
Prevalence of Sick Building Syndrome Symptoms in Residents During the COVID-19 Pandemic—A Case Study of Suzhou City, China


Abstract
1. Introduction
2. Materials and Methods
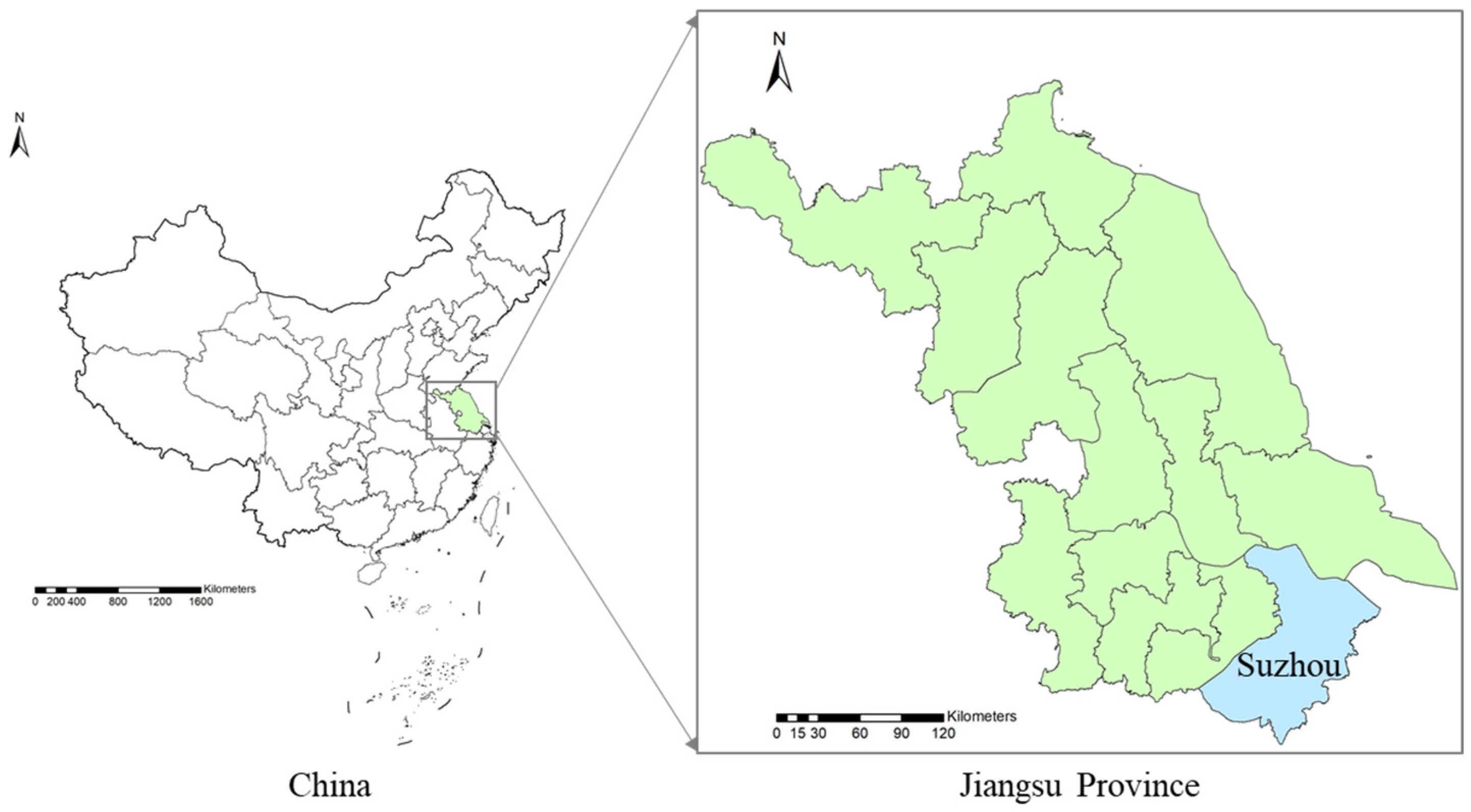
2.1. Study Area
2.2. Questionnaire Survey
2.3. Statistical Analysis
3. Results
3.1. Demographic Information of the Participants
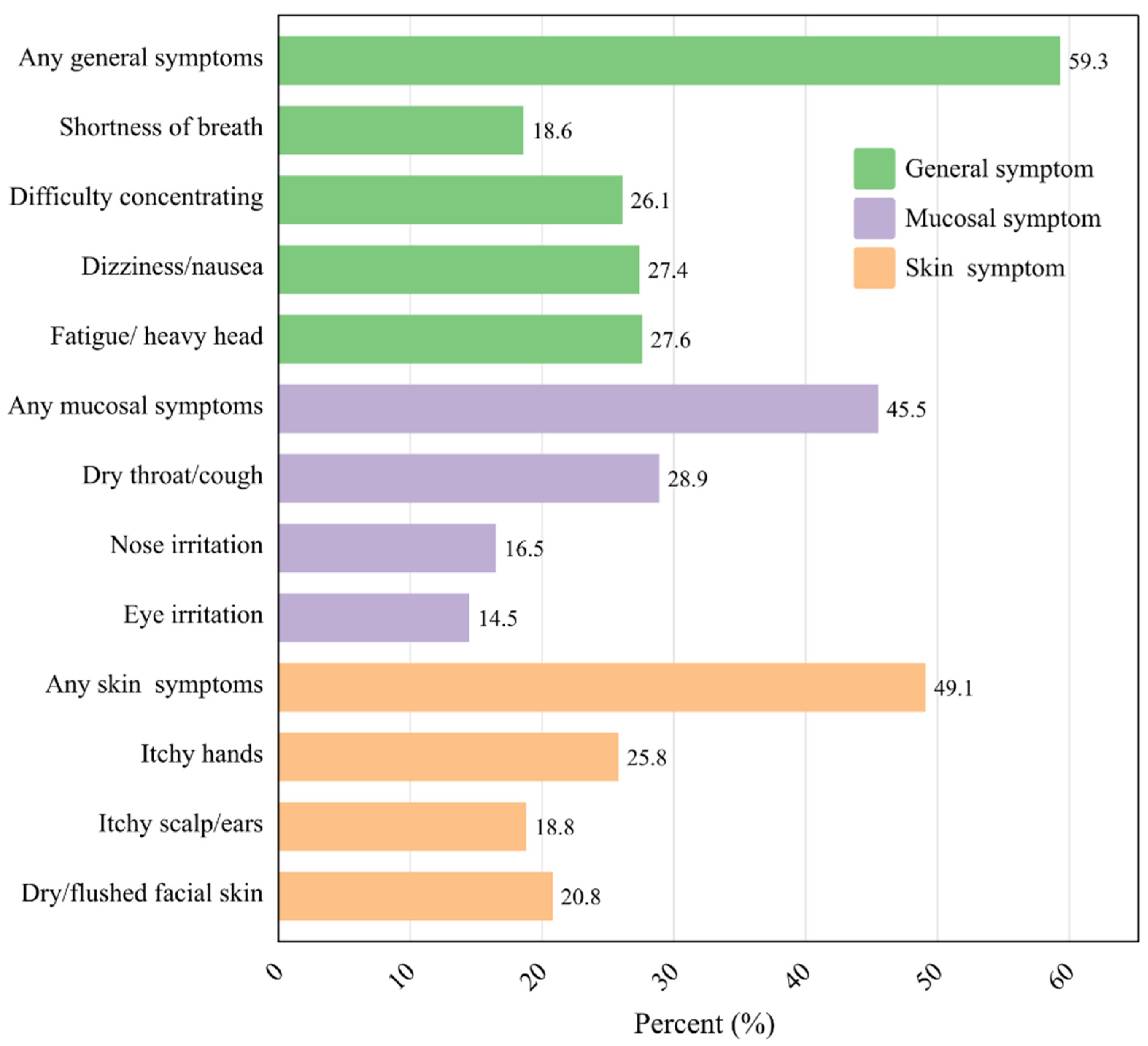
3.2. Prevalence of SBS Symptoms
3.3. Factors Associated with SBS
3.4. Behavioural Intentions to Improve Indoor Environmental Quality
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Variables | Adjusted Odds Ratio (95% CI) | ||||
|---|---|---|---|---|---|
| General Symptoms | Mucosal Symptoms | Skin Symptoms | |||
| Building characteristic | Neighbourhood pollution source | Yes | 36.3 (8.6–154.2) *** | 41.1 (5.6–303.6) *** | 25.5 (6.0–107.9) |
| No | 1.0 | 1.0 | 1.0 | ||
| Residential floor | >18 | 2.4 (1.0–5.4) * | 2.6 (1.1–5.8) * | 2.4 (1.1–5.4) * | |
| 10–18 | 1.8 (0.9–3.4) | 2.7 (1.4–5.2) ** | 2.0 (1.0–3.8) * | ||
| 7–9 | 1.9 (1.0–3.5) | 3.0 (1.6–5.8) ** | 2.5 (1.34–4.66) ** | ||
| 4–6 | 1.42 (0.8–2.7) | 1.1 (0.6–2.1) | 1.83 (1.0–3. 5) | ||
| 1–3 | 1.0 | 1.0 | 1.0 | ||
| Construction year | Before 1980 | 7.9 (3.0–20.6) *** | 6.9 (2.9–16.3) *** | 2.8 (1.2–6.2) * | |
| 1980–1990 | 3.4 (1.7–6.6) *** | 6.74 (3.3–13.9) *** | 4.34 (2.2–8.6) *** | ||
| 1991–2000 | 3.9 (2.7–7.4) *** | 3.7 (1.9–7.2) *** | 2.61 (1.4–4.9) ** | ||
| 2001–2010 | 1.5 (0.8–2.7) | 1.5 (0.8–3.0) | 1.0 (0.6–1.9) | ||
| 2011–now | 1.0 | 1.0 | 1.0 | ||
| Dwelling area | <60 m2 | 2.2 (1.1–4.5) * | 1.6 (0.8–3.2) | 1.9 (1.0–3.8) | |
| 61–90 m2 | 1.6 (1.0–2.8) | 1.6 (1.0–2.7) | 2.1 (1.2–3.5) ** | ||
| 91–120 m2 | 1.1 (0.6–1.9) | 1.3 (0.8–2.3) | 1.5 (0.8–2.5) | ||
| >120 m2 | 1.0 | 1.0 | 1.0 | ||
