

The Public Health Crisis Conceptual Model: Historical Application to the World’s First Nuclear Bomb Test




Abstract
1. Introduction
2. Methods
3. Results
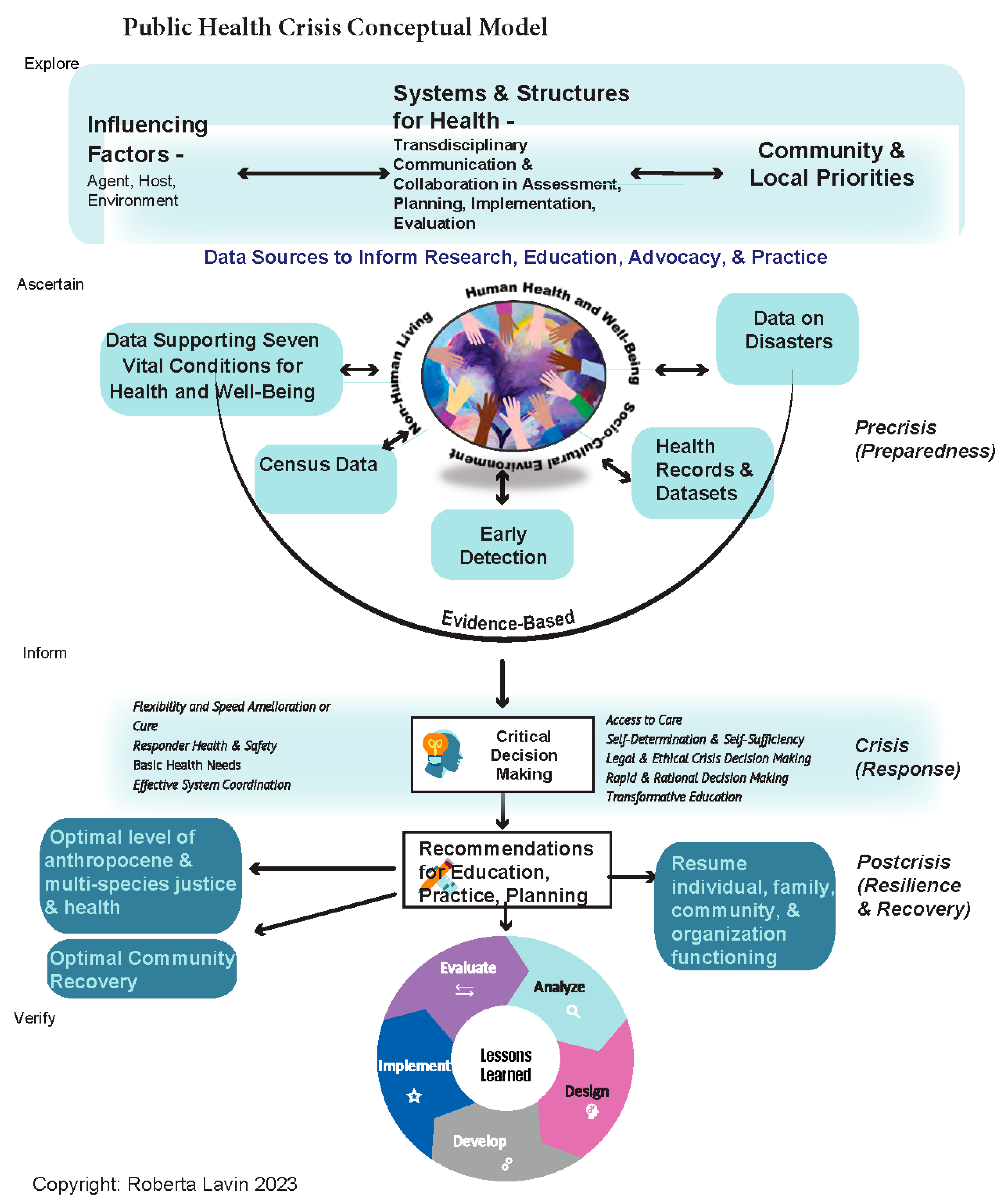
3.1. Influencing Factors
3.2. Systems and Structures
Besides the hazards normally present during construction and operation of a large chemical plant, dangers of a new kind were expected here. Two types of radiation hazard were anticipated—neutrons generated in the pile and alpha particles, beta particles and gamma rays emitted by products of the pile. Although the general effects of the radiations had been proved to be similar to those of X-rays, very little detailed knowledge was available. Obviously the amounts of radioactive material to be handled were many times greater than had ever been encountered before.
The health group had to plan three programs: (1) provision of instruments and clinical tests to detect any evidence of exposure of the personnel; (2) research on the effects of radiation on persons, instruments, etc.; and (3) estimates of what shielding and safety measures must be incorporated in the design and plan of operation of the plant.
3.3. Community and Local Priorities
3.4. Data Sources
- 41 bibliographies;
- 20 reports on fallout;
- 230 reports on monitoring, composition and distribution;
- 111 reports on effects;
- 12 reports on protective measures and decontamination;
- 12 reports on natural radioactivity;
- 21 reports on tolerance to radiation.
- The social determinants of health (Healthy People 2030, U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion n.d.);
- The seven vital conditions for health and well-being (Community Commons n.d.b);
- County-level statistics on the composition of the population (e.g., age and sex, race and ethnicity, population characteristics, housing, family and living arrangements, education, computer access and use, transportation, and income and poverty) (U.S. Census Bureau n.d.b);
- County health rankings and roadmaps (University of Wisconsin, Population Health Institute n.d.);
- National health statistics (Centers for Disease Control and Prevention, National Center for Health Statistics 2023);
- New Mexico Health and Human Services Data Book (New Mexico Human Services Department 2022).
3.5. Critical Decision Making
3.6. Recommendations for Education, Practice, and Planning
4. Discussion
… Volume 1 reviews developments since the 1957 hearings and presents new data on atmospheric and global fallout levels. It was stated that the program of fallout sampling and monitoring supported by the AEC is quite comprehensive and during 1959 approximately $2.6 million was spent on a program of scientific research with the purpose of understanding the factors that influence the patterns and rates of fallout onto the earth’s surface. This has meant sampling longitudinally, latitudinally, [sic] and vertically. A training program for scientists to carry out this program was maintained. Experimental and laboratory work centered on the movement of fallout into the food chain and water supplies and the effects of ionizing radiation on the human body and on human germ cells.
5. Limitations
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Adam, Frédéric, Dorota Kuchta, and Stanisław Stanek. 2022. Rational Decisions in Organisations: Theoretical and Practical Aspects. Available online: https://www.routledge.com/Rational-Decisions-in-Organisations-Theoretical-and-Practical-Aspects/Adam-Kuchta-Stanek/p/book/9781032193953 (accessed on 1 December 2023).
