1. Introduction
Rapid urbanization has transformed cities into hubs of economic opportunity and improved living standards, yet it also introduces significant challenges such as environmental degradation, social inequality, and health disparities [
1]. These urban pressures directly affect public health, particularly among vulnerable groups. Understanding patterns of healthcare utilization is therefore essential—not only for strengthening health systems but also for advancing health-related Sustainable Development Goals (SDGs) [
2]. The COVID-19 pandemic has magnified existing vulnerabilities within healthcare systems globally. With over 702 million confirmed cases and nearly 7 million deaths as of January 2025, countries have had to rapidly adapt to unprecedented surges in demand. Hospitals modified workflows, ramped up preventive care, and adjusted their protocols to maintain essential services. Despite these efforts, many individuals chose to delay or avoid healthcare visits due to fear of infection, a trend that reshaped public perceptions of health and access [
3].
Community health status has become an increasingly important focus in both policy and research. As an intermediary layer between national healthcare systems and individuals, community health reflects a complex interplay of local governance, institutional interventions, and individual behavior [
4,
5,
6]. The post-pandemic era has witnessed increased efforts to integrate local actors and community processes into public health strategies, thereby ensuring more resilient and inclusive healthcare delivery systems [
7,
8]. Effective community health governance involves not just health professionals but also social organizations, community leaders, and cross-sector partnerships [
9].
In the contemporary landscape, community health status is acknowledged as a vital metric for attaining universal health coverage and addressing both communicable and non-communicable diseases, marking a new era in healthcare prioritization and policymaking [
10].
In Malaysia, the government implemented Movement Control Orders (MCOs) from March 2020 to December 2021 to reduce viral transmission. While these measures were effective in containing outbreaks, they also disrupted social and economic life, particularly for lower-income and rural populations. These disruptions significantly influenced healthcare-seeking behavior. In Klang Valley, for instance, healthcare utilization dropped substantially during the pandemic [
11]. Healthcare services, which are essential for managing both acute and chronic conditions, have become underutilized, compounding the risks associated with delayed treatment.
Malaysia now faces a dual burden: a surge in Non-Communicable Diseases (NCDs) such as hypertension and diabetes, alongside recurring outbreaks of infectious diseases. This is particularly alarming as nearly 98% of Malaysian adults are reported to have at least one risk factor for NCDs [
12]. In this context, disparities in healthcare access threaten progress toward building equitable and sustainable urban health systems. SDG 11 emphasizes inclusive and safe cities, and equitable access to healthcare is fundamental to achieving this goal.
Urban health systems must respond to population growth while accounting for various health determinants. Numerous studies have identified strong correlations between health outcomes and factors such as genetics, behavior, environment, and healthcare accessibility [
13]. Socioeconomic variables—including age, income, gender, education, disability, and location—further shape the health profiles of different communities [
14]. The Social Determinants of Health (SDH) framework underscores the role of non-medical factors in shaping health outcomes—ranging from early life experiences and employment conditions to social networks and access to services [
15,
16,
17,
18].
In Malaysia, low levels of healthcare utilization are not solely due to infrastructural limitations. Behavioral and psychological factors, especially fear of infection and lack of trust, have also influenced individuals’ decisions to seek care during the pandemic [
19]. For patients with chronic conditions, such as kidney disease, treatment avoidance can have life-threatening consequences [
20]. These behavioral shifts highlight the need for targeted interventions to rebuild confidence in healthcare systems and promote preventive health-seeking behaviors.
This study investigates the relationship between sociodemographic characteristics and healthcare utilization during the COVID-19 pandemic in Penang, Malaysia. Penang represents a dynamic urban setting where public health challenges intersect with rapid urban development and demographic diversity. By applying Andersen’s behavioral model of health service use, the research examines how factors such as age, income, education level, self-rated health, illness status, and perceived community health influence individuals’ use of healthcare services.
The findings contribute to a more nuanced understanding of healthcare utilization in the Malaysian context, particularly in urban communities navigating post-pandemic recovery. By identifying key predictors of health-seeking behavior, the study offers actionable insights for healthcare providers and policymakers aiming to improve service delivery and address inequalities. Special attention is given to the aging population, which faces unique vulnerabilities and increasing healthcare demands.
In doing so, this research supports broader goals of enhancing community resilience, ensuring equitable access to healthcare, and strengthening urban health systems as part of Malaysia’s SDG commitments.
2. Inequalities and Healthcare Utilization in Malaysia
Despite Malaysia’s dual public–private healthcare system and commitment to Universal Health Coverage (UHC), socio-economic inequalities remain widespread in healthcare utilization. These disparities—across access, quality, timeliness, and type of care—are influenced by income, education, geography, and ethnicity [
21,
22].
Private health insurance (PHI) uptake is skewed toward higher-income groups. In 2019, only 22% of Malaysians had PHI, with older adults, women, Malays, rural residents, and those with less education least likely to be covered [
23] (Folayan et al., 2024). This contributes to unequal health outcomes, as PHI holders are more likely to receive timely diagnoses and better manage chronic conditions like hypertension and diabetes [
23,
24].
Healthcare access is further limited by geography. Rural and suburban populations face long travel distances, transport costs, and medical staff shortages [
25]. While mobile clinics and telemedicine exist, coverage in remote areas like Sabah and Sarawak is insufficient [
26].
Regional disparities in life expectancy illustrate deeper structural gaps. Males born in Kuala Lumpur live five years longer than those in Kelantan or Perlis [
27]. Education also plays a role; those with higher health literacy are more likely to seek care [
28]. Cultural factors intersect with economic status—urban poor women from marginalized ethnicities often turn to alternative medicine due to cost and cultural beliefs [
29].
While the WHO recommends that out-of-pocket (OOP) payments account for only 15–20% of total health expenditure, Malaysian households continue to bear a disproportionately high burden, with OOP spending constituting approximately 30–40% of total healthcare costs [
22,
30]. Public health spending remains at ~2% of GDP—well below the WHO’s 5–6% recommendation [
31]. Programs like PeKa B40 and mySalam are fragmented and often exclude informal workers and retirees [
21,
22,
28].
While this study focuses on health inequalities, it is important to distinguish them from inequities—unjust and avoidable differences [
31]. Bridging these gaps requires comprehensive reforms in health financing, stronger political will, and inclusive policies that ensure access for vulnerable populations. In conclusion, socio-economic inequalities in Malaysia are deeply embedded in patterns of healthcare utilization. They are driven by structural and systemic barriers—such as financing models and geographic disparities—as well as individual-level disadvantages like income, education, gender, and ethnicity. Addressing these gaps will require targeted, inclusive, and well-coordinated reforms to ensure that healthcare access truly becomes universal.
2.1. COVID-19 and Healthcare Utilization
The post-COVID-19 era presented both challenges and opportunities for urban health systems. The pandemic has laid bare the vulnerabilities of healthcare systems, particularly impacting marginalized populations like urban slum-dwellers [
32]. In India, enhancing the health infrastructure in small to medium-sized cities is imperative for fortifying the public health framework [
33]. Moreover, there is a pressing need to elevate housing infrastructure and conceptualize housing as a form of non-institutional care infrastructure [
34]. This paradigm shift can complement healthcare infrastructure and foster more inclusive, healthy, and resilient housing systems [
35]. The crisis underscores the significance of revisiting the social function of urban property and integrating it into urban planning and governance [
36]. Consequently, reimagining public health in the post-pandemic city offers an opportunity to spatially integrate health considerations and promote healthy social interactions.
The COVID-19 pandemic has significantly impacted healthcare utilization within communities worldwide. Research findings shed light on the extent of this impact across various regions. In Korea, Lee and You [
3] observed that areas with a high prevalence of COVID-19 cases experienced a pronounced decrease in healthcare service utilization among residents. Similarly, findings from Malaysia by Yunus, Puteh, Ali and Daud [
11] indicate that a substantial 80.5% of respondents avoided utilizing public healthcare services during the pandemic. Furthermore, both hospital admission rates and specialist visits saw a notable decline. In Germany, Michalowsky et al. [
37] noted a significant 39% reduction in hospital admissions during the early 2020 lockdown period. Mansfield et al. [
38] also corroborate these trends, reporting a decrease in healthcare utilization amid the pandemic situation.
