may be based on retrospective evaluations of growth perceived by the individual (Infurna and Jajawickreme 2019), dysfunctional reality distortions, coping strategies, and personality characteristics (Tennen and Affleck 2009). This raises the possibility that reports of PTG might be illusory (Boerner et al. 2017).
There were significant differences between groups, and concerning gender, women were found to have more Total ACEs (AlHemyari et al. 2022; Campbell et al. 2016; Giano et al. 2020; Felitti et al. 1998; Soares et al. 2016; Wong et al. 2019) and more Total PD (Agbaje et al. 2021;Matud et al. 2014) Women also reported higher levels of PTG; however, it was not statistically significant. Regarding ACEs domains, women reported more emotional abuse, more sexual abuse (Martin et al. 2022), emotional neglect (Soares et al. 2016), and more mental illness or suicide of a family member when compared to men. As far as PD, women reported more Total PD (Pereira et al. 2019), anxiety, and depression than men. According to Almuneef et al. (2017), an increased reporting of ACEs is linked to a high prevalence of psychological and mental disorders such as depression and anxiety in women. These findings can be supported by the idea that, as women experience more ACEs, they consequently experience more PD. Concerning Total PTG (even though there were no statistically significant differences regarding gender in this study) previous studies found that women show higher levels of PTG when compared to men (Tedeschi and Calhoun 1996; Vishnevsky et al. 2010), which can be related to the possibility that women tend to perceive a situation as a threat more often and rate events as more stressful (Olff et al. 2007), as a consequence leading to a more significant disruption of their assumptive world, creating conditions for greater reports of PTG (Calhoun and Tedeschi 2006). In addition, due to gender roles, women may be expected to share these experiences and to speak up about their mental health, as well as to seek psychological support (Nam et al. 2010). Moreover, women may have greater access to resources and sources of support that allow them to experience more PTG.
As for the differences between age groups, no significant statistical differences were found concerning Total ACEs, unlike previous research where there was a higher incidence of ACEs in younger people compared to older people (Campbell et al. 2016; Felitti et al. 1998; Nevárez-Mendoza and Ochoa-Meza 2022; Riedl et al. 2020). As far as ACEs domains, younger people reported more divorce or parental separation and mental illness or suicide of a family member, while older people reported more physical abuse and physical neglect (Novais et al. 2021; Riedl et al. 2020). Regarding PD, younger people reported more Total PD, anxiety, and depression, contrasting with the study findings of Pereira and colleagues (2019) in a Portuguese sample. However, previous research shows that younger adults report more psychological distress when compared to older adults (Best et al. 2023) and that younger age groups are more vulnerable to anxiety and depressive symptoms (Varma et al. 2021). Regarding PTG, findings show that older people report higher levels of Total PTG (e.g., greater openness to new possibilities and greater involvement in interpersonal relationships, as well as change in perception of the self and life, in general). These results may be linked to differences in the way they view past events (since there is more temporal spacing between older individuals and the occurrence of ACEs), which may underlie an interference in the memory process and the existence of a cognitive bias (Tennen and Affleck 2009). In addition, older individuals tend to acquire skills throughout their lives that are representative of protective factors that allow them to face difficulties such as resilience and coping strategies (Hoogland et al. 2019), leaving more room for PTG. Simultaneously, the fact that younger people present less Total PTG may mean that they have not yet had enough time or acquired the resilience to go through a process of integrating negative experiences into their identity.
Sexual minorities presented increased levels of Total ACEs and Total PD compared to heterosexual individuals (Andersen and Blosnich 2013; Ueno 2005), who showed higher levels of PTG. As for the ACE domains, sexual minorities reported more emotional and physical abuse (Balsam et al. 2005), emotional neglect, and mental illness or suicide of a family member. These results could be associated with manifestations or indicators of sexual orientation at an early age that resulted in exposure to adverse experiences. Regarding Total PD, depression, and anxiety subscales, sexual minorities reported greater levels when compared to their heterosexual counterparts. A study by McCabe et al. (2022) showed that sexual minorities are more exposed to ACEs presenting a higher risk of mental health disorders, and research by McLaughlin et al. (2012) revealed that gay or lesbian and bisexual individuals showed higher levels of psychopathology. These results may be related to adolescence (and the identity issues inherent to this life period), social stigma, lack of family support, and pressure to hide sexual minority status (Almeida et al. 2009; Hatzenbuehler 2011; Frost et al. 2007; Mimiaga et al. 2015), as well as the anticipation of rejection that can lead to isolation and low self-esteem (Hetrick and Martin 1987; Wyss 2004). Thus, these disparities seem to be associated with greater exposure to stress-inducing social experiences in a socially marginalized group (Hatzenbuehler et al. 2009; Meyer 1995), meaning that social contexts that perpetuate stigma against sexual minority groups jeopardize their mental health (Almeida et al. 2009; Hatzenbuehler 2011; Meyer 2003). Regarding Total PTG, sexual minorities presented lower levels than heterosexual individuals (who reported greater openness to new possibilities and greater involvement in interpersonal relationships, change in perception of the self and life in general, and spiritual change). This may be associated with risk factors that can hinder post-traumatic-growth for sexual minorities (Counselman-Carpenter and Redcay 2018) such as the fear of discrimination (McNair and Bush 2016) and internalized sexual stigma (Martínez et al. 2022) that may lead to not sharing adverse experiences and not seeking psychological support (Crockett et al. 2022). Moreover, the lack of social support can hinder the development of resilience, which is considered one of the most important factors in PTG development (Abraham et al. 2018; Poteat et al. 2016).
It is important to mention the need for greater investment in research in the future.
Significant, positive correlations were found between the different categories of ACEs (e.g., positive strong correlations between physical and emotional abuse, as well as a positive strong correlation between domestic violence in the household and substance abuse in the household) (Silveira and Pereira 2023), suggesting that they are multidimensional and influence each other, not occurring in an isolated way (Karatekin 2017; Soares et al. 2016; Riedl et al. 2020), which is expected. Also, emotional abuse has a stronger correlation with depression (compared to anxiety), as evidenced in the recent literature (Elmore and Crouch 2020), showing that exposure to emotional abuse is positively associated with psychopathology in adults, especially with mood disorders (Martins et al. 2014)
A significant, positive, and strong correlation was found between depression and anxiety (Lou et al. 2012). Despite being seen as two distinct conditions, they can co-exist in the same person. This can result in more severe symptoms, less effective treatment, and worse prognostics (Gorman 1996).
