Abstract
In Germany, 1.7 million individuals received reduced earning capacity pensions in 2020, but reintegrating them into the labor market remains challenging. For individuals who have a reduced earning capacity, this often leads to adverse consequences (e.g., low quality of life, poverty, social stigma). The project ‘Cooperation for prevention, fitness and health in the job center (KOPF22)’ focuses on early risk detection and prevention strategies for clients of the job center (who are recipients of Citizen’s Income) as they face various challenges in maintaining their ability to work. The padaCura App, a key component of the project, assesses the risk of reduced earning capacity using an ICF-based questionnaire. It offers immediate feedback reports to clients, categorizing their risk levels and suggesting actions in plain language with visual aids. Since the project emphasizes the client’s autonomy and voluntary participation, clients decide how to proceed with their results. If they decide to cooperate with the job center, then several offers for prevention and intervention measures can be used to increase employability. The first evaluations of the app and the questionnaire demonstrate its effectiveness in differentiating between employable persons and incapacitated individuals. Future developments should focus on enhancing the result reports to include more targeted interventions and on collaboration between employment support resources and healthcare systems to meet clients’ needs.
1. Introduction
The pension statistics of the Federal Ministry of Labour and Social Affairs (2021) in Germany revealed that in 2020, more than 1.7 million individuals received disability pensions due to reduced earning capacity. The reduced earning capacity pension provides a substitute income when individuals lose their earning capacity before reaching the regular retirement age. Individuals capable of working between three and six hours per day are entitled to a partial capacity pension, while those who can only work less than three hours per day receive a full reduced earning capacity pension (Becker et al. 2023).
In the field of vocational rehabilitation, extensive efforts have been undertaken to reintegrate individuals with reduced earning capacity into the labor market. However, empirical evidence reveals that the number of individuals who successfully return to work remains remarkably low (Köckerling et al. 2020; Zschucke and Lippke 2017).
For those affected, reduced earning capacity is often associated with a range of adverse consequences. Individuals with low work capacity report lower quality of life, more depressive symptoms, sleeping disorders, anxiety, and difficulties in meeting everyday demands in household, family, and leisure activities (Törnroos et al. 2017; Norström et al. 2019). Current research also indicates a link between reduced earning capacity and risky health behaviors, such as smoking and excessive alcohol consumption (Böckerman et al. 2018). Furthermore, they also face the social stigma of unemployment, regardless of whether it is attributable to reduced earning capacity or other reasons (Huikari and Korhonen 2015).
This underscores the necessity and importance of developing prevention strategies to avoid work disability and reduced earning capacity and to enable early risk detection (Becker et al. 2023).
2. Project Aim and Scope
Considering the abovementioned requirements for prevention and intervention approaches for preserving and restoring earning capacity, the project ‘Cooperation for prevention, fitness and health in the job center (KOPF22)’ was initiated by three job centers in Germany and is one of 101 funded projects in the federal program ‘rehapro’, which aims to preserve and restore earning capacity and to address threatened or existing earning capacity (Federal Ministry of Labour and Social Affairs 2018). These initiatives reaffirm the principles of the German social system of ‘prevention before rehabilitation’ and ‘rehabilitation before reduced earning capacity pension’.
The target group comprises individuals with anticipated or emerging rehabilitation needs, including those with psychological impairments, addiction disorders, and complex healthcare support requirements. The participants in the project align with the client base of the job centers under the legal principles of the German Social Code II (SGB II), also known as recipients of ‘Bürgergeld’ (Citizen’s Income).
Job centers are responsible for securing the financial livelihood of generally employable individuals who are actually not capable of working independently and guiding them (back) into the labor market. It is challenging to define a specific target group of job center clients due to the individualized nature of the reasons for receiving ‘Bürgergeld’ and the diverse backgrounds of recipients. The work of job centers reveals that unacknowledged health constraints can not only precipitate unemployment but also emerge as a consequence of unemployment. These interactions may contribute to both the perpetuation of unemployment (resulting in long-term unemployment) and a simultaneous deterioration of health (Hollederer 2002). When working with a client, it is pertinent to prevent the entrenchment of the described situations. However, discussing health issues with clients of the job centers remains difficult due to legal and cultural constraints.
The initial step in a needs-oriented consultation for clients of job centers must be a valid assessment of their risk of reduced earning capacity. For this purpose, a questionnaire was developed to assess the individual risk based on a cumulative score. The result can also be utilized to forecast how the risk will evolve if no action is taken. The questionnaire is administered in the padaCura App, whose content and development will be the central issue of this project report. The padaCura App was developed by three job centers in Germany ((1) Pro Arbeit-Kreis Offenbach-Kommunales Jobcenter, (2) Main Arbeit-Kommunales Jobcenter Offenbach am Main, (3) Main-Taunus-Kreis-Kommunales Jobcenter.) and the ‘Jobnet.AG’. The acronym ‘pada’ stands for ‘pass auf dich auf’ in German, which translates to ‘take care of yourself’, while ‘Cura’ is derived from Latin and means ‘care’. Interested clients can access it through their consultant in the job center. Clients who complete the questionnaire initially receive electronic feedback in the padaCura App regarding the potential risk of losing their earning capacity. Subsequently, clients independently decide how to use the feedback and what actions to take. They can either utilize their results for their own benefit or communicate them to the job center to receive further information and assistance, especially when there is a risk of reduced earning capacity.
