
The Economic Consequences of Decriminalizing Sex Work in Washington, DC—A Conceptual Model


Abstract
:1. Introduction
1.1. Legal Models of the Commercial Sex Industry
1.2. Economic Potential of Decriminalization
1.3. Context in the District of Columbia (DC)
1.4. Objectives
2. Materials and Methods
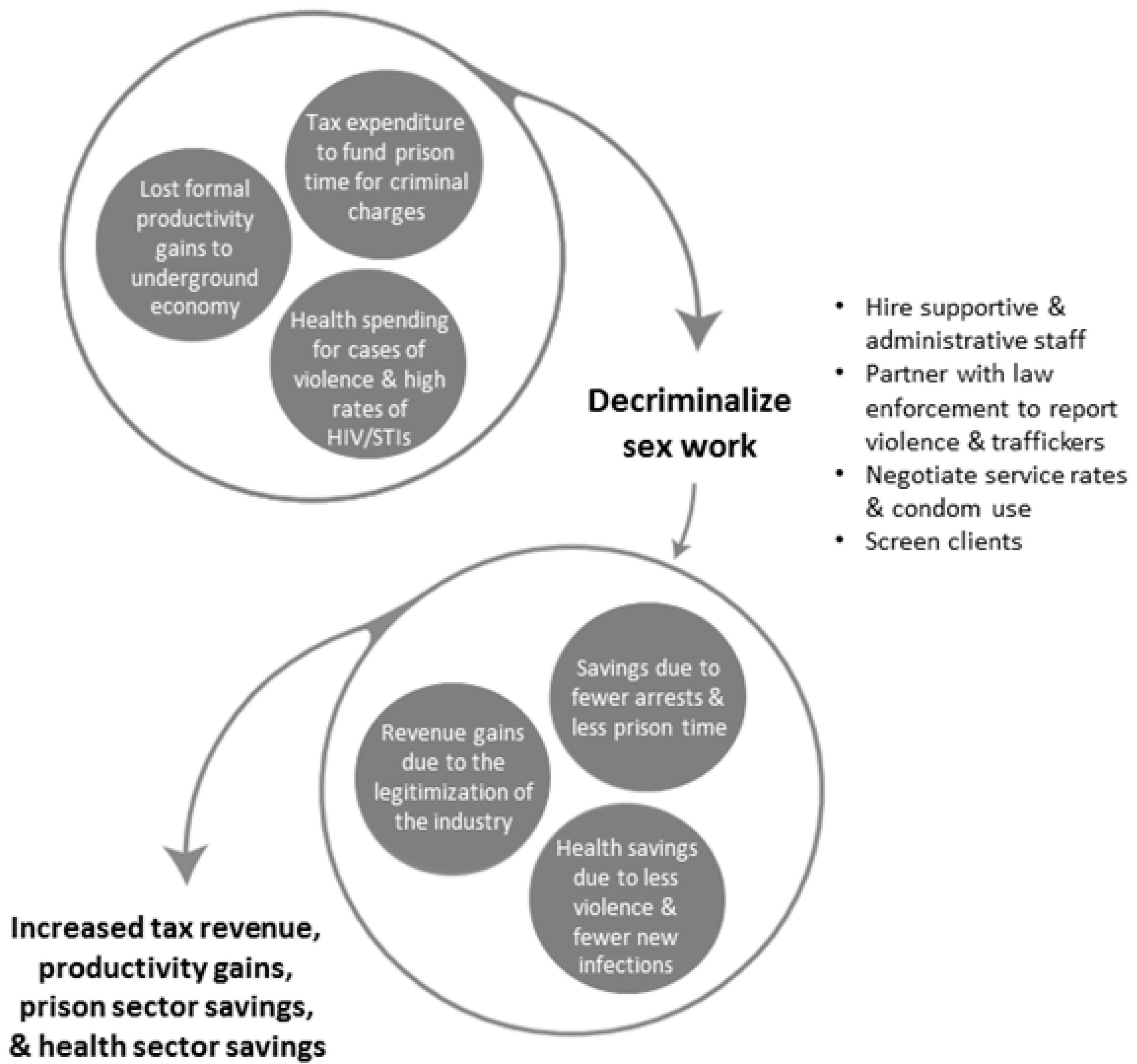
2.1. Study Design
2.1.1. Income Tax Generated
2.1.2. Criminal Justice System Savings
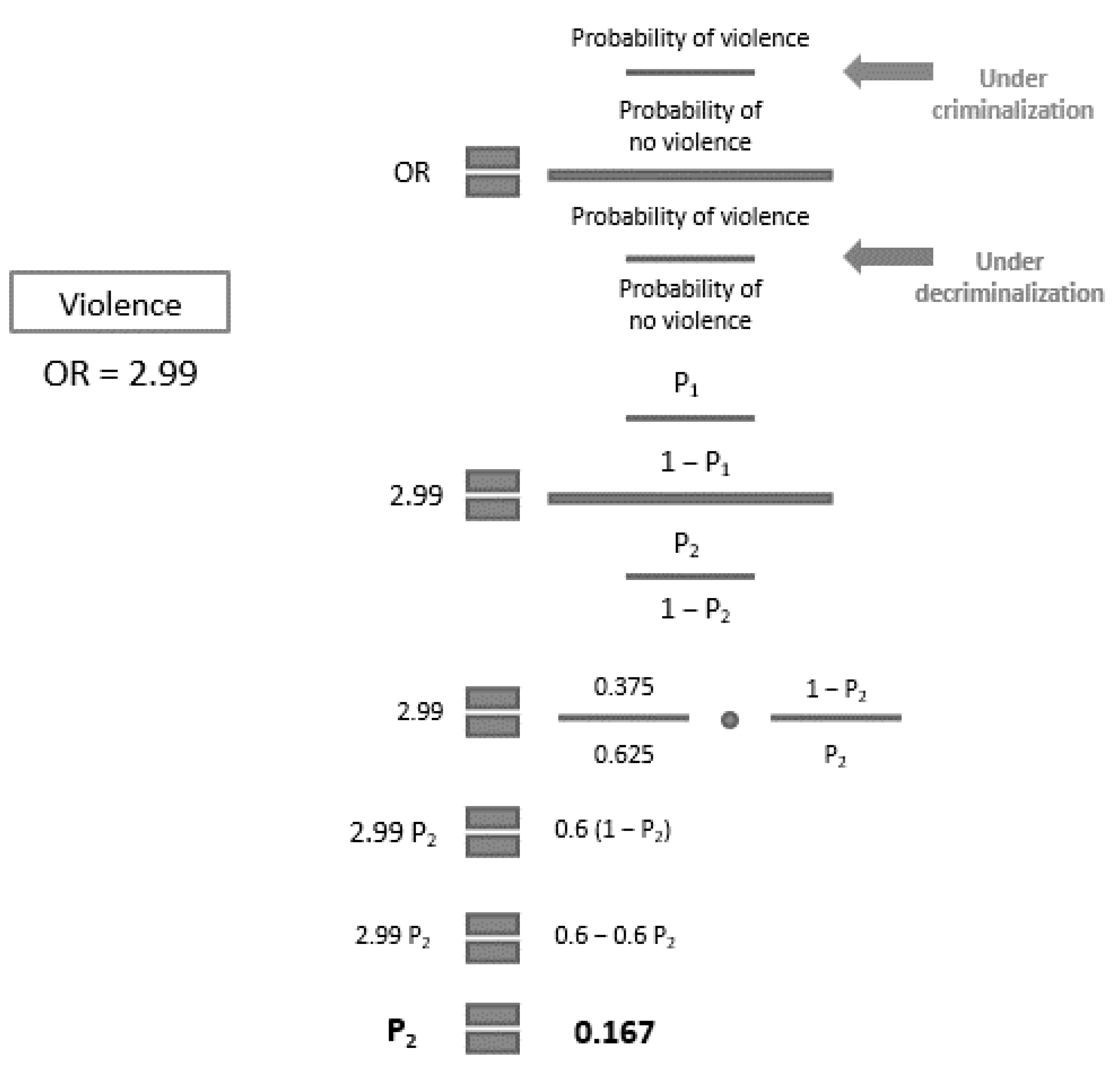
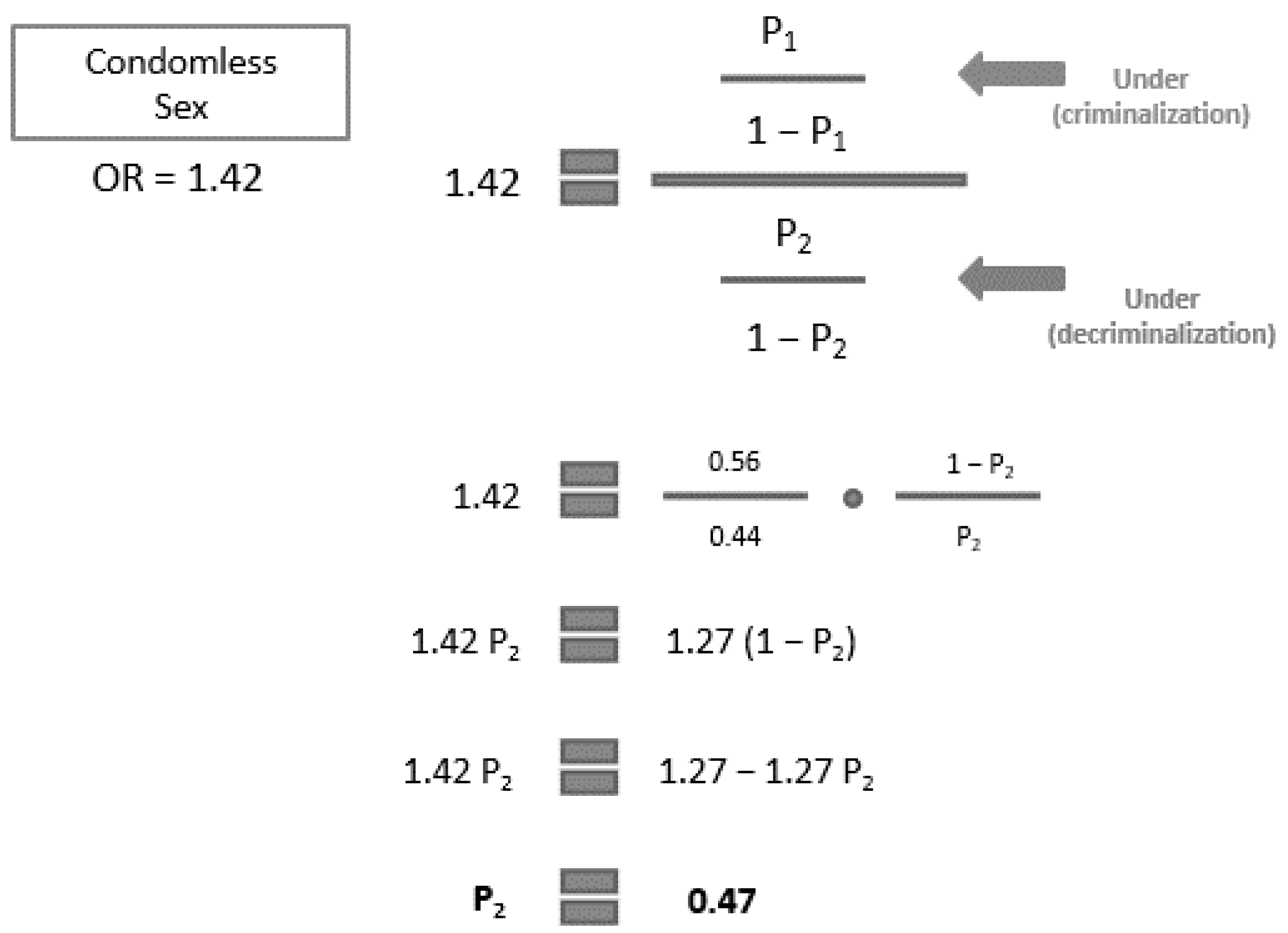
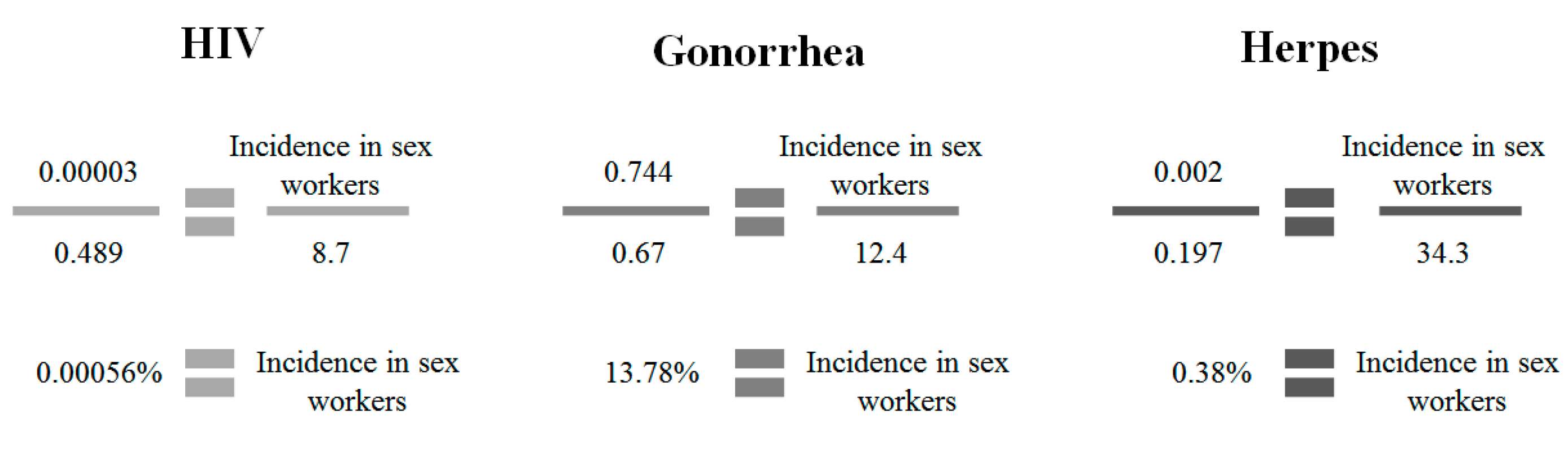
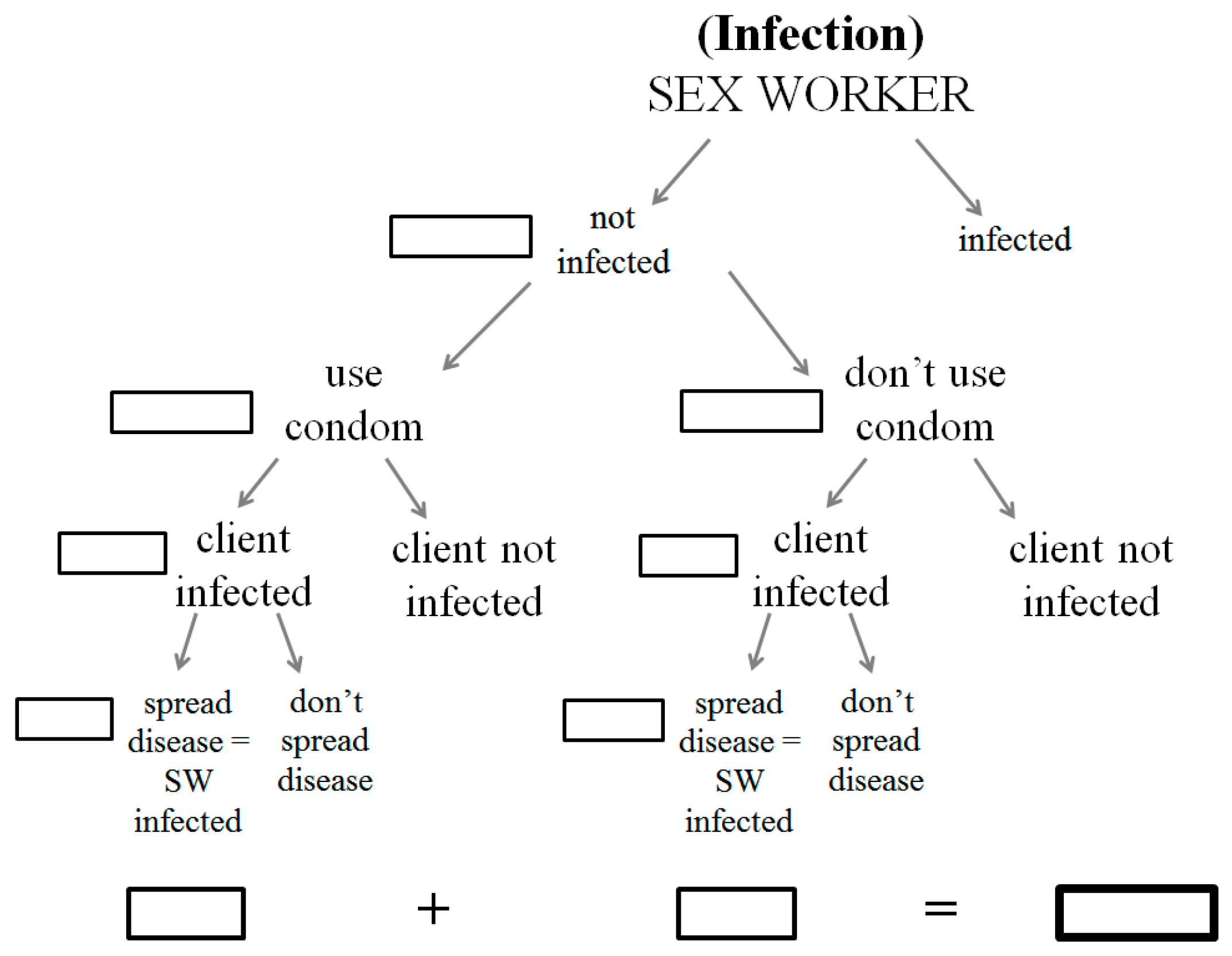
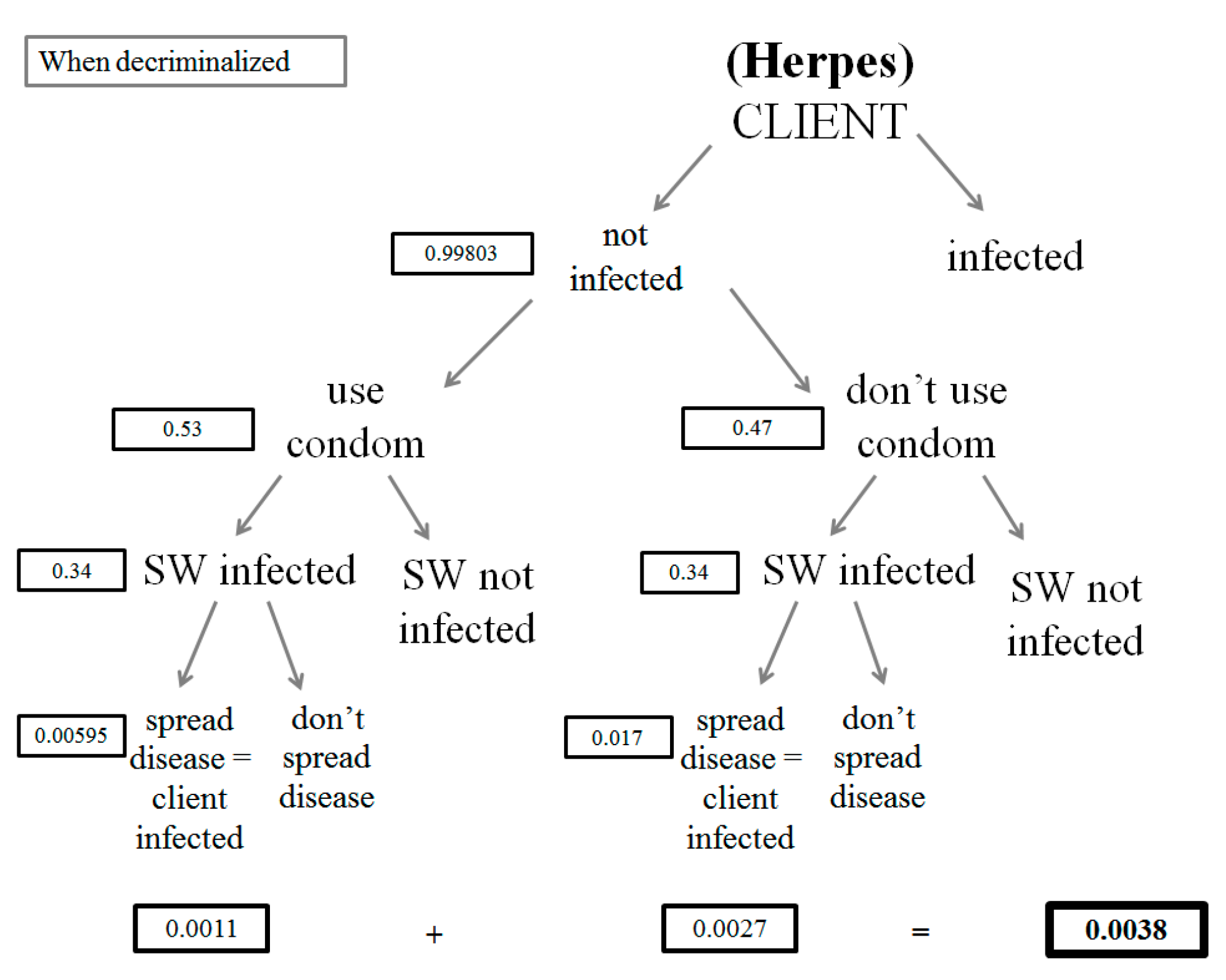
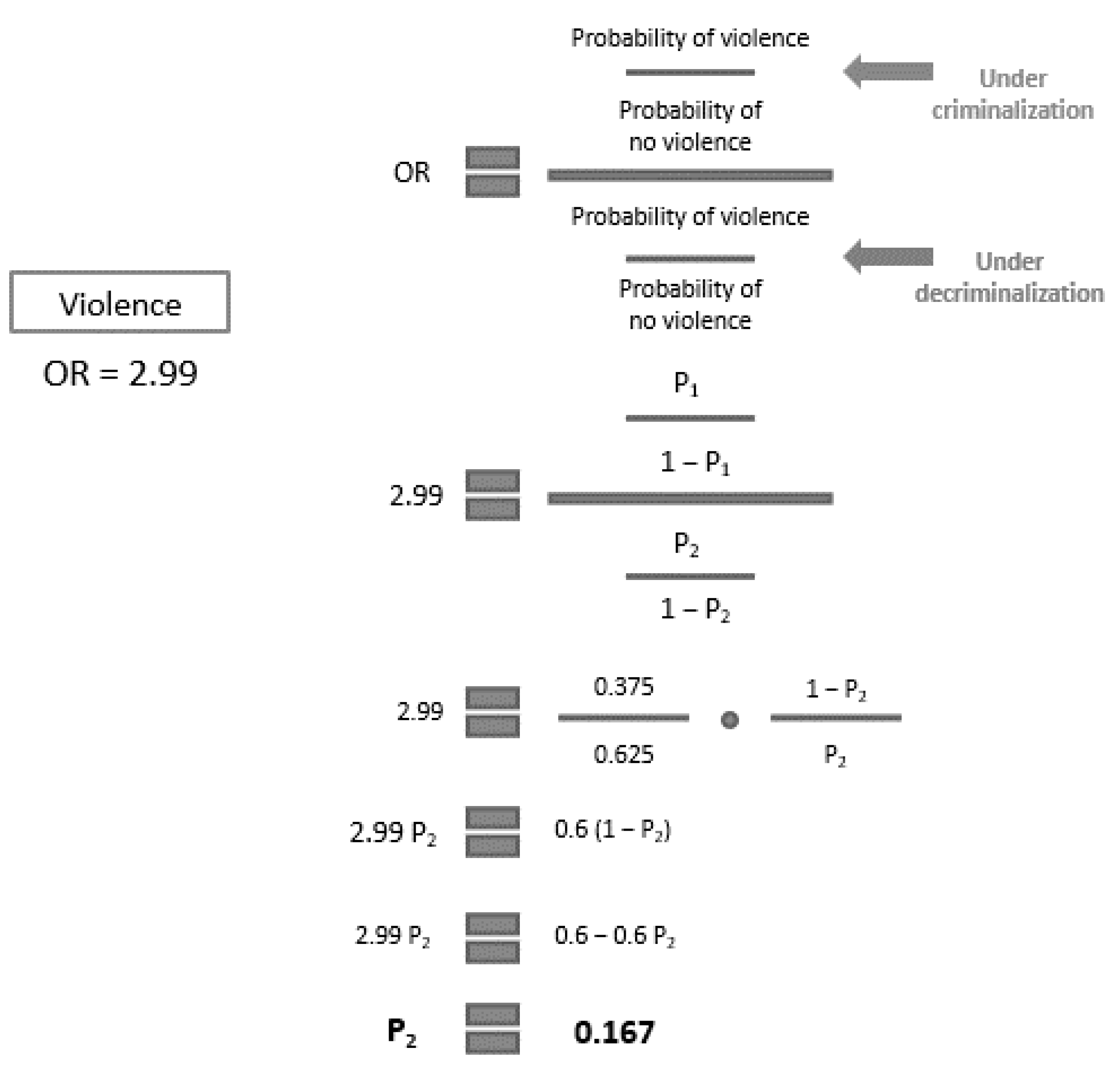
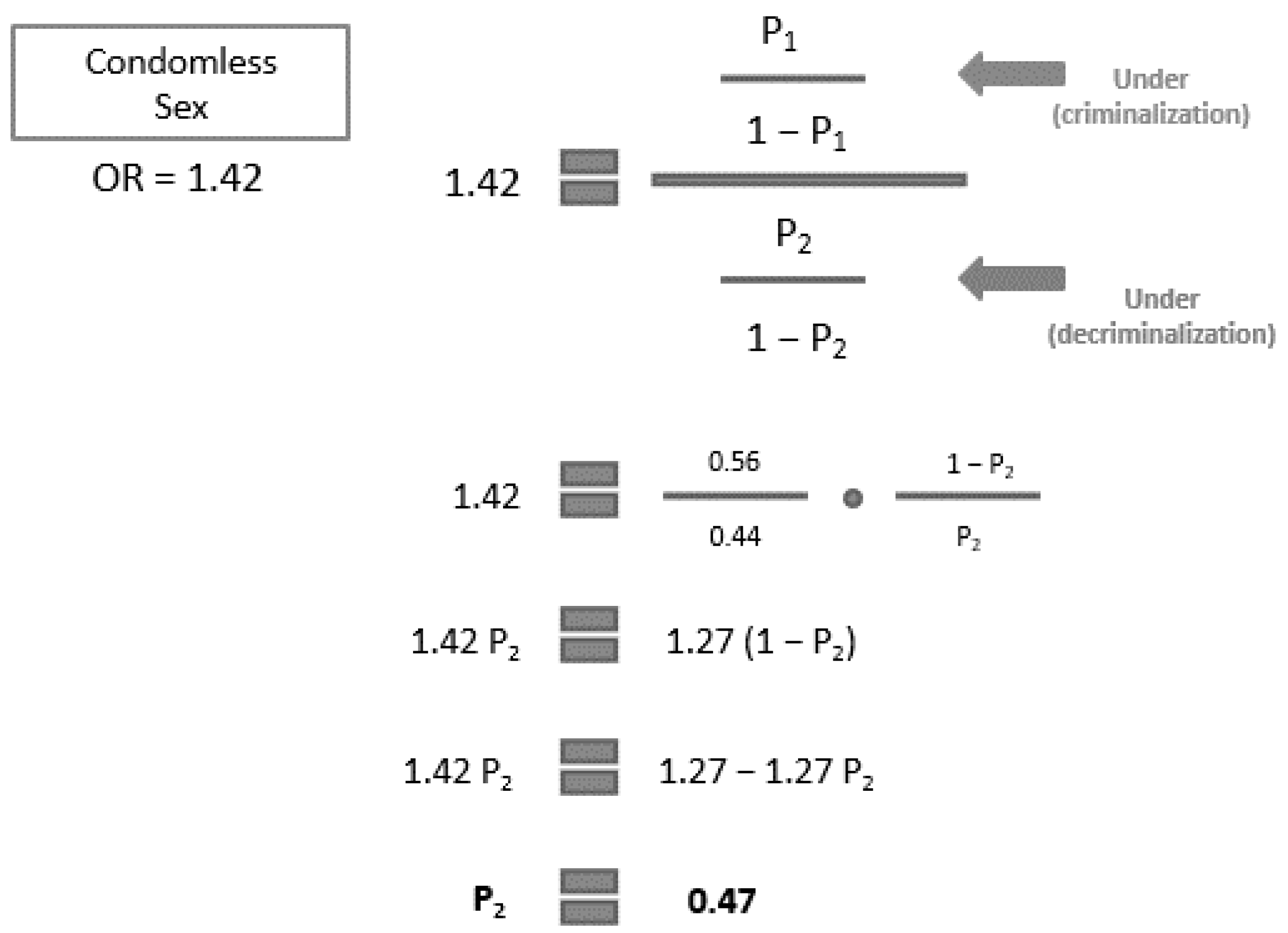
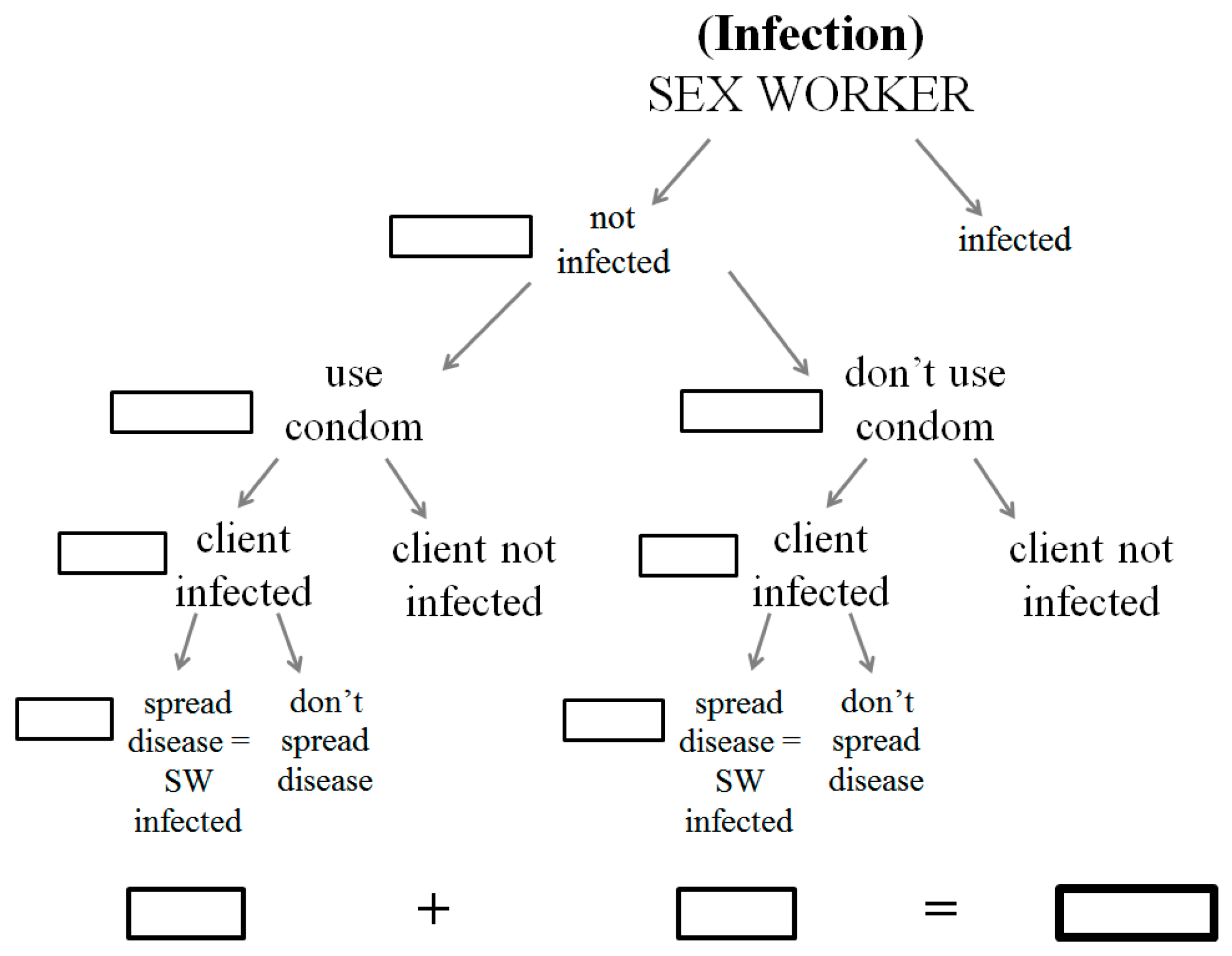
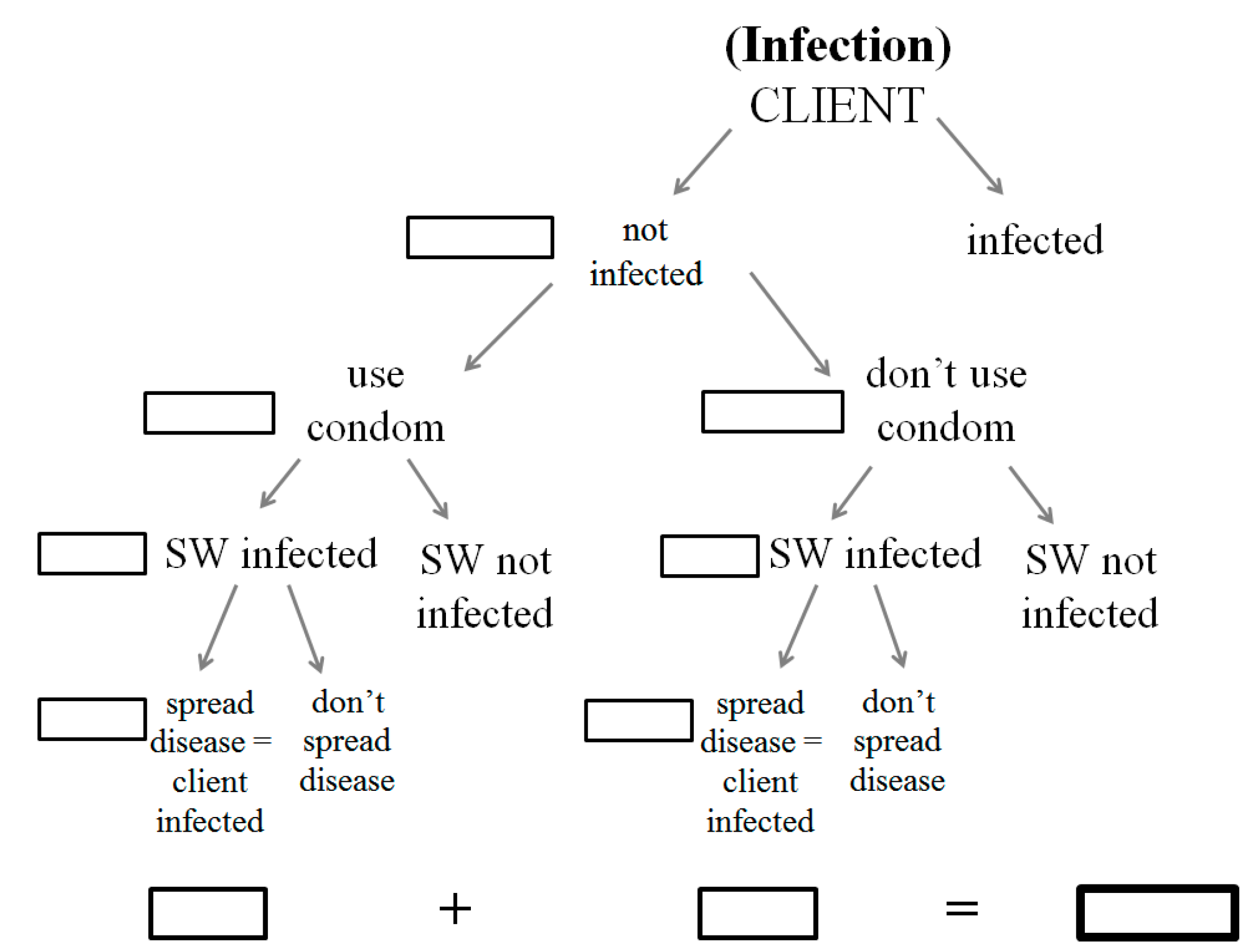
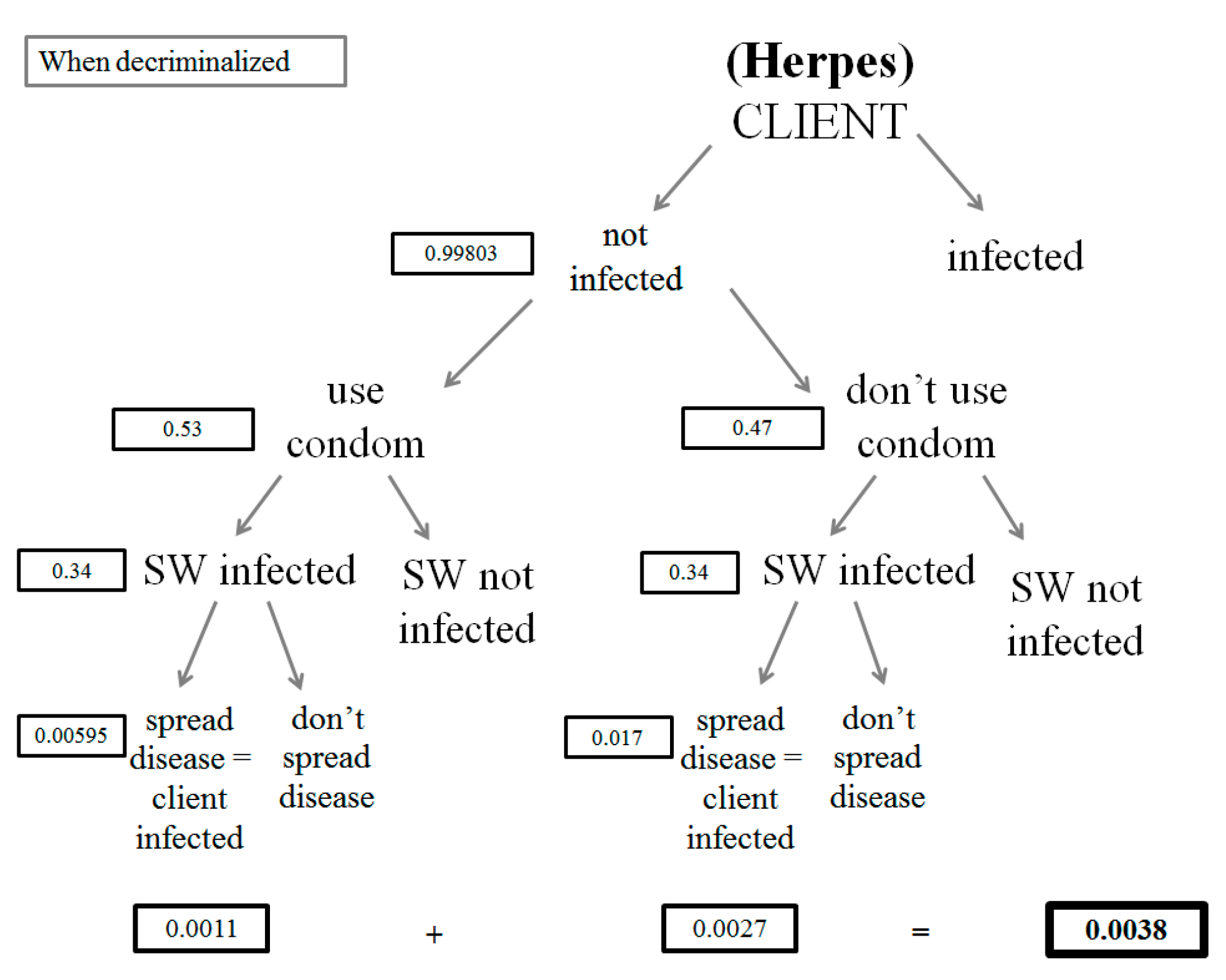
2.1.3. Health Sector Savings
2.1.4. Sensitivity Analysis
2.2. Data Sources
3. Results
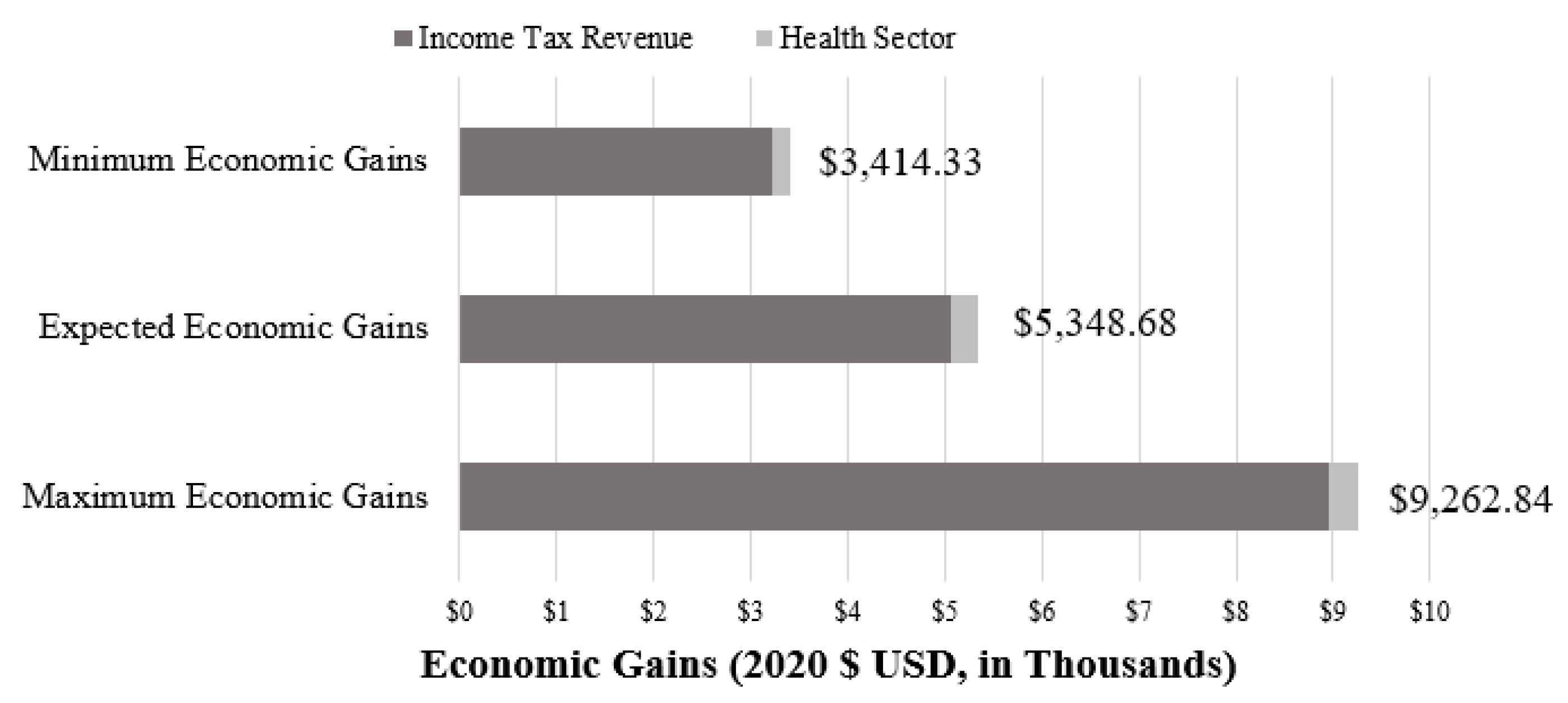
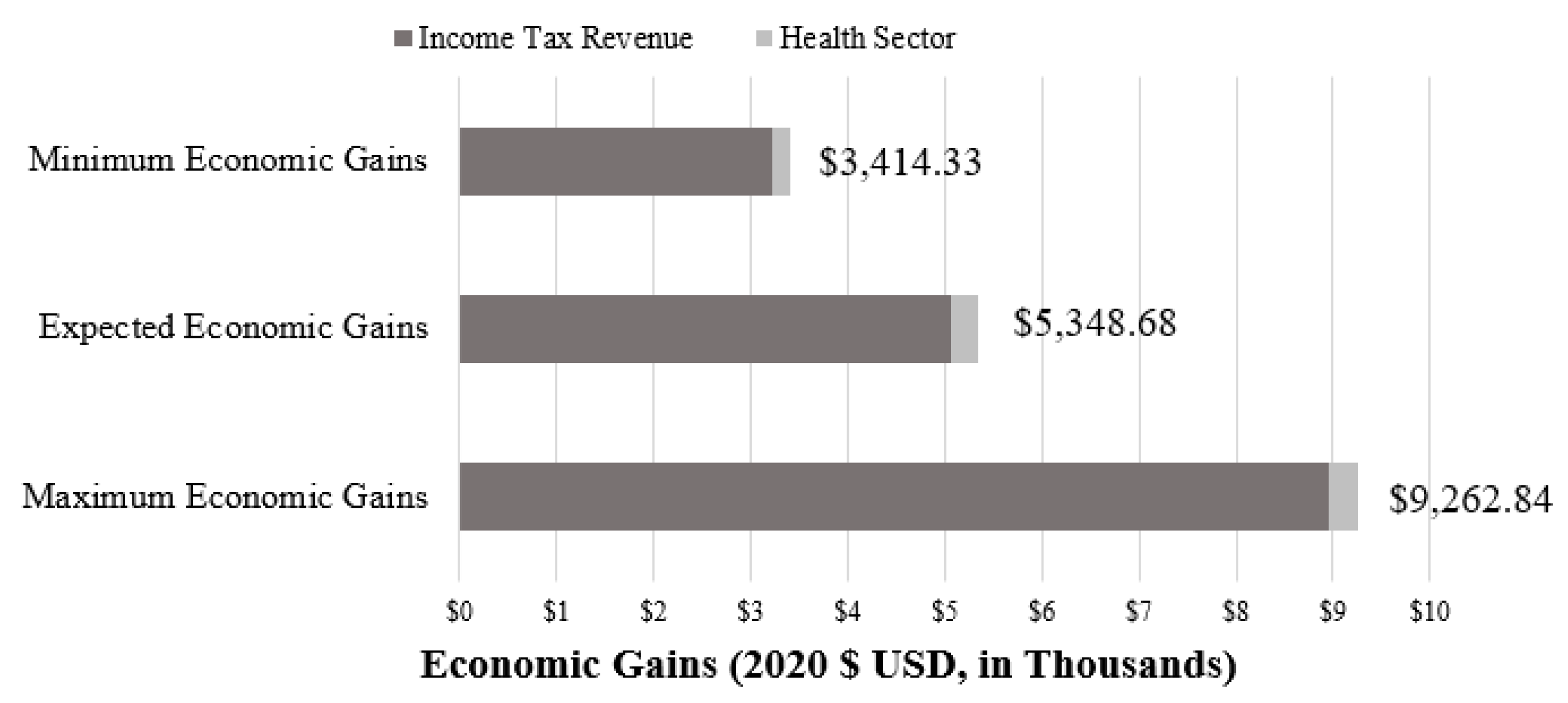
3.1. Main Results
3.2. Sensitivity Analysis
4. Discussion
4.1. Summary of Results
4.2. Comparison to Other Studies
4.3. Strengths and Limitations
4.4. Policy Implications
4.5. Recommendations and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Overestimation | Underestimation |
|---|---|---|
| Income Tax | Calculated from a tax rate based on individuals filing without dependents | Assumed sex worker salary would remain constant, rather than increase with demand |