| Ownership | Other | 2.6 (1.8–3.9) *** | 2.7 (1.8–4.0) *** | 2.9 (2.0–4.4) *** | |
| Owned | 1.0 | 1.0 | 1.0 | ||
| Lifestyles | Cleaning frequency | >1/week | 0.5 (0.2–1.2) | 0.9 (0.4–2.1) | 0.7 (0.3–1.6) |
| 1/week | 3.3 (0.6–2.9) | 1.5 (0.7–3.4) | 1.2 (0.6–2.7) | ||
| 1/2–4 days | 1.4 (0.60–3.3) | 2.0 (0.8–4.6) | 1.1 (0.5–2.4) | ||
| Everyday | 1.0 | 1.0 | 1.0 | ||
| Use of disinfectant | Everyday | 9.3 (5.1–19.2) *** | 7.9 (4.0–15.6) *** | 9.8 (4.8–19.8) *** | |
| 1/2–4 days | 9.0 (5.0–16.3) *** | 8.6 (4.5–16.4) *** | 13.1 (6.7–25.5) *** | ||
| 1/week | 8.0 (3.6–17.9) *** | 6.6 (2.9–14.9) *** | 17.0 (7.2–40.4) *** | ||
| >1/week | 1.0 | 1.0 | 1.0 | ||
| Use of air freshener | Everyday | 10.9 (5.7–21.0) *** | 11.3 (5.6–22.8) *** | 12.2 (5.8–25.4) *** | |
| 1/2–4 days | 8.6 (4.8–15.5) *** | 7.5 (3.9–14.6) *** | 16.0 (7.9–32.5) *** | ||
| 1/week | 5.6 (2.6–12.1) *** | 9.6 (4.2–21.9) *** | 18.5 (7.7–44.4) *** | ||
| >1/week | 1.0 | 1.0 | 1.0 | ||
| Use of kitchen hood | Yes | 0.4 (0.2–0.6) *** | 0.5 (0.3–0.7) *** | 0.6 (0.4–0.9) * | |
| No | 1.0 | 1.0 | 1.0 | ||
| Use of air cleaner | Yes | 0.4 (0.2–0.6) *** | 0.4 (0.3–0.7) *** | 0.4 (0.2–0.6) | |
| No | 1.0 | 1.0 | 1.0 | ||
| Pet keeping | Yes | 2.2 (1.5–3.4) *** | 1.5 (1.0–2.2) * | 2.0 (1.3–2.9) ** | |
| No | 1.0 | 1.0 | 1.0 | ||
| Exposing bedding to the sun | Yes | 0.3 (0.2–0.5) *** | 0.5 (0.3–0.7) ** | 0.5 (0.3–0.7) *** | |
| No | 1.0 | 1.0 | 1.0 | ||
| Indoor smoking | Often | 3.1 (1.9–5.2) *** | 2.4 (1.5–3.9) *** | 1.5 (0.9–2.3) | |
| Occasionally | 2.8 (1.7–4.5) *** | 2.1 (1.3–3.3) ** | 1.7 (1.1–2.6) * | ||
| No | 1.0 | 1.0 | 1.0 | ||
| Indoor environment | Indoor light duration | <2 h | 2.8 (1.6–4.9) *** | 2.1 (1.3–3.5) ** | 3.6 (2.1–6.0) *** |
