Bone Loss in Bruxist Patients Wearing Dental Implant Prostheses: A Finite Element Analysis



 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Dental Implants and Bone Type
- –
- M-12 (Oxtein, Madrid, Spain) is a tapered implant of grade IV titanium with double internal hexagons and an argon-treated surface. It has coronal microthreads, double U-spins in the middle third, and microthreads in the valleys, which increases the contact surface with the bone. This implant has a neck length of 3 mm and includes 6 coarse microthreads with a pitch of 0.3 mm and a depth of 0.15 mm (Figure 1A).
- –
- Astra (Astra Tech, Dentsply Sirona, New York, NY, USA) is a straight implant of grade IV titanium with double internal hexagons and a surface blasted with titanium dioxide and modified with fluorine. This implant has a neck length of 3.7 mm and fine microthreads along the entire neck, which have a pitch of 0.2 mm and a depth of 0.1 mm (Figure 1B).
2.2. Loading Spectrum
2.3. FEA Model
2.4. Constitutive Model
- ψt is the daily stress at the tissue level.
- nc is the number of loading cycles.
- m is the constant that quantifies the importance of the stress state and the number of daily cycles. Based on previous research, it may adopt values between 3 and 8 [39]. The calibration value of our model was 3.
- ρc is the maximum bone density.
- ρ is the apparent density.
- σ is the effective stress at the tissue level.
- ṗ is the derivative of density depending on time. An explicit Euler integration algorithm was used to obtain the state variable associated with it.
- ṙ is the speed of bone remodelling that quantifies the amount of bone formed on the available surface of the bone matrix per unit of time. This variable was not nil when the established threshold was surpassed.
- Su is the specific surface.
- ρt is the tissue density.
3. Results
4. Discussion
5. Conclusions
- All of the hypotheses adopted are representative of simulating the behaviour of the bone-implant interface, which was the study object.
- At the initial stress state of both implants, an overloading occurred on the left part of the cortical bone area at the implant neck, obtaining lower stress levels in the apical region.
- When compared to the Astra model, the M-12 implant allows better dissipation of forces in the neck area (where most forces are concentrated).
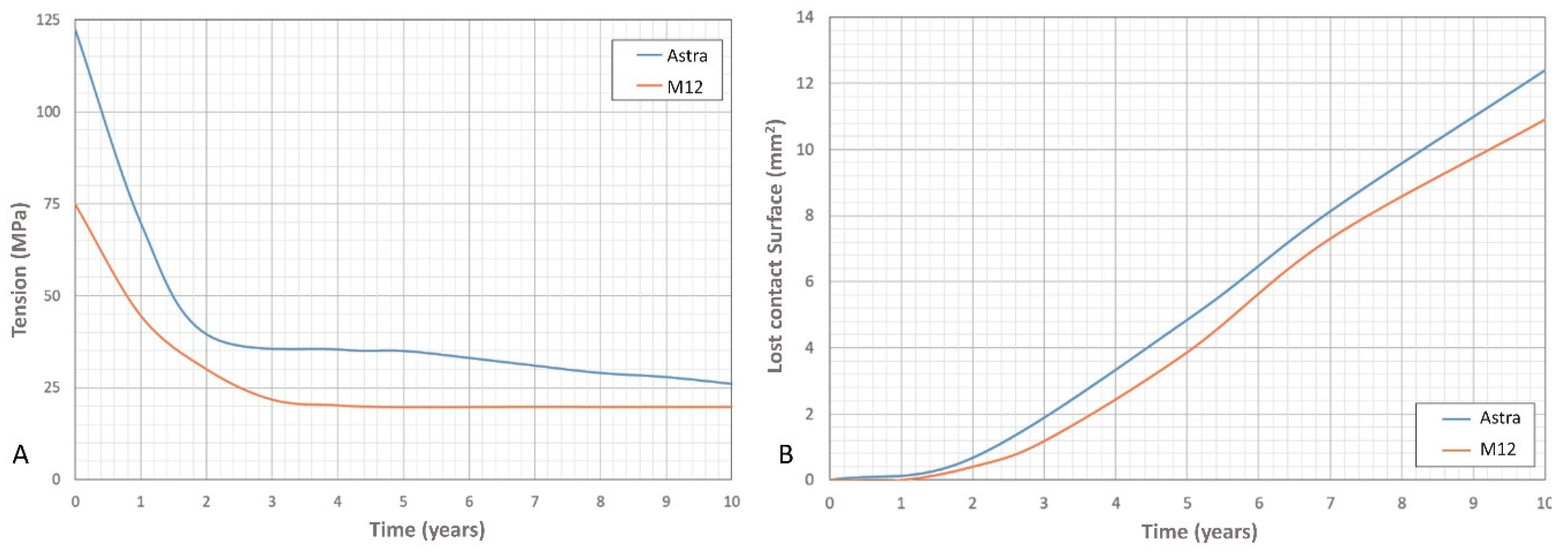
- In the Astra model, the greater sustained stress over time and the contact surface loss observed in the cortical bone around the implant’s neck area may be attributed to the lower contact surface initially achieved at the cervical level of this type of implant when compared to the M-12 implant.