| Included sex workers who are already filing income taxes | Excluded income generated by other workers in the industry | |
| Did not apply tax deductions to salary | ||
| Criminal Justice Sector | Excluded costs to train law enforcement | Assumed arrests for prostitution led to only one day of prison time |
| Excluded costs to disseminate educational materials | Did not account for higher costs to keep women in jail | |
| Health Sector | Assumed all instances of violence would require medical attention | Only measured direct, medical costs; clients’ productivity loss and all indirect medical costs were excluded |
| Assumed all new cases of HIV/STIs were transmitted through unprotected sex | Excluded medical services used by those not enrolled in health insurance | |
| Excluded the portion of sex workers who “sometimes used condoms” during vaginal sex | Only measured the savings due to HIV, gonorrhea, and herpes; all other STIs were excluded | |
| Utilized prevalence and incidence data of violence and HIV/STIs, which are often underreported | ||
| Assumed survivors of violence only experienced one episode of violence and sought treatment one time 1 | ||
| Sourced violence data from the UK, where sex work was less criminalized | ||
| Measured incidence of violence only when perpetrated by clients and not by police | ||
| Assumed that clients’ rate of infection was consistent with the general population | ||
| Assumed clients only solicited services once a year | ||
| Assumed all clients were men; did not account for clients who may be women, transgender, or gender non-conforming |
References
- Platt, L.; Grenfell, P.; Meiksin, R.; Elmes, J.; Sherman, S.G.; Sanders, T.; Mwangi, P.; Crago, A.-L. Associations between sex work laws and sex workers’ health: A systematic review and meta-analysis of quantitative and qualitative studies. PLoS Med. 2018, 15, e1002680. [Google Scholar] [CrossRef]
- Vanwesenbeeck, I. Sex Work Criminalization Is Barking Up the Wrong Tree. Arch. Sex. Behav. 2017, 46, 1631–1640. [Google Scholar] [CrossRef] [Green Version]
- McGlynn, E.A. Localize the Remedy; Rand Review. 2004. Available online: https://www.rand.org/content/dam/rand/pubs/corporate_pubs/2007/RAND_CP22-2004-08.pdf (accessed on 29 January 2019).
- Arrington, M.; Berkeley, S.; Gonzalez, L.C.; Hickey, D.; Kirby, J.; Langston, B.; Saunders, P.; Smith, E.; Turner, Z. Community Research Team. 2008. Available online: https://dctranscoalition.files.wordpress.com/2010/05/movealongreport.pdf (accessed on 29 January 2019).
- Biek, K. Hawaii Police Officers Allowed to Have Sex with Prostitutes. 2014. Available online: https://www.ajc.com/news/hawaii-police-officers-allowed-have-sex-with-prostitutes/DpmkFo8ooYW04jVlp6vlnO/ (accessed on 29 January 2019).
- Amnesty International. Q&A: Policy to Protect the Human Rights of Sex Workers. 2016. Available online: https://www.amnesty.org/en/qa-policy-to-protect-the-human-rights-of-sex-workers/ (accessed on 4 March 2019).