If the client submits the feedback report to the job center, then the results and identified level of risk can be the foundation for receiving additional counseling services. To achieve this, a strategy is developed within the framework of project KOPF22. Since the reduction in earning capacity is significantly influenced by health factors, it is crucial to establish appropriate connections with the health care system and specialists to provide timely access to medical diagnostics, especially for individuals who are not well connected to the health care system. Recognizing that this cannot and should not fall within the responsibilities of the job centers, an expert panel is installed to offer low-threshold access to diagnostics and address health and other issues that are beyond the primary scope of the job centers. Additionally, support opportunities are also sought within the job centers’ measures. KOPF22 provides a framework for adapting existing measures to the needs of the target group or, if necessary, developing new measures.
The main objective pursued within the project KOPF22 is to detect whether individuals are at risk of losing their employability. Clients face several obstacles that not only currently hinder their access to the job market but also impact their overall health condition to the extent that reintegration into the job market may become impossible even in the long term. Recognizing this problem, the need for a holistic approach that goes beyond merely prescribing health and illness and considers various factors influencing individual employability has been acknowledged and discussed in participating job centers. Consequently, the International Classification of Functioning, Disability, and Health (ICF) and the corresponding bio-psycho-social model (WHO 2001) were identified as useful frameworks for the development of the questionnaire and the subsequent consulting process and measures in the job center.
3. Development of the padaCura App
In this section, an overview of the conceptual background, questionnaire and app development, current empirical studies, feedback reports, and consulting process is provided.
3.1. Conceptual Background: ICF and Bio-Psycho-Social Model
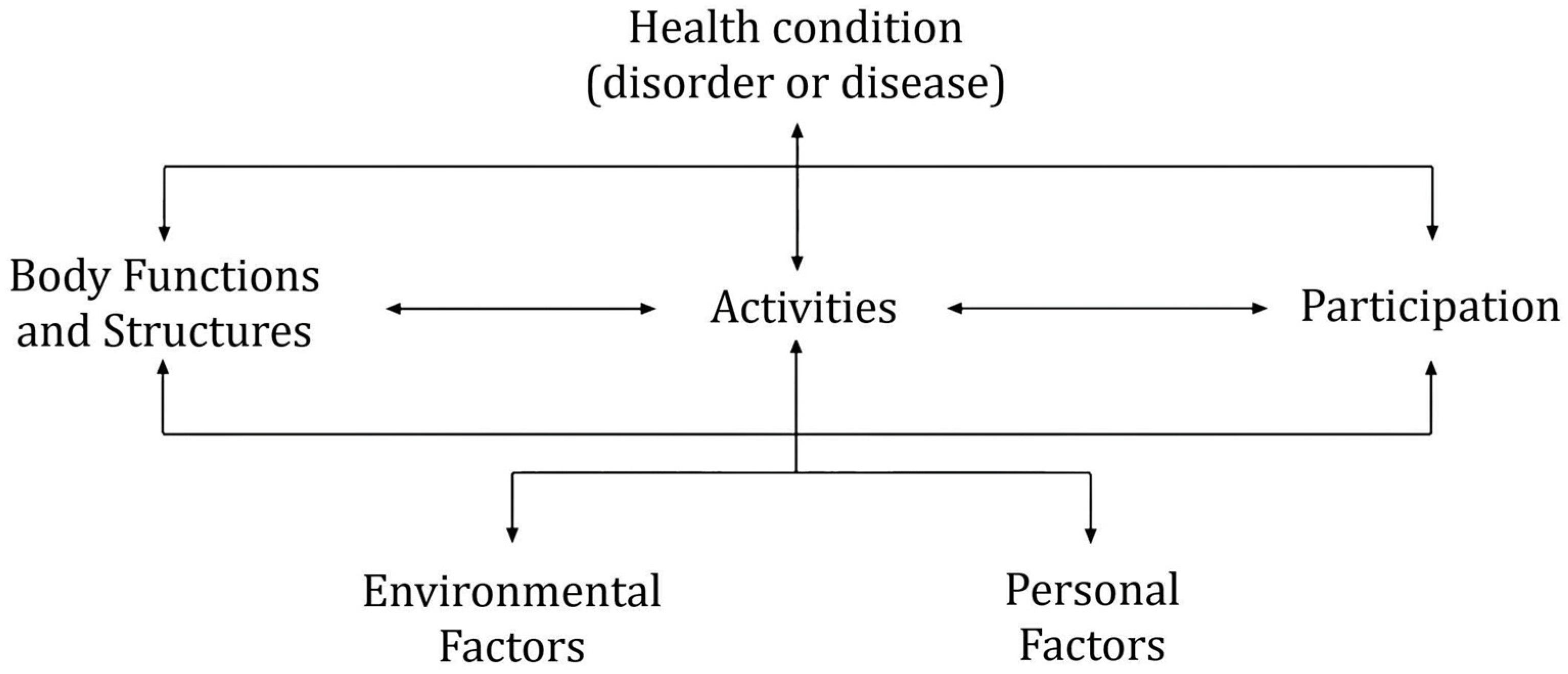
In the development of the padaCura App and questionnaire, the ICF and the bio-psycho-social model of the World Health Organization (WHO 2001) offer an approach that can comprehensively represent the holistic living conditions of clients. While the International Classification of Diseases (ICD) primarily focusses on diseases, diagnoses, and diagnostic criteria, the ICF emphasizes gaining a thorough understanding of health and functioning and delving deeper into the origins and consequences of health conditions. An important question that can be addressed using ICF and the bio-psycho-social model is as follows: To what extent does an individual’s health condition result in limitations or difficulties in participating in one or more aspects of life (e.g., work, sports, or leisure activities)? These participation issues are outcomes of a complex interplay among various factors. These factors and their interactions are represented in the bio-psycho-social model of the ICF (Figure 1).