These studies collectively underscore the widespread impact of the COVID-19 pandemic on healthcare service utilization, with communities worldwide exhibiting avoidance behaviors and decreased rates of hospital admissions and specialist visits during the crisis. Numerous studies have highlighted the significant impact of sociodemographic factors on healthcare utilization patterns [
39,
40,
41,
42]. In this study, we explored sociodemographic variables such as gender, age, ethnicity, educational level, occupation, and monthly household income as key determinants influencing the utilization of healthcare services. Sociodemographic factors are known to exert considerable influence on healthcare utilization trends.
Gender, for instance, serves as a prominent predisposing factor affecting healthcare service utilization. Research by Michalowsky, Hoffmann, Bohlken, and Kostev [
37] revealed that in Germany, 53.2% of hospital visits for medical treatment were made by females, indicating a higher utilization rate compared to males. Similarly, findings from Hungary indicated that women tend to utilize health services more frequently than men [
43]. This trend is partly attributed to factors such as pregnancy, which necessitates regular hospital visits for check-ups [
44]. These findings underscore the importance of considering sociodemographic factors, particularly gender, in understanding healthcare utilization patterns, thereby informing targeted interventions and healthcare policies tailored to diverse demographic groups.
Lastly, need factors, such as chronic illness, play a crucial role in influencing healthcare utilization within the community. Patients grappling with chronic conditions often exhibit a reduction in medical follow-up during periods of lockdown or heightened health crises. Research by various researchers [
37,
38,
43] underscores this trend, indicating that despite the overall decrease in hospital visits during the pandemic, individuals with chronic diseases continued to seek medical care. This underscores the strong association between health status and healthcare service utilization.
Examining past studies, we can employ behavioral models of health services to explore the association between sociodemographic factors and healthcare utilization. Consequently, understanding the intricate relationships among these variables becomes imperative in deciphering healthcare utilization patterns within the selected study area.
By unraveling the complex interplay between sociodemographic characteristics, health needs, and healthcare utilization behaviors, researchers can gain deeper insights into the dynamics shaping healthcare access and utilization within communities. This holistic understanding is pivotal for designing targeted interventions and policies aimed at enhancing healthcare delivery and addressing disparities in access and utilization across diverse demographic groups.
2.2. COVID-19 in Penang
On 25 January 2020, Malaysia reported its first COVID-19 case, linked to three Chinese nationals with prior contact in Singapore. Despite swift guidelines from the Ministry of Health (MOH), Malaysia confirmed its first positive case on 4 February 2020. Subsequently, Penang and other states reported initial cases in March 2020. Responding to rising cases, the Malaysian government imposed the Movement Control Order (MCO) on 16 March 2020, when cases reached 553. Additionally, it enacted three subsequent orders, Conditional Movement Control Order (CMCO), Recovery Conditional Movement Control Order (RCMCO), and Restricted Movement Control Order (RMCO), to curb further outbreaks.
As of 24 February 2024, Malaysia has recorded a total of 5,275,667 COVID-19-positive cases and 45,289 deaths (
Scheme 1). Penang state, with 10.9 positive cases per 100,000 population, ranks ninth among states, while average Malaysia as a whole has 12.3 positive cases per 100,000 population. The five most affected states, based on positive cases per 100,000 population, are Putrajaya (51.2), W.P. Kuala Lumpur (38.4), Terengganu (22.3), Melaka (21.3), and Perlis (19.0) [
45].
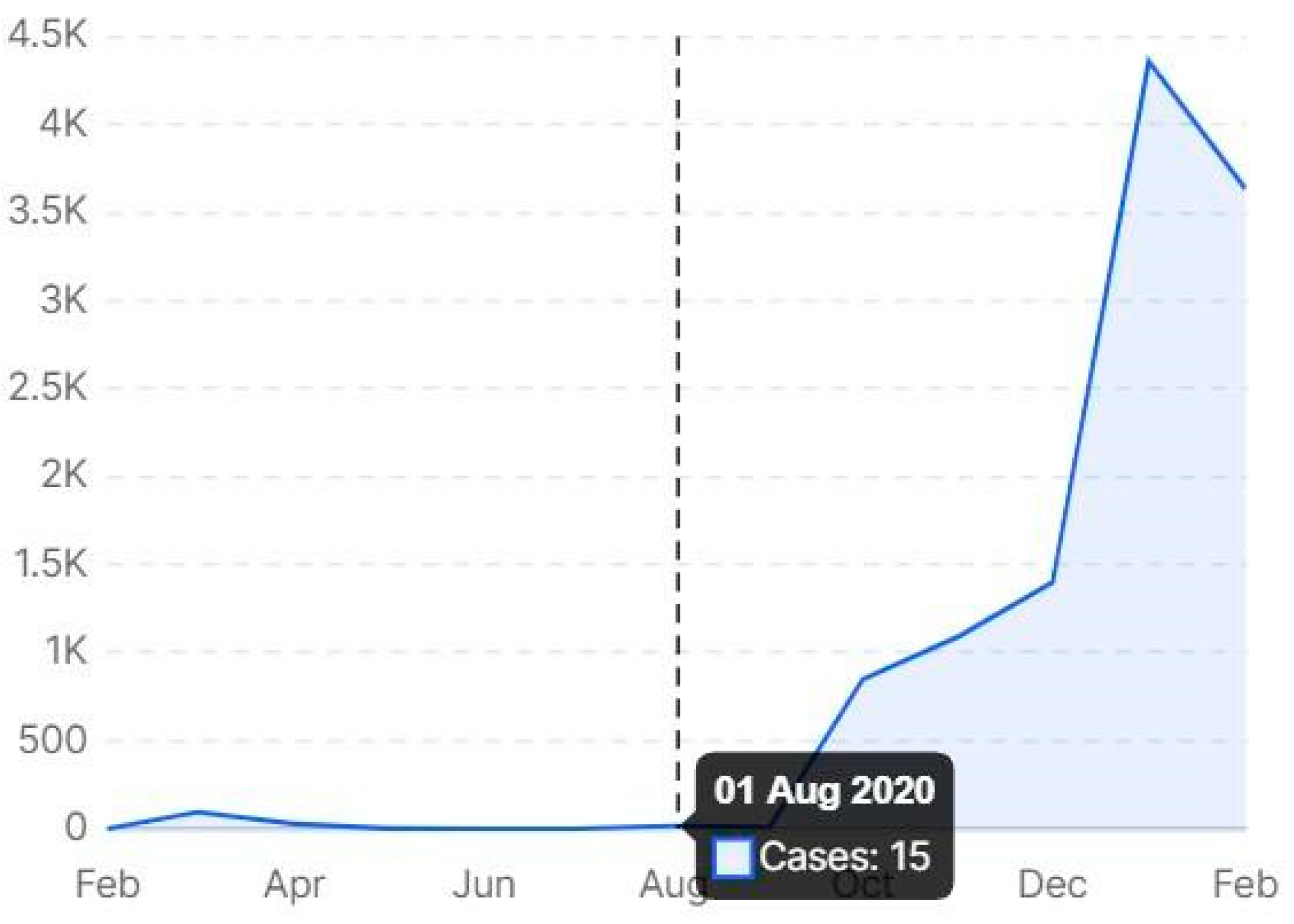
Despite Penang’s three-month streak without any new infections from May 2020 to August 2020, earning it the distinction of being the only state in Malaysia with a green status, the state was once again on alert following the emergence of new cases since August 2020 as shown in
Scheme 2.