- DECRIMNOW, DC. DecrimNow: What Media Should Be Telling You about the Fight to Decriminalize Sex Work | YouTube. 2018. Available online: https://www.youtube.com/watch?v=EtLIohf-4Ho (accessed on 10 March 2019).
- Tani, M. Sex Worker Explains the Difference between Legalizing and Decriminalizing Prostitution—Business Insider. 2015. Available online: https://www.businessinsider.com/sex-worker-explains-the-difference-between-legalizing-and-decriminalizing-prostitution-2015-6?IR=T (accessed on 29 January 2019).
- A Historic Breakthrough for Sex Workers’ Rights | The New Republic. Available online: https://newrepublic.com/article/154111/new-york-bill-decriminalization-prostitution-sex-worker-rights (accessed on 4 November 2019).
- Mac, J. The Laws That Sex Workers Really Want | TED Talk. 2016. Available online: https://www.ted.com/talks/juno_mac_the_laws_that_sex_workers_really_want (accessed on 29 January 2019).
- New Zealand Parliament. Prostitution Law Reform in New Zealand. 2012. Available online: https://www.parliament.nz/en/pb/research-papers/document/00PLSocRP12051/prostitution-law-reform-in-new-zealand/ (accessed on 1 March 2019).
- Disogra, C.E.; Mariño, R.; Minichiello, V. Self-reported use of health services, contact with police and views about sex work organizations among male sex workers in Cordoba, Argentina. J. Psychol. Hum. Sex 2005, 17, 171–195. [Google Scholar] [CrossRef]
- Segal, N.; Stolarick, K. Buy Me Love: Realizing the Economic Potential of Sex Work Decriminalization. 2013. Available online: www.martinprosperity.org (accessed on 26 February 2019).