| 3–6 h | 1.6 (1.0–2.5) * | 1.5 (0.9–2.3) | 1.6 (1.0–2.5) * | ||
| >6 h | 1.0 | 1.0 | 1.0 | ||
| Ventilation | <6 h/day | 1.6 (1.1–2.4) * | 1.7 (1.1–2.5) * | 1.3 (0.9–2.0) | |
| ≥6 h/day | 1.0 | 1.0 | 1.0 | ||
| Composite floor board | Yes | 1.6 (1.1–2.4) * | 1.7 (1.2–2.6) ** | 1.5 (1.1–2.3) * | |
| No | 1.0 | 1.0 | 1.0 | ||
| Renovation within a year | Yes | 1.8 (1.2–2.7) ** | 1.4 (1.0–2.1) | 2.0 (1.3–2.9) ** | |
| No | 1.0 | 1.0 | 1.0 | ||
| Mould spots | Yes | 1.1 (0.8–1.7) | 0.8 (0.5–1.2) | 1.3 (0.9–1.9) | |
| No | 1.0 | 1.0 | 1.0 | ||
| Damp stains | Yes | 1.3 (0.9–1.9) | 1.5 (1.0–2.2) * | 1.0 (0.7–1.5) | |
| No | 1.0 | 1.0 | 1.0 | ||
| Water damage | Yes | 1.4 (0.9–2.0) | 1.8 (1.2–2.6) ** | 1.2 (0.8–1.7) | |
| No | 1.0 | 1.0 | 1.0 | ||
| Condensation | Yes | 1.1 (0.7–1.6) | 1.1 (0.7–1.6) | 1.3 (0.9–1.9) | |
| No | 1.0 | 1.0 | 1.0 | ||
| Cockroaches | Yes | 1.3 (0.9–1.9) | 1.2 (0.8–1.7) | 1.2 (0.8–1.8) | |
| No | 1.0 | 1.0 | 1.0 | ||
| Rats | Yes | 3.0 (1.9–4.6) *** | 1.7 (1.2–2.6) ** | 2.1 (1.4–3.2) *** | |
| No | 1.0 | 1.0 | 1.0 | ||
| Mosquitoes /flies | Yes | 0.6 (0.4–0.9) ** | 0.6 (0.4–0.8) ** | 0.8 (0.5–1.2) | |
| No | 1.0 | 1.0 | 1.0 | ||
| Perception of indoor environment | Indoor air pollution | Yes | 2.2 (1.3–3.6) ** | 1.9 (1.2–3.0) ** | 2.3 (1.4–3.6) ** |
| No | 1.0 | 1.0 | 1.0 | ||
| Health hazards of indoor air pollution | Yes | 1.1 (0.7–1.7) | 1.1 (0.8–1.8) | 1.1 (0.7–1.6) | |
| No | 1.0 | 1.0 | 1.0 | ||
| Indoor environmental comfort | No | 5.1 (3.1–8.4) *** | 6.4 (3.5–11.4) *** | 4.5 (2.7–7.6) *** | |
| Yes | 1.0 | 1.0 | 1.0 | ||
| Psychological effect | Yes | 2.2 (1.4–3.5) ** | 1.5 (0.9–2.2) | 1.4 (0.9–2.1) | |
| No | 1.0 | 1.0 | 1.0 | ||
Appendix B
- (1)
- Is there any pollution source within 200 m of your house?
