Abstract
Most studies about life experiences and their long-term impact have relied on retrospective assessments and cross-sectional designs. However, there are concerns about the inconsistency of reports, which have been addressed in a limited scope. This study aimed to compare differences on inconsistency between positive and negative experiences to describe potential patterns and to identify sociodemographic, experiences-related and design-related predictors of inconsistency. Adults from community (N = 171) reported their life experiences twice, through self-report or interview. An overall trend of overreporting was found for positive and negative experiences. Additionally, inconsistency on positive experiences was higher than on negative although both variables were correlated. Regarding predictors of inconsistency, the model explained greater variance for negative experiences than for the positive ones. Nevertheless, most variables did not predict inconsistency, with few exceptions: impact for positive experiences, total of experiences for negative experiences, and time interval was marginally significant for both. Available data comparing inconsistency on positive and negative experiences as well as associated predictors are incipient. Overall, it seems that we know more about variables not involved in inconsistency than those that matter. Due to its relevancy, this issue should be further examined.
1. Introduction
Since the publication of the Social Readjustment Rating Scale (Holmes and Rahe 1967) in the sixties, retrospective life experience measures have been widely used to collect data for both research and clinical purposes (e.g., Kendall-Tackett and Becker-Blease 2004; Paykel 2001; Shaffer et al. 2008), usually through cross-sectional designs (e.g., Chapman et al. 2004; Sun et al. 2017). Concurrently, many claims arose warning about the lack of consistency in those reports (e.g., Jenkins et al. 1979; Klein and Rubovits 1987; Mesquita and Maia 2018; Zimmerman 1983), which is still a major challenge (Hardt and Rutter 2004). Surprisingly, little attention is given to the topic, which is far from being fully understood. Most studies aimed primarily to quantify inconsistency through descriptive approaches, and findings are quite inconclusive. For instance, when participants from the community were asked twice about childhood sexual abuse experiences, Dube et al. (2004) found substantial agreement, whereas Langeland et al. (2014) found only fair agreement. Therefore, the best current conclusion available is that at least some individuals will provide an inconsistent report. Moreover, reasons involved in inconsistent reporting remained mainly as a secondary or neglect aim (e.g., Casey et al. 1967; Dill et al. 1991; Widom et al. 2004), and this is a relevant gap.
Reasons involved in inconsistent reporting are an emerging line of research, which can be studied through two distinct approaches, namely statistical testing, such as been done by McKinney et al. (2009), or asking participants to identify relevant variables similarly to the study of Sobell et al. (1990). More recently, Langeland et al. (2014) concomitantly applied both approaches. Attending to our purposes, we focused mainly on the first one, which consists of collecting data about life experiences and potential associated variables at least in two distinct moments. Then, an inconsistency parameter was defined and tested against those factors. In a previous work (Azevedo et al. 2021), we grouped associated variables in three sets, namely individual-related (i.e., gender, age, marital status, depression, physical conditions), experience-related (i.e., time of occurrence, specific events, total of exposure), and design variables (i.e., time interval, method of data collection, interviewer’s characteristics). Typically, researchers addressed some variables from just one or two of these sets, especially from sociodemographic and health variables. Additionally, available studies assessed mainly childhood negative experiences (e.g., Colman et al. 2016; Langeland et al. 2014; Shields et al. 2015), and only two studies from community samples included also positive ones (Hardt et al. 2006; Yancura and Aldwin 2009) but analysed inconsistency as a whole. Therefore, current knowledge urges for some novelties, such as a more comprehensive approach of variables underlying inconsistent reports, i.e., through the analysis of more than two sets, a lifespan perspective and a more balanced assessment of positive and negative experiences, introducing comparative purposes.
Setting aside these caveats, some findings from community samples (Ayalon 2015; Colman et al. 2016; Dube et al. 2004; Fergusson et al. 2000; Hepp et al. 2006; Langeland et al. 2014; McKinney et al. 2009; Schraedley et al. 2002; Shields et al. 2015; Yancura and Aldwin 2009) are important to highlight. The majority of the studies analysed at least one sociodemographic variable, including age, gender, education, marital status, ethnicity, and income. However, the profile of inconsistent reporters is not well defined: some studies claimed that men are more inconsistent (e.g., Yancura and Aldwin 2009), whereas others found no impact based on gender (e.g., Dube et al. 2004). Age was not an explanatory variable in most studies, but younger participants are identified simultaneously as consistent (e.g., Shields et al. 2015) and inconsistent reporters (e.g., McKinney et al. 2009). Similar inconclusive results were found regarding other variables except for income, which was not a significant predictor of inconsistency (e.g., McKinney et al. 2009; Shields et al. 2015). Additionally, psychological symptoms and depression are among the most studied factors, but once again, some authors found significant effects (e.g., Ayalon 2015; Schraedley et al. 2002), whereas others did not (e.g., Colman et al. 2016; Fergusson et al. 2000). Besides, other factors, such as cognitive function, stress, mastery, personality characteristics, coping, self-esteem, post-traumatic stress disorder, suicide behaviours, or alcohol related problems, had also been occasionally studied, presenting mixed results. Experience-related variables, including specific experiences, specific answers, severity, and total of experiences, are much less studied, notwithstanding results revealing those are relevant factors involved in inconsistency. Lastly, design-related variables have not been recently addressed in community samples. In sum, no singular variable is known as a clear and robust predictor of inconsistent reporting, and non-significant effects seem to be the most common trend.