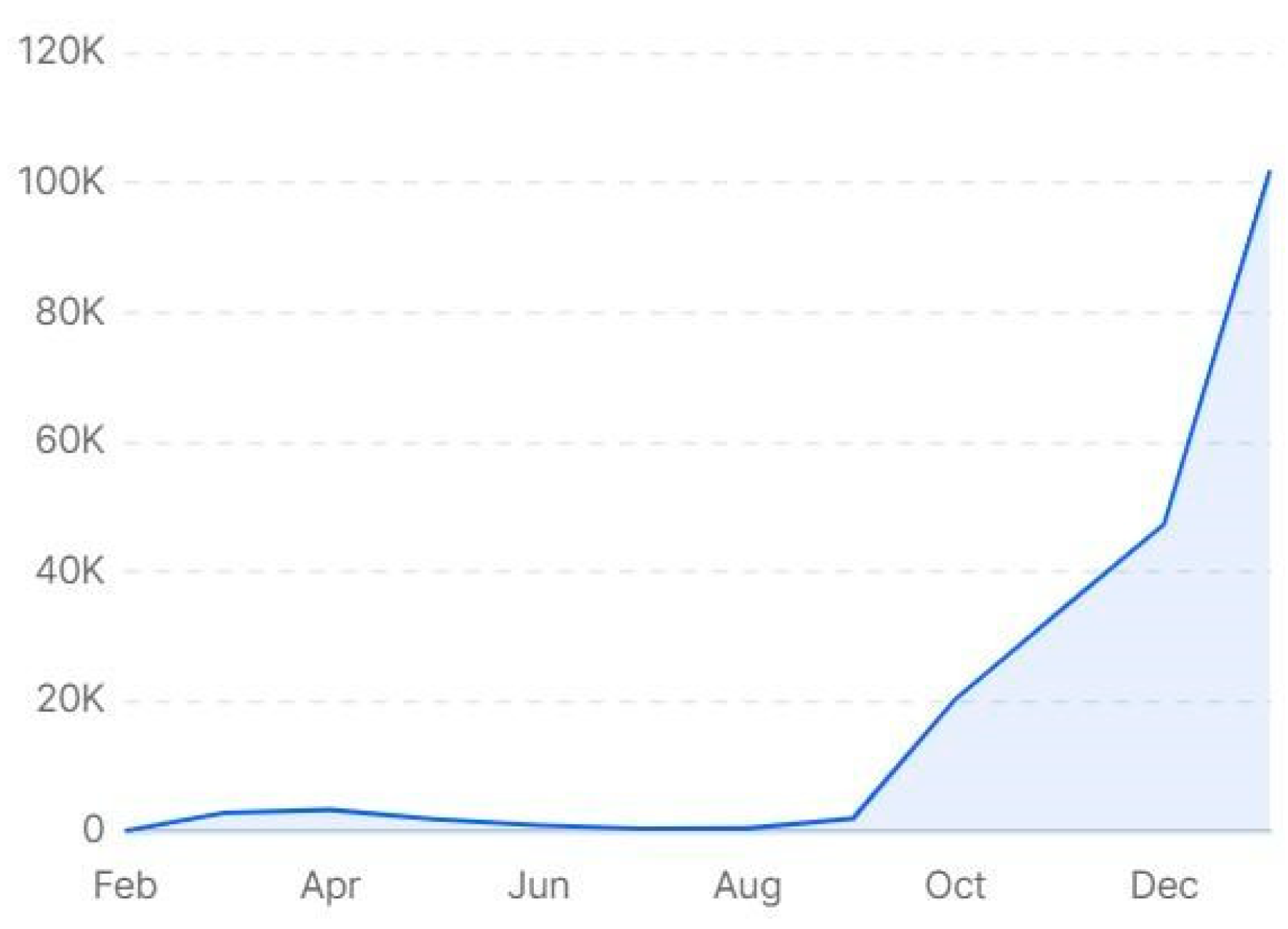
As shown in
Scheme 3, Malaysia faced the third wave of COVID-19 in October 2020, significantly impacting various regions, including Penang. Between November 2020 and February 2021, the wave intensified, leading to the emergence of two major COVID-19 clusters in Penang. Infections rose from 851 cases on 25 October to 1809 by 25 November, and further escalated to 3106 by 25 December 2020.
Despite the implementation of strict movement and activity restrictions by authorities, shopping malls, night markets, and wet markets continued to operate largely without disruption. Challenges persisted, however. On 13 November 2020, a wet market was ordered to close for 14 days after a trader was suspected of contracting COVID-19. Although frequent sanitization measures were carried out, market operations remained largely unaffected [
46].
3. Theoretical Background
The primary goal of this study is to investigate healthcare utilization in Penang, Malaysia, during the COVID-19 pandemic, with a particular focus on the factors influencing the demand for healthcare services and the public’s health-seeking behavior. To achieve this, the study adopts a conceptual framework grounded in Andersen’s Behavioral Model of Health Services Utilization. Although introduced over 25 years ago, this model remains a cornerstone in public health research, widely used for its ability to capture the complex interplay of individual and contextual determinants of healthcare use.
According to Andersen [
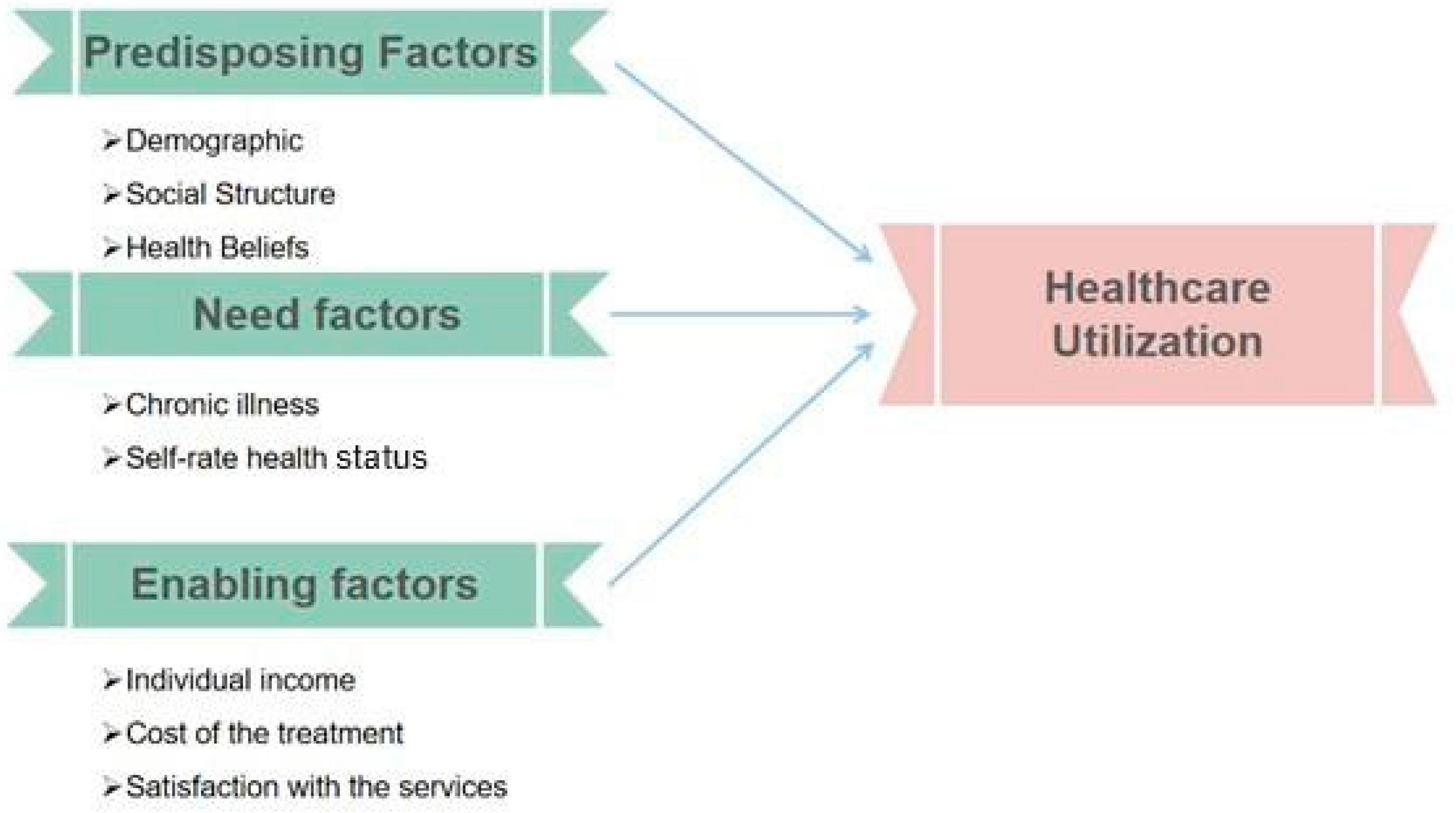
47], an individual’s likelihood of utilizing healthcare services is shaped by a combination of predisposing characteristics, enabling or limiting conditions, and perceived or evaluated needs. These components together form the foundation for understanding health-seeking behavior, as illustrated in
Figure 1.