- The higher loss of trabecular bone recorded in the M-12 model may be due to the shape of its bone extraction canals and implant thread. Given that the greater stress peaks were registered in these areas, more prone to bone loss a reduction of the canals and a modification of the implant thread may be suggested to avoid this problem.
- In light of the study results, prostheses placed over M-12 implants may be expected to have more predictable prognosis than those constructed onto Astra implants in bruxist patients.
Author Contributions
Funding
Conflicts of Interest
References
- Afrashtehfar, K.I.; Huynh, N. Five things to know about sleep bruxism. J. N. J. Dent. Assoc. 2016, 87, 14. [Google Scholar] [PubMed]
- Afrashtehfar, K.I.; Afrashtehfar, C.D.M.; Huynh, N. Managing a patient with sleep bruxism. J. Can. Dent. Assoc. 2014, 80, e48. [Google Scholar] [PubMed]
- Casas, E.B.L.; Ferreira, P.C.; Cimini, C.A.; Toledo, E.M.; Barra, L.P.D.S.; Cruz, M. Comparative 3D finite element stress analysis of straight and angled wedge-shaped implant designs. Int. J. Oral Maxillofac. Implant. 2008, 23, 215–225. [Google Scholar]
- Coray, R.; Zeltner, M.; Özcan, M. Fracture strength of implant abutments after fatigue testing: A systematic review and a meta-analysis. J. Mech. Behav. Biomed. Mater. 2016, 62, 333–346. [Google Scholar] [CrossRef] [PubMed]
- Papaspyridakos, P.; Mokti, M.; Chen, C.J.; Benic, G.I.; Gallucci, G.O.; Chronopoulos, V. Implant and prosthodontic survival rates with implant fixed complete dental prostheses in the edentulous mandible after at least 5 years: A systematic review. Clin. Implant. Dent. Relat. Res. 2013, 16, 705–717. [Google Scholar] [CrossRef] [PubMed]
- Palinkas, M.; Marrara, J.; Bataglion, C.; Hallak, J.; Canto, G.D.L.; Scalize, P.H.; Regalo, I.; Siéssere, S.; Regalo, S. Analysis of the sleep period and the amount of habitual snoring in individuals with sleep bruxism. Med. Oral. Patol. Oral. Cir. Bucal. 2019, 24, e782–e786. [Google Scholar] [CrossRef] [PubMed]
- Lobbezoo, F.; Ahlberg, J.; Glaros, A.G.; Kato, T.; Koyano, K.; Lavigne, G.J.; De Leeuw, R.; Manfredini, D.; Svensson, P.; Winocur, E. Bruxism defined and graded: An international consensus. J. Oral Rehabilit. 2013, 40, 2–4. [Google Scholar] [CrossRef]
- Lobbezoo, F.; Brouwers, J.E.I.G.; Cune, M.; Naeije, M. Dental implants in patients with bruxing habits. J. Oral Rehabilit. 2006, 33, 152–159. [Google Scholar] [CrossRef]
- Resnik, R. Misch’s Contemporary Implant Dentistry; Mosby-Elsevier: St Louis, MO, USA, 2020. [Google Scholar]
- Misch, C.E. Dental Implant Prosthetics; Mosby-Elsevier: St Louis, MO, USA, 2015. [Google Scholar]
- Manfredini, D.; Poggio, C.E.; Lobbezoo, F. Is bruxism a risk factor for dental implants? A systematic review of the literature. Clin. Implant. Dent. Relat. Res. 2014, 16, 460–469. [Google Scholar] [CrossRef]
- Huang, H.M.; Tsai, C.M.; Chang, C.C.; Lin, C.T.; Lee, S.Y. Evaluation of loading conditions on fatigue-failed implants by fracture surface analysis. Int. J. Oral Maxillofac. Implant. 2005, 20, 854–859. [Google Scholar]
- Albrektsson, T.; Donos, N.; Working Group Implant Survival and Complications. The Third EAO consensus conference 2012. Clin. Oral Implant. Res. 2012, 23, 63–65. [Google Scholar] [CrossRef] [PubMed]