There was also a significant, negative, and weak correlation between Total PD and Total PTG, and these results are like those found in the literature (Liu et al. 2014). One explanation for the low coefficient could be the existence of moderators between variables such as personality and coping strategies (Liu et al. 2014). Previous studies indicate that people with different personality traits tend to have different ways of coping with stress and upsetting emotions (Dombeck and Wells-Moran 2006), and the type of coping influences the development of PTG (Yeung et al. 2016).
Furthermore, a non-significant, negative, and weak correlation was found between Total ACEs and Total PTG (meaning that the more ACEs, the less positive psychological changes), which is in line with some previous studies (Widyorini et al. 2022), but not with others (Mohr and Rosén 2017). Such discrepancies may be related to some sample collection conditions, such as sociodemographic aspects, the individual impact of the trauma associated with the subject’s characteristics such as extroversion and openness to the experience (Tedeschi and Calhoun 1996), and extrinsic aspects such as social support (Nolen-Hoeksema and Davis 1999). There is a need for greater investment in research in the future.
Factor 2 of PTG, “Change in perception of self and life in general”, proved to be the biggest predictor of less perceived psychological distress, (since it increased the variance of the respective construct from 17% to 21%), which may suggest that after facing adverse experiences, people seem to value life more, trust themselves more, and have the ability to cope with complicated situations, perceiving some benefits when facing trauma (Calhoun and Tedeschi 2006).
Lastly, regarding the mediation model, it was found that Total ACEs have a direct and positive relationship with Total PD, which means that the more ACEs, the more PD symptomatology (as previously discussed). As for the mediating effect of Total PTG, there were no significant indicators, that is, post-traumatic growth did not prove to be a mediator of the relationship between Total ACEs and Total PD symptoms in adulthood. These findings may be linked to the possibility that PTG is not sufficiently reparative of the negative impact of ACEs in terms of minimizing PD and that therapeutic approaches are needed to help individuals repair their trauma. Furthermore, reports of PTG can be illusory and not reflect real positive psychological changes. For example, a person faced with changes following a trauma (which may be considered unacceptable to them or their social environment) may use a neurotic defense mechanism to transform negative emotions into gains, and by that, the emotion of loss is absent and not integrated. In this sense, reports of PTG may be rooted in maladaptive defensive processes that enable the person to avoid pain (Boerner et al. 2017). Moreover, PTG may be an insufficient measure to capture the complexity of the phenomenon and future measures need to be studied.
4.1. Limitations
Despite its contributions, this study presents some limitations such as the fact that the sample was collected via an online survey, which limited people’s access to it since it could only be filled in by those with access to the internet and an electronic device (such as a cell phone, computer or tablet). Since the sample was collected for convenience, there was a snowball effect, with more Caucasian, female, and heterosexual people participating, so this study cannot be generalized and is not representative of the population studied. In addition, collecting data through a questionnaire can lead to the social desirability effect, and since ACEs were reported retrospectively, participants may suffer from memory lapses and/or bias. In addition, the Portuguese Version of the Family ACE Questionnaire and the Post-Traumatic Growth Inventory for the Portuguese Population (CPTI) contain questions that could act as a trigger for previous traumas and adverse experiences. At the same time, the quantitative nature of the study means that it is not possible to gain an in-depth and complex understanding of the emotional aspects and nuances of the sample, and the cross-sectional nature makes it unable to monitor changes over time and establish a causal relationship between ACEs, PD, and PTG, which is why more mixed, qualitative, and longitudinal investigations are suggested. Finally, the lack of prior research regarding the mediation effect of PTG on the relationship between ACEs and PD makes it more complicated to compare our results with other studies.
4.2. Implications
As for the implications of the present study, the findings suggest that Total ACEs are prevalent and that ACE categories do not occur independently. An explanation for this would be that exposure to one ACE can increase the vulnerability of experiencing more. This can lead to cumulative ACEs, making the recovery process more challenging. Thus, the results suggest the existence of a relationship between ACEs and mental health, with Total ACEs having a positive direct relationship with Total PD. Moreover, depression and anxiety seem to occur, which may contribute to a worse prognosis. Furthermore, PTG did not mediate the impact of ACEs on Total PD. This information is central to clinical practice and health professionals, particularly those who work with trauma and adversity. In this regard, it is important to create rigorous and appropriate assessment methods concerning ACEs and PD, reminding practitioners that if anxiety or depression is present, the other disorder should be also assessed. In addition, rigorous and adequate intervention methods should be developed to mitigate ACEs’ negative consequences on mental health and promote positive psychological changes. Moreover, the findings of this study contribute to the regulation of mental health policies through actions of promotion, prevention, and intervention with children and adolescents and their social contexts like their families and communities. This would ensure the existence of resources and access to psychological care and early interventions, providing a protective environment for children and young people, promoting protective factors and simultaneously reducing risk factors.
4.3. Conclusions
The findings of this study show that ACEs are prevalent and have a direct positive relationship with PD. It was also found that the PTG factor “Change in perception of self and life in general” was the strongest predictor of less perceived Total PD. Moreover, PTG did not mediate the relationship between ACEs and PD and, therefore, did not act as a protective factor. The findings of this study highlight the need for a more in-depth understanding of the impact of ACEs on mental health and the improvement of clinical practice and health policies.
Author Contributions
Conceptualization, H.P.; methodology, S.C. and H.P.; software, S.C. and H.P.; validation, H.P. and S.C.; formal analysis, S.C.; investigation, S.C.; resources, S.C. and H.P.; data curation, H.P.; writing—original draft preparation, S.C.; writing—review and editing, S.C. and H.P.; visualization, S.C.; supervision, H.P.; project administration, H.P.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the University of Beira Interior, Portugal, for studies involving humans (CE-UBI-Pj-2021-047, date: 20 July 2021).
Informed Consent Statement
All subjects gave their informed consent for inclusion before they participated in the study.