More specifically, the behavioral model is structured around three primary components: predisposing, need, and enabling factors [
48]. To fully comprehend the drivers of healthcare service utilization, it is essential to explore each of these categories in greater depth.
Predisposing factors refer to an individual’s demographic and social characteristics, such as gender, age, ethnicity, education level, and health attitudes or knowledge, that influence the propensity to seek care [
49,
50]. These attributes shape individuals’ views on health and their perceived importance of seeking professional medical help.
Need factors, on the other hand, capture how individuals assess their own health status or illness symptoms, whether perceived or professionally evaluated. These assessments often play a decisive role in determining whether healthcare is sought [
51]. Enabling factors encompass the logistical and financial conditions that either facilitate or hinder access to care, including income, treatment costs, satisfaction with services, and geographic accessibility [
52].
In this study, Andersen’s model is employed to examine the impact of COVID-19 on healthcare-seeking behavior among vulnerable communities in Malaysia. The model, which has been expanded and refined over the years, offers a robust framework for investigating how sociodemographic, economic, and health-related factors interact to influence care-seeking during times of crisis [
52,
53]. Notably, Andersen’s model has evolved to incorporate feedback loops and broader contextual elements, including consumer satisfaction, health practices, and environmental influences, thus enhancing its relevance in modern healthcare research [
47,
49,
53].
Given the far-reaching social and economic effects of COVID-19, it is critical to adopt a comprehensive framework that includes both objective indicators (such as income or education) and subjective experiences (such as fear or perceived health risks). In light of these considerations, Andersen’s model—especially in its expanded form that incorporates contextual and individual characteristics—is well-suited to guide this study.
Accordingly, the model is applied to analyze healthcare utilization across four thematic dimensions: socioeconomic and demographic factors, individual-level variables, health beliefs, and institutional-level factors. These categories are examined in detail in the sections that follow, offering a structured pathway to assess healthcare-seeking behavior during the COVID-19 pandemic in Penang.
3.1. Predisposing Factors
The Andersen model identifies predisposing factors as inherent individual characteristics that exist prior to the onset of illness and significantly influence health-related behaviors. These factors include demographic attributes such as age, gender, and marital status, as well as broader societal elements like education, occupation, and ethnicity [
49]. Together with enabling and need factors, predisposing factors form one of the three primary determinants of health service utilization within the model.
Empirical studies have demonstrated that predisposing factors exert varying degrees of influence on healthcare behavior and service use. For example, in a study on college students’ access to on-campus mental health services, predisposing factors accounted for approximately 9% of the variance in service utilization decisions [
54]. Likewise, research conducted in Korea has highlighted the importance of factors such as sex, age, and marital status in predicting outpatient health service use [
55].
However, the influence of predisposing factors is not uniform across all health-related behaviors. In some contexts, such as academic performance outcomes linked to health issues, enabling factors have been shown to play a more prominent role, suggesting that the impact of predisposing factors may be more indirect or context-specific [
56]. This variability is echoed across numerous applications of the Andersen model, where the strength and direction of associations between predisposing factors and health service use often differ due to variations in study settings and population characteristics [
57].
The relevance of predisposing factors has also been observed in the context of COVID-19 care. For instance, patient-identified barriers and facilitators to ongoing treatment and antiretroviral therapy adherence reflect all domains of the Andersen model, including predisposing factors. This reinforces the notion that predisposing characteristics remain integral to understanding the complex behaviors that govern healthcare decisions during public health crises [
58].
In summary, existing literature underscores the foundational role of predisposing factors in shaping individuals’ orientation toward healthcare utilization. Characteristics such as higher education levels, older age, marital status, and unemployment have been positively associated with increased use of health services [
59]. Further, macro-level indicators like illiteracy rates and GDP per capita have been found to correlate with outpatient visit frequencies [
60]. Cultural dimensions—such as media exposure and previous hospitalization experience—also influence healthcare behavior, particularly in specific populations like American Indian women [
60,
61]. Collectively, these findings illustrate how predisposing factors establish a baseline understanding of individuals’ attitudes, beliefs, and social contexts that ultimately shape health-seeking behavior and service utilization.
3.2. Needs Factors
Within the Andersen model,
need factors refer to an individual’s perceived or evaluated necessity for healthcare services based on their health condition. These factors are central to understanding health behaviors, as they directly shape one’s motivation to seek medical care. Several studies have highlighted key need-related variables such as illness severity, overall health status, and hospitalization experience [
60,
62], which significantly influence healthcare utilization decisions.
For instance, individuals reporting higher levels of illness severity or poorer health status are generally more likely to perceive a stronger need for medical attention, thereby increasing the probability of seeking healthcare services. Likewise, those with prior hospitalization experience often possess greater awareness of their health needs and are correspondingly more inclined to utilize available healthcare resources.
Although need factors may not always be the dominant predictors across all outcomes, their influence remains substantial. For example, a study on college students found that while need factors were not the strongest predictors of academic performance impacts related to health, they still held notable relevance [
54]. A systematic review of longitudinal studies further supports this, showing consistent associations between poor self-rated health, chronic conditions, and higher levels of healthcare use [
63]. This pattern is especially pronounced in studies involving the elderly. Research has consistently identified need factors as the most significant predictors of various healthcare services among older populations [
64].
In the domain of oral health, variables such as the number of decayed or unsound teeth and perceived need for treatment have been linked to both personal health behaviors and overall oral health outcomes [
50]. Moreover, studies among veteran populations have shown that need factors, when combined with predisposing and enabling variables, provide a more comprehensive explanation of both medical and mental health service utilization [
65]. Perceived treatment needs in oral healthcare were also found to be shaped by prior unmet needs and self-perceptions of inferior oral health compared to peers [
66]. In summary, need factors play a critical role in the Andersen model as they represent the most immediate and tangible drivers of healthcare-seeking behavior. By reflecting both subjective perceptions and objective indicators of health, these factors consistently correlate with increased healthcare utilization across a range of populations and health conditions.
3.3. Enabling Factors
In the Andersen model, enabling factors refer to the resources, conditions, and opportunities that support or hinder an individual’s ability to access and utilize healthcare services. These include both personal and community-level resources, such as having a regular healthcare provider or access to health insurance. For example, individuals with a personal doctor or nurse, or those with non-Medicaid insurance, are more likely to receive timely medical care [
67].
A review of the literature identifies a wide range of enabling factors that contribute to health-seeking behavior. These include higher education, improved health knowledge, access to media such as TV and radio for health literacy, prior hospitalization experience, government subsidies for health screening, distribution of informational booklets, and frequent doctor visits—defined as five or more visits in the previous year [
56,
67,
68]. Collectively, these elements enhance individuals’ ability to engage with the healthcare system by providing essential support, information, and access.