In an effort to improve the current state of the art, the purpose of the current study was three-fold. First, based on a lifespan perspective, we aimed to compare differences on inconsistency between positive and negative experiences and, second, to describe the patterns of inconsistent reporting. Third, we aimed to identify sociodemographic, experiences-related, and design-related predictors of inconsistency, performing separated analyses for positive and negative experiences.
2. Materials and Methods
2.1. Participants
The 171 participants included 140 females (81.9%) and 31 males (18.1%), with an age range from 18 to 92 (M = 42.3 years, SD = 23.5) at first assessment (T1). Regarding marital status, 50.3% (n = 86) were single, 32.2% (n = 55) were married or cohabiting, 14% (n = 24) were widowed, and the remaining 3.5% (n = 6) were separated or divorced. Most had completed at least a high school education (74.2%, n = 117), and 33.3% (n = 47) had a college degree; however, 20.5% (n = 35) had none or less than four years of schooling. Additionally, 39.2% (n = 67) were students, 36.8% (n = 63) were employed, and 22.2% (n = 38) were retired, while three participants (1.8%) reported another labour force status.
In an effort to involve participants from the community and to promote heterogeneity of the sample, individuals were recruited from two different sites, namely schools and an adult day care centre from the north of Portugal, based upon three inclusion criteria: individuals being older than 18 years; capable of speaking, reading, and writing in Portuguese; and not planning migration in the short-medium term. Initially, the study was presented in detail to possible participants, and only those that signed an informed consent were assessed.
As displayed in Figure 1, 282 subjects completed the first assessment, and 16.24% (n = 38) refused to participate at the second (T2). Regarding the distribution of sociodemographic characteristics, participants at T2 (n = 178) were different from those assessed only at T1 (n = 102) on marital status, Χ2(2) = 7.22, p = 0.027; education, Χ2(2) = 14.18, p < 0.001; labour force status, Χ2(2) = 26.06, p < 0.001; and age, t(270) = −3.07, p = 0.002, but were similar in gender, Χ2(1) = 0.29, p = 0.590. Overall, participants at T2 were more heterogeneous and well balanced at a group level. Additionally, there were no significant differences among participants and nonparticipants at T2 regarding reported experiences at T1: t(278) = −0.41, p = 0.681 for total; t(278) = 0.22, p = 0.830 for positive experiences; and t(278) = −1.55, p = 0.123 for negative experiences.
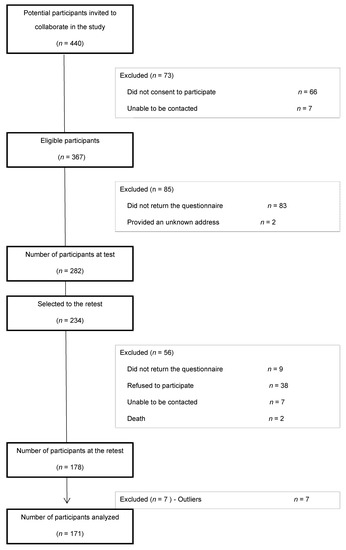
Figure 1.
Flow of participants chart.
2.2. Measures
The characterization of the participants was based on data collected through a sociodemographic questionnaire, which included questions about date of assessment, gender, age, marital status, education, and labour force status. Questions about ethnic group and income were deliberately not included for specific and general reasons, which deserve a comment. Indeed, ethnicity is an odd variable for our population, and (due to the national economic crisis) income would be misleading and unstable. Additionally, according to previous studies (e.g., Krinsley et al. 2003; Ouimette et al. 2005), those were not core variables in this field of research.