Data Availability Statement
Data available upon request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Abraham, Ruth, Lars Lien, and Ingrid Hanssen. 2018. Coping, resilience and posttraumatic growth among Eritrean female refugees living in Norwegian asylum reception centres: A qualitative study. International Journal of Social Psychiatry 64: 359–66. [Google Scholar] [CrossRef] [PubMed]
- Agbaje, Olaoluwa Samson, Chinwe Patience Nnaji, Evelyn Nwanebe Nwagu, Cylia Nkechi Iweama, Prince Christian Ifeanachor Umoke, Lawretta Eyuche Ozoemena, and Charles Chike Abba. 2021. Adverse childhood experiences and psychological distress among higher education students in Southeast Nigeria: An institutional-based cross-sectional study. Archives of Public Health 79: 1–15. [Google Scholar] [CrossRef] [PubMed]
- AlHemyari, Amena Hamood, Nada Adeeb Al-Zamil, Ahad Yasir Shaikh, Dalal Abdulaziz Al-Eidi, Hussam Waleed Al-Dahlan, and Sumiyah Sulaiman Al-Shamekh. 2022. Prevalence of adverse childhood experiences and their relationship to mental and physical illnesses in the Eastern Region of Saudi Arabia. Brain and Behavior 12: e2668. [Google Scholar] [CrossRef]
- Almeida, Joanna, Renee M. Johnson, Heather L. Corliss, Beth E. Molnar, and Deborah Azrael. 2009. Emotional Distress Among LGBT Youth: The Influence of Perceived Discrimination Based on Sexual Orientation. Journal of Youth and Adolescence 38: 1001–14. [Google Scholar] [CrossRef]
- Almuneef, Maha, Nathalie ElChoueiry, Hassan N. Saleheen, and Majid Al-Eissa. 2017. Gender-based disparities in the impact of adverse childhood experiences on adult health: Findings from a national study in the Kingdom of Saudi Arabia. International Journal for Equity in Health 16: 1–9. [Google Scholar] [CrossRef] [PubMed]
- Alves, Joana, Mariana Gonçalves, and Ângela Maia. 2022. Factors Associated With Physical and Psychological Health Outcomes Among Inmate Women in Portugal. Women & Criminal Justice 1–16. [Google Scholar] [CrossRef]
- Amaranggani, Anindhita Parasdyapawitra, and Kartika Sari Dewi. 2022. The role of forgiveness in post-traumatic growth: A cross-sectional study of emerging adults with adverse childhood experiences. Proceedings of International Conference on Psychological Studies 3: 1–12. Available online: https://proceeding.internationaljournallabs.com/index.php/picis/article/view/64 (accessed on 10 October 2023).
- American Psychological Association (APA). 2023. What are ACEs? Judges and Psychiatrists Leadership Iniciative. Available online: https://apafdn.org/impact/justice/judges-and-psychiatrists-leadership-initiative/free-resources/what-are-aces (accessed on 5 October 2023).
- Anda, Robert F., Vicent J. Felitti, J. Douglas Bremner, Jonh D. Walker, Charles Whitfield, Bruce D. Perry, Shanta R. Dube, and Wayne H. Giles. 2006. The enduring effects of abuse and related adverse experiences in childhood. European Archives of Psychiatry and Clinical Neuroscience 256: 174–86. [Google Scholar] [CrossRef]
- Andersen, Judith P, and John Blosnich. 2013. Disparities in Adverse Childhood Experiences among Sexual Minority and Heterosexual Adults: Results from a Multi-State Probability-Based Sample. PLoS ONE 8: e54691. [Google Scholar] [CrossRef]
- Babad, Sara, Amanda Zwilling, Kaitlin W. Carson, Victoria Fairchild, and Valentina Nikulina. 2022. Childhood Environmental Instability and Social-Emotional Outcomes in Emerging Adults. Journal of Interpersonal Violence 37: 7–8. [Google Scholar] [CrossRef]
- Balsam, Kimberly F., Esther D. Rothblum, and Theodore P. Beauchaine. 2005. Victimization Over the Life Span: A Comparison of Lesbian, Gay, Bisexual, and Heterosexual Siblings. Journal of Consulting and Clinical Psychology 73: 477–87. [Google Scholar] [CrossRef]
- Belay, Alemayehu Sayih, Melak Menberu Guangul, Wondwossen Niguse Asmare, and Gebremeskel Mesafint. 2021. Prevalence and Associated Factors of Psychological Distress among Nurses in Public Hospitals, Southwest, Ethiopia: A cross-sectional Study. Ethiopian Journal of Health Sciences 31: 1247–56. [Google Scholar] [CrossRef]
- Best, Ryan, JoNell Strough, and Wändi Bruine de Bruin. 2023. Age differences in psychological distress during the COVID-19 pandemic: March 2020–June 2021. Frontiers in Psychology 14: 1101353. [Google Scholar] [CrossRef]
- Boerner, Michaela, Stephen Joseph, and David Murphy. 2017. A Theory on Reports of Constructive (Real) and Illusory Posttraumatic Growth. Journal of Humanistic Psychology 60: 384–99. [Google Scholar] [CrossRef]
- Boullier, Mary, and Mitch Blair. 2018. Adverse childhood experiences. Paediatrics and Child Health 28: 132–37. [Google Scholar] [CrossRef]
- Brockie, Teresa N., Gail Dana-Sacco, Gwenyth R. Wallen, Holly C. Wilcox, and Jacquelyn C. Campbell. 2015. The Relationship of Adverse Childhood Experiences to PTSD, Depression, Poly-Drug Use and Suicide Attempt in Reservation-Based Native American Adolescents and Young Adults. American Journal of Community Psychology 55: 411–21. [Google Scholar] [CrossRef]
- Calhoun, Lawrence, and R. G. Tedeschi. 2006. The Foundations of Posttraumatic Growth: An Expanded Framework. In Handbook of Posttraumatic Growth: Research & Practice. Edited by L. G. Calhoun and R. G. Tedeschi. Mahwah: Lawrence Erlbaum Associates Publishers, pp. 3–23. [Google Scholar]
- Calhoun, Lawrence G., and Richard G. Tedeschi, eds. 1999. Facilitating Posttraumatic Growth: A Clinician’s Guide, 1st ed. London: Routledge. [Google Scholar] [CrossRef]
- Campbell, Jennifer A., Rebekah J. Walker, and Leonard E. Egede. 2016. Associations Between Adverse Childhood Experiences, High-Risk Behaviors, and Morbidity in Adulthood. American Journal of Preventive Medicine 50: 344–52. [Google Scholar] [CrossRef] [PubMed]
- Campos, João Oliveira Cavalcante, Clara Cela de Arruda Coelho, and Clarissa Marceli Trentini. 2021. Crescimento Pós-Traumático no Câncer de Mama: Centralidade de Evento e Coping. Psico-USF 26: 417–28. [Google Scholar] [CrossRef]