- Sankofa, J. From Margin to Center: Sex Work Decriminalization Is a Racial Justice Issue. Available online: https://www.amnestyusa.org/from-margin-to-center-sex-work-decriminalization-is-a-racial-justice-issue/ (accessed on 14 January 2020).
- Luo, N. Decriminalizing Survival: Policy Platform and Polling on the Decriminalization of Sex Work. 2020. Available online: https://www.filesforprogress.org/memos/decriminalizing-sex-work.pdf (accessed on 29 January 2019).
- Cunningham, S.; Shah, M. Decriminalizing Indoor Prostitution: Implications for Sexual Violence and Public Health. 2017. Available online: http://www.restud.com/wp-content/uploads/2017/11/MS21721manuscript.pdf (accessed on 1 March 2019).
- Roderick, L. What We Owe to the Hidden, Groundbreaking Activism of Sex Workers—Broadly. 2017. Available online: https://broadly.vice.com/en_us/article/8x4gmx/what-we-owe-to-the-hidden-groundbreaking-activism-of-sex-workers (accessed on 24 February 2019).
- Gunderson, A. The Effect of Decriminalizing Prostitution on Public Health and Safety—Chicago Policy Review. 2018. Available online: http://chicagopolicyreview.org/2018/02/26/the-effect-of-decriminalizing-prostitution-on-public-health-and-safety/ (accessed on 14 May 2019).
- Rosen, D. It’s Time to Decriminalize Sex Work. 2018. Available online: https://progressive.org/op-eds/its-time-to-decriminalize-sex-work-180814/ (accessed on 4 March 2019).