Life experiences were assessed using Lifetime Experiences Scale (LIFES Azevedo et al. 2020), a measure composed of two sections: lived versus non-lived experiences. In this study, only the first section was analysed, which includes 75 items organized into a thematic framework: school, work, health, leisure, life conditions, adverse experiences, achievements, and people and relationships. For each item, participants noted whether it occurred—yes vs. no vs. not remember; if they answered positively, additional questions were asked, namely developmental stage (childhood, adolescence, and adulthood), valence (negative vs. neutral vs. positive), and impact, using a five-point Likert scale ranging from 0 (not at all) to 4 (absolutely). Attending to our aims, this study analysed only two questions: occurrence to compute inconsistency and impact as a potential predictor. The distinction between positive and negative items was based on a previous study (Azevedo et al. 2017) that revealed that 39 items representing positive experiences and 30 denoting negative experiences. The remaining corresponded to filter items. LIFES was validated in community sample, and due to its nature, it is not appropriate to report Cronbach’s alpha (Hooper et al. 2011).
2.3. Procedures
This study applied a test-retest procedure and involved both within- and between-groups analyses. Before the recruitment of the participants, the study was reviewed and approved by the Institutional Review Board of School of Psychology–University of Minho and the Portuguese Data Protection Authority—Autorização n.º7665/2012. Participants were informed about the topic, procedures, and participating conditions, and only those who gave written informed consent were further assessed.
Data were collected using different strategies depending on the site. On one hand, participants recruited through the adult day care centre were face-to-face interviewed both at T1 and T2 (n = 36). On the other hand, participants recruited at schools were assessed at T1 using self-reports; at T2, data were collected using face-to-face interviews (n = 59) or self-reports (n = 76). Face-to-face interviews took place in private and calm settings and were conducted by research’s team members, who were properly trained. Self-reports were collected through mailed questionnaires returned by pre-paid envelopes or face-to-face individually or in small groups sessions, according to participants’ availability. At T2, participants recruited from schools were randomly selected and allocated to one mode of data collection—self-report vs. interview. In sum, data collection occurred using a same mood procedure, including being face-to-face interviewed or completing a self-report at both assessments (n = 112) or a different mode procedure, which consisted of an evaluation using self-report at T1 and face-to-face interviews at T2 (n = 59). Although participants were aware that it was a two-wave study and that data could be collected through self-report or interview, they were not informed that exactly the same measures would be applied twice nor that mode of assessment could change.
Data were collected between January 2013 and May 2015, and mean elapsed time was 147.3 days (SD = 114.1, range = 20–370). At both assessments, the booklet of assessment was similar and included the sociodemographic questionnaire and LIFES, described below; it took between 30–45 min to be completed. Ethical issues were considered throughout the process.
2.4. Variables
According to our aims, potential predictors included variables related with sociodemographic, experiences, and design features. Gender, age (in years), marital status (i.e., single vs. married vs. other status), labour force status (student vs. employed vs. other status), and education (i.e., four or less years of school vs. between six and twelve years of schools vs. graduated studies) were the sociodemographic variables included. Missing answers (corresponding to the count of missing answers across T1 and T2), total of reported positive and negative experiences (corresponding to the count of yes answers across T1 and T2), and impact (corresponding to a mean value computed from the sum of total impact and total of reported experiences) were the experience-related variables assessed. Lastly, design-related variables included time interval (computed as the difference in days between T1 and T2’s dates), mode of data collection (same mode at T1 and T2 vs. different mode at T1 and T2), and similarity between participant and interviewer corresponding to the comparison of gender and age, which established three groups: not similar vs. similar in one characteristic vs. similar in both characteristics).
The outcome variables were inconsistency on positive and on negative life experiences, which were specifically computed for this study. More specifically, answers of occurrence for individual items were compared and subtracted (i.e., T2–T1), in order to identify if it was a consistent or inconsistent response, which could represent under or overreporting. Then, the number of inconsistent responses was counted for the 39 items devoted to positive experiences and 30 to negative ones, resulting in the main variables under study. Patterns of under and overreporting were clarified through the count of negative and positive values, respectively, on differences between T1 and T2. The sum of these values corresponds to the total of inconsistency on positive and negative experiences. Then, these patterns were further compared to distinguish participants that were mainly under-reporters, mainly over-reporters, or undefined reporters (when there was a tie between under and overreporting).