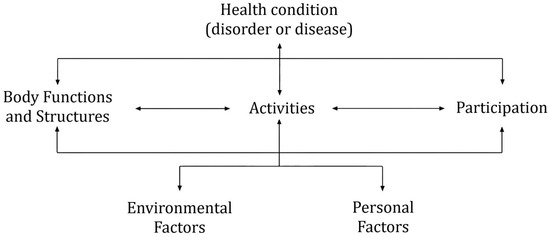
Figure 1.
The bio-psycho-social model of the WHO (2001).
As a result, work participation can be hindered by a variety of factors. One potential factor is the individual’s health condition itself, which is closely linked to body functions and structures. Body functions refer to physiological and mental functions of the body, while body structures describe the anatomical parts of the body. For instance, a body function could encompass the range and ease of movement of a specific joint, while the body structure would be the joint itself. Typically, every health condition or disease is accompanied by impairments in body functions or structures. Consequently, health conditions and/or impaired body functions and structures can lead to difficulties in performing job-related activities. If this results in job loss or the inability to secure employment, the individual’s work participation becomes restricted. Work participation can also be influenced by various contextual factors such as environmental and personal factors. Environmental factors “encompass the physical, social, and attitudinal environment in which people live and conduct their lives” (WHO 2001, p. 16). These factors can act as either barriers or facilitators. For example, the social environment can positively influence an individual’s job-seeking activities by proofreading application letters or researching job offers. Conversely, the physical environment may act as a barrier in terms of job availability, particularly in rural areas. Personal factors refer to intrinsic characteristics of an individual that may interact with other components of the bio-psycho-social model. They “encompass features that are not directly related to the health condition and address factors that influence an individual’s functioning on a case-by-case basis” (Grotkamp et al. 2020, p. 3). Examples include motivation to work, attitudes toward receiving government benefits, and overall life satisfaction.
The interplay of factors within the bio-psycho-social model can involve primary and secondary processes (Schuntermann 2005). Primary processes originate from an existing health condition, which can impact participation in one or more aspects of life (e.g., work). This occurs through the influence of various factors, including impaired body functions and structures, limitations in performing important activities, and contextual factors serving as facilitators or barriers. Secondary processes describe reverse effects in which, for instance, the lack of work participation can also affect the progression and exacerbation of the health condition and the development of comorbidities. An example of this could be an individual who can no longer work due to a musculoskeletal disease and may develop depressive symptoms as a result of the lack of work participation. Gedikli et al. (2022, p. 128) describe this interaction as the “cycle of unemployment and poor wellbeing”.
3.2. Designing the Questionnaire
The fundamental questions that the padaCura questionnaire aims to assist with are as follows:
- To what extent is an individual capable of participating in a significant life domain, such as work, that is meaningful to them?
- To what extent are they able to perform the relevant activities associated with this domain, or in which necessary activities are they impaired?
- What is the potential risk of occupational disability, and what is the corresponding need for interventions?
The variables considered for the determination of the padaCura Score were identified through a multistage process. This process initially involved a systematic literature review about relevant factors influencing the risk of work disability. Publications were included according to the following criteria: (1) the study was conducted in Germany; (2) the study addressed the issue of reduced earning capacity; and (3) the publication presented empirical findings. In total, 80 relevant publications were identified through the REHADAT database and reviewed regarding relevant influencing factors on reduced earning capacity. These publications primarily comprised a reduced number of factors that influence the risk of reduced earning capacity, e.g., health condition, utilization of health services, and motivation to return to work (Briest 2020); a selection of sociodemographic factors (Hagen and Himmelreicher 2014); various health conditions (Roski et al. 2017); or an examination of data from the German pension insurance system, which includes, for example, the duration of sickness benefits, receipt of benefits for participation in working life, gender, income, and level of education (Bethge et al. 2011). Further publications address the effectiveness of medical and vocational rehabilitation programs (Dannenmaier et al. 2020).
Additionally, a review of existing questionnaires used in the field of vocational rehabilitation was conducted—including the Work Ability Index (Ebener and Hasselhorn 2019), the Work Rehabilitation Questionnaire (Finger et al. 2019), and the WHO Disability Assessment Schedule (Üstün et al. 2010). Furthermore, existing ICF Core Sets were considered. An ICF Core Set “provides a selection of essential categories from the full ICF classification that are considered most relevant for describing the functioning of a person with a specific health condition or in a specific health care context” (Selb et al. 2015, p. 106). Due to their relation to the field of work disability, the ICF Core Set for Vocational Rehabilitation (Finger et al. 2012) and the Core Set for Disability Evaluation in Social Security (Brage et al. 2008) were considered.
The padaCura questionnaire was designed to examine the interplay of these aspects of employability. In total, 38 relevant factors were derived from the reviewed instruments and publications and mapped to the ICF.
The questionnaire consists of five areas: (1) sociodemographic data, (2) activities (physical, mental/psychological, health), (3) employability, (4) environmental factors, and (5) personal factors (see Table 1). Since job centers do not have the authority to ask clients questions about existing diagnoses and diseases, the corresponding elements of the bio-psycho-social model (health condition, body functions, body structures) are not represented in the questionnaire. Consequently, limitations are captured through questions about activities and employability. Currently, the questionnaire includes 56 items.

Table 1.
The five areas of the padaCura questionnaire with exemplary topics.