For instance, a study on healthcare utilization in Korea found that enabling factors, such as education level, economic engagement, and insurance type, were significantly associated with inpatient service use. However, their explanatory power was somewhat lower compared to predisposing and need factors [
64]. Still, higher education and awareness were shown to empower individuals to make more informed choices about health screenings [
56,
60]. Similarly, access to government-subsidized screening and informational materials was linked to greater participation in preventive healthcare services [
60], Furthermore, having a dedicated healthcare provider and non-Medicare insurance coverage was associated with increased likelihood of accessing medical care [
48,
69].
Among vulnerable populations, particularly the elderly, enabling factors are often examined in conjunction with predisposing and need factors to provide a more holistic understanding of healthcare utilization patterns. This integrated perspective highlights the importance of considering all three constructs of the Andersen model simultaneously when analyzing access to and engagement with healthcare services [
70].
3.4. Fear of COVID-19
The fear of COVID-19 played a pivotal role in shaping healthcare utilization patterns during the pandemic. Perceptions of healthcare facilities as high-risk zones for virus transmission led to widespread avoidance of care, especially in residential areas severely impacted by the virus. Many individuals, particularly among married populations, opted to forgo primary healthcare services during lockdowns due to concerns over potential exposure [
3]. This behavioral shift, driven by uncertainty and heightened anxiety, illustrates how fear overrode even urgent medical needs.
The influence of fear extended beyond general avoidance, contributing to a marked decline in hospital admissions and specialist visits. For instance, hospital admissions dropped by 39%, while visits to General Practitioners (GPs) and specialists decreased by 6% [
37]. Patients managing chronic illnesses such as diabetes, ischemic heart disease, and depression were especially vulnerable, as many delayed or skipped routine care—ultimately worsening their conditions. Nevertheless, certain subgroups, including older adults, women, and individuals with chronic diseases, were more likely to continue accessing healthcare services [
43]. This may reflect a heightened awareness of the risks of neglecting ongoing health issues despite the pandemic.
Importantly, the fear of COVID-19 often outweighs perceived medical need, leading to significant delays in care and interruptions in disease management. Addressing these fear-driven behaviors requires a multifaceted approach: rebuilding trust in healthcare systems, improving communication about infection control and safety protocols, and providing accessible alternatives such as telehealth.
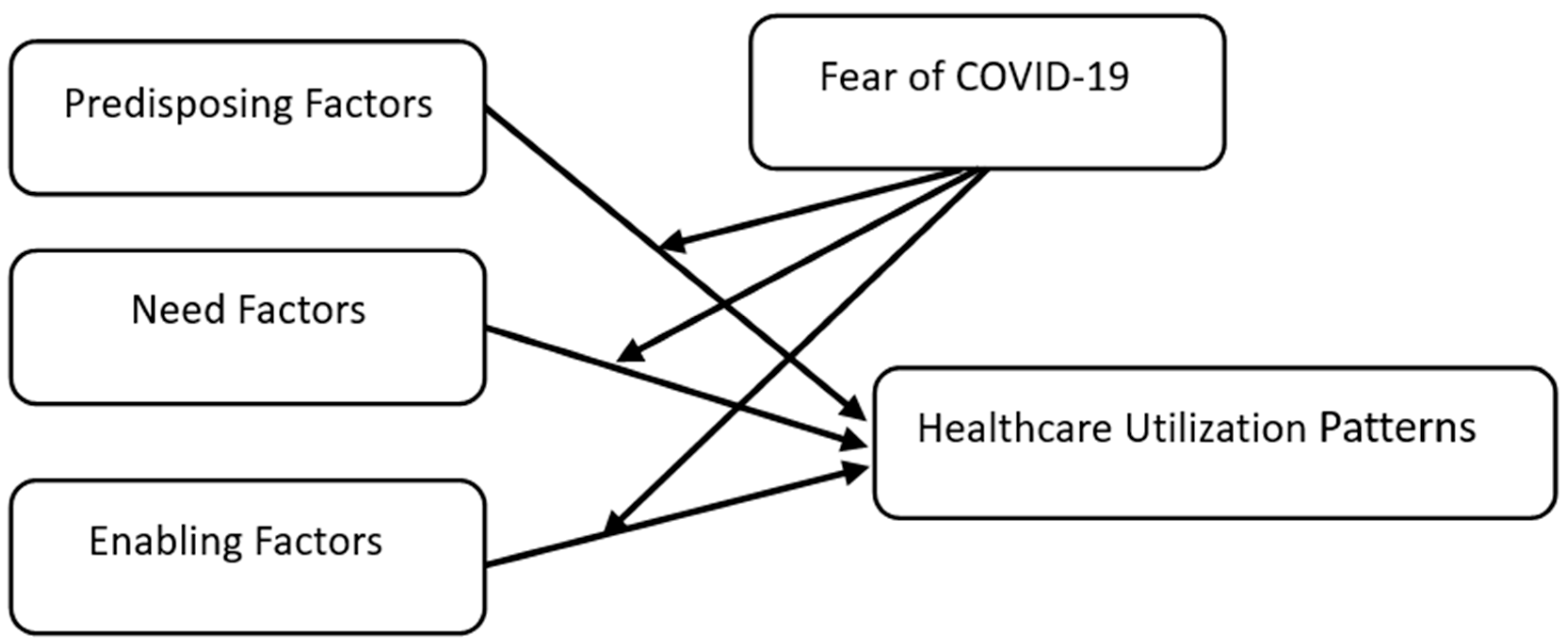
Considering these dynamics, and drawing upon the components of Andersen’s Behavioral Model, the proposed research framework is illustrated in
Figure 2 below.
In line with Andersen’s Behavioral Model, our model argues that the Healthcare Utilization Patterns (HUP) dimensions are associated with the three dimensions. Three hypotheses are developed in this article:
H1: Predisposing Factors (PF), Need Factors (NF), Enabling Factors (EF), and Healthcare Utilization Patterns (HUP) are significantly correlated.
H2: Predisposing Factors (PF), Need Factors (NF), and Enabling Factors (EF) significantly predict variations in Healthcare Utilization Patterns (HUP).
H3: The fear of COVID-19 significantly moderates the relationship between Predisposing Factors (PF), Need Factors (NF), Enabling Factors (EF), and Healthcare Utilization Patterns (HUP).
4. Method and Material
This study investigates the interplay between sociodemographic factors and healthcare utilization during the COVID-19 pandemic in Malaysia, with a specific focus on Penang Island. Using a quantitative approach, the research aims to clarify how individual vulnerability influenced healthcare utilization patterns throughout the pandemic. To address the research objectives, a closed-ended questionnaire was developed to assess respondents’ attitudes, experiences, and perceptions regarding healthcare utilization between 2021 and 2022. The questionnaire, distributed randomly, achieved a 58% response rate, with responses collected from 364 individuals who had resided in Penang between 2019 and 2022 and had experience with public healthcare services before and after the onset of COVID-19.
Quantitative analysis methods, including descriptive and correlational techniques, were applied to the data from 211 randomly selected respondents. This descriptive-correlational study explores the relationships between key research variables through hypothesis testing. Data analysis was conducted using SmartPLS 4 software, which supports the development of measurement models and evaluates variable relationships through parameter estimation, correlation analysis, and significance testing.
4.1. Questionnaire
For the data collection phase, residents of Penang Island were asked to complete a self-administered questionnaire. The survey was conducted in November 2022. To be eligible, participants were required to have lived on Penang Island for at least one year prior to the onset of COVID-19 and be above 18 years of age, ensuring they could make independent decisions rather than relying on advice from family or friends.
A probability sampling method was employed, with respondents selected at random. Babbie [
71] emphasized that probability sampling enables statistical generalization to a larger population. Out of 410 questionnaires distributed to households, 238 were returned, yielding a response rate of 58%. After data cleaning, 27 responses were excluded due to incompleteness, inadequate answers, or failure to meet inclusion criteria, resulting in a final sample of 211 valid respondents.