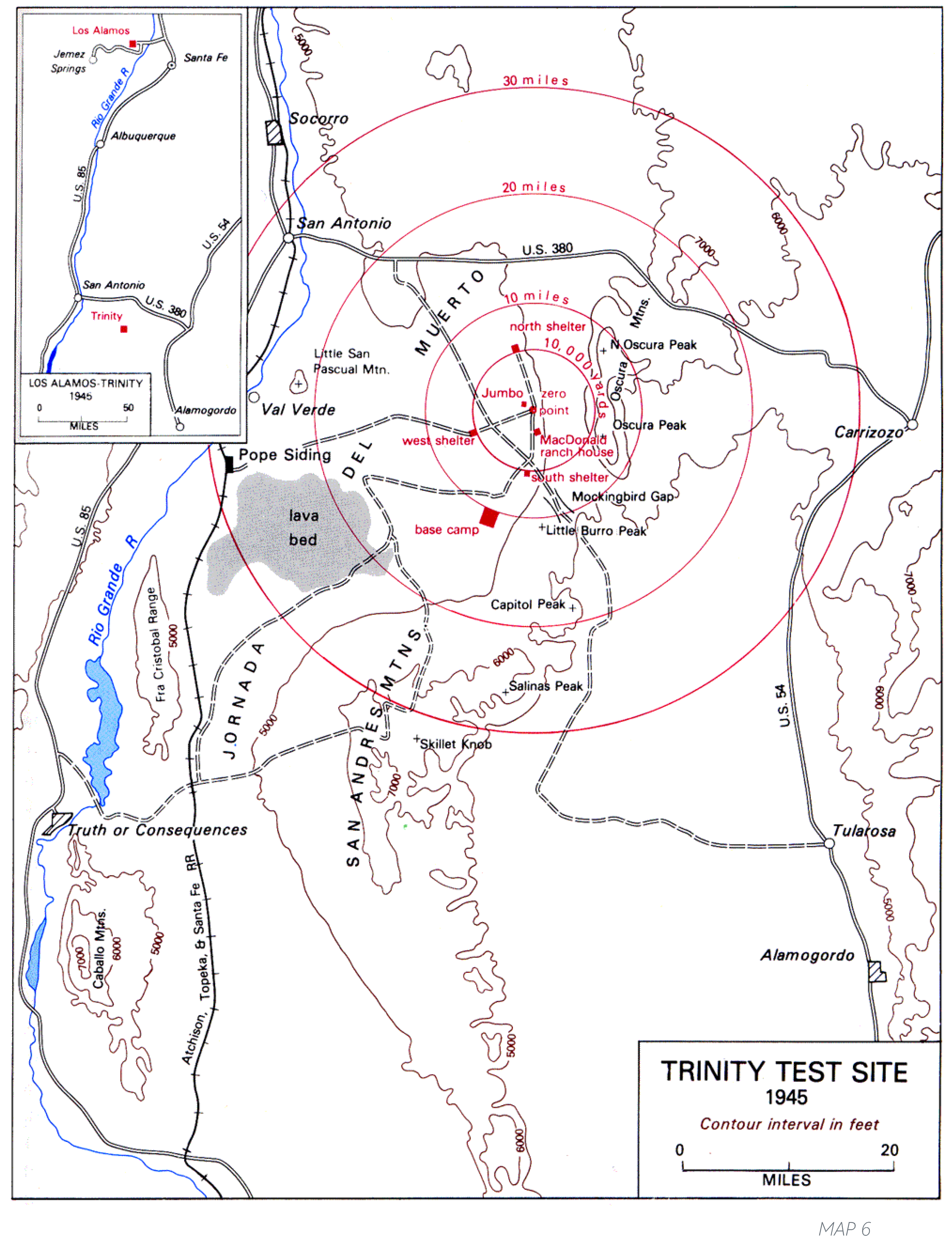
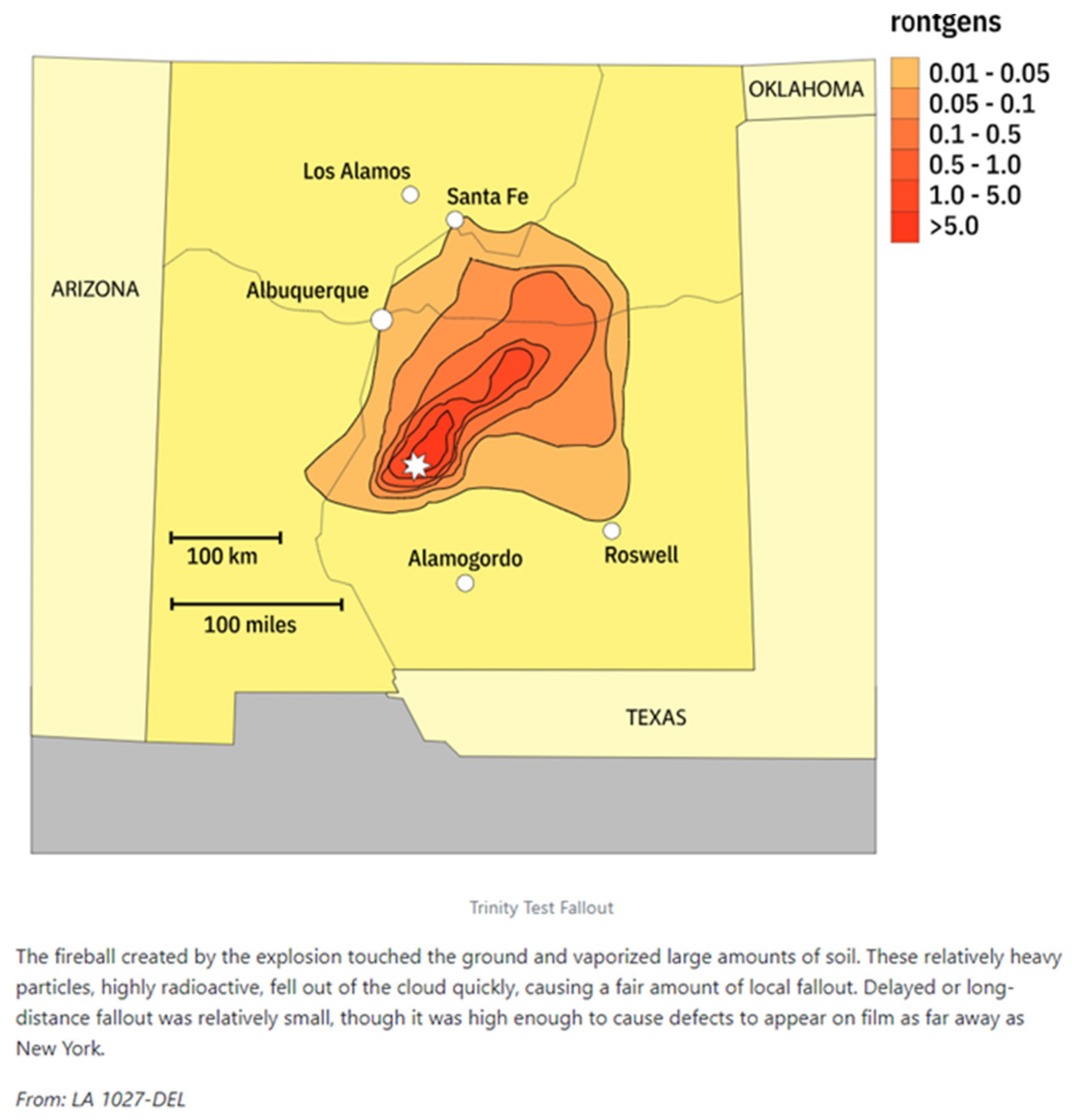
- Atomicarchive.com. n.d. Trinity Test Fallout. Media Gallery, Maps. Available online: https://www.atomicarchive.com/media/maps/trinity-fallout.html (accessed on 27 November 2023).