3.3. Empirical Evaluation of the padaCura Questionnaire
The padaCura questionnaire and the underlying algorithm with which the padaCura Score is calculated are constantly evolving. This means that the psychometric properties, the correlations between various influencing factors on reduced earning capacity, and the outcome (placement in work versus reduced earning capacity pension) are regularly evaluated and adjusted through continuous questionnaire application and the acquisition of new data. However, in the beginning, to make the questionnaire applicable and assess its predictive value, a retrospective survey was conducted with N = 416. All participants were former clients of job centers and could be assigned to one of two subsamples. Convenience sampling was used, and participants were recruited by the research survey panel ‘survey engine’. This procedure was necessary because neither individuals with reduced earning capacity nor employed individuals are clients of the job center. Consequently, the job centers are not allowed to use their data for research, and it would have been difficult to obtain informed consent. Due to the process of recruiting and the voluntary nature of participation, we were not able to collect a randomized sample. However, to compensate for this and improve representativity, we deliberately chose a broad sample (in terms of sex, age, educational background, and different health conditions). Subsample 1 consisted of n = 210 individuals who were already receiving the reduced earning capacity pension at the time of the survey (59.5% female, 41.5% male; age: M = 42.4, SD = 5.3). Subsample 2 comprised n = 206 participants who were employed at the time of the survey (49.5% female, 51.5% male; age: M = 37.4, SD = 5.5). Their educational background ranged from ‘no educational degree’ to ‘Abitur/A-Level’. Furthermore, the health background of the sample was surveyed (see Table 2).
Table 2.
Description of the two subsamples regarding their health condition.
The two subsamples were compared and analyzed using binary logistic regression and receiver operating characteristics (ROC) analyses. The results of the Omnibus Test show a significant model (Chi-Quadrat(1) = 64.73, p < 0.001, N = 416). In total, 70.4% of the participants were classified correctly with respect to the subsample to which they belonged (subsample 1 = reduced earning capacity, subsample 2 = employed). The corresponding effect size of f2 = 0.25 can be seen as moderate. The ROC analysis showed an area under the curve (AOC) of 0.85, which confirms that the padaCura questionnaire can effectively differentiate between individuals who are employable and those with reduced earning capacity. The coordinates of the curve, under consideration of sensitivity and specificity, were also used to establish cutoff points for four risk levels of reduced earning capacity (likelihood of reduced earning capacity: 0–19%, 20–49%, 50–79%, and 80–100%), which were applied for electronic feedback for the clients (see Section 3.5). For better comprehensibility, the padaCura score, with a maximum of 132, is converted into a value from 0 to 100.
Furthermore, a study was conducted to examine the usability of the app and the questionnaire within the participating job centers. The evaluation of the app focused primarily on its intuitiveness (see Section 3.4). The evaluation of the questionnaire, in which N = 122 job center clients participated, addressed the following questions: (1) Are the items of the questionnaire easy to understand? (2) Are the questions formulated in a way that clients do not feel that their privacy is violated when answering them? (3) Do clients consider the items relevant to determine the risk of reduced earning capacity? Items were included in the questionnaire if a majority of the participants found them understandable, appropriate, and important. Items that did not meet these criteria were either significantly revised or removed from the questionnaire.
3.4. Designing the Framework and Process If Using the padaCura App
The padaCura questionnaire, which is provided in the padaCura App, is intended to be as straightforward as possible to allow the clients of the job center to complete it without prior consultation. Clients can answer the questionnaire on a computer using a common web browser or on their mobile devices (smartphone, tablet). For this purpose, the padaCura App is available for download in the Apple App Store and Google Play Store and is designed to be intuitively usable.
The questions and answer options in the questionnaire were formulated in plain language. The explanatory texts and information on data protection were also kept as simple as possible while respecting the legal framework. To facilitate the handling of the app for clients whose native language is not German, the whole app is usable in 15 different languages. During the development of the app, all relevant data protection aspects were considered, which are very strict in Germany, especially for health-related data.
All information about the padaCura App, the general condition for its use, and access data for the initial login are sent by the job centers to their clients in two letters. This is necessary because the username and password may not be sent together for data protection reasons. If a client decides to use the padaCura App, it can be accessed or downloaded on their device of choice. After selecting the language and the login, it is mandatory to agree to the data protection policy. This is followed by a request to change the password, which is necessary because the data for the initial login were provided by the job center and a new password prevents any third-party use of the access.
The next step is to start answering the questions. Until the survey is finished, it is possible to logout and login again. The survey can then be continued from the point at which the user previously logged out. Furthermore, it is possible to return up to five questions to adjust answers if necessary. Thus far, experience has shown that the questionnaire takes approximately 15–20 min to complete.
After answering the last question, the client receives immediate feedback, which describes their individual risk of reduced earning capacity with respect to the padaCura Score and gives a recommendation for action. In the app, clients can actively make their decision on whether they want to share their result with their consultant at the job center. This decision can also be withdrawn. If the client decides to share the feedback, then the data are immediately visible for the job center in the consultant screen of the browser-based padaCura system. These data can be initially used by the consultants to prepare the next consultation with their clients to discuss the next steps and appropriate measures. However, at no point in the process are the client’s answers to the specific questions transmitted. The answers to the questions are not saved in the app or in the system after the result is ascertained. At any time, the details of the answers are only visible for the clients.
3.5. Designing the Feedback Report
Based on the padaCura Score, clients receive immediate and automatic feedback indicating their degree of risk for reduced earning capacity, along with recommendations on how to proceed.