2.5. Data Analysis
Descriptive and inferential statistical analyses were performed using software IBM Statistical Package for Social Sciences (IBM SPSS, version 22 for Windows). In order to compare experiences reported at T1 and T2 and to test differences between the inconsistency on positive and negative experiences, descriptive results and paired sample t-tests were used. Additionally, a Pearson correlation was computed to clarify the relationship between the inconsistencies on positive and negative experiences. The patterns of inconsistency were explored through descriptive data and a chi-square test. Two multiple linear regressions, using the entry method, were independently performed to identify predictors of inconsistency on positive and on negative experiences. Initially, separate correlations (e.g., Pearson correlations between numerical variables) or differences tests (e.g., independent t-tests for grouping variables with two groups or ANOVA for grouping variables analysing three groups) were calculated for each potential predictor. Those variables that were statistically significant in these bivariate analyses advanced for the multiple linear regressions, namely impact and time interval as predictors of inconsistencies on positive experiences and marital status, labour force status, age, impact, total of negative experiences reported, and time interval for the negative experiences. Due to the fact that SPSS only computed regression for dichotomized categorical variables and to avoid the outspread of variables, simple linear regressions that were performed to explore each groups of marital status and labour force status should be tested in the model; consequently, single vs. other status and students vs. other status were the groups selected since they represented the highest variance explained; other variables were numerical. Initially, outliers at outcome variables were identified through z-scores, and before the models’ interpretation, the assumptions for linear regression were checked, including Mahalanobis distances. The level of significance at the bivariate and multivariate analyses was p < 0.05. Dataset and SPSS syntax that support this manuscript are available at Open Science Framework-https://osf.io/xgbcd/?view_only=eaed8810aa0a4a398661f90ff3c699a5 (accessed on 7 February 2022).
3. Results
3.1. Inconsistency on Positive and Negative Life Experiences
On average, participants reported a significantly higher number of positive life experiences at T2 (M = 21.6, SD = 4.4) than at T1 (M = 20, SD = 4.84), t(170) = −4.97, p < 0.001; the same trend applied to negative life experiences (M = 5.81, SD = 2.96 versus M = 5.55, SD = 2.97), t(170) = −1.97, p = 0.051. When the inconsistency on positive and negative life experiences was compared, there were significant differences between their totals, respectively, M = 3.6, SD = 1.9 vs. M = 2.1, SD = 1.5, t(170) = 9.49, p < 0.001, and proportions, M = 0.1, SD = 0.1 vs. M = 0.1, SD = 0.1, t(170) = 5.06, p < 0.001, indicating a higher number of inconsistencies on positive experiences. Additionally, the inconsistencies on positive and on negative life experiences were positively correlated, r = 0.27, p < 0.001, suggesting that participants reporting a higher number of inconsistencies on positive experiences also presented greater inconsistencies on negative ones.
Regarding the patterns of inconsistency, shown in Table 1, the mean value for overreporting (no to yes change) achieved the highest value for both positive and negative experiences. Moreover, when participants were grouped by pattern of inconsistency on positive experiences, 49.1% (n = 84) presented a trend of overreporting, 28.1% (n = 48) a trend of underreporting, and 22.8% (n = 39) a tie between under and overreporting responses. For negative experiences, a similar result was achieved: 39.2% (n = 67) exhibited a trend of overreporting, 33.3% (n = 57) of underreporting, and 27.5% (n = 47) of undefined. However, a chi-square analysis revealed that the patterns of inconsistency for positive and negative experiences were not associated, Χ2(4) = 3.39, p = 0.495; indeed, cross-tabulations showed only 39.5% of the participants presented the same pattern (namely, 22.2% in overreporting, 9.9% in underreporting, and 7.6% in undefined) between positive and negative experiences.

Table 1.
Means and Standard Deviations of Inconsistency on Positive and Negative Life Experiences by Groups.
According to descriptive results provided on Table 1, a high value of inconsistencies on both positive and negative life experiences were exhibited by males, divorced or widowed participants, people that were not employed or studying, and by those that were assessed using two different modes. Participants with four or less years of education presented a high number of inconsistencies on positive life experiences, while those with graduated studies presented a high number of inconsistencies on negative experiences. Regarding similarity between interviewer and participant, inconsistencies on positive experiences were high for those participants that shared only one characteristic with the interviewer, whereas participants not similar to the interviewer presented a high mean value for negative experiences.
3.2. Predicting Inconsistency on Positive Experiences
Bivariate tests revealed significant correlations between inconsistencies on positive experiences and impact, r = −0.22, p = 0.004, and time interval, r = 0.16, p = 0.037. Additionally, inconsistencies on positive experiences were not statistically correlated with age, r = 0.11, p = 0.166; number of missing questions, r = −0.09, p = 0.225; and total of reported positive experiences, r = 0.02, p = 0.758. Moreover, there were no differences on inconsistencies on positive experiences based on gender, t(169)= 0.127, p = 0.899; mode of data collection, t(169) = −1.27, p = 0.205; marital status, F(2,168) = 2.40, p = 0.094; labour force status, F(2,168) = 2.17, p = 0.117; education, F(2,168) = 0.25, p = 0.777; and similarity between participant and interviewer, F(2,92) = 0.19, p = 0.830.