The first section of the questionnaire collected demographic data. The remaining 23 items focused on respondents’ healthcare needs, health-seeking behaviors, community health engagement, prevalence of chronic illness, self-rated health status, self-medication frequency in the past 12 months, and fear of COVID-19.
Of the 211 respondents, 54.97% were male and 45.03% female. The ethnic breakdown was 46.4% Malay, 38.9% Chinese, and 14.7% Indian. In terms of age, 28% were aged 18–29, 41.2% were 30–49, and 30.8% were over 50, categorizing them as part of the aging population. Hence, the majority of respondents were youth, predominantly of Malay ethnicity.
Marital status revealed that 42.7% were married, 41.2% single, and 16.1% divorced, separated, or widowed. In terms of employment, most respondents were engaged in full-time work (58.8%), with 1.4% employed part-time.
Regarding monthly household income, the majority of participants belonged to the lower-income (B40) category, with 14.2% reporting earnings below RM 999. In contrast, only 10.4% reported earning over RM 4850 per month, classifying them within the middle-income (M40) and upper-income (T20) groups [
72].
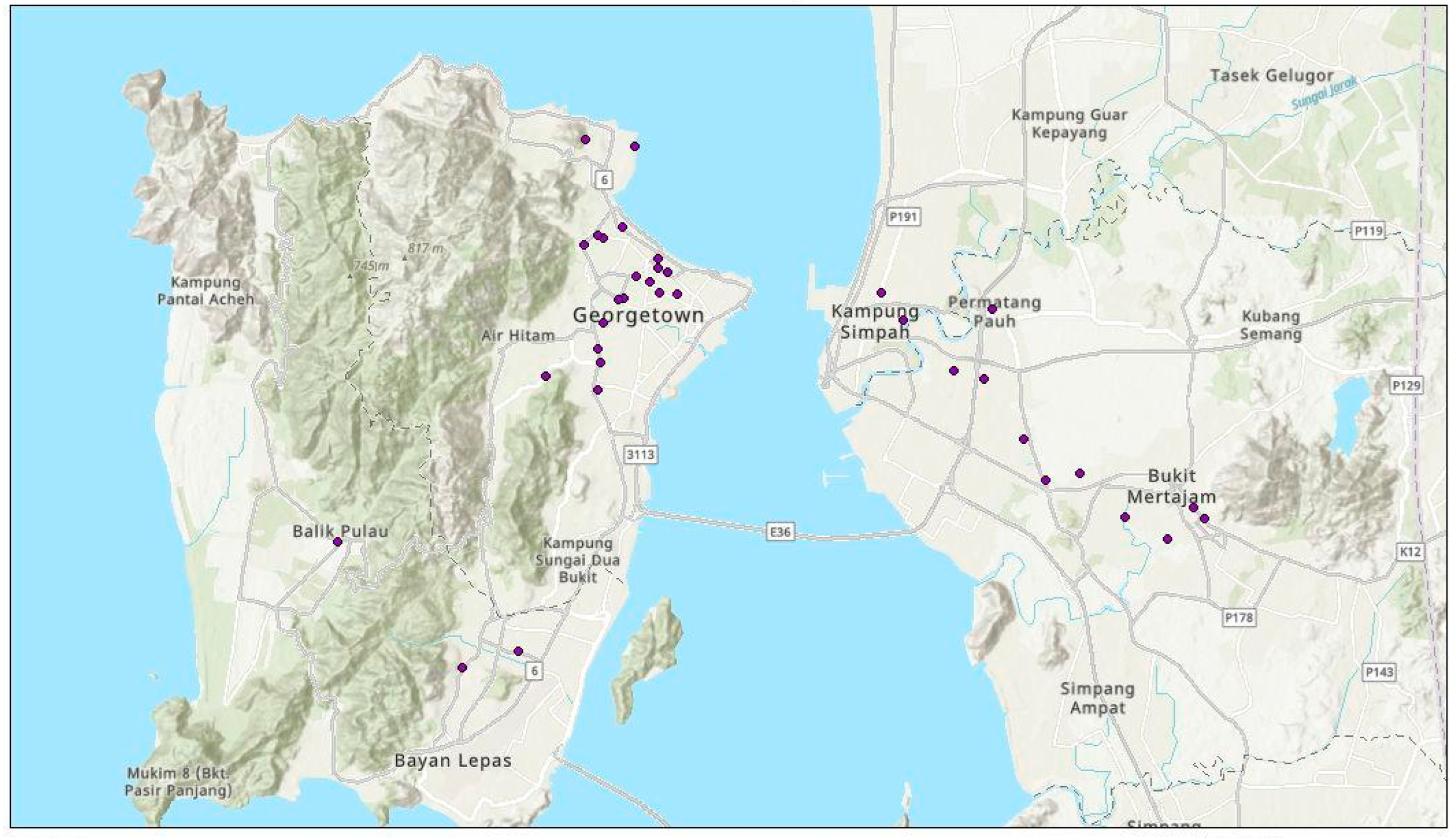
4.2. Study Area
The study was conducted in Penang, Malaysia, situated in the northwestern region of Peninsular Malaysia, which is the second smallest state in the country by land mass and has been ranked as the second highest state in tax collection after Sarawak. George Town serves as the capital city of Penang. As of 2021, Penang’s estimated population stands at 1.77 million, and it has a total area of 1049 km
2 [
72]. The urbanization trend in Penang has led to a rapid increase in both population numbers and the establishment of health facilities. According to the Penang State Health Department [
73], Penang is home to 23 hospitals, comprising 6 government hospitals and 17 private hospitals. Additionally, the region boasts approximately 696 health clinics, including both public and private facilities. Illustrated in
Figure 3, the majority of hospitals are concentrated in Georgetown, which exhibits the highest population density within Penang state. Georgetown accommodates 561,300 residents across an area equivalent to 113.1 km
2, resulting in a density of 4218 people per km
2 [
74].
5. Results
5.1. Correlation Analysis
As shown in
Table 1, the correlation analysis provided evidence for Hypothesis 1 (H1), which posited that Predisposing Factors (PF), Need Factors (NF), Enabling Factors (EF), and Healthcare Utilization Patterns (HUP) are significantly correlated. Predisposing Factors (PF1) showed a significant positive correlation with HUP (r = 0.545,
p < 0.01), confirming their influence. Similarly, Need Factors (NF) were significantly correlated with HUP (r = 0.537,
p < 0.01), emphasizing their role in shaping healthcare utilization. Enabling Factors (EF) were positively correlated with HUP (r = 0.111); however, this relationship did not reach statistical significance (
p = 0.106). Fear of COVID-19 exhibited more nuanced relationships, playing a moderating role in certain pathways, as explored in the moderation analysis. These findings partially supported H1, with significant correlations evident for PF2 and NF3 but not uniformly across all factors.