- DC—B23-0318|BillTrack50. Available online: https://www.billtrack50.com/BillDetail/1131430 (accessed on 6 November 2019).
- Improving Laws and Policies to Protect Sex Workers and Promote Health and Wellbeing: A Report On Criminalization of Sex Work in the District of Columbia, Washington, D.C. 2020. Available online: https://whitmanwalkerimpact.org/wp-content/uploads/2020/12/Sex-Worker-Law-and-Policy-Report-FINAL.pdf (accessed on 8 July 2021).
- Thacker, H. It’s Time for the D.C. Council to Decriminalize Sex Work. Available online: https://www.gwhatchet.com/2020/12/24/its-time-for-the-d-c-council-to-decriminalize-sex-work/ (accessed on 13 September 2021).
- Geographic Distribution|Statistics Overview|Statistics Center|HIV/AIDS|CDC. Available online: https://www.cdc.gov/hiv/statistics/overview/geographicdistribution.html (accessed on 6 November 2019).
- HHS; CDC; Oid; NCHHSTP; DSTDP. 2018 STD Surveillance Report: State Ranking Tables. 2018. Available online: https://www.cdc.gov/std/stats18/STDSurveillance2018-full-report.pdf (accessed on 29 January 2019).
- Justice Policy Institute. A Capitol Concern. 2010. Available online: www.justicepolicy.org (accessed on 8 March 2019).
- DC Fiscal Policy Institute. DC Poverty Demographics. 2014. Available online: https://www.dcfpi.org/wp-content/uploads/2009/03/DC-Poverty-Demographics.pdf (accessed on 15 March 2019).
- Dank, M. The Hustle: Economics of the Underground Commercial Sex Economy. 2014. Available online: http://apps.urban.org/features/theHustle/index.html (accessed on 15 March 2019).