- Beaton, Randal, Elizabeth Bridges, Mary K. Salazar, Mark W. Oberle, Andy Stergachis, Jack Thompson, and Patricia Butterfield. 2008. Ecological model of disaster management. AAOHN Journal: Official Journal of the American Association of Occupational Health Nurses 56: 471–78. [Google Scholar] [CrossRef] [PubMed]
- Bell, Sue Anne, Lydia K. Krienke, Sarah Dickey, and Raymond G. De Vries. 2021a. “Helping fill that gap:” A qualitative study of aging in place after disaster through the lens of home-based care providers. BMC Geriatrics 21: 235. [Google Scholar] [CrossRef] [PubMed]
- Bell, Sue Anne, Sarah Dickey, and Marie-Anne Rosemberg. 2021b. “You get three different hats on and try to figure it out:” Home based care provision during a disaster. BMC Nursing 20: 155. [Google Scholar] [CrossRef] [PubMed]
- Bronfenbrenner, Urie. 1979. The Ecology of Human Development: Experiments by Nature and Design. Available online: https://www.hup.harvard.edu/books/9780674224575 (accessed on 1 December 2023).
- Centers for Disease Control and Prevention. 1999. Ten Great Public Health Achievements—United States, 1900–1999; Atlanta: Centers for Disease Control and Prevention, vol. 48. Available online: https://www.cdc.gov/mmwr/pdf/wk/mm4812.pdf (accessed on 1 December 2023).
- Centers for Disease Control and Prevention. 2010. Final Report of the Los Alamos Historical Document Retrieval 502 and Assessment (LAHDRA) Project [Government]. Final Report of the Los Alamos Historical Document Re-503 trieval and Assessment (LAHDRA) Project. Available online: https://stacks.cdc.gov/view/cdc/131522 (accessed on 15 December 2023).
- Centers for Disease Control and Prevention, National Center for Health Statistics. 2018. Stats of the State of New Mexico [Government]; Hyattsville: National Center for Health Statistics. Available online: https://www.cdc.gov/nchs/pressroom/states/newmexico/newmexico.htm (accessed on 2 December 2023).
- Centers for Disease Control and Prevention, National Center for Health Statistics. 2023. National Center for Health Statistics; Hyattsville: National Center for Health Statistics. Available online: https://www.cdc.gov/nchs/index.htm (accessed on 3 December 2023).
- Community Commons. n.d.a Basic Needs for Health & Safety As a Vital Condition. Available online: https://www.communitycommons.org/collections/Basic-Needs-for-Health-and-Safety-as-a-Vital-Condition (accessed on 2 December 2023).
- Community Commons. n.d.b Seven Vital Conditions for Health and Well-Being. Community Commons. Available online: https://www.communitycommons.org/collections/Seven-Vital-Conditions-for-Health-and-Well-Being#:~:text=Our%20freedom%20to%20thrive%20depends,care%2C%20and%20other%20basic%20necessities (accessed on 2 December 2023).
- Cook, Cathy. 2023. Setback for Downwinders: Congress pulls funding. Albuquerque Journal. Available online: https://abqjournal.pressreader.com/article/281483576159657 (accessed on 7 December 2023).
- Cuthbertson, Joe, and Greg Penney. 2023. Ethical Decision Making in Disaster and Emergency Management: A Systematic Review of the Literature. Prehospital and Disaster Medicine 38: 622–27. Available online: https://www.cambridge.org/core/services/aop-cambridge-core/content/view/4878C7119B423DA49BD1FF117835F188/S1049023X23006325a.pdf/div-class-title-ethical-decision-making-in-disaster-and-emergency-management-a-systematic-review-of-the-literature-div.pdf (accessed on 3 December 2023).
- Dick, James L., William R. Hurdlow, and Ellen M. Hippeli. 1956. Safe Levels of Contamination from Fission Products. Report (AFSWC-TN-56-2, 29 pps). New Mexico: Air Force Special Weapons Center. Kirtland, Air Force Base. [Google Scholar]
- Environmental Protection Agency. n.d. Significant Discoveries and the History of Radiation Protection [Government]; Washington: Environmental Protection Agency. Available online: https://www.epa.gov/sites/default/files/2018-12/documents/significant_discoveries_history_radiation_protection-worksheet_rp_1.pdf (accessed on 3 December 2023).
- Faerron Guzman, Carlos, and Teddie Potter. n.d. Planetary Health Education Framework. Washington: Planetary Health Alliance. Available online: https://www.planetaryhealthalliance.org/education-framework (accessed on 13 December 2023).
- Federal Emergency Management Agency. 2023. Radiological Emergency Preparedness. Risk Management; Washington: Federal Emergency Management Agency. Available online: https://www.fema.gov/emergency-managers/practitioners/hazardous-response-capabilities/radiological (accessed on 16 November 2023).
- Glanz, Karen, Barbara K. Rimer, and Kasisomayajula Viswanath, eds. 2015. Health Behavior: Theory, Research, and Practice, 5th ed. Hoboken: Wiley. Available online: https://www.wiley.com/en-us/Health+Behavior%3A+Theory%2C+Research%2C+and+Practice%2C+5th+Edition-p-9781118629000 (accessed on 14 December 2023).
- Gomez, Myrriah. 2017. Unknowing, Unwilling and Uncompensated: The Effects of the Trinity Test on New Mexicans and the Potential Benefits of a Radiation Exposure Compensation Act (RECA) Amendment. Available online: https://2da8c03d-74f5-4bef-aa16-a6b9c4cb1631.filesusr.com/ugd/2b2028_8e221b260de7468bbcb67cbddc498dbe.pdf (accessed on 14 December 2023).