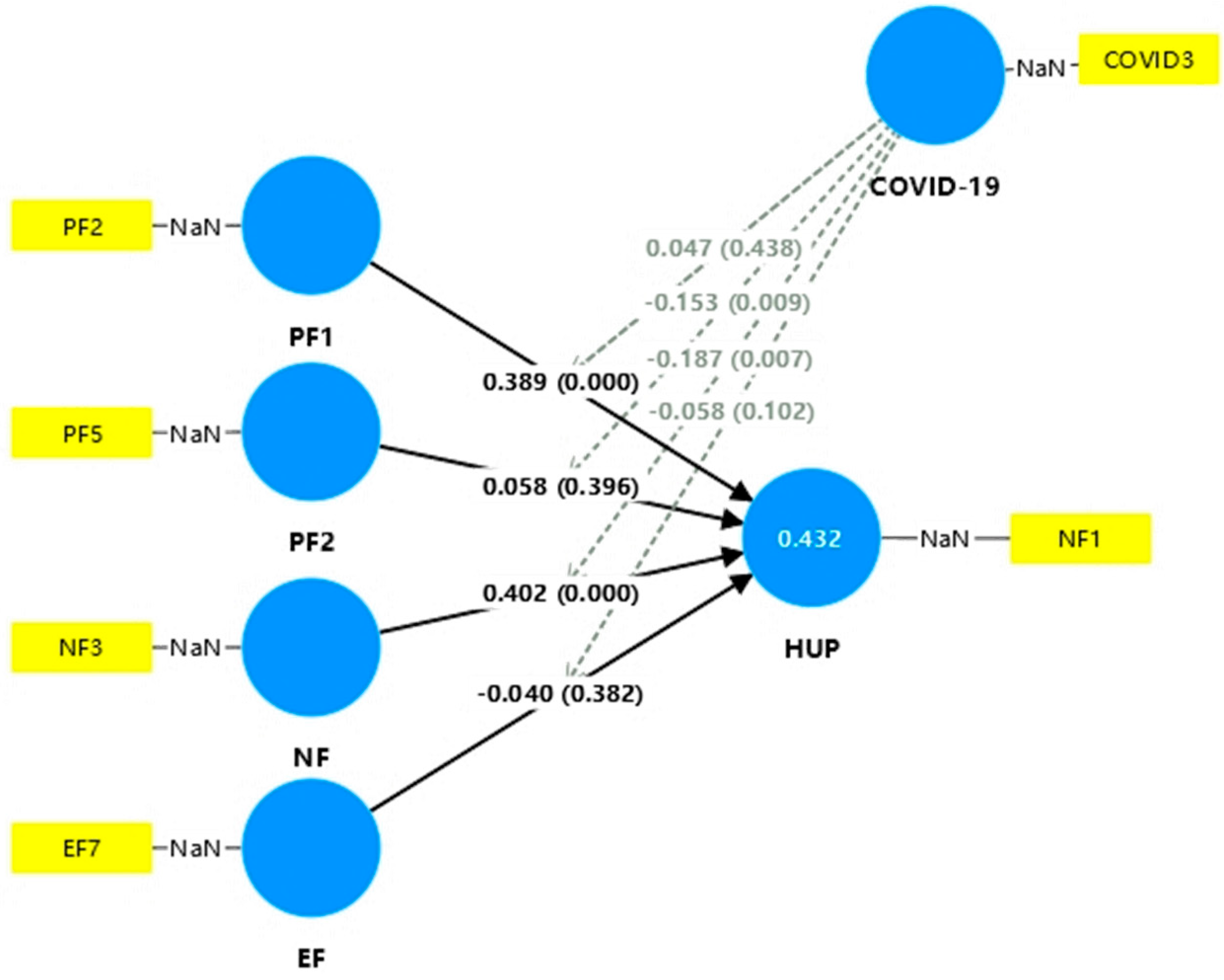
5.2. Path Analysis
Path analysis was used to explore Hypothesis 2 (H2), which indicated that Predisposing Factors (PF), Need Factors (NF), and Enabling Factors (EF) can significantly predict changes in Healthcare Utilization Patterns (HUP). As shown in
Figure 4, the R
2 of the model is 0.432, indicating that 43.2% of the variance in HUP can be explained by the combination of PF, NF, and EF, as well as the moderating effect of fear of COVID-19. This value emphasizes the strong explanatory power of the model while indicating that other untested factors may affect HUP.
Results showed that PF1 had a strong and significant positive effect on HUP (β = 0.389,
p < 0.001; 95% CI [0.264, 0.508]), confirming its predictive ability as indicated in in
Table 2. Similarly, NF showed a strong predictive effect (β = 0.402,
p < 0.001; 95% CI [0.266, 0.529]). In contrast, PF2 (β = 0.058,
p = 0.396) and EF (β = −0.040,
p = 0.382) failed to significantly predict HUP, indicating that their direct effects on HUP were minimal. Variance inflation factor (VIF) scores for all predictors were below the generally accepted threshold of 3, indicating the absence of severe multicollinearity. Notably, the interaction term COVID-19 × PF2 (VIF = 1.968) had the highest VIF, indicating that this interaction term, while noteworthy, did not inflate the variance to problematic levels. These results partially supported Hypothesis 2, as PF1 and NF emerged as significant predictors, whereas PF2 and EF did not.
5.3. Moderation Analysis
As shown in
Table 3, moderation analysis addressed Hypothesis 3 (H3), which proposed that fear of COVID-19 significantly moderates the relationships between predisposing factors, need factors, enabling factors, and healthcare utilization patterns. Although PF1 had the highest VIF score (1.968), the interaction between fear of COVID-19 and PF1 was not significant (β = 0.047,
p = 0.438), indicating that its effect was small and did not significantly change the direct effect of PF1 on HUP. However, fear of COVID-19 significantly moderated the effect of PF2 on HUP with a negative interaction effect (β = −0.153,
p = 0.009; 95% CI [−0.266, −0.035]), indicating that fear weakened the effect of PF2 on HUP. Similarly, the interaction between fear of COVID-19 and NF was also significant (β = −0.187,
p = 0.007; 95% CI [−0.315, −0.046]), indicating that fear weakened the predictive power of NF on HUP. The interaction between fear of COVID-19 and EF was not statistically significant (β = −0.058,
p = 0.102). These findings provide partial support for H3, highlighting the moderating effect of fear on specific pathways, specifically reducing the effects of PF2 and NF on HUP.
The results provided evidence for the study’s hypotheses. H1 and H2 were partially supported, with PF1 and NF having significant correlations and predictive effects, emphasizing their roles in healthcare utilization patterns. H3 was also partially supported, as fear of COVID-19 moderated specific relationships, especially with PF2 and NF. The results illuminate the complex interplay of factors influencing healthcare behaviors during the pandemic, affirming the relevance of Andersen’s Behavioral Model in this context.
6. Discussion
Urbanization inevitably leads to an increase in urban population, which places mounting pressure on cities to meet the basic needs of their inhabitants, including access to healthcare. As Heinberg [
75] emphasizes, sustainable cities must maintain economic stability while ensuring the health and well-being of their populations. Health is a fundamental component of quality of life and is critical to the resilience of communities. This study investigates the interplay between sociodemographic factors, healthcare utilization patterns, and health-seeking behaviors during the COVID-19 pandemic in Penang, Malaysia.
In urban settings, healthcare utilization is influenced by a combination of predisposing, enabling, and need factors, as outlined by Andersen’s Behavioral Model. This study specifically explores the role of these factors alongside fear of COVID-19 as a moderating variable. Predisposing factors include sociodemographic characteristics such as gender, age, ethnicity, education level, and health knowledge. These elements shape individuals’ attitudes and perceptions toward healthcare. For example, individuals with higher educational attainment may have better health literacy, increasing their likelihood of seeking preventive care [
43]. Cultural norms and gender beliefs may also influence willingness to access healthcare services. However, despite prior research indicating a significant relationship between gender and healthcare utilization [
3,
37,
43,
76,
77], our findings do not support a statistically significant association. This discrepancy may be attributed to external influences, such as concerns about COVID-19 infection in healthcare settings, as reported by other studies [
39,
40,
41,
42].
In contrast, age showed a strong and consistent association with healthcare utilization, echoing findings from previous studies [
43]. Older respondents demonstrated higher rates of healthcare use, which is expected due to increased vulnerability and chronic health conditions associated with aging. Thus, age remains a key predisposing factor in health-seeking behavior. Need factors also showed a significant relationship with healthcare utilization. These refer to individuals’ self-assessment of their health and perceived illness severity, which typically drive their decisions to seek care [
51]. Consistent with earlier findings [
37,
38,
43], our results indicate that individuals with chronic illnesses continued to utilize healthcare services even during the pandemic, highlighting the enduring role of need despite public health restrictions.