- Dockterman, E. Economics of Prostitution Study Shows Pimping Isn’t That Profitable | Time. 2014. Available online: http://time.com/21351/prostitution-isnt-as-profitable-as-you-think/ (accessed on 2 May 2019).
- Mai, C.; Subramanian, R. The Price of Prisons: Examining State Spending Trends, 2010–2015|Vera Institute of Justice. 2017. Available online: https://storage.googleapis.com/vera-web-assets/downloads/Publications/price-of-prisons-2015-state-spending-trends/legacy_downloads/the-price-of-prisons-2015-state-spending-trends.pdf (accessed on 8 March 2019).
- Vera Institute of Justice. A Guide to Calculating Justice-System Marginal Costs. 2013. Available online: www.vera.org/marginalcosts (accessed on 26 August 2019).
- America’s Health Rankings. Uninsured in District of Columbia in 2018. 2018. Available online: https://www.americashealthrankings.org/explore/annual/measure/HealthInsurance/state/DC (accessed on 29 January 2019).
- St. James Infirmary. SJI Research, Publications & Presentations. 2002. Available online: https://stjamesinfirmary.org/wordpress/?page_id=30 (accessed on 11 April 2019).
- Warner, L.; Newman, D.R.; Austin, H.D.; Kamb, M.L.; Douglas, J.M.; Malotte, C.K.; Zenilman, J.M.; Rogers, J.; Bolan, G.; Fishbein, M.; et al. Condom effectiveness for reducing transmission of gonorrhea and chlamydia: The importance of assessing partner infection status. Am. J. Epidemiol. 2004, 159, 242–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, J.E. Appendix D Estimates of the Economic Burden of STDs: Review of the Literature with Updates. Available online: https://www.ncbi.nlm.nih.gov/books/NBK232924/ (accessed on 16 March 2019).
- Szucs, T.D.; Berger, K.; Fisman, D.N.; Harbarth, S. The estimated economic burden of genital herpes in the United States. An analysis using two costing approaches. BMC Infect. Dis. 2001, 1, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Office of Tax and Revenue. DC Individual and Fiduciary Income Tax Rates. 2019. Available online: https://otr.cfo.dc.gov/page/dc-individual-and-fiduciary-income-tax-rates (accessed on 11 April 2019).
- U.S. Bureau of Labor Statistics. Consumer Price Index. 2020. Available online: https://www.bls.gov/cpi/ (accessed on 10 August 2021).
- 2019 and 2020 Tax Brackets: Find Your Federal Tax Rate Schedules—TurboTax Tax Tips & Videos. Published 11 May 2021. Available online: https://turbotax.intuit.com/tax-tips/irs-tax-return/current-federal-tax-rate-schedules/L7Bjs1EAD (accessed on 12 August 2021).
- Social Security Administration. Social Security Announces 2.8 Percent Benefit Increase for 2019. 2018. Available online: https://www.ssa.gov/news/press/releases/2018/#10-2018-1 (accessed on 11 April 2019).
- Lutnick, A.; Cohan, D. Can the Decriminalization of Sex Work Assist HIV Prevention? Female Sex Workers in San Francisco, California Give Their Opinions. 2008. Available online: https://stjamesinfirmary.org/wordpress/wp-content/uploads/2008/08/lutnick_-sex-work-legal.pdf (accessed on 1 May 2019).
- Metropolitan Police Department. MPD Adult Arrests (2013–2020). 2020. Available online: https://mpdc.dc.gov/publication/mpd-adult-arrests-2013-2020 (accessed on 12 August 2021).
- Church, S.; Henderson, M.; Barnard, M.; Hart, G. Violence by clients towards female prostitutes in different work settings: Questionnaire survey. BMJ 2001, 322, 524–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Max, W.; Rice, D.P.; Finkelstein, E.; Bardwell, R.A.; Leadbetter, S. The economic toll of intimate partner violence against women in the United States. Violence Vict. 2004, 19, 259–272. Available online: http://www.ncbi.nlm.nih.gov/pubmed/15631280 (accessed on 16 March 2019). [CrossRef] [PubMed]
- IMHE. GBD Compare | IHME Viz Hub. 2017. Available online: https://vizhub.healthdata.org/gbd-compare/ (accessed on 23 January 2019).
- CDC. STD Curriculum for Clinical Educators | Gonorrhea Module. 2013. Available online: https://www2a.cdc.gov/stdtraining/ready-to-use/Manuals/Gonorrhea/gonorrhea-notes-April-2013.docx (accessed on 29 January 2019).
- DC Health Matters. Gonorrhea Incidence Rate: District of Columbia | DC Health Matters. 2017. Available online: http://www.dchealthmatters.org/indicators/index/view?indicatorId=248&localeId=130951 (accessed on 16 March 2019).
- Boily, M.-C.; Baggaley, R.; Wang, L.; Masse, B.; White, R.; Hayes, R.; Alary, M. Heterosexual risk of HIV-1 infection per sexual act: Systematic review and meta-analysis of observational studies. Lancet Infect. Dis. 2009, 9, 118–129. [Google Scholar] [CrossRef] [Green Version]
- Schiffer, J.T.; Mayer, B.T.; Fong, Y.; Swan, D.A.; Wald, A. Herpes simplex virus-2 transmission probability estimates based on quantity of viral shedding. J. R. Soc. Interface 2014, 11, 20140160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinkerton, S.D.; Abramson, P.R. Effectiveness of condoms in preventing HIV transmission. Soc. Sci. Med. 1997, 44, 1303–1312. [Google Scholar] [CrossRef]
- Magaret, A.S.; Mujugira, A.; Hughes, J.P.; Lingappa, J.R.; Bukusi, E.A.; De Bruyn, G.; Delany-Moretlwe, S.; Fife, K.H.; Gray, G.E.; Kapiga, S.; et al. Effect of Condom Use on Per-act HSV-2 Transmission Risk in HIV-1, HSV-2-discordant Couples. Clin. Infect. Dis. 2015, 62, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Gebo, K.A.; Fleishman, J.A.; Conviser, R.; Hellinger, J.; Hellinger, F.J.; Josephs, J.S.; Keiser, P.; Gaist, P.; Moore, R.D. Contemporary costs of HIV healthcare in the HAART era. AIDS 2010, 24, 2705–2715. [Google Scholar] [CrossRef] [PubMed]
- Monto, M.A.; Milrod, C. Ordinary or Peculiar Men? Comparing the Customers of Prostitutes With a Nationally Representative Sample of Men. Int. J. Offender Ther. Comp. Criminol. 2013, 58, 802–820. [Google Scholar] [CrossRef] [PubMed]
- World Population Review. District of Columbia Population 2019. 2019. Available online: http://worldpopulationreview.com/states/district-of-columbia-population/ (accessed on 8 May 2019).
- Shannon, K.; Strathdee, S.; Goldenberg, S.; Duff, P.; Mwangi, P.; Rusakova, M.; Reza-Paul, S.; Lau, J.; Deering, K.; Pickles, M.; et al. Global epidemiology of HIV among female sex workers: Influence of structural determinants. Lancet 2015, 385, 55–71. [Google Scholar] [CrossRef] [Green Version]
- Seib, C.; Dunne, M.P.; Fischer, J.; Najman, J.M. Predicting the Job Satisfaction of Female Sex Workers in Queensland, Australia. Int. J. Sex. Health 2012, 24, 99–111. [Google Scholar] [CrossRef] [Green Version]
- Levitt, S.D.; Venkatesh, S.A. An Empirical Analysis of Street-Level Prostitution. 2007. Available online: https://pdfs.semanticscholar.org/658c/72e46d6357d1dc2962aa3adcd342bdbab430.pdf?_ga=2.169507297.1531079438.1545097193-2532700.1545097193 (accessed on 29 January 2019).
- Hoomans, T.; Severens, J.L. Economic evaluation of implementation strategies in health care. Implement. Sci. 2014, 9, 168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenstone, M. Effective Regulation through Credible Cost-Benefit Analysis: The Opportunity Costs of Superfund. 2009. Available online: https://static1.squarespace.com/static/585017d2bebafbe412f1a838/t/5b4640fd0e2e7261549f41aa/1531330822047/New+Theory+Ch2+Greenstone+Effective+Regulation+through+Credibe+Cost+Beneift+Analysis+The+Opportunity+Costs+of+Superfund.pdf (accessed on 29 January 2019).
- Vining, A.R.; Weimer, D.L. Policy Analysis. In International Encyclopedia of the Social & Behavioral Sciences, 2nd ed.; Elsevier Inc.: Philadelphia, PA, USA, 2015; pp. 273–280. [Google Scholar]
- Shapiro, S. The Evolution of Cost-Benefit Analysis in U.S. Regulatory Decisionmaking. 2010. Available online: http://regulation.huji.ac.il (accessed on 26 November 2019).