- Gostin, Lawrence O. 2007. A theory and definition of public health law. Journal of Health Care Law and Policy 10: 1–12. Available online: https://digitalcommons.law.umaryland.edu/jhclp/vol10/iss1/2 (accessed on 14 December 2023).
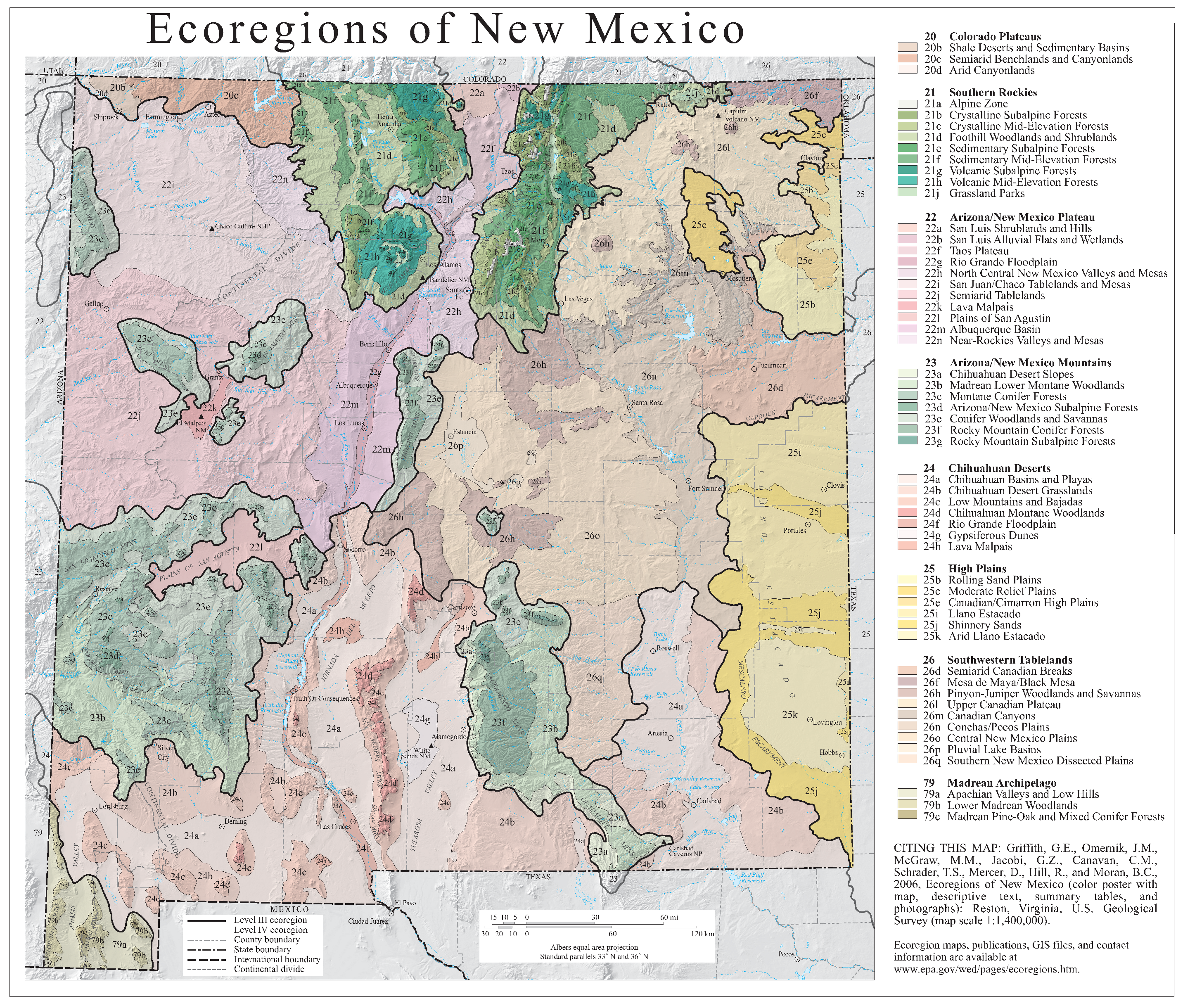
- Griffith, Glen E., J. M. Omernik, Maryann M. McGraw, Gerald Z. Jacobi, Christopher M. Canavan, T. Scott Schrader, David Mercer, Robert Hill, and Brian C. Moran. 2006. Ecoregions of New Mexico (Color Poster with Map, Descriptive Text, Summary Tables, and Photographs) [Map]; Reston: U.S. Geological Survey. Available online: https://gaftp.epa.gov/EPADataCommons/ORD/Ecoregions/nm/nm_pg.pdf (accessed on 3 December 2023).
- Grove, Susan K., and Jennifer Gray. 2021. Burns and Grove’s the Practice of Nursing Research: Appraisal, Synthesis, and Generation of Evidence, 9th ed. Amsterdam: Elsevier. [Google Scholar]
- Gultekin, Laura, Yasamin Kusunoki, Laura Sinko, Lindsay Cannon, Kathryn Abramoski, Angubeen G. Khan, and Julia Seng. 2019. The eco-social trauma intervention model. Public Health Nursing 36: 709–15. [Google Scholar] [CrossRef] [PubMed]
- Healthy People 2030, U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion. n.d. Social Determinants of Health. Healthy People 2030. Available online: https://health.gov/healthypeople/priority-areas/social-determinants-health (accessed on 14 December 2023).
- Hodge, James G., Jr., Andrea M. Garcia, Evan D. Anderson, and Torrey Kaufman. 2009. Emergency legal preparedness for hospitals and health care personnel. Disaster Medicine and Public Health Preparedness 3 Suppl. S2: S37–S44. [Google Scholar] [CrossRef]
- Institute of Medicine. 2003. Preparing for the Psychological Consequences of Terrorism: A Public Health Strategy. Washington: National Academies Press. [Google Scholar] [CrossRef]
- Institute of Medicine. 2009. Guidance for Establishing Crisis Standards of Care for Use in Disaster Situations: A Letter Report. Washington: The National Academies Press. [Google Scholar] [CrossRef]
- Jones, Vincent C. 1985. The Atomic Communities in New Mexico. In United States Army in World War II: Special Studies: Manhattan: The Army and the Atomic Bomb. Washington: United States Army, Center of Military History, p. 479. Available online: https://history.army.mil/html/books/011/11-10/CMH_Pub_11-10.pdf (accessed on 25 November 2023).