- (2)
- On which floor do you live?
- (3)
- The construction year of your residential building.
- (4)
- The dwelling area of your home.
- (5)
- Do you own your home?
- (6)
- How often do you clean your home?
- (7)
- How often do you use the disinfectant?
- (8)
- How often do you use the air freshener?
- (9)
- Do you use an extractor hood when cooking?
- (10)
- Do you use an air cleaner?
- (11)
- Do you have pets in your home?
- (12)
- Do you often expose your bedding to the sun?
- (13)
- Does anyone smoke in your home?
- (14)
- How long does the light in your house last?
- (15)
- How long do you ventilate every day?
- (16)
- Do you use composite flooring?
- (17)
- Have you carried out any renovation work in your home in the last year?
- (18)
- Did you see any mould spot in your house before?
- (19)
- Did you see any damp stain in your house before?
- (20)
- Did you see condensation on the window panels in your home in winter before?
- (21)
- Did you see any cockroaches in your home before?
- (22)
- Did you see any rats in your house before?
- (23)
- Did you see any mosquitos/flies in your house before?
- (24)
- In your opinion, how polluted is the air in your home?
- (25)
- Do you think that indoor air pollution is harmful to humans?
- (26)
- How do you feel about the comfort of the indoor environment? Please complete the following form.
| Indoor Environment | Very Comfortable | Comfortable | Generally | Uncomfortable | Very Uncomfortable | |
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | ||
| 1. | Lighting condition | □ | □ | □ | □ | □ |
| 2. | Ventilation | □ | □ | □ | □ | □ |
| 3. | Noise level | □ | □ | □ | □ | □ |
| 4. | Indoor air quality | □ | □ | □ | □ | □ |
| 5. | Humidity | □ | □ | □ | □ | □ |
| 6. | Temperature | □ | □ | □ | □ | □ |
- (27)
- Is your psychological state affected by staying at home for a long time?
- (28)
- What will you do if indoor air is polluted? Please complete the following form.
| Behavioural Intentions | Yes | No | |
|---|---|---|---|
| 1. | Reducing indoor smoking | □ | □ |
| 2. | Improving ventilation | □ | □ |
| 3. | Using adsorption materials or green plants | □ | □ |
| 4. | Detecting indoor air pollutants | □ | □ |
| 5. | Treating indoor air pollution | □ | □ |
| Have You Had Any of the Following Symptoms in the Last Three Months When You Were at Home? | Did the Symptoms Subside When You Left the House? | |||||
|---|---|---|---|---|---|---|
| Often (Every Week) | Sometimes (1–2 Weeks) | Rarely (>2 Weeks) | Never | Yes | No | |
| General symptoms | ||||||
| Fatigue/heavy head | □ | □ | □ | □ | □ | □ |
| Dizziness/nausea | □ | □ | □ | □ | □ | □ |
| Difficulty concentrating | □ | □ | □ | □ | □ | □ |
| Shortness of breath | □ | □ | □ | □ | □ | □ |
| Mucosal symptoms | ||||||
| Dry throat/cough | □ | □ | □ | □ | □ | □ |
| Nose irritation | □ | □ | □ | □ | □ | □ |
| Eye irritation | □ | □ | □ | □ | □ | □ |
| Skin symptoms | ||||||
| Itchy hands | □ | □ | □ | □ | □ | □ |
| Itchy scalp/ears | □ | □ | □ | □ | □ | □ |
| Dry/flushed facial skin | □ | □ | □ | □ | □ | □ |
- (29)
- Gender
- (30)
- Age
- (31)
- Occupation
- (32)
- Educational attainment
- (33)
- Your household income per month (CNY)
- (34)
- Do you have a history of respiratory disease?