However, enabling factors—such as financial access or physical proximity to healthcare services—did not significantly influence utilization during the COVID-19 period. This may be due to Malaysia’s universal healthcare system and government interventions that subsidized or fully covered COVID-19 testing and treatment [
78], effectively shifting utilization patterns from being resource-driven to need-driven.
While our findings highlight the dominant role of need factors in healthcare utilization during the pandemic, it is important to recognize the broader structural and contextual realities that shape health behaviors—particularly among vulnerable populations. As highlighted by Kwiringira et al. [
79], healthcare access and utilization are not solely determined by individual-level needs but are embedded within a complex web of geographic, institutional, and socio-environmental conditions. In remote or resource-limited settings, the ability to seek care may depend as much on transportation, health facility distribution, workforce capacity, and community norms as on illness severity. Therefore, our findings should be interpreted within this broader systems-based framework, acknowledging that health behavior is multi-layered and shaped by both individual and collective factors.
A notable contribution is the inclusion of fear of COVID-19 as a moderating variable, revealing its differential impact across various factors. Fear significantly moderated the relationship between education level and healthcare utilization, where more educated individuals, typically more likely to seek care, reported reduced healthcare visits due to heightened risk perception [
50,
80]. Educated individuals often have better access to information about preventive health measures, thus reducing their likelihood of needing medical care for COVID-19. Additionally, while need factors usually encourage healthcare utilization, fear caused high-risk patients to avoid healthcare centers [
81]. These individuals may have relied more on digital health tools and self-care measures. Indeed, the expansion of telemedicine services and platforms like MySejahtera enabled remote consultations, medication tracking, and follow-ups, thereby reducing the need for in-person visits [
80]. This contributed to a linear effect of need factors within the community, as individuals adapted to remote care.
Despite the transformative role of digital tools like MySejahtera, their equitable accessibility remains a critical concern. Vulnerable groups, particularly older adults, those with limited digital literacy, or those without access to smart devices or the internet, may have been left behind in this digital shift. The assumption that digital health platforms are universally accessible risks reinforcing existing health inequities. Without parallel efforts to enhance digital inclusivity and support (e.g., digital literacy programs, multilingual interfaces, or assisted registration services), such tools may inadvertently marginalize those most in need of care. This highlights the need to view enabling factors not only in physical or economic terms but also through the lens of digital equity, which is increasingly central to healthcare resilience in crisis settings [
79].
Furthermore, given the demographic of older adults and those with chronic conditions who continued to access care, it is critical to acknowledge the elevated vulnerability of individuals with pre-existing cardiovascular disease. As highlighted by Ielapi et al. [
82], cardiovascular conditions—such as hypertension, coronary heart disease, and arrhythmias—not only increase susceptibility to COVID-19 infection but also significantly worsen prognosis. The pathophysiological interactions between COVID-19 and cardiovascular systems, including ACE2-related mechanisms and heightened inflammatory responses, exacerbate risks for acute cardiac injury and thromboembolic events. This intersection of chronic illness and pandemic exposure underscores the urgency of targeted health interventions for cardiovascular patients, especially those facing barriers to digital or physical access. In line with the findings of Ielapi et al. [
82], our results reaffirm the importance of integrating risk stratification and chronic disease management in pandemic response strategies.
7. Conclusions
Understanding the factors that influence healthcare utilization within a community is essential for enhancing the responsiveness and effectiveness of the health system. Guided by Andersen’s behavioral model of health service utilization, this study explored the interaction between individual characteristics and healthcare service use. The findings highlight the significant role of need-based factors, such as age, income, education level, self-rated health status, illness condition, and community health status, as key determinants of healthcare utilization among residents of Penang.
From a practical standpoint, the insights gained from this research offer valuable implications for healthcare providers. These findings can inform strategies to design and deliver tailored healthcare packages that address the specific needs of different demographic groups, particularly the aging population. Proactive initiatives, such as establishing specialized geriatric care facilities, are recommended to accommodate the expected increase in healthcare demand due to demographic shifts. By applying these insights, healthcare institutions can better align their services with the evolving needs of the community.
Moreover, the findings offer direction for policymakers to design targeted interventions for population groups most likely to benefit from specialized health programs. Notably, the study revealed unique patterns in healthcare-seeking behavior among married individuals in Penang, which differ from trends observed in other regions. This suggests that marriage plays a pivotal role in promoting societal stability and sustainable development.
Married individuals often demonstrate a strong sense of responsibility toward their families and communities, contributing to social cohesion, economic resilience, intergenerational support, civic engagement, and environmental awareness. Their active participation in community initiatives positions them as key contributors to building resilient and sustainable societies.
Concurrently, fostering collaboration between governmental and non-governmental healthcare providers, along with urban management entities, is essential to ensure equitable access to healthcare services. Strengthening accessibility across all social strata, including vulnerable populations, is a crucial step toward promoting justice and equality in healthcare. The study calls for immediate action from local authorities to improve public transportation infrastructure, thereby enhancing residents’ connectivity to both public and private healthcare facilities. This initiative can significantly boost healthcare accessibility and inclusivity, helping to establish a more equitable healthcare landscape for all residents.
In summary, the research reveals a notable trend among Penang residents, with a majority continuing to seek treatment at hospitals and clinics even during the pandemic. This behavior reflects a high level of trust in the healthcare system and highlights the importance of maintaining and enhancing the system’s reputation, particularly as Penang positions itself as a premier destination for health tourism.
While professional healthcare services are widely utilized, there remains a pressing need to strengthen public awareness and health education. These efforts should aim to reduce reliance on self-medication and encourage timely professional medical intervention. Simultaneously, improvements in service quality and the expansion of healthcare coverage are necessary to support these behavioral shifts. By integrating awareness campaigns with service enhancements, Penang can cultivate a culture of proactive healthcare-seeking behavior and further solidify its status as a center of medical excellence.
The study also provides fresh insights into the healthcare-seeking behaviors of married individuals in Penang, revealing patterns that differ from findings in other regions. This highlights the influence of marital status on healthcare utilization and emphasizes the broader societal impact of family structures in achieving sustainable development goals.
Finally, the research reinforces the importance of cross-sectoral collaboration between public and private healthcare entities and urban planners to remove systemic barriers to healthcare access. Notably, the emphasis on enhancing public transportation to connect residents with healthcare facilities showcases the study’s innovative and integrative approach. Overall, this research advances understanding in the field of healthcare utilization and underscores the value of proactive, inclusive strategies for building a resilient and equitable healthcare system.
As with any research endeavor, this study has certain limitations that warrant acknowledgment. Foremost is the geographical scope, which is limited to Penang. While Penang offers a diverse yet urbanized population, it may not adequately reflect the socio-cultural, infrastructural, and healthcare accessibility conditions of other Malaysian states. For instance, rural areas in Sabah, Sarawak, or Kelantan may face distinct barriers such as limited healthcare infrastructure, lower digital health adoption, and differing cultural beliefs regarding illness and care-seeking. These differences may significantly mediate healthcare utilization patterns and the applicability of Andersen’s model across regions. Moreover, the modest sample size, though statistically valid for the analysis conducted, restricts broader national extrapolation. Future studies incorporating multi-regional or nationally representative samples would provide a more comprehensive understanding of healthcare-seeking behavior across Malaysia’s diverse contexts.
Additionally, although the distance between residential areas and healthcare centers was identified as a significant factor influencing healthcare service utilization during the pandemic, its relevance in Penang may be limited due to the state’s relatively compact size. The spatial constraints of Penang may not accurately represent the dynamics observed in larger geographical regions.
Looking ahead, there is a clear need for further research to deepen the understanding of healthcare utilization patterns in Malaysia, particularly in the areas of chronic illness management and the application of Andersen’s behavioral model among individuals with mobility impairments. Addressing these gaps will allow future studies to generate more nuanced insights into healthcare utilization within the local context, ultimately supporting the development of targeted interventions and policies to improve healthcare accessibility and equity in Penang.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}