- Khare, Pooja, Preeti Nair, Amit Khare, Vandana Singh, and Rhiti Chatterjee. 2014. The Road To Radiation Protection: A Rocky Path. Journal of Clinical and Diagnostic Research: JCDR 8: ZE01–ZE04. [Google Scholar] [CrossRef] [PubMed]
- Lavin, Roberta, and Fermin Ramos. 2022. Disaster Risk Assessment and Safety Training Interprofessional Capability (DRASTIC) Tool [Dataset]. Available online: https://www.arcgis.com/home/item.html?id=fe701977973b451da12dc271573b20a6 (accessed on 14 December 2023).
- Lavin, Roberta, and Sylvia Menifee. 2009. Disaster Case Management: Implementation Guide; Washington: U.S. Department of Health and Human Services, Administration for Children and Families. Available online: https://cybercemetery.unt.edu/archive/nccd/20110426214344/http://www.acf.hhs.gov/ohsepr/dcm/docs/Draft_DCM_ImplementationGuide.pdf (accessed on 14 December 2023).
- Lavin, Roberta, Lisa Schemmel-Rettenmeier, and Molly Frommelt-Kuhle. 2012. Reconsidering “special needs” populations during a disaster. Annual Review of Nursing Research 30: 125–47. [Google Scholar] [CrossRef] [PubMed]
- Lavin, Roberta, Tener G. Veenema, Joanne C. Langan, Rachel L. Charney, Rick S. Zimmerman, and Annah Bender. 2019. Zika and Flint water public health emergencies: Disaster training tool kits relevant to pregnant women and children. The Journal of Perinatal & Neonatal Nursing 33: 229. [Google Scholar] [CrossRef]
- Lavin, Roberta, Xi Gong, Fermin Ramos, Mary Pat Couig, Xiaozhong Yu, Yujian Lu, and Heidi H. Rogers. 2023. Climate change associated disasters—Linking nursing schools, regional risks, and pillars of health and well-being. Manuscript submitted for publication. [Google Scholar]
- Lopez, C. Todd. 2022. Building Asymmetric Advantage in Indo-Pacific Part of DOD Approach to Chinese Aggression [Government]; Virginia: U.S. Department of Defense. Available online: https://www.defense.gov/News/News-Stories/Article/Article/3107197/building-asymmetric-advantage-in-indo-pacific-part-of-dod-approach-to-chinese-a/ (accessed on 16 November 2023).
- Los Alamos Historical Document Retrieval and Assessment Project, National Center for Environmental Health Studies U.S. Radiation Studies Branch, ENSR Corporation, Shonka Research Associates, and ChemRisk. 2010. Final Report of the Los Alamos Historical Document Retrieval and Assessment (LAHDRA) Project. Available online: https://stacks.cdc.gov/view/cdc/131522 (accessed on 14 December 2023).
- Mousseau, Timothy A. 2021. The Biology of Chernobyl. Annual Review of Ecology, Evolution, and Systematics 52: 87–109. [Google Scholar] [CrossRef]
- New Mexico Department of Health, Office of New Mexico Vital Records and Health Statistics, Public Health Division. 2002. New Mexico Public Health Achievements During the 20th Century. Santa Fe: New Mexico Department of Health. Available online: https://www.nmhealth.org/data/view/vital/1884/ (accessed on 3 December 2023).
- New Mexico Department of Homeland Security and Emergency Management. n.d. Building a Resilient New Mexico. Available online: https://www.nmdhsem.org/ (accessed on 16 November 2023).
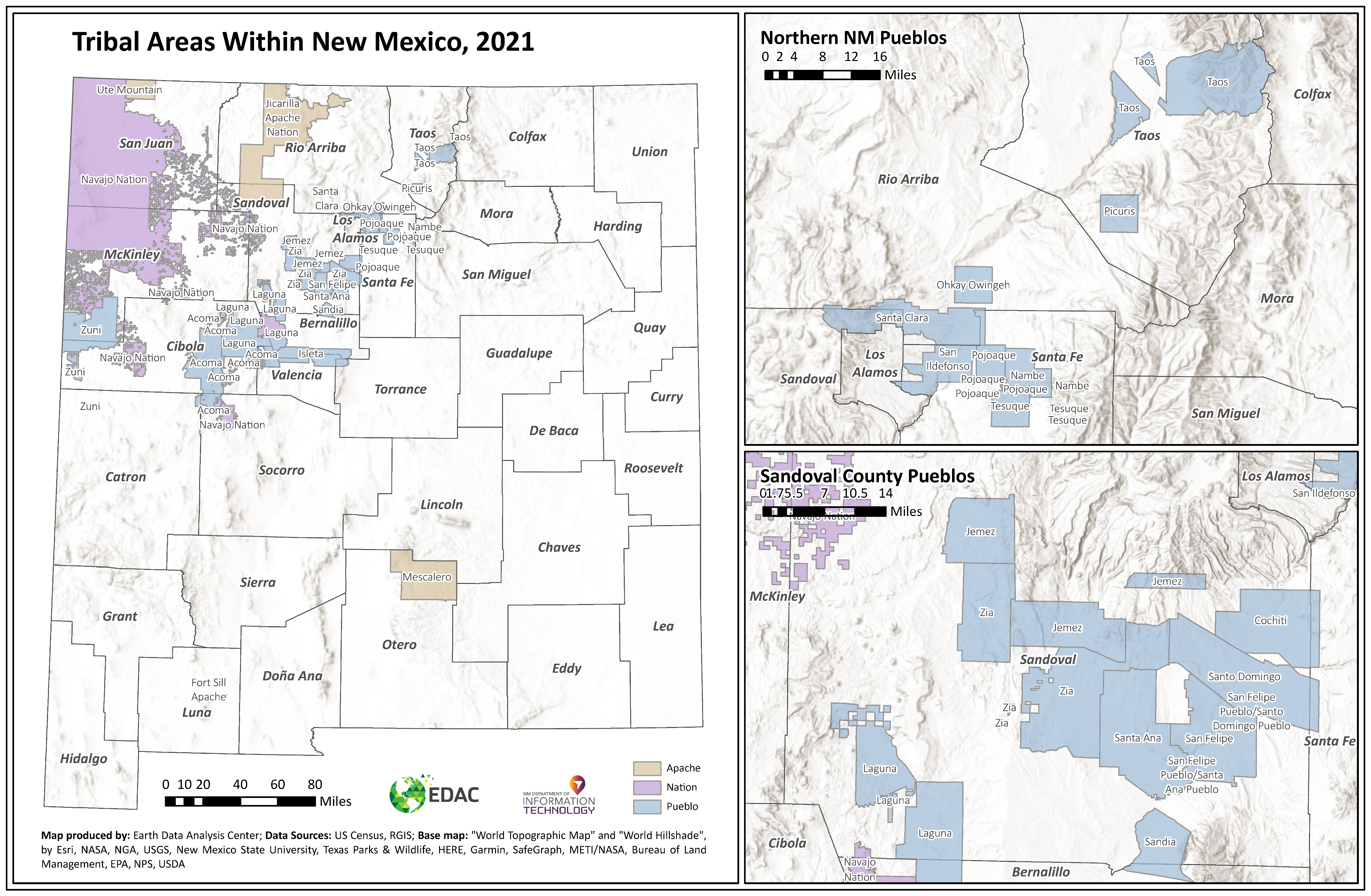
- New Mexico Department of Information Technology. 2021. Tribal Areas Within New Mexico. Available online: https://www.doit.nm.gov/wp-content/uploads/sites/4/2021/12/NM_Tribal_Areas_2021.pdf (accessed on 20 March 2024).