- Paesani, D.A.; Lobbezoo, F.; Gelos, C.; Nardini, L.G.; Ahlberg, J.; Manfredini, D. Correlation between self-reported and clinically based diagnoses of bruxism in temporomandibular disorders patients. J. Oral Rehabilit. 2013, 40, 803–809. [Google Scholar] [CrossRef] [PubMed]
- Chitumalla, R.; Kumari, K.H.; Mohapatra, A.; Parihar, A.S.; Anand, K.; Katragadda, P. Assessment of survival rate of dental implants in patients with bruxism: A 5-year retrospective study. Contemp. Clin. Dent. 2018, 9, S278–S282. [Google Scholar] [CrossRef] [PubMed]
- Manfredini, D.; Lobbezoo, F. Relationship between bruxism and temporo-mandibular disorders: A systematic review of literature from 1998 to 2008. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, e26–e50. [Google Scholar] [CrossRef]
- Lavigne, G.J.; Khoury, S.; Abe, S.; Yamaguchi, T.; Raphael, K.G. Bruxism physiology and pathology: An overview for clinicians. J. Oral Rehabilit. 2008, 35, 476–494. [Google Scholar] [CrossRef]
- Manfredini, D.; Winocur, E.; Guarda-Nardini, L.; Paesani, D.; Lobbezoo, F. Epidemiology of bruxism in adults: A systematic review of the literature. J. Orofac. Pain 2013, 27, 99–110. [Google Scholar] [CrossRef]
- Behr, M.; Hahnel, S.; Faltermeier, A.; Bürgers, R.; Kolbeck, C.; Handel, G.; Proff, P. The two main theories on dental bruxism. Ann. Anat. Anz. 2012, 194, 216–219. [Google Scholar] [CrossRef]
- Ilovar, S.; Zolger, D.; Castrillon, E.E.; Car, J.; Huckvale, K. Biofeedback for treatment of awake and sleep bruxism in adults: Systematic review protocol. Syst. Rev. 2014, 3, 42. [Google Scholar] [CrossRef]
- De La Hoz-Aizpurua, J.L.; Díaz-Alonso, E.; LaTouche-Arbizu, R.; Mesa-Jiménez, J. Sleep bruxism. Conceptual review and update. Med. Oral Patol. Oral Cir. Bucal. 2011, 16, e231–e238. [Google Scholar] [CrossRef]
- Balshi, T.J. An analysis and management of fractured implants: A clinical report. Int. J. Oral Maxillofac. Implant. 1996, 11, 660–666. [Google Scholar]
- Chrcanovic, B.R.; Kisch, J.; Albrektsson, T.; Wennerberg, A. Bruxism and dental implant treatment complications: A retrospective comparative study of 98 bruxer patients and a matched group. Clin. Oral Implant. Res. 2016, 28, e1–e9. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.E. Contemporary Implantology; Mosby-Elsevier: St Louis, MO, USA, 2009. [Google Scholar]
- Koenig, V.; Wulfman, C.; Bekaert, S.; Dupont, N.; Le Goff, S.; Eldafrawy, M.; Vanheusden, A.; Mainjot, A.K.J. Clinical behavior of second-generation zirconia monolithic posterior restorations: Two-year results of a prospective study with Ex vivo analyses including patients with clinical signs of bruxism. J. Dent. 2019, 91, 103229. [Google Scholar] [CrossRef] [PubMed]
- Pirmoradian, M.; Naeeni, H.A.; Firouzbakht, M.; Toghraie, D.; Khabaz, M.K.; Darabi, R. Finite element analysis and experimental evaluation on stress distribution and sensitivity of dental implants to assess optimum length and thread pitch. Comput. Methods Programs Biomed. 2020, 187, 105258. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Kong, L.; Wang, Y.; Hu, K.; Song, L.; Liu, B.; Li, D.; Shao, J.; Ding, Y. Selection of optimal dental implant diameter and length in type IV bone: A three-dimensional finite element analysis. Int. J. Oral Maxillofac. Surg. 2009, 38, 1077–1083. [Google Scholar] [CrossRef] [PubMed]
- Zarei, I.; Khajehpour, S.; Sabouri, A.; Haghnegahdar, A.Z.; Jafari, K.D. Assessing the effect of dental implants thread design on distribution of stress in impact loadings using three dimensional finite element method. J. Dent. Biomater. 2016, 3, 233–240. [Google Scholar]