- Chapman, Daniel P, Charles L Whitfield, Vincent J. Felitti, Shanta R. Dube, Valeri J. Edwards, and Robert F. Anda. 2004. Adverse childhood experiences and the risk of depressive disorders in adulthood. Journal of Afecctive Disorders 82: 217–225. [Google Scholar] [CrossRef]
- Counselman-Carpenter, Elisabeth, and Alex Redcay. 2018. Mining for Posttraumatic Growth (PTG) in Sexual Minority Women Who Survive Intimate Partner Violence: A Conceptual Perspective. Behavioral Sciences 8: 77. [Google Scholar] [CrossRef]
- Craig, Francesco, Rocco Servidio, Maria Luigia Calomino, Francesca Candreva, Lucia Nardi, Adriana Palermo, Alberto Polito, Maria Francesca Spina, Flaviana Tenuta, and Angela Costabile. 2023. Adverse Childhood Experiences and Mental Health among Students Seeking Psychological Counseling Services. International Journal of Environmental Research and Public Health 20: 5906. [Google Scholar] [CrossRef]
- Crouch, Elizabeth, Elizabeth Radcliff, Monque Brown, and Peiyin Hung. 2019. Exploring the Association between Parenting Stress and a child’s Exposure to Adverse Childhood Experiences (ACEs). Children and Youth Services Review 102: 186–192. [Google Scholar] [CrossRef]
- Crockett, Marcelo A., Vania Martínez, and Patricio Caviedes. 2022. Barriers and Facilitators to Mental Health Help-Seeking and Experiences with Service Use among LGBT+ University Students in Chile. International Journal of Environmental Research and Public Health 19: 16520. [Google Scholar] [CrossRef]
- Devine, Katie A., Bonney Reed-Knight, Kristin A. Loiselle, Nicole Fenton, and Ronald L. Blount. 2010. Posttraumatic Growth in Young Adults Who Experienced Serious Childhood Illness: A Mixed-Methods Approach. Journal of Clinical Psychology in Medical Settings 17: 340–48. [Google Scholar] [CrossRef] [PubMed]
- Dombeck, Mark, and J. Wells-Moran. 2006. Coping Strategies and Defense Mechanisms: Basic and Intermediate Defenses. Available online: http://www.mentalhelp.net/poc/view_doc.php?id=9791&cn=353 (accessed on 1 April 2024).
- Elmore, Amanda L., and Elizabeth Crouch. 2020. The Association of Adverse Childhood Experiences With Anxiety and Depression for Children and Youth, 8 to 17 Years of Age. Academic Pediatrics 20: 600–8. [Google Scholar] [CrossRef] [PubMed]
- Esaki, Nina, and Heather Larkin. 2013. Prevalence of Adverse Childhood Experiences (ACEs) among Child Service Providers. Families in Society: The Journal of Contemporary Social Services 94: 31–37. [Google Scholar] [CrossRef]
- Felitti, Vincent J., Robert F. Anda, Dale Nordernberg, David F. Williamson, David F. Williamson, Alison M. Spitz, Valerie Edwards, Mary P. Koss, and James S. Marcks. 1998. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The adverse childhood experiences (ACE) study. American Journal of Preventive Medicine 14: 245–58. [Google Scholar] [CrossRef] [PubMed]
- Freed, Gary L., Matthew M. Davis, Dianne C. Singer, Acham Gebremariam, Sara L. Schultz, Amilcar Matos-Moreno, and Mark Wietecha. 2018. Variation in Generational Perceptions of Child Health and Well-being. Academic Pediatrics 18: 384–89. [Google Scholar] [CrossRef] [PubMed]
- Frost, David M., Jeffrey T. Parsons, and José E. Nanín. 2007. Stigma, Concealment and Symptoms of Depression as Explanations for Sexually Transmitted Infections among Gay Men. Journal of Health Psychology 12: 636–40. [Google Scholar] [CrossRef] [PubMed]
- Giano, Zachary, Denna L. Wheeler, and Randolph D. Hubach. 2020. The frequencies and disparities of adverse childhood experiences in the U.S. BMC Public Health 20: 1–12. [Google Scholar] [CrossRef]
- Giano, Zachary, Ricky L. Camplain, Carolyn Camplain, George Pro, Shane Haberstroh, Julie A. Baldwin, Denna L. Wheeler, and Randolph D. Hubach. 2021. Adverse Childhood Events in American Indian/Alaska Native Populations. American Journal of Preventive Medicine 60: 213–21. [Google Scholar] [CrossRef]
- Gignac, Gilles E., and Eva T. Szodorai. 2016. Effect size guidelines for individual differences researchers. Personality and Individual Differences 102: 74–78. [Google Scholar] [CrossRef]
- Giovanelli, Alison, Arthur J. Reynolds, Christina F. Mondi, and Suh-Ruu Ou. 2016. Adverse Childhood Experiences and Adult Well-Being in a Low-income, Urban Cohort. Pediatrics 137: e20154016. [Google Scholar] [CrossRef] [PubMed]
- Goodman, Michael L., Larissa Baker, Agnes Karambu Maigallo, Aleisha Elliott, Philip Keiser, and Lauren Raimer-Goodman. 2022. Adverse childhood experiences, adult anxiety and social capital among women in rural Kenya. Journal of Anxiety Disorders 91: 102614. [Google Scholar] [CrossRef] [PubMed]
- Gorman, Jack M. 1996. Comorbid depression and anxiety spectrum disorders. Depression and Anxiety 4: 160–68. [Google Scholar] [CrossRef]
- Hales, George, Agata Debowska, Richard Rowe, Daniel Boduszek, and Liat Levita. 2023. Comparison of Person-Centered and Cumulative Risk Approaches in Explaining the Relationship Between Adverse Childhood Experiences and Behavioral and Emotional Problems. Journal of Interpersonal Violence 38: 8065–87. [Google Scholar] [CrossRef] [PubMed]
- Hatzenbuehler, Mark L. 2011. The Social Environment and Suicide Attempts in Lesbian, Gay, and Bisexual Youth. Pediatrics 127: 896–903. [Google Scholar] [CrossRef] [PubMed]
- Hatzenbuehler, Mark L., Katherine M. Keyes, and Deborah S. Hasin. 2009. State-Level Policies and Psychiatric Morbidity In Lesbian, Gay, and Bisexual Populations. American Journal of Public Health 99: 2275–81. [Google Scholar] [CrossRef] [PubMed]
- Hayes, Andrew F. 2012. PROCESS: A Versatile Computational Tool for Observed Variable Mediation, Moderation, and Conditional Process Modeling [White Paper]. Available online: http://www.afhayes.com/public/process2012.pdf (accessed on 12 December 2023).