References
- WHO. Indoor Air Pollutants: Exposure and Health Effects; EURO Reports and Studies 78; WHO: Copenhagen, Denmark, 1983. [Google Scholar]
- Dorizas, P.V.; Assimakopoulos, M.N.; Santamouris, M. A holistic approach for the assessment of the indoor environmental quality, student productivity, and energy consumption in primary schools. Environ. Monit. Assess. 2015, 187, 259. [Google Scholar] [CrossRef] [PubMed]
- Mansor, A.A.; Abdullah, S.; Ahmad, A.N.; Ahmed, A.N.; Zulkifli, M.F.R.; Jusoh, S.M.; Ismail, M. Indoor air quality and sick building syndrome symptoms in administrative office at public university. Dialogues Health 2024, 4, 100178. [Google Scholar] [CrossRef]
- Sarkhosh, M.; Najafpoor, A.A.; Alidadi, H.; Shamsara, J.; Amiri, H.; Andrea, T.; Kariminejad, F. Indoor Air Quality associations with sick building syndrome: An application of decision tree technology. Build. Environ. 2021, 188, 107446. [Google Scholar] [CrossRef]
- Ghaffarianhoseini, A.; Alwaer, H.; Omrany, H.; Ghaffarianhoseini, A.; Alalouch, C.; Clements-Croome, D.; Tookey, J. Sick building syndrome: Are we doing enough? Archit. Sci. Rev. 2018, 61, 99–121. [Google Scholar] [CrossRef]
- Huo, X.; Sun, Y.; Hou, J.; Wang, P.; Kong, X.; Zhang, Q.; Sundell, J. Sick building syndrome symptoms among young parents in Chinese homes. Build. Environ. 2020, 169, 106283. [Google Scholar] [CrossRef]
- Cheng, H.; Norback, D.; Zhang, H.; Yang, L.; Li, B.; Zhang, Y.; Zhao, Z.; Deng, Q.; Huang, C.; Yang, X.; et al. Home environment exposure and sick building syndrome (SBS) symptoms among adults in southern China: Health associations in 2010 and 2019. Build. Environ. 2024, 248, 111061. [Google Scholar] [CrossRef]
- Marasinghe, S.A.; Sun, Y.; Norback, D.; Adikari, A.M.P.; Mlambo, J. Indoor environment in Sri Lankan university dormitories: Associations with ocular, nasal, throat and dermal symptoms, headache, and fatigue among students. Build. Environ. 2024, 251, 111194. [Google Scholar] [CrossRef]
- Dhungana, P.; Chalise, M. Prevalence of sick building syndrome symptoms and its associated factors among bank employees in Pokhara Metropolitan, Nepal. Indoor Air 2020, 30, 244–250. [Google Scholar] [CrossRef]
- Nakayama, Y.; Nakaoka, H.; Suzuki, N.; Tsumura, K.; Hanazato, M.; Todaka, E.; Mori, C. Prevalence and risk factors of pre-sick building syndrome: Characteristics of indoor environmental and individual factors. Environ. Health Prev. Med. 2019, 24, 77. [Google Scholar] [CrossRef]
- Subri, M.S.M.; Arifin, K.; Sohaimin, M.F.A.M.; Abas, A. The parameter of the Sick Building Syndrome: A systematic literature review. Heliyon 2024, 10, e32431. [Google Scholar] [CrossRef]
- Lu, C.Y.; Tsai, M.C.; Muo, C.H.; Kuo, Y.H.; Sung, F.C.; Wu, C.C. Personal, psychosocial and environmental factors related to sick building syndrome in official employees of Taiwan. Int. J. Environ. Res. Public Health 2018, 15, 7. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Norback, D.; Cheng, H.; Li, B.; Zhang, Y.; Zhao, Z.; Deng, Q.; Huang, C.; Yang, X.; Lu, C.; et al. Dampness and mould in Chinese homes and sick building syndrome (SBS) symptoms—Associations with climate, family size, cleaning and ventilation. Build. Environ. 2023, 245, 1180878. [Google Scholar] [CrossRef]
- Wang, Z.; Liu, J.; Yao, M.; He, M.; Shang, W.; Dong, X. Indoor air quality and sick-building syndrome at a metro station in Tianjin, China. Environ. Int. 2024, 187, 1008673. [Google Scholar] [CrossRef]
- Hosseini, M.R.; Godini, H.; Fouladi-Fard, R.; Ghanami, Z.; Ghafoory, N.; Balali, M.; Faridan, M. Comparing classic regression with credit scorecard model for predicting sick building syndrome risk: A machine learning perspective in environmental assessment. Build. Environ. 2024, 253, 111351. [Google Scholar] [CrossRef]
- Surawattanasakul, V.; Sirikul, W.; Sapbamrer, R.; Wangsan, K.; Assavanopakun, P.; Panumasvivat, J. Perceived draught and odors: The key to SBS and indoor environment in hospital administrative offices—The AIRMED project. Build. Environ. 2024, 258, 111592. [Google Scholar] [CrossRef]