- Azcarate-Velázquez, F.; Castillo-Oyagüe, R.; Oliveros-López, L.G.; Torres-Lagares, D.; Martínez-González, Á.-J.; Pérez-Velasco, A.; Lynch, C.D.; Gutiérrez-Pérez, J.L.; Serrera-Figallo, M.A. Influence of bone quality on the mechanical interaction between implant and bone: A finite element analysis. J. Dent. 2019, 88, 103161. [Google Scholar] [CrossRef]
- Sivrikaya, E.C.; Guler, M.S.; Bekci, M.L. A comparative study between zirconia and titanium abutments on the stress distribution in parafunctional loading: A 3D finite element analysis. Technol. Health Care 2020, 10, THC-202305. [Google Scholar] [CrossRef]
- Radaelli, M.T.B.; Idogava, H.T.; Spazzin, A.O.; Noritomi, P.Y.; Boscato, N. Parafunctional loading and occlusal device on stress distribution around implants: A 3D finite element analysis. J. Prosthet. Dent. 2018, 120, 565–572. [Google Scholar] [CrossRef]
- Nishigawa, K.; Bando, E.; Nakano, M. Quantitative study of bite force during sleep associated bruxism. J. Oral Rehabilit. 2001, 28, 485–491. [Google Scholar] [CrossRef]
- UNE-EN ISO 14801:2016. Dentistry—Implants—Dynamic Loading Test for Endosseous Dental Implants; International Organization for Standardization: Geneva, Switzerland, 2017. [Google Scholar]
- Koca, O.L.; Eskitascioglu, G.; Usumez, A.; Eskitaşcıoğlu, G. Three-dimensional finite-element analysis of functional stresses in different bone locations produced by implants placed in the maxillary posterior region of the sinus floor. J. Prosthet. Dent. 2005, 93, 38–44. [Google Scholar] [CrossRef]
- Iplikçioğlu, H.; Akça, K. Comparative evaluation of the effect of diameter, length and number of implants supporting three-unit fixed partial prostheses on stress distribution in the bone. J. Dent. 2002, 30, 41–46. [Google Scholar] [CrossRef]
- Levadnyi, I.; Awrejcewicz, J.; Gubaua, J.E.; Pereira, J.T. Numerical evaluation of bone remodelling and adaptation considering different hip prosthesis designs. Clin. Biomech. 2017, 50, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Tresguerres-Hernández-Gil, I.; Alobera-Gracia, M.A.; Del-Canto-Pingarrón, M.; Blanco-Jerez, L. Physiological bases of bone regeneration II. The remodeling process. Med. Oral Patol. Oral Cir. Bucal. 2006, 11, 151–157. [Google Scholar]
- Hassler, C.R.; Rybicki, E.F.; Cummings, K.D.; Clark, L.C. Quantification of bone stresses during remodeling. J. Biomech. 1980, 13, 185–190. [Google Scholar] [CrossRef]
- Beaupré, G.S.; Orr, T.E.; Carter, D.R. An approach for time-dependent bone modeling and remodeling-theoretical development. J. Orthop. Res. 1990, 8, 651–661. [Google Scholar] [CrossRef]
- Afrashtehfar, K.I.; Afrashtehfar, C.D. Lack of association between overload and peri-implant tissue loss in healthy conditions. Evid. Based Dent. 2016, 17, 92–93. [Google Scholar] [CrossRef]
- Fabris, D.; Souza, J.C.; Silva, F.S.; Fredel, M.; Gasik, M.; Henriques, B. Influence of specimens’ geometry and materials on the thermal stresses in dental restorative materials during thermal cycling. J. Dent. 2018, 69, 41–48. [Google Scholar] [CrossRef]
- Favot, L.M.; Berry-Kromer, V.; Haboussi, M.; Thiébaud, F.; Ben Zineb, T. Numerical study of the influence of material parameters on the mechanical behaviour of a rehabilitated edentulous mandible. J. Dent. 2014, 42, 287–297. [Google Scholar] [CrossRef]