- Hetrick, Emery S., and A. Damien Martin. 1987. Developmental Issues and Their Resolution for Gay and Lesbian Adolescents. Journal of Homosexuality 14: 25–43. [Google Scholar] [CrossRef]
- Hoogland, Aasha I., Heather S. L. Jim, Nancy E. Schoenberg, John F. Watkins, and Graham D. Rowles. 2019. Positive Psychological Change Following a Cancer Diagnosis in Old Age. Cancer Nursing 44: 190–96. [Google Scholar] [CrossRef]
- Hughes, Karen, Mark A Bellis, Katherine A Hardcastle, Dinesh Sethi, Alexander Butchart, Christopher Mikton, Lisa Jones, and Michael P Dunne. 2017. The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. The Lancet Public Health 2: e356–e366. [Google Scholar] [CrossRef] [PubMed]
- Infurna, Frank J., and Eranda Jajawickreme. 2019. Fixing the Growth Illusion: New Directions for Research in Resilience and Posttraumatic Growth. Current Directions in Psychological Science 28: 152–58. [Google Scholar] [CrossRef]
- Jayawickreme, Eranda, and Laura E. R. Blackie. 2014. Post–traumatic Growth as Positive Personality Change: Evidence, Controversies and Future Directions. European Journal of Personality 28: 312–31. [Google Scholar] [CrossRef]
- Jayawickreme, Eranda, Frank J. Infurna, Kinan Alajak, Laura E. R. Blackie, William J. Chopik, Joanne M. Chung, Anna Dorfman, William Fleeson, Marie J. C. Forgeard, Patricia Frazier, and et al. 2020. Post-traumatic growth as positive personality change: Challenges, opportunities, and recommendations. Journal of Personality 89: 145–65. [Google Scholar] [CrossRef] [PubMed]
- Jin, Yuchang, Jiuping Xu, and Dongyue Liu. 2014. The relationship between post traumatic stress disorder and post traumatic growth: Gender differences in PTG and PTSD subgroups. Social psychiatry. Sozialpsychiatrie. Psychiatrie sociale 49: 1903–10. [Google Scholar] [CrossRef] [PubMed]
- Jones, Christopher M., Melissa T. Merrick, and Debra E. Houry. 2020. Identifying and Preventing Adverse Childhood Experiences. JAMA 323: 25–26. [Google Scholar] [CrossRef] [PubMed]
- Jones, Melissa S., Hayley Pierce, and Kevin Shafer. 2022. Gender differences in early adverse childhood experiences and youth psychological distress. Journal of Criminal Justice 83. [Google Scholar] [CrossRef]
- Kalmakis, Karen A., and Genevieve E. Chandler. 2014. Adverse childhood experiences: Towards a clear conceptual meaning. Journal of Advanced Nursing 70: 1489–501. [Google Scholar] [CrossRef] [PubMed]
- Karatekin, Canan. 2017. Adverse Childhood Experiences (ACEs), Stress and Mental Health in College Students. Stress & Health 34: 36–45. [Google Scholar] [CrossRef]
- Kaye-Tzadok, Avital, and Tamar Icekton. 2022. A phenomenological exploration of work-related post-traumatic growth among high-functioning adults maltreated as children. Frontiers in Psychology 13: 1048295. [Google Scholar] [CrossRef]
- Kessler, Ronald C., Peggy R. Barker, Lisa J. Colpe, Joan F. Epstein, Joseph C. Gfroerer, Eva Hiripi, Mary J. Howes, Sharon-Lise T. Normand, Ronald W. Manderscheid, Ellen E. Walters, and et al. 2003. Screening for Serious Mental Illness in the General Population. Archives of General Psychiatry 60: 184–189. [Google Scholar] [CrossRef] [PubMed]
- Liu, Jun-E, Hui-Ying Wang, Mu-Lan Wang, Ya-Li Su, and Pi-Lin Wang. 2014. Posttraumatic growth and psychological distress in Chinese early-stage breast cancer survivors: A longitudinal study. Psycho-Oncology 23: 437–43. [Google Scholar] [CrossRef] [PubMed]
- Lou, Peian, Yanan Zhu, Peipei Chen, Pan Zhang, Jiaxi Yu, Ning Zhang, Na Chen, Lei Zhang, Hongmin Wu, and Jing Zhao. 2012. Prevalence and correlations with depression, anxiety, and other features in outpatients with chronic obstructive pulmonary disease in China: A cross-sectional case control study. BMC Pulmonary Medicine 12: 53–53. [Google Scholar] [CrossRef] [PubMed]
- Lu, Weili, Kim T. Mueser, Stanley D. Rosenberg, and Mary Kay Jankowski. 2008. Correlates of Adverse Childhood Experiences Among Adults With Severe Mood Disorders. Psychiatric Services 59: 1018–26. [Google Scholar] [CrossRef]
- Maia, Ãngela, Carla Guimarães, Eunice Magalhães, Liliana Capitão, Márica Campos, and Susana Capela. 2006. Experiências adversas e funcionamento actual: Um estudo com jovens portugueses. In Actas do VI Simpósio Nacional de Investigação em Psicologia. Évora: Associação Portuguesa de Psicologia, vol. XII, pp. 54–73. [Google Scholar]