Based on previous results, the multiple linear model included two predictors, namely impact and time interval. As displayed in Table 2, the model explained 6.6% of the variance for the inconsistency on positive experiences, and it was statistically significant; the only significant predictor was impact, suggesting that higher ratings of impact predict lower inconsistencies on positive experiences.
Table 2.
Multiple Linear Regression Analyses Predicting Inconsistency on Positive and Negative Life Experiences.
3.3. Predicting Inconsistency on Negative Experiences
According to bivariate analyses, age, the number of reported negative experiences, impact, and time interval were significantly correlated with inconsistencies on negative experiences, r = 0.17, p = 0.025, r = 0.42, p < 0.001; r = −0.20, p = 0.012; r = 0.21, p = 0.006, respectively. The number of inconsistencies on negative experiences differed according marital status, F(2,168) = 6.83, p = 0.001, and labour force status, F(2,168) = 6.26, p = 0.002. On the other hand, there were no significant correlations between inconsistencies on negative experiences and the number of missing questions, r = −0.01, p = 0.947. Besides, gender, t(169) = 0.20, p = 0.841; mode of data collection, t(69) = −1.40, p = 0.164; education, F(2,168) = 2.31, p = 0.102; and similarity between participant and interviewer, F(2,92) = 2.24, p = 0.138, did not significantly affect inconsistencies on negative experiences.
The final model for inconsistency on negative experiences included six variables, namely marital status (single vs. other status), labour force status (students vs. other status), age, impact, time interval, and the total number of negative experiences. According to Table 2, this model accounted for 24.3% of the variance, and a significant regression equation was found. More specifically, whereas the total of negative experiences reported was a significant predictor, time interval was a marginally significant predictor of inconsistency on negative experiences. Therefore, higher numbers of negative experiences on both assessment and longer delays between T1 and T2 are predictors of a high value of inconsistency. No other variable emerged as a significant predictor.
4. Discussion
Overall inconsistency consists mainly of overreporting, i.e., an increased number of affirmative answers. Additionally, there were a higher number of inconsistencies on positive experiences than on negative, but both variables were significantly correlated. Moreover, the model for inconsistency on positive experiences explained less variance than for negative ones. Despite the comprehensive set of variables analysed, including sociodemographic, experiences-related, and design-related variables, few predictors were identified for inconsistency on the report of positive and negative experiences.
Despite the difficulties in comparing our results with previous research, our trend of overreporting contradicts a more common finding toward underreporting (Ayalon 2015; Dill et al. 1991; Hardt et al. 2006; Hepp et al. 2006); nevertheless, other authors (e.g., Suh et al. 1996) also achieved similar results. Although being equally disturbing as underreporting, this pattern can be more easily justified: it may be due to reminiscence effects, to greater comfort in disclosing personal information, or it can result from new experiences (despite our efforts to track them); nonetheless, these are only potential explanations that should be further explored. To our best knowledge, no previous study compared positive and negative experiences on a community sample applying a lifespan perspective, but our results extended available findings. More specifically, lower values of agreement seemed to be presented by positive experiences than negative ones (Hardt et al. 2006; Monteiro 2014; Pinto et al. 2014; Yancura and Aldwin 2009). Similarly, Suh et al. (1996, p. 1095) concluded that “bad events seemed to be experienced with much more consistency than good events.” In our opinion, these patterns of results are additional evidences to Baumeister et al.’s (2001) statement that bad is stronger than good. The correlation between inconsistency on positive and negative experiences is also an interesting finding, which deserves further attention, as it can be a signal of a general trend of reporting.