- Lin, C.L.; Chang, S.H.; Wang, J.C.; Chang, W.J. Mechanical interactions of an implant/tooth-supported system under different periodontal supports and number of splinted teeth with rigid and non-rigid connections. J. Dent. 2006, 34, 682–691. [Google Scholar] [CrossRef]
- Oliva Quecedo, J. Modelos de Cálculo Para Solicitaciones Estáticas y Dinámicas en Huesos. Aplicación a la Simulación Mediante Elementos Finitos de Impactos en El Fémur Humano. Ph.D. Thesis, Mecánica de Medios Contínuos y Teoría de Estructuras, Universidad Politécnica de Madrid, Madrid, Spain, 2007. [Google Scholar]
- Chou, H.-Y.; Jagodnik, J.J.; Muftu, S. Predictions of bone remodeling around dental implant systems. J. Biomech. 2008, 41, 1365–1373. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Bruxism and dental implants: A meta-analysis. Implant. Dent. 2015, 24, 505–516. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Kisch, J.; Albrektsson, T.; Wennerberg, A. Bruxism and dental implant failures: A multilevel mixed effects parametric survival analysis approach. J. Oral Rehabilit. 2016, 43, 813–823. [Google Scholar] [CrossRef] [PubMed]
- Chrcanovic, B.R.; Kisch, J.; Albrektsson, T.; Wennerberg, A. Factors influencing the fracture of dental implants. Clin. Implant. Dent. Relat. Res. 2008, 20, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Manfredini, D.; Bucci, M.B.; Bucci-Sabattini, V.; Lobbezoo, F. Bruxism: Overview of current knowledge and suggestions for dental implants planning. Cranio 2011, 29, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Brocard, D.; Barthet, P.; Baysse, E.; Duffort, J.F.; Eller, P.; Justumus, P.; Marin, P.; Oscaby, F.; Simonet, T.; Benqué, E.; et al. A multicenter report on 1,022 consecutively placed ITI implants: A 7-year longitudinal study. Int. J. Oral Maxillofac. Implant. 2000, 15, 691–700. [Google Scholar]
- Moy, P.K.; Medina, D.; Shetty, V.; Aghaloo, T.L. Dental implant failure rates and associated risk factors. Int. J. Oral Maxillofac. Implant. 2005, 20, 569–577. [Google Scholar]
- Meyle, J.; Casado, P.; Fourmousis, I.; Kumar, P.; Quirynen, M.; Salvi, G.E. General genetic and acquired risk factors, and prevalence of peri-implant diseases—Consensus report of working group 1. Int. Dent. J. 2019, 69 (Suppl. 2), 3–6. [Google Scholar] [CrossRef]
- Adell, R.; Lekholm, U.; Rockler, B.; Brånemark, P.-I. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int. J. Oral Surg. 1981, 10, 387–416. [Google Scholar] [CrossRef]
- Cruz, M.; Lourenço, A.F.; Toledo, E.M.; Barra, L.P.D.S.; Lemonge, A.C.D.C.; Wassall, T. Finite element stress analysis of cuneiform and cylindrical threaded implant geometries. Technol. Health Care 2006, 14, 421–438. [Google Scholar] [CrossRef]
- Moeen, F.; Nisar, S.; Dar, N. A step by step guide to finite element analysis in dental implantology. Pak. Oral Dental J. 2014, 1, 164–169. [Google Scholar]
- Keyak, J.; Meagher, J.; Skinner, H.; Mote, C.D., Jr. Automated three-dimensional finite element modelling of bone: A new method. J. Biomed. Eng. 1990, 12, 389–397. [Google Scholar] [CrossRef]