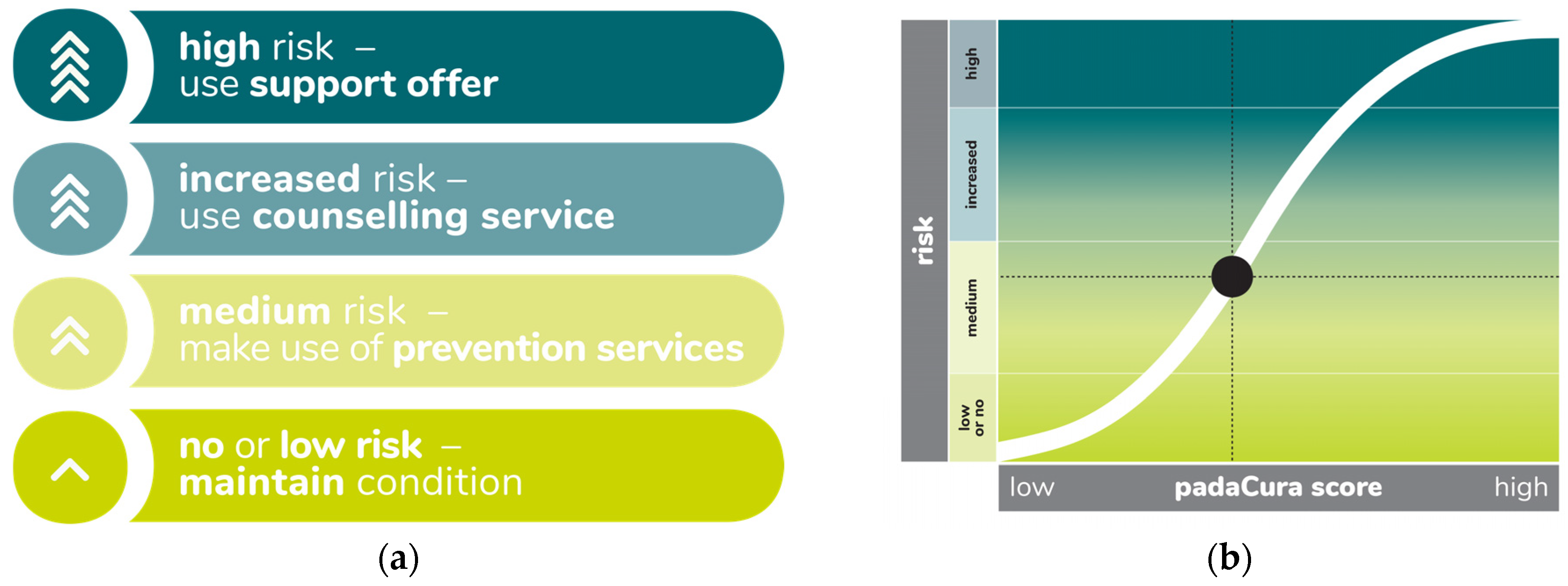
The feedback represents the risk of reduced earning capacity at four levels: (1) no or low risk—maintain condition, (2) medium risk—make use of prevention services, (3) increased risk—use counseling service, and (4) high risk—use support offer. For example, when explaining a medium risk result, the feedback would be as follows: ‘Your score indicates a medium risk of becoming incapacitated for work. You currently feel a medium degree of impairment. The questionnaire identified initial fields of concern that we can work on together. It is good to talk about what we can do together to maintain your employability and to find solutions to existing challenges’.
In designing the feedback report, particular emphasis was placed on formulating the results in plain language and highlighting the need for action. This approach is strengthened by graphic design, where the urgency of becoming active is emphasized by the number of arrows and by the gradient from lighter green to darker blue colors (see Figure 2). Although using traffic light colors (red, yellow, green) may seem intuitive at first glance, but we decided against it for several reasons. First, the goal was to visualize the risk of reduced earning capacity at four levels, which does not align with the three traffic light colors. Second, the red color can signify ‘stop, do not proceed’. However, the padaCura App and the feedback aim to encourage clients to take an active role in managing their health and employability. Last, we decided in favor of color gradients and against clear contrasted areas as we wanted to suggest to the participants that developments and transitions between different risk levels are positive. Furthermore, such a visualization can also be more realistic from a scientific point of view with respect to statistical error probabilities and confidence intervals. Additionally, participants receive a chart illustrating the correlation between the risk level of reduced earning capacity and their specific padaCura Score. The purpose of this chart is to assist participants in comprehending their individual results within the entire potential range of the padaCura Score (see Figure 2).
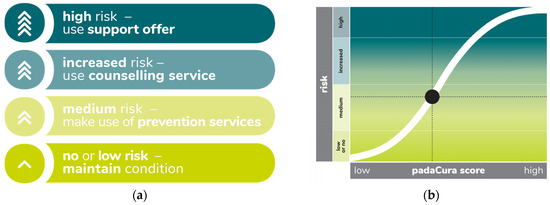
Figure 2.
(a) Graphic presentation of the feedback at different risk levels. (b) Feedback about the correlation between the risk level of reduced earning capacity and the specific padaCura Score.