- New Mexico Human Services Department. 2022. New Mexico Health & Human Services Data Book. Santa Fe: New Mexico Human Services Department, vol. 32022.2, p. 501. Available online: https://www.hsd.state.nm.us/wp-content/uploads/Data-Book-2022-FINAL-Spring-2022.pdf (accessed on 16 November 2023).
- New Mexico Indian Affairs Department. n.d. History. Available online: https://www.iad.state.nm.us/about-us/history/ (accessed on 20 March 2024).
- NM Department of Homeland Security and Emergency Management. n.d. Hazardous Materials Program. Available online: https://www.nmdhsem.org/preparedness-bureau/hazmat-program/ (accessed on 20 November 2023).
- Oxford English Dictionary. n.d. Downwinder. Available online: https://www.oed.com/search/dictionary/?scope=Entries&q=downwinder (accessed on 20 March 2024).
- Phelan, Joy. 2022. How Many Nuclear Weapons Exist, and Who Has Them? Scientific American. Available online: https://www.scientificamerican.com/article/how-many-nuclear-weapons-exist-and-who-has-them/ (accessed on 16 November 2023).
- Philippe, Sébastien, Susan Alzner, Gilbert P. Compo, Mason Grimshaw, and Megan Smith. 2023. Fallout from U.S. atmospheric tests in New Mexico and Nevada (1945–1962). arXiv arXiv:2307.11040. Available online: https://arxiv.org/ftp/arxiv/papers/2307/2307.11040.pdf (accessed on 1 December 2023).
- Priya, Arya. 2021. Case Study Methodology of Qualitative Research: Key Attributes and Navigating the Conundrums in Its Application. Sociological Bulletin 70: 94–110. [Google Scholar] [CrossRef]
- Radiation Emergency Medical Management. 2023. Nuclear Detonation: Weapons, Improvised Nuclear Devices; Washington: U.S. Department of Health & Human Services. Available online: https://remm.hhs.gov/nuclearexplosion.htm (accessed on 16 November 2023).
- Shigemura, Jun, Takero Terayama, Mie Kurosawa, Yuki Kobayashi, Hiroyuki Toda, Masanori Nagamine, and Aihide Yoshino. 2021. Mental health consequences for survivors of the 2011 Fukushima nuclear disaster: A systematic review. Part 1: Psychological consequences. CNS Spectrums 26: 14–29. [Google Scholar] [CrossRef] [PubMed]
- Shultz, James M., David Forbes, David Wald, Fiona Kelly, Helena M. Solo-Gabriele, Alexa Rosen, Zelde Espinel, Andrew McLean, Oscar Bernal, and Yuval Neria. 2013. Trauma signature analysis of the great East Japan disaster: Guidance for psychological consequences. Disaster Medicine and Public Health Preparedness 7: 201–14. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Shultz, James M., Zelde Espinel, Sandro Galea, and Dori Reissman. 2007. Disaster ecology: Implications for disaster psychiatry. In Textbook of Disaster Psychiatry. Edited by Robert J. Ursano, Carol S. Fullerton, Beverley Raphael and Lars Weisaeth. Cambridge: Cambridge University Press, pp. 69–96. [Google Scholar] [CrossRef]
- Simon, Steven L. 2020. Introduction to the Trinity Nuclear Test Collection of Papers. Health Physics 119: 389. [Google Scholar] [CrossRef] [PubMed]
- Simon, Steven L., André Bouville, and Harold L. Beck. 2021. Estimated radiation doses and projected cancer risks for New Mexico residents from exposure to radioactive fallout from the Trinity Nuclear Test. Nuclear Technology 207: S380–S396. Available online: https://www.tandfonline.com/doi/abs/10.1080/00295450.2021.1918985 (accessed on 28 November 2023).
- Smyth, Henry D. 1945. Atomic Energy for Military Purposes: A General Account of the Development of Methods of Using Atomic Energy for Military Purposes; Princeton: Princeton University Press, p. 264. Available online: https://www.osti.gov/opennet/manhattan-project-history/publications/smyth_report.pdf (accessed on 26 November 2023).
- The White House. 2022. National Security Strategy; Washington: The White House, p. 48. Available online: https://www.whitehouse.gov/wp-content/uploads/2022/10/Biden-Harris-Administrations-National-Security-Strategy-10.2022.pdf (accessed on 16 November 2023).
- Tularosa Basin Downwinders Consortium. n.d.a Affidavits. Trinitydownwinders. Available online: https://www.trinitydownwinders.com/affidavits (accessed on 9 December 2023).
- Tularosa Basin Downwinders Consortium. n.d.b Tularosa Basin Downwinders Consortium. Trinitydownwinders. Available online: https://www.trinitydownwinders.com (accessed on 9 December 2023).
- U.S. Census Bureau. 1940. New Mexico. p. 696. Available online: https://www2.census.gov/library/publications/decennial/1940/population-volume-1/33973538v1ch07.pdf (accessed on 25 November 2023).
- U.S. Census Bureau. 2021. New Mexico. Census.Gov, Guide to 2010 State and Local Census Geography. Available online: https://www.census.gov/geographies/reference-files/2010/geo/state-local-geo-guides-2010/new-mexico.html (accessed on 26 November 2023).
- U.S. Census Bureau. n.d.a. QuickFacts: New Mexico. Available online: https://www.census.gov/quickfacts/fact/table/NM/PST045222 (accessed on 26 November 2023).
- U.S. Census Bureau. n.d.b. U.S. Census Bureau Quickfacts: Lincoln County, New Mexico. QuickFacts. Available online: https://www.census.gov/quickfacts/fact/table/lincolncountynewmexico,NM/PST045222 (accessed on 26 November 2023).
- U.S. Congress. 1959. Fallout from Nuclear Weapons Tests. Hearings before the Special Subcommittee on Radiation of the Joint Committee on Atomic Energy, Congress of the United States, Eighty-Sixth Congress, First Session on fallout from nuclear weapons tests, May 5, 6, 7, and 8, 1959. Volume 1. Available online: https://www.osti.gov/biblio/6290229 (accessed on 26 November 2023).