- CDC. HIV Risk Among Persons Who Exchange Sex for Money or Nonmonetary Items. 2018. Available online: https://www.cdc.gov/hiv//group/sexworkers.html (accessed on 12 April 2019).
| Type of Data | Value |
|---|---|
| USD161,972.43 |
| USD32,748 + 32% of amount over USD160,725 = 33,147.18 |
| USD3500 + 8.5% of amount over USD60,000 = 12,167.66 |
| 1.45% of all income + 6.2% of income up to USD137,700 = 10,886.00 |
| 9% |
| Type of Data | Value |
|---|---|
| 273 |
| USD99.55 |
| USD73.95 |
| Type of Data | Value |
|---|---|
| 37.5% |
| USD1374.04 |
| 2.99 |
| 96.1% |
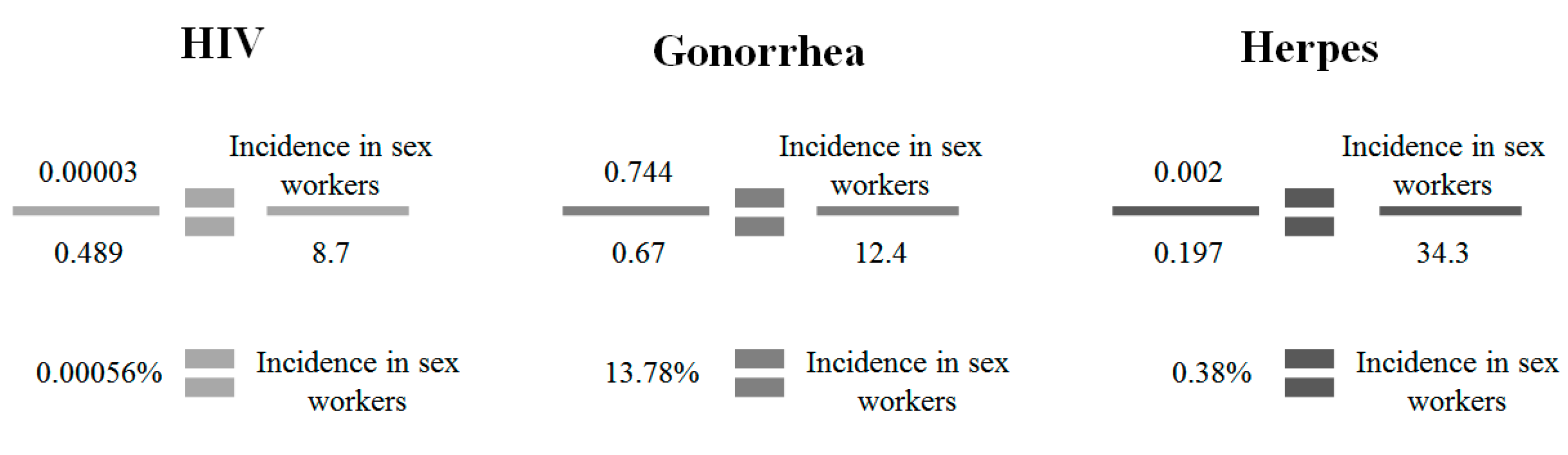
| Type of Data | Infection | ||
|---|---|---|---|
| HIV | Gonorrhea | Herpes | |
| 0.489% | 0.67% | 0.197% |
| 0.00003% | 0.744% 1 | 0.002% |
| 8.7% | 12.4% | 34.3% |
| 0.08% | 60% | 1.7% |
| 95% | 58% 3 | 96% |
| 0.004% | 25.2% | 0.068% |
| USD25,563.03 | USD1725.79 4 | USD523.55 5 |
| 44% | ||
| 96.1% | ||
| 1.42 | ||
| Type of Data | Infection | ||
|---|---|---|---|
| HIV | Gonorrhea | Herpes | |
| 0.04% | 20% | 1.7% |
| 95% | 58% 2 | 65% |
| 0.002% | 8.4% | 0.595% |
| 1% | ||
| 334,213.8 | ||
| Variable | Price in Base Year | Base Year | CPI from Base Year to 2020 | Price in 2020 USD |
|---|---|---|---|---|
| USD129,785.60 | 2007 | 24.8% | USD161,972.43 |
| USD91.16 | 2015 | 9.2% | USD99.55 |
| USD60.83 | 2009 | 20.6% | USD73.95 |
| USD809.21 | 2005 | 69.8% | USD1374.04 |
| USD19,912 | 2006 | 28.4% | USD25,563.03 |
| USD988.20 | 1994 | 74.6% | USD1725.79 |
| USD317.40 | 1996 | 65.0% | USD523.55 |
| Type of Data | Source |
|---|---|
| Dank et al., 2014 [27] |
| TurboTax, 2021 [38] |
| DC Office of Tax and Revenue, 2018 [36] |
| Social Security Administration, 2018 [39] |
| Lutnick and Cohan, 2008 [40] |
| Type of Data | Source |
|---|---|
| Metropolitan Police Department, 2020 [41] |
| Vera Institute of Justice, 2017 [29] |
| Vera Institute of Justice, 2013 & 2017 [29,30] |
| Type of Data | Source |
|---|---|
| Church et al., 2001 [42] |
| Max et al., 2004 [43] |
| Platt et al., 2018 [1] |
| America’s Health Rankings, 2018 [31] |
| Type of Data | Infection | ||
|---|---|---|---|
| HIV | Gonorrhea | Herpes | |
| IMHE, 2017 [44] | Centers for Disease Control and Prevention, 2013 (in DC) [45] | IMHE, 2017 [44] |
| IMHE, 2017 [44] | DC Health Matters, 2017 (in DC) [46] 1 | IMHE, 2017 [44] |
| St. James Infirmary, 2006 (in San Francisco) [32] | St. James Infirmary, 2006 (in San Francisco) [32] | St. James Infirmary, 2006 (in San Francisco) [32] |
| Boily et al., 2009 [47] | Centers for Disease Control and Prevention, 2013 [45] | Schiffer et al., 2015 [48] |
| Pinkerton and Abramson, 1997 [49] | Warner et al., 2004 [33] 3 | Magaret et al., 2016 [50] |
| Calculated by the author, based on available data | Calculated by the author, based on available data | Calculated by the author, based on available data |
| Gebo et al., 2010 [51] | Siegel, 1997 [34] | Szucs, 2001 [35] |
| St. James Infirmary, n.d. [32] | ||
| America’s Health Rankings, 2018 [31] | ||
| Platt et al., 2018 [1] | ||
| Type of Data | Infection | ||
|---|---|---|---|
| HIV | Gonorrhea | Herpes | |
| Boily et al., 2009 [47] | Centers for Disease Control and Prevention, 2013 [45] | Schiffer et al., 2015 [48] |
| Pinkerton and Abramson, 1997 [49] | Warner et al., 2004 [33] 2 | Magaret et al., 2016 [50] |
| Calculated by the author, based on available data | Calculated by the author, based on available data | Calculated by the author, based on available data |
| Monto and Milrod, 2014 [52] | ||
| World Population Review, 2019 [53] | ||
| Sex Worker Variable | Revenue/Costs under Criminalization | Revenue/Costs under Decriminalization | Gains/Savings per Sex Worker | |
|---|---|---|---|---|
| Income Tax Revenue | - | USD5058.08 | USD5058.08 | |
| Health Sector | Violence | USD486.42 | USD216.62 | USD274.65 |
| HIV | USD0.14 | USD0.12 | USD0.02 | |
| Gonorrhea | USD228.49 | USD212.85 | USD15.64 | |
| Herpes | USD1.92 | USD1.64 | USD0.29 | |
| TOTAL/SEX WORKER | USD5348.68 | |||
| Variable | Costs under Criminalization | Costs under Decriminalization | Savings for All Sex Workers |
|---|---|---|---|
| Criminal Justice System | USD20,118.48 | USD0 | USD20,118.48 |
| TOTAL/ALL | USD20,118.48 |
| Client Variable | Costs under Criminalization | Costs under Decriminalization | Savings per Client | Estimated Number of Clients | Total Savings | |
|---|---|---|---|---|---|---|
| Health Sector | HIV | USD0.47 | USD0.42 | USD0.05 | 3342.14 | USD167.11 |
| Gonorrhea | USD29.36 | USD27.03 | USD2.32 | 3342.14 | USD7753.00 | |
| Herpes | USD2.06 | USD1.90 | USD0.16 | 3342.14 | USD534.74 | |
| TOTAL/CLIENT | USD2.53 | TOTAL/ALL | USD8455.61 | |||
| Variable Modified | Expected Value | Lower Parameter | Upper Parameter |
|---|---|---|---|
| Sex Worker Income | USD161,972.43 | USD113,380.70 | USD210,564.16 |
| Sex Workers Paying Income | 9% | 6.3% | 11.7% |
| Income Tax Revenue | USD5058.08 | USD3210.91 | USD8960.45 |
| Insured Sex Workers Seeking Medical Services When Needed | 96.1% | 67.27% | 100% |
| Health Sector Savings | USD290.60 | USD203.42 | USD302.39 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Srsic, A.; Dubas-Jakóbczyk, K.; Kocot, E. The Economic Consequences of Decriminalizing Sex Work in Washington, DC—A Conceptual Model. Societies 2021, 11, 112. https://doi.org/10.3390/soc11030112
Srsic A, Dubas-Jakóbczyk K, Kocot E. The Economic Consequences of Decriminalizing Sex Work in Washington, DC—A Conceptual Model. Societies. 2021; 11(3):112. https://doi.org/10.3390/soc11030112
Chicago/Turabian StyleSrsic, Amanda, Katarzyna Dubas-Jakóbczyk, and Ewa Kocot. 2021. "The Economic Consequences of Decriminalizing Sex Work in Washington, DC—A Conceptual Model" Societies 11, no. 3: 112. https://doi.org/10.3390/soc11030112
APA StyleSrsic, A., Dubas-Jakóbczyk, K., & Kocot, E. (2021). The Economic Consequences of Decriminalizing Sex Work in Washington, DC—A Conceptual Model. Societies, 11(3), 112. https://doi.org/10.3390/soc11030112