Regarding variables involved in inconsistency, our results are in line with previous research in suggesting that individual characteristics, such as age or gender, are not relevant (Dube et al. 2004; Hepp et al. 2006; Langeland et al. 2014; Shields et al. 2015). Inversely, two experiences-related variables (i.e., impact and total of negative experiences) were significant predictors of inconsistency on positive and negative experiences, respectively. Although it seems reasonable to think that those reporting more experiences are more likely to be inconsistent, due to forgetting or difficulties to retrieve specific experiences, our results refute those from McKinney et al. (2009), which concluded that consistent reporters of childhood physical abuse tended to experience multiple types of abuse (vs. only one type). Additionally, low impact was a significant predictor of inconsistency on positive but surprisingly not on negative experiences. For instance, the same authors found that inconsistent reporters of childhood physical abuse reported more moderate forms of abuse, while consistent reporters reported more severe forms of abuse; a similar trend was presented by Langeland et al. (2014) regarding reports of childhood sexual abuse. This discrepancy can be due to design specificities (e.g., domains included lifespan perspective); moreover, attending to the fact that usually people lived more positive than negative experiences (Baumeister et al. 2001; Overbeek et al. 2010), perhaps impact plays a stronger role in the recall of positive ones. Despite our relatively short time interval, it marginally affected inconsistency, which is not implausible; indeed, as time passes, there are more chances to forget, to live new experiences, and to revisit past ones, in sum, more time to change. Although our results can be explained by the large standard deviation, this finding represents a challenge. At this point, there are no golden rules about optimal time intervals (Taris 2008), and despite all carefulness, they are actually defined by participants.
Despite the novelties and advances achieved, some limitations deserve comment. First, due to contextual circumstances, a relatively small convenience sample was used, which constrained results generalization. Additionally, participants were assessed through different modes of data collection, which according to our results, did not affect inconsistency; nonetheless, a deeper comparison should be made in upcoming studies. Third, although health variables are commonly addressed, they were not included here. The distinction between positive and negative experiences was based on normative ratings of valence, a strategy that benefits general perceptions while missing idiosyncrasies. This is also a limitation attending to the fact that valence involves not only very personal appraisals but also some inconsistent appraisals (Azevedo 2016); it would be interesting to replicate this study applying a more subjective approach. Lastly, self-selection at the recruitment phase and at T2 can also limit, in an uncertain way, our findings. Indeed, it is reasonable to suspect that individuals who did not complete the assessments are somehow different from completers (Gray 2016); for instance, they can demonstrate a willingness to respond and some interest in the topic, but the reasons involved in refusals and non-responses, as well as their impact, are unknown.
A better knowledge about variables involved in inconsistent reporting deeply impacts the assessment of life experiences for both clinical and research purposes; therefore, it should not remain a neglected topic. Currently, we know more about variables not involved in inconsistency than those that matter. Therefore, future research efforts are needed to overcome current limitations, address new variables, and improve design features.
Author Contributions
Conceptualization, V.A., C.M. and Â.M.; methodology, V.A., C.M. and Â.M.; formal analysis, V.A.; writing—original draft preparation, V.A.; writing—review and editing, V.A., C.M. and, Â.M.; supervision, C.M. and Â.M.; funding acquisition, V.A., C.M. and Â.M. All authors have read and agreed to the published version of the manuscript.
Funding
This manuscript is part of a doctoral dissertation which had the support of the Portuguese Foundation for Science and Technology (FCT), through the PhD grant with the reference SFRH/BD/6022/2011, funded by POPH-QREN-Typology 4.1-Advanced Training–reimbursed by the European Social Fund and national funds from State Budget. This study was conducted at the Psychology Research Centre (CIPsi/UM) School of Psychology, University of Minho, supported by the Foundation for Science and Technology (FCT) through the Portuguese State Budget (UIDB/01662/2020).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of School of Psychology-University of Minho (CA_CIPSI_082012.1) and the Portuguese Data Protection Authority—Autorização n.º7665/2012.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Dataset and SPSS syntax that support this manuscript are available at Open Science Framework (https://osf.io/xgbcd/) (accessed on 13 December 2021).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ayalon, Liat. 2015. Retrospective reports of negative early life events over a 4-year period: A test of measurement invariance and response consistency. Journals of Gerontology: Social Sciences 72: 901–12. [Google Scholar] [CrossRef]