- Qiao, R.; Lou, X.; Sun, Y.; Liu, Y. Effects of occupant behaviors on perceived dormitory air quality and sick building syndrome symptoms among female college students. Indoor Air 2022, 32, e13153. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Li, B.; Yang, Q.; Yu, W.; Wang, H.; Norback, D.; Sundell, J. Odors and sensations of humidity and dryness in relation to sick building syndrome and home environment in Chongqing, China. PLoS ONE 2013, 8, e72385. [Google Scholar] [CrossRef]
- Mizoue, T.; Reijula, K.; Andersson, K. Environmental tobacco smoke exposure and overtime work as risk factors for sick building syndrome in Japan. Am. J. Epidemiol. 2001, 154, 803–808. [Google Scholar] [CrossRef]
- He, Y.; Zhang, S.; Wei, X.; Shang, S.; Wang, Y.; Zhang, R.; Guo, J.; Sun, M.; Li, Y.; Ma, Y. A high environmental composite quality factor score was associated with the risk of sick building syndrome among adults in northeast China. J. Environ. Manag. 2022, 306, 114458. [Google Scholar] [CrossRef]
- Irga, P.J.; Torpy, F.R. Indoor air pollutants in occupational buildings in a sub-tropical climate: Comparison among ventilation types. Build. Environ. 2016, 100, 227. [Google Scholar] [CrossRef]
- Koren, M.; Peto, R. Business disruptions from social distancing. PLoS ONE 2020, 15, e0239113. [Google Scholar] [CrossRef] [PubMed]
- De Haas, M.; Faber, R.; Hamersma, M. How COVID-19 and the Dutch ‘intelligent lockdown’ change activities, work and travel behaviour: Evidence from longitudinal data in the Netherlands. Transp. Res. Perspect. 2020, 6, 100150. [Google Scholar] [CrossRef] [PubMed]
- Mahabee-Gittens, E.M.; Merianos, A.L.; Matt, G.E. Letter to the editor regarding: “An imperative need for research on the role of environmental factors in transmission of novel coronavirus (COVID-19)”-Secondhand and Thirdhand Smoke As Potential Sources of COVID-19. Environ. Sci. Technol. 2020, 54, 5309–5310. [Google Scholar] [CrossRef]
- Hosseini, M.R.; Fouladi-Fard, R.; Aali, R. COVID-19 pandemic and sick building syndrome. Indoor Built Environ. 2020, 29, 1181–1183. [Google Scholar] [CrossRef]
- Awada, M.; Becerik-Gerber, B.; Hoque, S.; O’Neill, Z.; Pedrielli, G.; Wen, J.; Wu, T. Ten questions concerning occupant health in buildings during normal operations and extreme events including the COVID-19 pandemic. Build. Environ. 2021, 188, 107480. [Google Scholar] [CrossRef] [PubMed]
- Roh, T.; Moreno-Rangel, A.; Baek, J.; Obeng, A.; Hasan, N.T.; Carrillo, G. Indoor air quality and health outcomes in employees working from home during the COVID-19 pandemic: A pilot study. Atmosphere 2021, 12, 1665. [Google Scholar] [CrossRef]
- Napoli, P.E.; Nioi, M.; Fossarello, M. The “Quarantine Dry Eye”: The lockdown for coronavirus disease 2019 and its implications for ocular surface health. Risk Manag. Healthc. Policy 2021, 14, 1629–1636. [Google Scholar] [CrossRef]
- Suzhou Bureau of Statistics. Suzhou Statistical Yearbook; Suzhou Bureau of Statistics: Suzhou, China, 2023. [Google Scholar]
- Che, W.W.; Tso, C.Y.; Sun, L.; Ip, D.Y.K.; Lee, H.; Chao, C.Y.H.; Lau, A.K.H. Energy consumption, indoor thermal comfort and air quality in a commercial office with retrofitted heat, ventilation and air conditioning (HVAC) system. Energy Build. 2019, 201, 202–215. [Google Scholar] [CrossRef]
- Suzuki, N.; Nakayama, Y.; Nakaoka, H.; Takaguchi, K.; Tsumura, K.; Hanazato, M.; Hayashi, T.; Mori, C. Risk factors for the onset of sick building syndrome: A cross-sectional survey of housing and health in Japan. Build. Environ. 2021, 202, 107976. [Google Scholar] [CrossRef]
- Hao, D. Survey Methods in Social Research, 4th ed.; China Renmin University Press: Beijing, China, 2019. [Google Scholar]
- Shao, Z.; Bi, J.; Yang, J.; Ma, Z. Indoor PM2.5, home environmental factors and lifestyles are related to sick building syndrome among residents in Nanjing, China. Build. Environ. 2023, 235, 110204. [Google Scholar] [CrossRef]
- Dutheil, F.; Baker, J.S.; Navel, V. COVID-19 as a factor influencing air pollution? Environ. Pollut. 2020, 263, 114466. [Google Scholar] [CrossRef] [PubMed]