3.6. Consequences for the Consulting Process
The feedback is intended to strengthen the client’s awareness of their own health and employability, regardless of whether a client decides to use the support service offered by the job center. In this way, clients should be encouraged to engage in the placement process in a self-determined and self-responsible manner. This aligns with a broader shift in working with the target group of the SGB II in Germany, where extensive reforms are ongoing (e.g., Citizen’s Income). Within the job centers, the premise is that the entire process, starting from the decision to complete the questionnaire to the transmission of the electronic feedback, is initiated by the clients and requires their active consent. If a client decides to share the result with the job center and a need for action occurs, then it is essential for the job center to ensure that immediate measures and support can be provided to address the client’s needs promptly. For the consultation that follows the transmission of the padaCura Score, a consultation guideline has been developed. This guideline is based on the Motivational Interviewing Approach (Rollnick and Miller 1995; Unger and Sann 2023) and provides guidance for the beginning of the conversation, the discussion of the results, the identification of specific limitations, and potential focal points for further measures and interventions.
4. Outlook
Project KOPF22 has a contract period until December 2024. For the remaining time, but also beyond that, various issues will arise about the further development of the padaCura App, as well as the questionnaire and feedback. From the practical perspective, the bilateral work with the result on the part of client and consultant will also result in further developments. A third focus will be on the precise allocation to existing and newly developed measures of the job center and further collaborating institutions from the fields of medicine, physiotherapy, and social work.
4.1. Further Development and Differentiation of the padaCura Score
The result of the padaCura App is intended to provide a starting point for discussions about specific impairments and limitations in important activities. However, since counselors do not have access to the specific answers provided by clients in the questionnaire, they must rely on the feedback from their clients, who often struggle to recall the issues they found challenging. To address this limitation, we plan to provide more differentiated feedback that can serve as a guideline for both clients and consultants during the consultation process. This enhanced result report will cover four key areas where the need for prevention or intervention can arise: (1) health competencies, (2) physical fitness, (3) mental and psychological fitness, and (4) environmental factors. Clients will receive the following explanations for each of these four key areas:
- ‘Health Competencies’: To maintain your employability, it is important to take sufficient care of your health. This applies to maintaining a healthy lifestyle and getting proper nutrition, exercise, and recovery. In addition, it involves preventive medical care and adhering to medical prescriptions (e.g., taking medication regularly).
- ‘Physical fitness’ indicates how well you feel able to cope with physical requirements that arise in an occupational activity. This can be certain movements (motoric) or can also concern the ability to withstand exertion over a longer period.
- ‘Mental and Psychological Fitness’ indicates how well you can cope with mental demands in the workplace. This includes concentrating under difficult conditions, learning new content, and dealing with situations that cause stress or anger.
- Environmental Factors are also important to consider in light of the bio-psycho-social model. ‘Environmental Factors’ describe the extent to which your general living circumstances, such as living, shopping, visiting public offices, or sufficient support from your social environment, allow you to lead a good life, or whether you feel restricted by them.
The scores in the respective fields will also be categorized into four risk levels, in alignment with the general padaCura Score. This differentiation into four key areas and the corresponding four risk levels enables the establishment of specific focal points for interventions and support measures.
4.2. Practical Implications for the Use of the padaCura App
In their current and future activities within the project network KOPF22, the participating job centers are placing particular emphasis on how to effectively utilize the results obtained from the padaCura App. Recognizing a risk of reduced earning capacity does not automatically provide information about which factors need to be addressed as part of support interventions. By collaborating with job center consultants, clients can specifically identify which activities are affected and where their support needs lie. However, a holistic view of the individual, in line with the bio-psycho-social model, also encompasses the assessment of the individual’s health condition from a medical perspective—a task beyond the capacity of the job center. Sustainable and comprehensive counseling for job center clients, therefore, necessitates collaboration between the employment support and healthcare systems, a synergy being advanced in KOPF22 project.
When individual needs cannot be fully met with existing job center measures, measures from collaborating partners can be applied, and, if needed, new support instruments can be developed. These expanded counseling processes aim to not only improve the assessment and servicing of individual needs but also address another phenomenon frequently observed in daily practical work. In the assignment of clients to job center measures, it is often retrospectively noted that the resilience and performance capacity of individuals are frequently overestimated. This phenomenon is particularly evident in prevention measures, where it is subsequently discovered that clients are significantly more limited than initially indicated during the counseling process. In this context, the approach of conducting a risk assessment at the beginning of the counseling process seeks to address this issue.
4.3. Implications for Further Research
The present study used a retrospective survey of N = 416 former clients of job centers to examine whether the padaCura questionnaire is able to differentiate between employed individuals and persons who receive a reduced earning capacity pension. From this it was derived that the padaCura questionnaire is able to predict the risk of reduced earning capacity among current clients of the job centers. This leads to some limitations with respect to our sample and its representativity, as the validity of our results can currently only be assumed for the sample described. To further evaluate the prognostic validity of the questionnaire, a long-term follow-up of a sample of job center clients is needed to be able to map the real outcome with the prediction of reduced earning capacity by our questionnaire. Further longitudinal studies are also necessary and relevant to map the external validity of our results in other contexts. Other possible frameworks of using the padaCura questionnaire could be in the context of occupational reintegration, returning to work after a temporary reduced earning capacity pension, or before vocational rehabilitation measures.
5. Conclusions
The development of the padaCura App represents a significant and effective tool for assessing the risk of reduced earning capacity among job center clients. Within the framework of the KOPF22 project, the padaCura questionnaire, which is incorporated into the app, serves as the crucial initial step toward a standardized assessment of limitations in work participation. By aligning with the bio-psycho-social model of the WHO (2001) and the diverse existing and evolving possibilities for providing result reports and feedback to clients, it enables a holistic perspective on individuals and their life conditions. This perspective can be addressed during consultations in job centers. In this context, specifically created materials, such as the feedback report for clients and the consultation guideline, facilitate the counseling process. The support needs that are identified during the consultation can be met through existing measures of the job center; through measures offered by collaborating partners in the fields of medicine, physiotherapy, and social work; or by newly designed interventions.