- Azevedo, Vanessa. 2016. Life Experiences and Psychopathological Symptons (re)told in Adulthood: What People Tell about Them? How Consistent are Their Reports? And Which Variables Matter? Doctoral thesis, University of Minho, Braga, Portugal. [Google Scholar]
- Azevedo, Vanessa, Carla Martins, and Ângela Maia. 2017. Life experiences throughout the lifespan: What people say (or not) about them? Journal of Adult Development 3: 69–85. [Google Scholar] [CrossRef]
- Azevedo, Vanessa, Carla Martins, and Ângela Maia. 2020. Lifetime Experiences Scale (LIFES): Development and validation in community samples. Psicologia 34: 174–94. [Google Scholar] [CrossRef]
- Azevedo, Vanessa, Carla Martins, Margarida Carvalho, and Ângela Maia. 2021. Inconsistent reporting of life experiences: What people think and how they explain it. Análise Psicológica 39: 199–211. [Google Scholar] [CrossRef]
- Baumeister, Roy F., Ellen Bratslavsky, Catrin Finkenauer, and Kathleen D. Vohs. 2001. Bad is stronger than good. Review of General Psychology 5: 323–70. [Google Scholar] [CrossRef]
- Casey, Robert L., Minoru Masuda, and Thomas H. Holmes. 1967. Quantitative study of recall of life events. Journal of Psychosomatic Research 11: 239–47. [Google Scholar] [CrossRef]
- Chapman, Daniel P., Charles L. Whitfield, Vincent J. Felitti, Shanta R. Dube, Valerie J. Edwards, and Robert F. Anda. 2004. Adverse childhood experiences and the risk of depressive disorders in adulthood. Journal of Affective Disorders 82: 217–25. [Google Scholar] [CrossRef] [PubMed]
- Colman, Ian, Mila Kingsbury, Y. Garad, Yiye Zeng, Kiyuri Naicker, Scott Patten, Peter B. Jones, T. Cameron Wild, and Angus H. Thompson. 2016. Consistency in adult reporting of adverse childhood experiences. Psychological Medicine 46: 543–49. [Google Scholar] [CrossRef] [PubMed]
- Dill, Diana L., James A. Chu, Mollie C. Grob, and Susan V. Eisen. 1991. The reliability of abuse history reports: A comparison of two inquiry formats. Comprehensive Psychiatry 32: 166–69. [Google Scholar] [CrossRef]
- Dube, Shanta R., David F. Williamson, Ted Thompson, Vincent J. Felitti, and Robert F. Anda. 2004. Assessing the reliability of retrospective reports of adverse childhood experiences among adult HMO members attending a primary care clinic. Child Abuse and Neglect 28: 729–37. [Google Scholar] [CrossRef]
- Fergusson, David M., John Horwood, and Lianne J. Woodward. 2000. The stability of child abuse reports: A longitudinal study of the reporting behaviour of young adults. Psychological Medicine 30: 529–44. [Google Scholar] [CrossRef] [PubMed]
- Gray, Linsay. 2016. The importance of post hoc approaches for overcoming non-response and attrition bias in population-sampled studies. Social Psychiatry and Psychiatric Epidemiology 51: 155–57. [Google Scholar] [CrossRef]
- Hardt, Jochen, Anna Sidor, Michael Bracko, and Ulrich Tiber Egle. 2006. Reliability of retrospective assessments of childhood experiences in Germany. The Journal of Nervous and Mental Disease 194: 676–83. [Google Scholar] [CrossRef]
- Hardt, Jochen, and Michael Llewellyn Rutter. 2004. Validity of adult retrospective reports of adverse childhood experiences: Review of the evidence. Journal of Child Psychology and Psychiatry 45: 260–73. [Google Scholar] [CrossRef] [PubMed]
- Hepp, Urs, Alex Gamma, Gabriella Milos, Dominique Eich, Vladeta Ajdacic-Gross, Wulf Rössler, Jules Angst, and Ulrich Schnyder. 2006. Inconsistency in reporting potentially traumatic events. British Journal of Psychiatry 188: 278–83. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Holmes, Thomas H., and Richard H. Rahe. 1967. The Social Readjustment Rating Scale. Journal of Psychosomatic Research 11: 213–18. [Google Scholar] [CrossRef]
- Hooper, Lisa M., Patricia Stockton, Janice L. Krupnick, and Bonnie L. Green. 2011. Development, use, and psychometric properties of the Trauma History Questionnaire. Journal of Loss and Trauma 16: 258–83. [Google Scholar] [CrossRef]
- Jenkins, C. David, Michael W. Hurst, and Robert M. Rose. 1979. Life changes: Do people really remember? Archives of General Psychiatry 36: 379–84. [Google Scholar] [CrossRef]
- Kendall-Tackett, Kathleen, and Kathryn Becker-Blease. 2004. The importance of retrospective findings in child maltreatment research. Child Abuse and Neglect 28: 723–27. [Google Scholar] [CrossRef]