- Takigawa, T.; Wang, B.L.; Sakano, N.; Wang, D.H.; Ogino, K.; Kishi, R. A longitudinal study of environmental risk factors for subjective symptoms associated with sick building syndrome in new dwellings. Sci. Total Environ. 2009, 407, 5223–5228. [Google Scholar] [CrossRef] [PubMed]
- Colton, M.D.; MacNaughton, P.; Vallarino, J.; Kane, J.; Bennett-Fripp, M.; Spengler, J.D.; Adamkiewicz, G. Indoor air quality in green vs conventional multifamily low-income housing. Environ. Sci. Technol. 2014, 48, 7833–7841. [Google Scholar] [CrossRef] [PubMed]
- Jarvis, D.L.; Leaderer, B.P.; Chinn, S.; Burney, P.G. Indoor nitrous acid and respiratory symptoms and lung function in adults. Thorax 2005, 60, 474–479. [Google Scholar] [CrossRef] [PubMed]
- Engvall, K.; Norrby, C.; Bandel, J.; Hult, M.; Norback, D. Development of a multiple regression model to identify multi-family residential buildings with a high prevalence of sick building syndrome (SBS). Indoor Air 2000, 10, 101–110. [Google Scholar] [CrossRef]
- Fu, P.; Zhao, Z.; Norback, D.; Zhang, X.; Yung, K.K.L. Associations between indoor environment and lifestyles and sick building syndrome symptoms among adults in Taiyuan and Urumqi of China. Indoor Air 2022, 32, e13081. [Google Scholar] [CrossRef]
- Mckee, K.; Soaita, A.M.; Hoolachan, J. ‘Generation rent’ and the emotions of private renting: Self-worth, status and insecurity amongst low-income renters. Hous. Stud. 2020, 35, 1468–1487. [Google Scholar] [CrossRef]
- Yau, Y.H.; Phuah, K.S. Indoor air quality study in four Malaysian hospitals for centralized and non-centralized ACMV systems. Air Qual. Atmos. Health 2023, 16, 375–390. [Google Scholar] [CrossRef]
- Azuma, K.; Ikeda, K.; Kagi, N.; Yanagi, U.; Osawa, H. Prevalence and risk factors associated with nonspecific building-related symptoms in office employees in Japan: Relationships between work environment, Indoor Air Quality, and occupational stress. Indoor Air 2015, 25, 499–511. [Google Scholar] [CrossRef]
- Rice, J.L.; Brigham, E.; Dineen, R.; Muqueeth, S.; O’Keefe, G.; Regenold, S.; Koehler, K.; Rule, A.; McCormack, M.; Hansel, N.N.; et al. The feasibility of an air purifier and secondhand smoke education intervention in homes of inner city pregnant women and infants living with a smoker. Environ. Res. 2018, 160, 524–530. [Google Scholar] [CrossRef]
- Cooper, E.; Wang, Y.; Stamp, S.; Burman, E.; Mumovic, D. Use of portable air purifiers in homes: Operating behaviour, effect on indoor PM2.5 and perceived indoor air quality. Build. Environ. 2021, 191, 107621. [Google Scholar] [CrossRef]
- Takaoka, M.; Suzuki, K.; Norback, D. Sick building syndrome among junior high school students in Japan in relation to the home and school environment. Glob. J. Health Sci. 2015, 8, 165–177. [Google Scholar] [CrossRef] [PubMed]
- Nevalainen, A.; Pasanen, A.L.; Niininen, M.; Reponen, T.; Kalliokoski, P.; Jantunen, M.J. The indoor air quality in finnish homes with mold problems. Environ. Int. 1991, 17, 299–302. [Google Scholar] [CrossRef]
- Zhang, X.; Li, F.; Zhang, L.; Zhao, Z.; Norback, D. A Longitudinal Study of Sick Building Syndrome (SBS) among Pupils in Relation to SO2, NO2, O-3 and PM10 in Schools in China. PLoS ONE 2014, 9, e112933. [Google Scholar] [CrossRef]
- Luo, N.; Weng, W.; Xu, X.; Hong, T.; Fu, M.; Sun, K. Assessment of occupant-behavior-based indoor air quality and its impacts on human exposure risk: A case study based on the wildfires in Northern California. Sci. Total Environ. 2019, 686, 1251–1261. [Google Scholar] [CrossRef]
| Variables | Total (%) (N = 442) | General Symptoms | Mucosal Symptoms | Skin Symptoms | ||||
|---|---|---|---|---|---|---|---|---|
| Yes (%) | p-Value | Yes (%) | p-Value | Yes (%) | p-Value | |||
| Gender | Male | 200 (45.2) | 62.5% | - | 48.5% | - | 52.5% | - |
| Female | 242 (54.8) | 56.6% | 43.0% | 46.3% | ||||
| Age | 16–25 | 116 (26.2) | 66.4% | - | 46.6% | * | 58.6% | * |
| 26–40 | 155 (35.1) | 52.9% | 36.8% | 40.6% | ||||
| 41–50 | 53 (12.0) | 50.9% | 45.3% | 47.2% | ||||
| 51–60 | 57 (12.9) | 61.4% | 52.6% | 49.1% | ||||
| >60 | 61 (13.8) | 67.2% | 59.0% | 54.1% | ||||
| Occupation | Self-employed | 77 (17.4) | 67.5% | * | 50.6% | - | 57.1% | - |
| Housewife | 14 (3.2) | 71.4% | 35.7% | 50.0% | ||||