- Manyema, Mercy, Shane A. Norris, and Linda M. Richter. 2018. Stress begets stress: The association of adverse childhood experiences with psychological distress in the presence of adult life stress. BMC Public Health 18: 1–12. [Google Scholar] [CrossRef]
- Martin, Aisling, Carol Nixon, Kirsty Leanne Watt, Abigail Taylor, and P J Kennedy. 2022. Exploring the Prevalence of Adverse Childhood Experiences in Secure Children’s Home Admissions. Child & Youth Care Forum 51: 921–35. [Google Scholar] [CrossRef]
- Martins, Camila Maria Severi, Cristiane Von Werne Baes, Sandra Marcia de Carvalho Tofoli, and Mario Francisco Juruena. 2014. Emotional Abuse in Childhood Is a Differential Factor for the Development of Depression in Adults. Journal of Nervous & Mental Disease 202: 774–82. [Google Scholar] [CrossRef]
- Martínez, Claudio, Alemka Tomicic, Mario Dominguez, and Christian Spuler. 2022. Internalización del estigma en personas LGB: Análisis de su impacto sobre la salud mental y la búsqueda de ayuda psicoterapéutica en Chile. Terapia Psicológica 40: 49–69. [Google Scholar] [CrossRef]
- Matud, M. Pilar, Juan M. Bethencourt, and Ignacio Ibáñez. 2014. Gender differences in psychological distress in Spain. International Journal of Social Psychiatry 61: 560–568. [Google Scholar] [CrossRef]
- McCabe, Sean Esteban, Tonda L. Hughes, Sarah Beal, Rebecca J. Evans-Polce, Luisa Kcomt, Curtiss Engstrom, Brady T. West, Phil Veliz, Kate Leary, Vita V. McCabe, and et al. 2022. Sexual orientation differences in childhood sexual abuse, suicide attempts, and DSM-5 alcohol, tobacco, other drug use, and mental health disorders in the US. Child Abuse & Neglect 123: 105377. [Google Scholar] [CrossRef]
- McLaughlin, Katie A., Mark L. Hatzenbuehler, Ziming Xuan, and Kerith J. Conron. 2012. Disproportionate exposure to early-life adversity and sexual orientation disparities in psychiatric morbidity. Child Abuse & Neglect 36: 645–55. [Google Scholar] [CrossRef] [PubMed]
- McNair, Ruth P., and Rachel Bush. 2016. Mental health help seeking patterns and associations among Australian same sex attracted women, trans and gender diverse people: A survey-based study. BMC Psychiatry 16: 1–16. [Google Scholar] [CrossRef] [PubMed]
- Merrick, Melissa T., Katie A. Ports, Derek C. Ford, Tracie O. Afifi, Elizabeth T. Gershoff, and Andrew Grogan-Kaylor. 2017. Unpacking the impact of adverse childhood experiences on adult mental health. Child Abuse & Neglect 69: 10–19. [Google Scholar] [CrossRef] [PubMed]
- Meyer, Ilan H. 1995. Minority Stress and Mental Health in Gay Men. Journal of Health and Social Behavior 36: 38–56. [Google Scholar] [CrossRef] [PubMed]
- Meyer, Ilan H. 2003. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin 129: 674–97. [Google Scholar] [CrossRef] [PubMed]
- Mimiaga, Matthew J., Elizabeth F. Closson, Beena Thomas, Kenneth H. Mayer, Theresa Betancourt, Sunil Menon, and Steven A. Safren. 2015. Garnering an in-depth understanding of men who have sex with men in Chennai, India: A qualitative analysis of sexual minority status and psychological distress. Archives of Sexual Behavior 44: 2077–86. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Mohr, Danielle, and Lee A. Rosén. 2017. The Impact of Protective Factors on Posttraumatic Growth for College Student Survivors of Childhood Maltreatment. Journal of Aggression, Maltreatment & Trauma 26: 756–71. [Google Scholar] [CrossRef]
- Monnat, Shannon M., and Raeven Faye Chandler. 2015. Long-Term Physical Health Consequences of Adverse Childhood Experiences. The Sociological Quarterly 56: 723–52. [Google Scholar] [CrossRef] [PubMed]
- Nam, Suk Kyung, Hui Jung Chu, Mi Kyoung Lee, Ji Hee Lee, Nuri Kim, and Sang Min Lee. 2010. A Meta-analysis of Gender Differences in Attitudes Toward Seeking Professional Psychological Help. Journal of American College Health 59: 110–16. [Google Scholar] [CrossRef]
- National Commission for the Promotion of the Rights and Protection of Children and Young People. 2023. Annual Report on the Evaluation of the Activity of the CPCJ 2022. Activity Reports—National Commission for the Promotion of the Rights and Protection of Children and Youth. Available online: https://www.cnpdpcj.gov.pt/documents/10182/15650/Relat%C3%B3rio+de+Atividades+2022/f111c8fa-242d-4267-8c42-6b026502a704 (accessed on 24 October 2023).