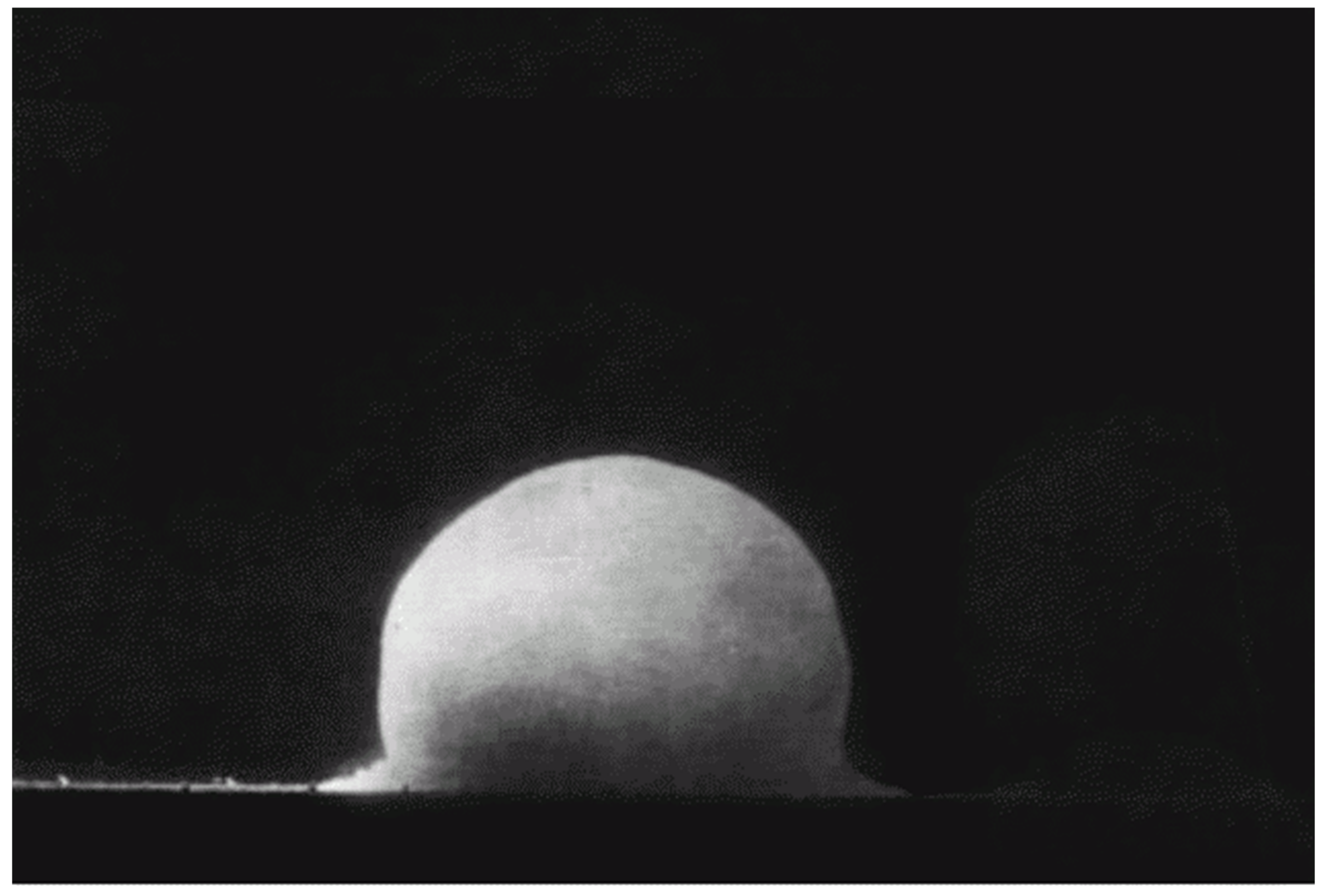
- U.S. Department of Energy. n.d. Trinity Site—World’s First Nuclear Explosion; Washington: Trinity Site-World’s First Nuclear Explosion, Office of Legacy Management. Available online: https://www.energy.gov/lm/trinity-site-worlds-first-nuclear-explosion (accessed on 28 November 2023).
- U.S. Department of Energy, Office of History and Heritage Resources. n.d. Manhattan Project: Espionage and the Manhattan Project, 1940–1945. The Manhattan Project: An Interactive History. Available online: https://www.osti.gov/opennet/manhattan-project-history/Events/1942-1945/espionage.htm (accessed on 29 November 2023).
- U.S. Department of Justice. 2023. Radiation Exposure Compensation Act Trust Fund. Available online: https://www.justice.gov/d9/2023-03/reca_fy_2024_pb_narrative_3.1.23_omb_cleared.pdf (accessed on 14 December 2023).
- U.S. Nuclear Regulatory Commission. 2022. New Mexico. NRC Web. Available online: https://www.nrc.gov/info-finder/region-state/new-mexico.html (accessed on 26 November 2023).
- University of Wisconsin, Population Health Institute. n.d. Lincoln, New Mexico: County Health Rankings & Roadmaps. Madison: Explore Health Rankings. Available online: https://www.countyhealthrankings.org/explore-health-rankings/new-mexico/lincoln (accessed on 26 November 2023).
- US Air Force, US Army, Department of Energy, and National Park Service. n.d. Trinity: World’s First Nuclear Test. Available online: https://www.afnwc.af.mil/About-Us/History/Trinity-Nuclear-Test/ (accessed on 25 November 2023).