| Company employee | 142 (32.1) | 56.3% | 43.7% | 43.0% | ||||
| Student | 57 (12.9) | 64.9% | 40.4% | 54.4% | ||||
| Civil servant | 122 (27.6) | 56.6% | 47.5% | 51.6% | ||||
| Retiree | 23 (5.2) | 60.9% | 60.9% | 47.8% | ||||
| Other | 7 (1.6) | 0.0% | 0.0% | 0.0% | ||||
| Education | Primary school | 26 (5.9) | 73.1% | *** | 42.3% | ** | 61.5% | - |
| Junior high school | 37 (8.4) | 64.9% | 43.2% | 54.1% | ||||
| Senior high school | 54 (12.2) | 79.6% | 64.8% | 55.6% | ||||
| University | 234 (52.9) | 56.0% | 45.7% | 50.0% | ||||
| Postgraduate | 91 (20.6) | 49.5% | 35.2% | 37.4% | ||||
| Monthly household income (CNY) | ≤5000 | 77 (17.4) | 72.7% | * | 58.4% | - | 51.9% | - |
| 5001–10,000 | 129 (29.2) | 59.7% | 43.4% | 48.8% | ||||
| 10,001–20,000 | 138 (31.2) | 57.2% | 42.0% | 50.7% | ||||
| ≥20,001 | 98 (22.2) | 51.0% | 42.9% | 44.9% | ||||
| History of respiratory disease | Yes | 192 (43.4) | 55.6% | - | 42.0% | - | 49.6% | - |
| No | 250 (56.6) | 64.1% | 50.0% | 48.4% | ||||
| Variables | Adjusted Odds Ratio (95% CI) | |||
|---|---|---|---|---|
| General Symptom | Mucosal Symptom | Skin Symptom | ||
| Pollution source | Yes | 10.8 (2.4–48.6) ** | 10.8 (1.4–85.4) * | 7.6 (1.6–36.9) * |
| No | 1.0 | 1.0 | 1.0 | |
| Construction year | Before 1980 | - | 3.9 (1.5–9.7) ** | - |
| 1980–1990 | - | 3.1 (1.4–6.7) ** | - | |
| 1991–2000 | - | 1.8 (0.9–3.7) | - | |
| 2001–2010 | - | 1.3 (0.6–2.8) | - | |
| 2011–now | 1.0 | 1.0 | 1.0 | |
| Ownership | No | - | - | 1.6 (1.0–2.6) * |
| Yes | 1.0 | 1.0 | 1.0 | |
| Use of air freshener | Everyday | 4.9 (2.4–10.0) *** | 5.3 (2.4–11.5) *** | 4.6 (1.6–13.1) ** |
| 1/2–4 days | 3.7 (1.9–7.1) *** | 2.8 (1.4–5.9) ** | 5.3 (2.0–13.9) ** | |
| 1/week | 2.8 (1.2–6.3) * | 4.4 (1.8–10.7) ** | 6.1 (2.3–16.1) *** | |
| >1/week | 1.0 | 1.0 | 1.0 | |
| Use of disinfectant | Everyday | - | - | 1.7 (0.6–4.7) |
| 1/2–4 days | - | - | 2.0 (0.8–5.3) | |
| 1/week | - | - | 4.0 (1.5–10.7) ** | |
| >1/week | 1.0 | 1.0 | 1.0 | |
| Use of air cleaner | Yes | 0.5 (0.3–0.9) * | - | - |
| No | 1.0 | 1.0 | 1.0 | |
| Damp stains | Yes | 1.6 (1.0–2.5) * | - | |
| No | 1.0 | 1.0 | 1.0 | |
| Water damage | Yes | 1.6 (1.0–2.5) * | - | |
| No | 1.0 | 1.0 | 1.0 | |
| Indoor environmental comfort | No | 2.2 (1.2–4.0) ** | 3.1 (1.6–6.0) ** | - |
| Yes | 1.0 | 1.0 | 1.0 | |
| Psychological effect | Yes | 1.3 (1.1–1.7) * | - | - |
| No | 1.0 | 1.0 | 1.0 | |
| SBS Symptoms | Reducing Indoor Smoking (%) | p-Value | Improving Ventilation (%) | p-Value | Using Adsorption Materials or Green Plants (%) | p-Value | Detecting Indoor Air Pollutants (%) | p-Value | Indoor Air Pollution Treatment (%) | p-Value | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| General symptoms | No | 42.3 | ** | 56.8 | *** | 43.5 | * | 34.7 | ** | 32.5 | *** |
| Yes | 57.7 | 43.2 | 56.5 | 65.3 | 67.5 | ||||||
| Mucosal symptoms | No | 54.8 | - | 72.3 | *** | 56.8 | - | 51.5 | - | 46.7 | *** |
| Yes | 45.2 | 27.7 | 43.2 | 48.5 | 53.3 | ||||||
| Skin symptoms | No | 51.7 | - | 64.3 | *** | 53.9 | * | 49.4 | - | 39.2 | *** |
| Yes | 48.3 | 35.7 | 46.1 | 50.6 | 60.8 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shao, Z.; Wu, C.; Shao, Q.; Yang, J.; Xie, M. Prevalence of Sick Building Syndrome Symptoms in Residents During the COVID-19 Pandemic—A Case Study of Suzhou City, China. Buildings 2024, 14, 3388. https://doi.org/10.3390/buildings14113388
Shao Z, Wu C, Shao Q, Yang J, Xie M. Prevalence of Sick Building Syndrome Symptoms in Residents During the COVID-19 Pandemic—A Case Study of Suzhou City, China. Buildings. 2024; 14(11):3388. https://doi.org/10.3390/buildings14113388
Chicago/Turabian StyleShao, Zhijuan, Chenying Wu, Qi Shao, Jie Yang, and Mingjie Xie. 2024. "Prevalence of Sick Building Syndrome Symptoms in Residents During the COVID-19 Pandemic—A Case Study of Suzhou City, China" Buildings 14, no. 11: 3388. https://doi.org/10.3390/buildings14113388
APA StyleShao, Z., Wu, C., Shao, Q., Yang, J., & Xie, M. (2024). Prevalence of Sick Building Syndrome Symptoms in Residents During the COVID-19 Pandemic—A Case Study of Suzhou City, China. Buildings, 14(11), 3388. https://doi.org/10.3390/buildings14113388