Throughout the development of the padaCura App, the voluntary nature of client participation was ensured at every step. This commitment to voluntary participation remains a top priority in all future developments, especially in processes involving collaboration between employment support and healthcare systems. At each phase of the project, clients have the autonomy to decide whether to participate or continue their involvement. Building on the concept of informed citizenship, individuals who recognize potential risks but choose not to seek additional support from the job center can independently assess their needs, prospects, and available options to mitigate their risks and initiate relevant measures.
Author Contributions
Conceptualization, A.G.-B., R.W. and C.M.B.; methodology, R.W. and F.L.C.L.; software, C.M.B.; validation, F.L.C.L. and R.W.; formal analysis, A.G.-B., investigation, R.W. and F.L.C.L., resources, A.G.-B. and C.M.B.; data curation, F.L.C.L.; writing—original draft preparation, R.W., C.M.B. and A.G.-B.; writing—review and editing, R.W. and F.L.C.L.; visualization, C.M.B. and R.W.; supervision, A.G.-B. and F.L.C.L., project administration, A.G.-B., C.M.B. and R.W.; funding acquisition, A.G.-B. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the German federal program ‘rehapro’ (grant number: 661Z0812K1).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. Ethical review and approval where waived for this study as in our study no risk of harm to the participants can be assumed due to the following reasons: (1) it ist not an intervention study, (2) it is a non-clinical sample, (3)The data presented is a retrospective survey, (4) The questionnaire and the app have also been approved by the data protection officers of the participating job center.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on reasonable request from the corresponding author. The data are not publicly available due to reasons of data privacy.
Acknowledgments
The authors would like to thank all members of the KOPF22 project network, as well as the Jobnet.AG team who were involved in the development of the padaCura app.
Conflicts of Interest
Corinna Manuela Busacker is employee of Jobnet.AG, which has developed and currently provides the padaCura App. All other authors have no conflict of interest to declare.
Correction Statement
This article has been republished with a minor correction to resolve spelling and grammatical errors. This change does not affect the scientific content of the article.
References
- Becker, Sebastian, Annica Gehlen, Johannes Geyer, and Peter Haan. 2023. Reform of reduced earning capacity pension cuts risk of poverty, but comes late. DIW Weekly Report 13: 123–98. [Google Scholar]
- Bethge, Matthias, Uwe Egner, Marco Streibelt, Friedrich M. Radoschewski, and Karla Spyra. 2011. Risikoindex Erwerbsminderungsrente (RI-EMR) [Risk index reduced earning capacity pension (RI-EMR)]. Bundesgesundheitsblatt 54: 1221–28. [Google Scholar] [CrossRef] [PubMed]
- Böckerman, Petri, Ari Hyytinen, Jaakko Kaprio, and Terhi Maczulskij. 2018. If you drink, don’t smoke: Joint associations between risky health behaviors and labor market outcomes. Social Science and Medicine 207: 55–63. [Google Scholar] [CrossRef] [PubMed]
- Brage, Sören, Peter Donceel, and Freddy Falez. 2008. Development of ICF core set for disability evaluation in social security. Disability and Rehabilitation 18: 1392–96. [Google Scholar] [CrossRef] [PubMed]
- Briest, Juliane. 2020. Gesundheitszustand, Inanspruchnahme von Gesundheitsleistungen und Einstellung zur Rückkehr ins Erwerbsleben bei zeitlich befristeten Erwerbsminderungsrentnern [Health condition, health care utilisation and attitude towards return to work in individuals receiving temporary disability pension]. Das Gesundheitswesen 82: 794–800. [Google Scholar] [CrossRef] [PubMed]
- Dannenmaier, Julia, Lena Tepohl, Desiree Immel, Ulrich Hartschuh, Rainer Kaluscha, and Gert Krischak. 2020. Effekt der Rehabilitation auf den verzögerten Eintritt in die Berentung aufgrund von Erwerbsminderung [Effect of rehabilitation on the delayed entry into the retirement due to reduced earning capacity]. Die Rehabilitation 59: 10–16. [Google Scholar] [CrossRef] [PubMed]
- Ebener, Melanie, and Hans Martin Hasselhorn. 2019. Validation of short measures of work ability for research and employee surveys. International Journal of Environmental Research and Public Health 16: 3386. [Google Scholar] [CrossRef] [PubMed]
- Federal Ministry of Labour and Social Affairs. 2018. Bekanntmachung. Förderrichtlinien für das Bundesprogramm “Innovative Wege zur Teilhabe am Arbeitsleben—Rehapro” zur Umsetzung von §1 des Neunten Sozialgesetzbuchs. Available online: https://www.modellvorhaben-rehapro.de/SharedDocs/Downloads/DE/Bundesprogramm_rehapro_Foerderrichtlinie.pdf (accessed on 29 September 2023).
- Federal Ministry of Labour and Social Affairs. 2021. Die Rentenbestände in der gesetzlichen Rentenversicherung in der Bundesrepublik Deutschland. Available online: https://www.bmas.de/SharedDocs/Rentenbestandsstatistik-2020.pdf (accessed on 29 September 2023).