- Nevárez-Mendoza, Blanca Patricia, and Gerardo Ochoa-Meza. 2022. Relationship between adverse childhood experiences and the physical and mental health in Mexican adults. Salud Mental 45: 61–69. [Google Scholar] [CrossRef]
- Nolen-Hoeksema, Susan, and Christopher G. Davis. 1999. “Thanks for sharing that”: Ruminators and their social support networks. Journal of Personality and Social Psychology 77: 801–14. [Google Scholar] [CrossRef]
- Novais, Márcia, Teresa Henriques, Maria João Vidal-Alves, and Teresa Magalhães. 2021. When Problems Only Get Bigger: The Impact of Adverse Childhood Experience on Adult Health. Frontiers in Psychology 12: 693420. [Google Scholar] [CrossRef]
- Nurius, Paula S., Sara Green, Patricia Logan-Greene, and Sharon Borja. 2015. Life course pathways of adverse childhood experiences toward adult psychological well-being: A stress process analysis. Child Abuse & Neglect 45: 143–53. [Google Scholar] [CrossRef]
- Olff, Miranda, Willie Langeland, Nel Draijer, and Berthold P. R. Gersons. 2007. Gender differences in posttraumatic stress disorder. Psychological Bulletin 133: 183–204. [Google Scholar] [CrossRef]
- Pereira, Anabela, Carla Andreia Oliveira, Ana Bártolo, Sara Monteiro, Paula Vagos, and Jacinto Jardim. 2019. Reliability and Factor Structure of the 10-item Kessler Psychological Distress Scale (K10) among Portuguese adults. Ciencia & Saude Coletiva 24: 729–36. [Google Scholar] [CrossRef]
- Pinto, Vanessa Cristina Pires, Joana Ferreira Cardoso Alves, and Ângela Costa Maia. 2015. Adversidade na infância prediz sintomas depressivos e tentativas de suicídio em mulheres adultas portuguesas. Estudos de Psicologia (Campinas) 32: 617–25. [Google Scholar] [CrossRef]
- Portuguese Association for Victim Support. 2023. Associação Portuguesa de Apoio à Vítima. Estatísticas APAV: Relatório Anual. 2022. Available online: https://apav.pt/apav_v3/images/pdf/Estatisticas-APAV_Relatorio-anual-2022.pdf (accessed on 16 October 2023).
- Poteat, V. Paul, Jerel P. Calzo, and Hirokazu Yoshikawa. 2016. Promoting Youth Agency Through Dimensions of Gay–Straight Alliance Involvement and Conditions that Maximize Associations. Journal of Youth and Adolescence 45: 1438–51. [Google Scholar] [CrossRef]
- Qu, Guangbo, Shaodi Ma, Haixia Liu, Tiantian Han, Huimei Zhang, Xiuxiu Ding, Liang Sun, Qirong Qin, Mingchun Chen, and Yehuan Sun. 2022. Positive childhood experiences can moderate the impact of adverse childhood experiences on adolescent depression and anxiety: Results from a cross-sectional survey. Child Abuse & Neglect 125: 105511. [Google Scholar] [CrossRef]
- Quan, Lijuan, Bijun Lü, Jialei Sun, Xintong Zhao, and Qingsong Sang. 2022. The relationship between childhood trauma and post-traumatic growth among college students: The role of acceptance and positive reappraisal. Frontiers in Psychology 13: 921362. [Google Scholar] [CrossRef]
- Ramiro, Laurie S., Bernadette J. Madrid, and David W. Brown. 2010. Adverse childhood experiences (ACE) and health-risk behaviors among adults in a developing country setting. Child Abuse & Neglect 34: 842–55. [Google Scholar] [CrossRef]
- Resende, Catarina, Sandra Sendas, and Ângela Maia. 2008. Estudo das características psicométricas do Posttraumatic Growth Inventory—PTGI—(Inventário de Crescimento Pós-Traumático) para a População Portuguesa. In XIII Conferência Internacional de Avaliação psicológica: Formas e contextos. Edited by Ana Paula Noronha, Carla Machado, Leandro Almeida, Miguel Gonçalves, Sara Martins and Vera Ramalho. Braga: Psiquilibrios Edições, pp. 1–16. [Google Scholar]
- Riedl, David, Astrid Lampe, Silvia Exenberger, Tobias Nolte, Iris Trawöger, and Thomas Beck. 2020. Prevalence of adverse childhood experiences (ACEs) and associated physical and mental health problems amongst hospital patients: Results from a cross-sectional study. General Hospital Psychiatry 64: 80–86. [Google Scholar] [CrossRef]
- Sánchez-Jáuregui, Teresa, Arnoldo Téllez, Diana Almaraz, Arturo Valdez, Rogelio Hinojosa-Fernández, Hugo García-Balvaneda, and Dehisy Marisol Juárez-García. 2023. Adverse Childhood Experiences in Mexico: Prevalence and Association with Sociodemographic Variables and Health Status. Psychology in Russia: State of the Art 16: 48–62. [Google Scholar] [CrossRef]
- Schaefer, Lauren M., Kathryn H. Howell, Laura E. Schwartz, Jamison S. Bottomley, and Candice B. Crossnine. 2018. A concurrent examination of protective factors associated with resilience and posttraumatic growth following childhood victimization. Child Abuse & Neglect 85: 17–27. [Google Scholar] [CrossRef]
- Schickedanz, Adam, José J. Escarce, Neal Halfon, Narayan Sastry, and Paul J. Chung. 2021. Intergenerational Associations between Parents’ and Children’s Adverse Childhood Experience Scores. Children 8: 747. [Google Scholar] [CrossRef]
- Serviço Nacional de Saúde. 2018. Distress Psicológico. Available online: https://www.sns.gov.pt/noticias/2018/01/23/distress-psicologico/ (accessed on 15 October 2023).