- Veenema, Tener Goodwin, Roberta Proffitt Lavin, Sarah Schneider-Firestone, Mary Pat Couig, Joanne C. Langan, Kristine Qureshi, Danny Scerpella, and Lesley Sasnett. 2019. National assessment of nursing schools and nurse educators readiness for radiation emergencies and nuclear events. Disaster Medicine and Public Health Preparedness 13: 936–45. [Google Scholar] [CrossRef] [PubMed]
- Wallace, Roger. 1958. Bibliography of Technical Reports on the Effects of Fallout (UCRL–8412, 4275599). Los Angeles: University of California, Ernest O. Lawrence Radiation Laboratory. [Google Scholar] [CrossRef]
- World Nuclear Association. 2023. Nuclear Power in the World Today. Information Library, Current and Future Generation. Available online: https://world-nuclear.org/information-library/current-and-future-generation/nuclear-power-in-the-world-today.aspx (accessed on 12 December 2023).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Concept | Definition |
|---|---|
| Access to Care | “Access to routine and critical health care is also an important factor to maintaining health and well-being.” (Community Commons n.d.a) |
| Amelioration or Cure | Health care providers diagnose and treat injuries and disease to ease symptoms and, where possible, cure conditions (Gostin 2007). |
| Anthropocene and Environmental Shifts (Agent, Host, Environment) | Epidemiologic principles of an external agent, a susceptible host, and a physical and social environment that brings the host and agent or vector together (Institute of Medicine 2003). |
| Basic Health Needs | “Physical and mental well-being starts with access to fresh air and water, nutritious food, and the security of a stable home. People also need healthy relationships-with freedom to express gender and sexuality-and a life free from violence, injury, and toxic stress.” (Community Commons n.d.a) |
| Community and Local Priorities | Communities must be included during all phases for their input in planning, implementing, and evaluating disaster research and other activities. |
| Crisis (Response) | The response phase when the goal is amelioration or cure (Lavin et al. 2012) of the human, animals, and the environment, requiring critical decision making. |
| Effective System Coordination | Effective system coordination requires community-based disaster response capabilities and communication infrastructure. Coordination should include capacity for coordination in extenuating and changing circumstances and unknown factors should be considered, planned for, and anticipated. |
| Flexibility and Speed | Persons adversely impacted by a disaster need immediate access to resources, even if they have lost their documentation. Previous eligibility should continue without interruption, and new eligibility should be established quickly. Hence, the federal government should endeavor to provide states and local governments with as much latitude as possible in delivering benefits equitably (Lavin and Menifee 2009). |
| Legal and Ethical Crisis Decision Making | The legal environment may change during a disaster, and the declaration of an emergency may trigger special powers to facilitate the response through increased flexibility, limiting liability, changes in interstate healthcare licensure requirements, and changes in standards of care (Hodge et al. 2009; Institute of Medicine 2009). Ethical decision-making in disaster often involves adhering to core principles, such as humanity, impartiality, neutrality, and independence (Cuthbertson and Penney 2023). These principles provide a framework to guide actions and decisions, ensuring they are ethically sound and align with professional standards and humanitarian values. Incorporating such principles into ethical decision-making helps ensure actions are morally sound and align with core values. |
| Postcrisis (Resilience and Recovery) | The recovery phase is when the goal is rehabilitation, maintenance of an optimal level of well-being, and support for the community and its environment (Lavin et al. 2012). Lessons learned are key to improving education, practice, and planning. |
| Precrisis (Preparedness) | The preparedness phase prior to a disaster or event is a time to gather evidence and engage the community about priorities, communicate with the systems and structures, and identify influencing factors and evidence. The goal of this period is health promotion, disease prevention, and mitigation (Lavin et al. 2012). |
| Rapid and Rational Decision Making | Rational decision-making involves a rigorous process that relies on objective information and logical reasoning. This includes determining the issue at hand, collecting relevant data, exploring choices and potential outcomes, carefully analyzing options, examining interconnections, and, finally, selecting from among feasible options (Adam et al. 2022). |
| Responder Health and Safety | It is critical to protect the health and safety of disaster responders. A healthy and safe workforce is better able to help communities in response and recovery. |
| Self-Determination | Individuals and families impacted by a disaster have the same rights and responsibilities as everybody else. Government aid to persons adversely impacted by a disaster should therefore seek to support the self-determination of persons adversely impacted by a disaster, as they seek access to public benefits and consider relocation opportunities. Individuals and families focusing on their own needs, resources, and interests are more likely to achieve favorable results for themselves and for the broader society than when government restricts or directs their choices (Lavin and Menifee 2009). |
| Self-Sufficiency | The object of disaster case management assistance, including efforts targeted toward persons adversely impacted by a disaster and persons with pre-disaster vulnerabilities, should be individual and family self-sufficiency. As we seek to provide every necessary benefit to help persons adversely impacted by a disaster recover from the disaster and restart their lives, the measure of our success should not be the number of new entrants into disaster assistance systems or dollars expended. Success should be measured by how quickly and successfully persons adversely impacted by a disaster and persons with pre-disaster vulnerabilities are able to become economically self-sufficient and socially integrated. These new lives may be established either in the homes and communities they occupied before the disaster or in new locations selected based on the individual’s or family’s best judgment of where their goals and aspirations may best be fulfilled (Lavin and Menifee 2009). |
| Systems and Structures for Health | This includes both the systems and structures for routine and emergency healthcare, mental health, and community-based and public health care. It also comprises the systems used to provide immediate care during a disaster and recovery. |
| Transdisciplinary Communication and Collaboration in Assessment, Planning, Implementation, and Evaluation | Building systems of communication that allow for interdisciplinary collaboration and leadership models, centered on developing relationships before tasks, and including diverse insights, perspectives, values and priorities to more comprehensively understand and respond to unfolding environmental disasters should be prioritized. |
| Transformative Education | Health professions education, just-in-time training, environmental health, climate change, and health and the Planetary Health Education Framework are used to inform disaster preparedness education and improve health professionals’ action competence in disaster preparedness, response, systems thinking, and health equity. |
| NM Leading Causes of Death, 2017 | Deaths | Rate *** | State Rank * | U.S. Rate ** |
|---|---|---|---|---|
| 1. Heart Disease | 3896 | 151.4 | 32nd | 165.0 |
| 2. Cancer | 3620 | 138.3 | 44th | 152.5 |
| 3. Accidents | 1460 | 68.2 | 5th | 49.4 |
| 4. Chronic Lower Respiratory Disease | 1143 | 44.2 | 26th | 40.9 |
| 5. Stroke | 878 | 34.7 | 37th | 37.6 |
| 6. Diabetes | 673 | 26.5 | 7th | 21.5 |
| 7. Chronic Liver Disease/Cirrhosis | 605 | 26.8 | 1st | 10.9 |
| 8. Alzheimer’s disease | 572 | 22.7 | 32nd | 31.0 |
| 9. Suicide | 491 | 23.3 | 4th | 14.0 |
| 10. Flu/Pneumonia | 338 | 13.6 | 32nd | 14.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Couig, M.P.; Lavin, R.; Rogers, H.H.; Nugent, S.B. The Public Health Crisis Conceptual Model: Historical Application to the World’s First Nuclear Bomb Test. Soc. Sci. 2024, 13, 186. https://doi.org/10.3390/socsci13040186
Couig MP, Lavin R, Rogers HH, Nugent SB. The Public Health Crisis Conceptual Model: Historical Application to the World’s First Nuclear Bomb Test. Social Sciences. 2024; 13(4):186. https://doi.org/10.3390/socsci13040186
Chicago/Turabian StyleCouig, Mary Pat, Roberta Lavin, Heidi Honegger Rogers, and Sara Bandish Nugent. 2024. "The Public Health Crisis Conceptual Model: Historical Application to the World’s First Nuclear Bomb Test" Social Sciences 13, no. 4: 186. https://doi.org/10.3390/socsci13040186
APA StyleCouig, M. P., Lavin, R., Rogers, H. H., & Nugent, S. B. (2024). The Public Health Crisis Conceptual Model: Historical Application to the World’s First Nuclear Bomb Test. Social Sciences, 13(4), 186. https://doi.org/10.3390/socsci13040186