- Huang, H.L.; Huang, J.S.; Ko, C.C.; Hsu, J.T.; Chang, C.H.; Chen, M.Y.C. Effects of splinted prosthesis supported a wide implant or two implants: A three-dimensional finite element analysis. Clin. Oral Implant. Res. 2005, 16, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Winter, W.; Klein, D.; Karl, M. Micromotion of dental implants: Basic mechanical considerations. J. Med. Eng. 2012, 2013, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kong, L.; Liu, B.; Hu, K.J.; Li, D.H.; Song, Y.L.; Ma, P.; Yang, J. Optimized thread pitch design and stress analysis of the cylinder screwed dental implant. Hua Xi Kou Qiang Yi Xue Za Zhi 2006, 24, 509–512. [Google Scholar]
- Bicudo, P.; Reiß, J.; Deus, A.M.; Reis, L.; Vaz, M.F. Mechanical behaviour of dental implants. Procedia Struct. Integr. 2016, 1, 26–33. [Google Scholar] [CrossRef][Green Version]
- Santiago, J.F.; Verri, F.R.; Almeida, D.A.D.F.; De Souza Batista, V.E.; Lemos, C.A.A.; Pellizzer, E.P.; Junior, J.F.S. Finite element analysis on influence of implant surface treatments, connection and bone types. Mater. Sci. Eng. C 2016, 63, 292–300. [Google Scholar] [CrossRef]
- Ao, J.; Li, T.; Liu, Y.; Ding, Y.; Wu, G.; Hu, K.; Kong, L. Optimal design of thread height and width on an immediately loaded cylinder implant: A finite element analysis. Comput. Biol. Med. 2010, 40, 681–686. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bone Density | Description | Anatomical Location |
|---|---|---|
| D1 | Dense corticae | Mandibular anterior area |
| D2 | Porous corticae and thick trabecular | Mandibular anterior area Mandibular posterior area Maxilla anterior area |
| Mandibular posterior area | Porous (thin) corticae and thin trabecular | Maxilla anterior area Maxilla posterior area Mandibular posterior area |
| Maxilla anterior area | Thin trabecular | Maxilla posterior |
| Data Employed in the Numerical Models | Young Module (GPa) | Poisson Coefficient | Density (g/cm3) |
|---|---|---|---|
| Implants | 110 | 0.3 | - |
| Trabecular bone | 1.6 | 0.3 | 0.91 |
| Cortical bone | 13.7 | 0.3 | 1.89 |
| Tooth Surface Loss between Cortical Bone and Implant | Total Surface Area (mm2) | Surface Area Lost | % |
|---|---|---|---|
| M-12 | 18.85 | 10.81 | 57.3 |
| Astra | 18.85 | 12.40 | 65.9 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliveros-López, L.-G.; Castillo-de-Oyagüe, R.; Serrera-Figallo, M.-Á.; Martínez-González, Á.-J.; Pérez-Velasco, A.; Torres-Lagares, D.; Gutiérrez-Pérez, J.-L. Bone Loss in Bruxist Patients Wearing Dental Implant Prostheses: A Finite Element Analysis. Metals 2020, 10, 1132. https://doi.org/10.3390/met10091132
Oliveros-López L-G, Castillo-de-Oyagüe R, Serrera-Figallo M-Á, Martínez-González Á-J, Pérez-Velasco A, Torres-Lagares D, Gutiérrez-Pérez J-L. Bone Loss in Bruxist Patients Wearing Dental Implant Prostheses: A Finite Element Analysis. Metals. 2020; 10(9):1132. https://doi.org/10.3390/met10091132
Chicago/Turabian StyleOliveros-López, Luis-Guillermo, Raquel Castillo-de-Oyagüe, María-Ángeles Serrera-Figallo, Álvaro-José Martínez-González, Andrea Pérez-Velasco, Daniel Torres-Lagares, and José-Luis Gutiérrez-Pérez. 2020. "Bone Loss in Bruxist Patients Wearing Dental Implant Prostheses: A Finite Element Analysis" Metals 10, no. 9: 1132. https://doi.org/10.3390/met10091132
APA StyleOliveros-López, L.-G., Castillo-de-Oyagüe, R., Serrera-Figallo, M.-Á., Martínez-González, Á.-J., Pérez-Velasco, A., Torres-Lagares, D., & Gutiérrez-Pérez, J.-L. (2020). Bone Loss in Bruxist Patients Wearing Dental Implant Prostheses: A Finite Element Analysis. Metals, 10(9), 1132. https://doi.org/10.3390/met10091132