- Silva, Susana, and Ângela Costa Maia. 2010. Experiências adversas na infância e tentativas de suicídio em adultos com obesidade mórbida. Revista de Psiquiatria Do Rio Grande Do Sul 32: 69–72. [Google Scholar] [CrossRef][Green Version]
- Silva, Susana Sofia P., and Ângela Maia. 2008. Versão Portuguesa do Family ACE Questionnaire (Questionário da História de Adversidade na Infância). In Actas da XIII Conferência Internacional de Avaliação Psicológica: Formas e contextos. Coordinator by Ana Paula Noronha, Carla Machado, LeandroAlmeida, MiguelGonçalves, Sara Martins, and Vera Ramalho. Braga: Psiquilibrios. [Google Scholar]
- Silveira, Daniela, and Henrique Pereira. 2023. The Impact of Adverse Childhood Experiences on Mental Health and Suicidal Behaviors: A Study from Portuguese Language Countries. Journal of Child & Adolescent Trauma 16: 1041–52. [Google Scholar] [CrossRef]
- Soares, Ana Luiza Gonçalves, Laura D. Howe, Alicia Matijasevich, Fernando C. Wehrmeister, Ana M.B. Menezes, and Helen Gonçalves. 2016. Adverse childhood experiences: Prevalence and related factors in adolescents of a Brazilian birth cohort. Child Abuse & Neglect 51: 21–30. [Google Scholar] [CrossRef]
- Soares, Sara, Armine Abrahamyan, Mariana Amorim, Ana Cristina Santos, and Sílvia Fraga. 2022. Prevalence of Adverse Childhood Experiences in the First Decade of Life: A Study in the Portuguese Cohort, Generation XXI. International Journal of Environmental Research and Public Health 19: 8344. [Google Scholar] [CrossRef]
- Stein, Catherine H., Catherine E. Petrowski, Sabina M. Gonzales, Gina M. Mattei, Jessica Hartl Majcher, Maren W. Froemming, Sarah C. Greenberg, Erin B. Dulek, and Matthew F. Benoit. 2018. A Matter of Life and Death: Understanding Continuing Bonds and Post-traumatic Growth When Young Adults Experience the Loss of a Close Friend. Journal of Child and Family Studies 27: 725–38. [Google Scholar] [CrossRef]
- Stith, Sandra M., Ting Liu, L. Christopher Davies, Esther L. Boykin, Meagan C. Alder, Jennifer M. Harris, Anurag Som, Mary McPherson, and J.E.M.E.G. Dees. 2009. Risk factors in child maltreatment: A meta-analytic review of the literature. Aggression and Violent Behavior 14: 13–29. [Google Scholar] [CrossRef]
- Tedeschi, Richard G., and Lawrence G. Calhoun. 1996. The posttraumatic growth inventory: Measuring the positive legacy of trauma. Journal of Traumatic Stress 9: 455–71. [Google Scholar] [CrossRef]
- Tedeschi, Richard G., and Lawrence G. Calhoun. 2004. TARGET ARTICLE: “Posttraumatic Growth: Conceptual Foundations and Empirical Evidence”. Psychological Inquiry 15: 1–18. [Google Scholar] [CrossRef]
- Tennen, Howard, and Glenn Affleck. 2009. Assessing positive life change: In search of meticulous methods. In Medical Illness and Positive Life Change: Can Crisis Lead to Personal Transformation? Edited by Crystal L. Park, Suzanne C. Lechner, Michael. H. Antoni and Annette L. Stanton. Washington, DC: American Psychological Association, pp. 31–49. [Google Scholar] [CrossRef]
- Thai, Truc Thanh, Phuong Le Tran Cao, Loan Xuan Kim, Doan Phuoc Tran, Minh Binh Bui, and Han Hy Thi Bui. 2020. The effect of adverse childhood experiences on depression, psychological distress and suicidal thought in Vietnamese adolescents: Findings from multiple cross-sectional studies. Asian Journal of Psychiatry 53: 102134. [Google Scholar] [CrossRef]
- Thompson, Martie P., J. B. Kingree, and Dorian Lamis. 2019. Associations of adverse childhood experiences and suicidal behaviors in adulthood in a U.S. nationally representative sample. Child: Care, Health and Development 45: 121–28. [Google Scholar] [CrossRef]
- Ueno, Koji. 2005. Sexual Orientation and Psychological Distress in Adolescence: Examining Interpersonal Stressors and Social Support Processes. Social Psychology Quarterly 68: 258–77. [Google Scholar] [CrossRef]
- Varela, Ana, Anabela Pereira, Ariana Pereira, and José Carlos Santos. 2017. Psychological distress: Contributes for the portuguese adaption of the SQ-48. Psicologia, Saúde & Doença 18: 278–96. [Google Scholar] [CrossRef]
- Varma, Prerna, Moira Junge, Hailey Meaklim, and Melinda L. Jackson. 2021. Younger people are more vulnerable to stress, anxiety and depression during COVID-19 pandemic: A global cross-sectional survey. Progress in Neuro-Psychopharmacology and Biological Psychiatry 109: 2–8. [Google Scholar] [CrossRef]
- Vishnevsky, Tanya, Arnie Cann, Lawrence G. Calhoun, Richard G. Tedeschi, and George J. Demakis. 2010. Gender Differences in Self-Reported Posttraumatic Growth: A Meta-Analysis. Psychology of Women Quarterly 34: 110–120. [Google Scholar] [CrossRef]
- Watt, Toni, Natalie Ceballos, Seoyoun Kim, Xi Pan, and Shobhit Sharma. 2019. The Unique Nature of Depression and Anxiety among College Students with Adverse Childhood Experiences. Journal of Child & Adolescent Trauma 13: 163–72. [Google Scholar] [CrossRef]
- Widyorini, Endang, Maria Yang Roswita, Emiliana Primastuti, and Daniswara Agusta Wijaya. 2022. The role of resilience towards the correlation between adverse childhood experiences and post-traumatic growth. The Open Psychology Journal 15: 1–11. [Google Scholar] [CrossRef]
- Wong, Alexander E., Shrija R. Dirghangi, and Shelley R. Hart. 2019. Self-concept clarity mediates the effects of adverse childhood experiences on adult suicide behavior, depression, loneliness, perceived stress, and life distress. Self and Identity 18: 247–66. [Google Scholar] [CrossRef]
- Woodward, Clare, and Stephen Joseph. 2003. Positive change processes and post-traumatic growth in people who have experienced childhood abuse: Understanding vehicles of change. Psychology and Psychotherapy: Theory, Research and Practice 76: 267–83. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). 2020. Adverse Childhood Experiences International Questionnaire (ACE-IQ). Available online: https://www.who.int/publications/m/item/adverse-childhood-experiences-international-questionnaire-(ace-iq).
- Wyss, Shannon E. 2004. ‘This was my hell’: The violence experienced by gender non?conforming youth in US high schools. International Journal of Qualitative Studies in Education 17: 709–30. [Google Scholar] [CrossRef]
- Yeung, Nelson C. Y., Qian Lu, Celia C. Y. Wong, and Hung C. Huynh. 2016. The roles of needs satisfaction, cognitive appraisals, and coping strategies in promoting posttraumatic growth: A stress and coping perspective. Psychological Trauma: Theory, Research, Practice, and Policy 8: 284–92. [Google Scholar] [CrossRef]
- Yuan, Manqiong, Fengzhi Qin, Zi Zhou, and Ya Fang. 2021. Gender-specific effects of adverse childhood experiences on incidence of activities of daily life disability in middle-age and elderly Chinese population. Child Abuse & Neglect 117: 105079. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).