- Finger, Monika E., Reuben Escorpizo, and Alan Tennant. 2019. Measuring work-related functioning using the Work Rehabilitation Questionnaire (WORQ). International Journal of Environmental Research and Public Health 16: 2795. [Google Scholar] [CrossRef]
- Finger, Monika E., Reuben Escorpizo, Andrea Glässel, Hans Peter Gmünder, Miriam Lückenkemper, Chetwyn Chan, Julie Fritz, Urban Studer, Jan Ekholm, Nenad Konstanjsek, and et al. 2012. ICF Core Set for vocational rehabilitation: Results of an international consensus conference. Disability and Rehabilitation 34: 429–38. [Google Scholar] [CrossRef]
- Gedikli, Cigdem, Mariella Miraglia, Sara Connolly, Mark Bryan, and David Watson. 2022. The relationship between unemployment and wellbeing: An updated meta-analysis of longitudinal evidence. European Journal of Work and Organizational Psychology 32: 128–44. [Google Scholar] [CrossRef]
- Grotkamp, Sabine, Wolfgang Cibis, Silke Brüggemann, Michaela Coenen, Hans Peter Gmünder, Klaus Keller, Elisabeth Nüchtern, Urban Schwegler, Wolfgang Seger, Stefan Staubli, and et al. 2020. Personal factors classification revisited: A proposal in the light of the biopsychosocial model of the World Health Organization (WHO). The Australian Journal of Rehabilitation Counselling 26: 73–91. [Google Scholar] [CrossRef]
- Hagen, Christine, and Ralf K. Himmelreicher. 2014. Erwerbsminderungsrente in Deutschland—Ein unterschätztes Risiko (?) [Reduced earning capacity pension in Germany—An underestimated risk (?)]. Vierteljahreshefte zur Wirtschaftsforschung 83: 115–38. [Google Scholar] [CrossRef]
- Hollederer, Alfons. 2002. Arbeitslosigkeit und Gesundheit [Workloss and health]. Mitteilungen aus der Arbeitsmarkt- und Berufsforschung 35: 411–28. [Google Scholar]
- Huikari, Sanna, and Marko Korhonen. 2015. The impact of unemployment on well-being: Evidence from the Regional Level Suicide Data in Finland. Social Indicators Research 128: 1103–19. [Google Scholar] [CrossRef]
- Köckerling, Elena, Odile Sauzet, Bettina Hesse, Michael Körner, and Oliver Razum. 2020. Return to Work aus einer zeitlich befristeten Erwerbsminderungsrente [Return to work after temporary disability pension]. Das Gesundheitswesen 82: 894–900. [Google Scholar] [CrossRef] [PubMed]
- Norström, Frederik, Anna-Karin Waenerlund, Lars Lindholm, Rebecka Nygren, Klas-Göran Sahlen, and Anna Brydsten. 2019. Does unemployment contribute to poorer health-related quality of life among Swedish adults? BMC Public Health 19: 457. [Google Scholar] [CrossRef] [PubMed]
- Rollnick, Stephen, and William M. Miller. 1995. What is Motivational Interviewing? Behavioural and Cognitive Psychotherapy 23: 325–34. [Google Scholar] [CrossRef]
- Roski, Christian, Matthias Romppel, and Gesine Grande. 2017. Risikofaktoren der Erwerbsminderungsberentung aufgrund psychischer Erkrankungen—Eine systematische Übersichtsarbeit [Risk factors for disability pensioning caused by mental disorders—A systematic review]. Das Gesundheitswesen 79: 472–83. [Google Scholar] [CrossRef]
- Schuntermann, Michael. 2005. The implementation of the International Classification of Functioning, Disability and Health in Germany: Experiences and problems. International Journal of Rehabilitation Research 28: 93–102. [Google Scholar] [CrossRef]
- Selb, Melissa, Reuben Escorpizo, Nenad Konstanjsek, Gerold Stucki, Tevfik Bedirhan Ustun, and Alarcos Cieza. 2015. A guide on how to develop an International Classification of Functioning, Disability and Health Core Set. European Journal of Physical and Rehabilitation Medicine 51: 105–17. [Google Scholar]
- Törnroos, Kaisa, Claudia Bernhard-Oettel, and Constanze Leineweber. 2017. Perceived employability trajectories: A Swedish cohort study. Journal of Occupational Health 59: 336–44. [Google Scholar] [CrossRef]
- Unger, Frank, and Uli Sann. 2023. Promoting Self-Determination and Motivation as Leadership Skills: A Didactics to Strengthen Autonomy Support and the Importance of Role Models in Social Work Management Education. In Handbook of Applied Teaching and Learning in Social Work Management Education. Theories, Methods, and Practices in Higher Education. Edited by Maik Arnold. Cham: Springer, pp. 5–16. [Google Scholar] [CrossRef]
- Üstün, T. Bedirhan, Somnath Chatterji, Nenad Konstanjsek, Jürgen Rehm, Cille Kennedy, Joanne Epping-Jordan, Shekhar Saxena, Michael von Korff, and Charles Pull. 2010. Developing the World Health Organization Disability Assessment Schedule 2.0. Bulletin of the World Health Organization 88: 815–23. [Google Scholar] [CrossRef] [PubMed]
- WHO. 2001. ICF: International Classification of Functioning, Disability and Health. Geneva: World Health Organization. [Google Scholar]
- Zschucke, Elisabeth, and Sonia Lippke. 2017. Erwerbsminderungsrente und Rückkehr ins Erwerbsleben aus Sicht der Betroffenen. Diskussionsforum Rehabilitations- und Teilhaberecht Beitrag D15-2017. Available online: https://www.reha-recht.de/fachbeitraege/beitrag/artikel/beitrag-d15-2017/ (accessed on 29 September 2023).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).