- Klein, Daniel N., and David R. Rubovits. 1987. The reliability of subjects’ reports on stressful life events inventories: A longitudinal study. Journal of Behavioral Medicine 10: 501–12. [Google Scholar] [CrossRef] [PubMed]
- Krinsley, Karen E., James G. Gallagher, Frank W. Weathers, Catherine J. Kutter, and Danny G. Kaloupek. 2003. Consistency of retrospective reporting about exposure to traumatic events. Journal of Traumatic Stress 16: 399–409. [Google Scholar] [CrossRef] [PubMed]
- Langeland, Willemien, Jan H. Smit, Harald Merckelbach, Gerard De Vries, Adriaan W. Hoogendoorn, and Nel Draijer. 2014. Inconsistent retrospective self-reports of childhood sexual abuse and their correlates in the general population. Social Psychiatry and Psychiatric Epidemiology 50: 603–12. [Google Scholar] [CrossRef]
- McKinney, Christy M., Robert Harris, and Raul Caetano. 2009. Reliability of self-reported childhood physical abuse by adults and factors predictive of inconsistent reporting. Violence and Victims 24: 653–68. [Google Scholar] [CrossRef] [PubMed]
- Mesquita, Cristina, and Ângela Maia. 2018. What is told when the story is retold? Consistency of reports in psychiatric patients. Scandinavian Journal of Psychology 59: 311–318. [Google Scholar] [CrossRef]
- Monteiro, Débora. 2014. Experiências de vida positivas em jovens com história de maltrato: Resiliência e estabilidade dos relatos. Master’s thesis, Universidade do Minho, Braga, Portugal. [Google Scholar]
- Ouimette, Paige, Jennifer Read, and Pamela J. Brown. 2005. Consistency of retrospective reports of DSM-IV criterion A traumatic stressors among substance use disorder patients. Journal of Traumatic Stress 18: 43–51. [Google Scholar] [CrossRef] [PubMed]
- Overbeek, Geertjan, Ad Vermulst, Ron De Graaf, Margreet Ten Have, Rutger Engels, and Ron Scholte. 2010. Positive life events and mood disorders: Longitudinal evidence for an erratic lifecourse hypothesis. Journal of Psychiatric Research 44: 1095–100. [Google Scholar] [CrossRef] [PubMed]
- Paykel, Eugene. 2001. The evolution of life events research in psychiatry. Journal of Affective Disorders 62: 141–49. [Google Scholar] [CrossRef]
- Pinto, Ricardo, Liliana Correia, and Ângela Maia. 2014. Assessing the reliability of retrospective reports of adverse childhood experiences among adolescents with documented childhood maltreatment. Journal of Family Violence 29: 431–438. [Google Scholar] [CrossRef]
- Schraedley, Pamela K., Jay Turner, and Ian H. Gotlib. 2002. Stability of retrospective reports in depression: Traumatic events, past depressive episodes, and parental psychopathology. Journal of Health and Social Behavior 43: 307–16. [Google Scholar] [CrossRef]
- Shaffer, Anne, Lisa Huston, and Byron Egeland. 2008. Identification of child maltreatment using prospective and self-report methodologies: A comparison of maltreatment incidence and relation to later psychopathology. Child Abuse and Neglect 32: 682–92. [Google Scholar] [CrossRef]
- Shields, Margot, Wendy Hovdestad, and Lil Tonmyr. 2015. Assessment of the quality of the childhood physical abuse measure in the National Population Health Survey. Health Reports 26: 3–10. [Google Scholar]
- Sobell, Linda C., Tony Toneatto, Mark B. Sobell, Reinhard Schuller, and Maxine Maxwell. 1990. A procedure for reducing errors in reports of life events. Journal of Psychosomatic Research 34: 163–70. [Google Scholar] [CrossRef]
- Suh, Eunkook, Ed Diener, and Frank Fujita. 1996. Events and subjective well-being: Only recent events matter. Journal of Personality and Social Psychology 70: 1091–102. [Google Scholar] [CrossRef] [PubMed]
- Sun, Xiao-Jun, Geng-Feng Niu, Zhiqi You, Zong-Kui Zhou, and Yun Tang. 2017. Gender, negative life events and coping on different stages of depression severity: A cross-sectional study among Chinese university students. Journal of Affective Disorders 209: 177–81. [Google Scholar] [CrossRef] [PubMed]
- Taris, Toon W. 2008. Reliability issues in longitudinal research. In Handbook of Longitudinal Research: Design, Measurement, and Analysis. Edited by Scott Menard. London: Academic Press, pp. 139–51. [Google Scholar]
- Widom, Cathy Spatz, Karen Raphael, and Kimberly A. DuMont. 2004. The case for prospective longitudinal studies in child maltreatment research: Commentary on Dube. Child Abuse and Neglect 28: 715–22. [Google Scholar] [CrossRef]
- Yancura, Loriena A., and Carolyn M. Aldwin. 2009. Stability and change in retrospective reports of childhood experiences over a 5-year period: Findings from the Davis Longitudinal Study. Psychology and Aging 24: 715–21. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, Mark. 1983. Methodological issues in the assessment of life events: A review of issues and research. Clinical Psychology Review 3: 339–70. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).