How Colonial Power, Colonized People, and Nature Shaped Hansen’s Disease Settlements in Suriname



Abstract
1. Introduction
1.1. Hansen’s Disease and the Natural Environment
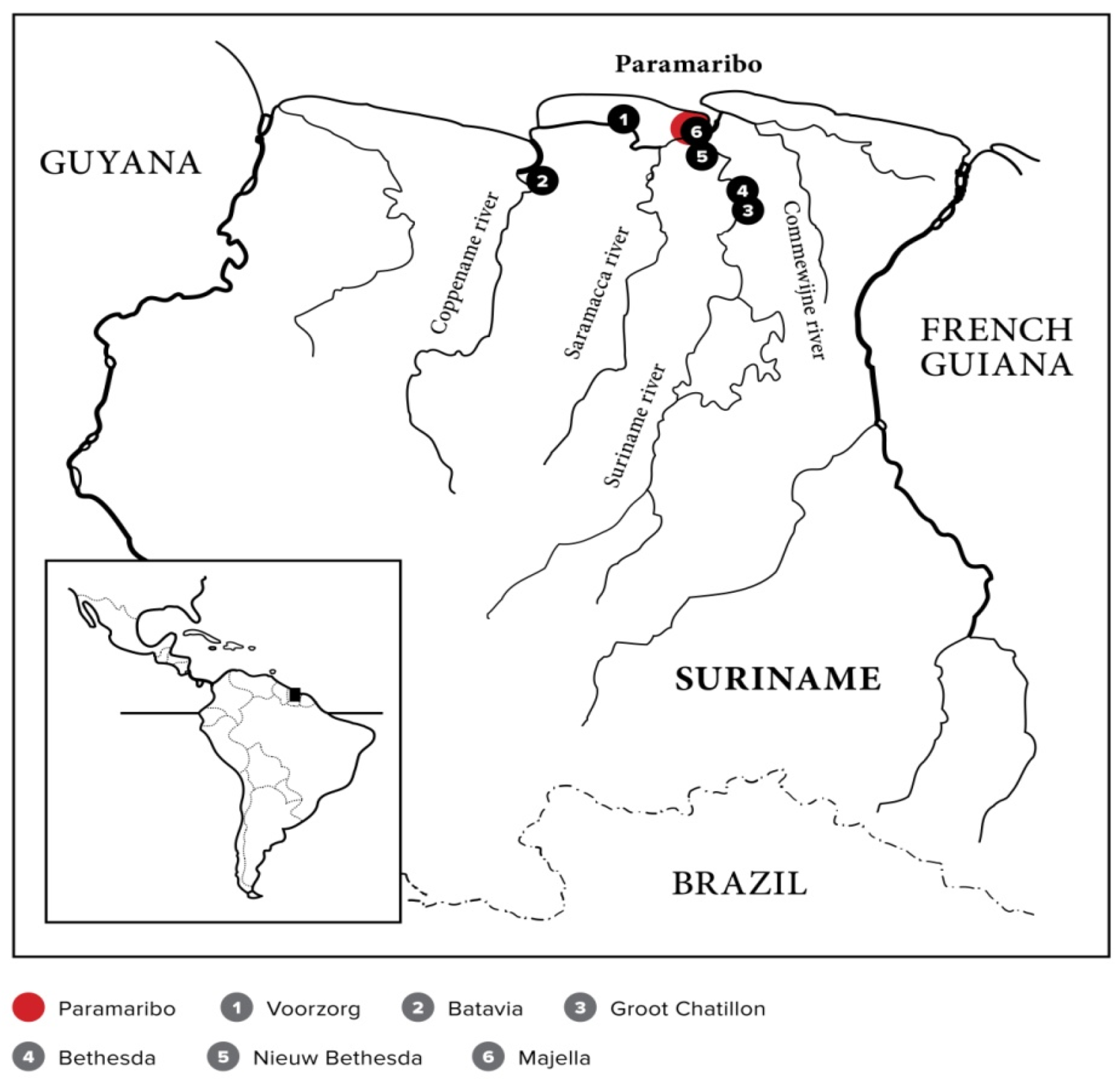
1.2. Suriname
1.3. Leprosy in Suriname
1.4. Ecology and Surinamese Leprosy Narratives, an Unexplored Area
2. Objective and Methods
3. Results and Discussion
3.1. The Colonizers’ Views and Strategies
3.1.1. Contagion
3.1.2. The Construction of a “Cordon Sanitaire”
When I was seven years old, white spots were detected on my buttocks during a medical examination at school. I was brought before the leprosy commission, six physicians, all of them had a light skin: whites, Jews, basradyu (bastard Jews), and mulattos. In those days you could not study [to become a doctor] when you were black, even if you were intelligent. The commission decided [about your future]. If four of the six said that you had to be turned in, then you had to go to a leprosy colony. The commission decided that [for the time being] I had to stay at home. There was no verification [of my home isolation]. But [they counted on] “dalaskowtu,” anonymous informers, receiving one dollar, when bringing in “sick children” walking on public roads. Incidentally, [dalaskowtu] did not only betray sick children but everyone who violated the law. They were a sort of policemen or spies for the colonial government. They were Surinamese who were used to oppress other Surinamese.
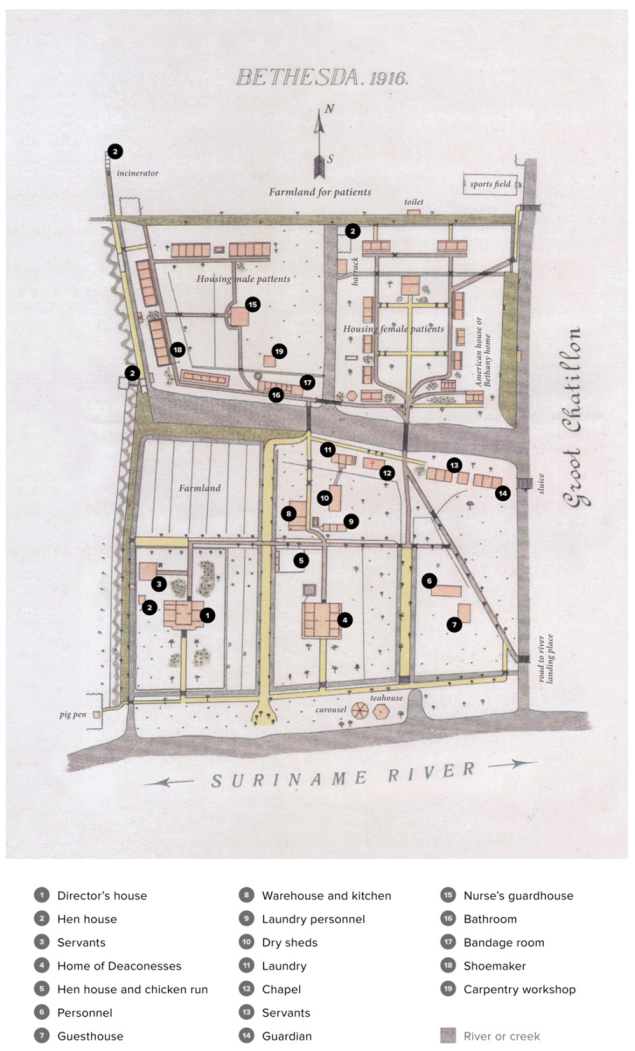
If you wanted to surprise a family member with something you had made yourself, for instance a beautiful frame, it had to be disinfected, with [methylated] spirit, I think. [The object] was kept in a special cabinet [for a while]. When you brought it [to the nurse] to be disinfected, you felt the pain, it’s a strange feeling. Even if you wanted to send a letter it had to be disinfected. Those were the rules in Bethesda.
In Chatillon, my four children were born. They were taken away from me at once after birth, to prevent them from contracting leprosy. Those were the rules. I handed them over to my mother-in-law, but when I was released from the asylum, I took them back to raise them myself.
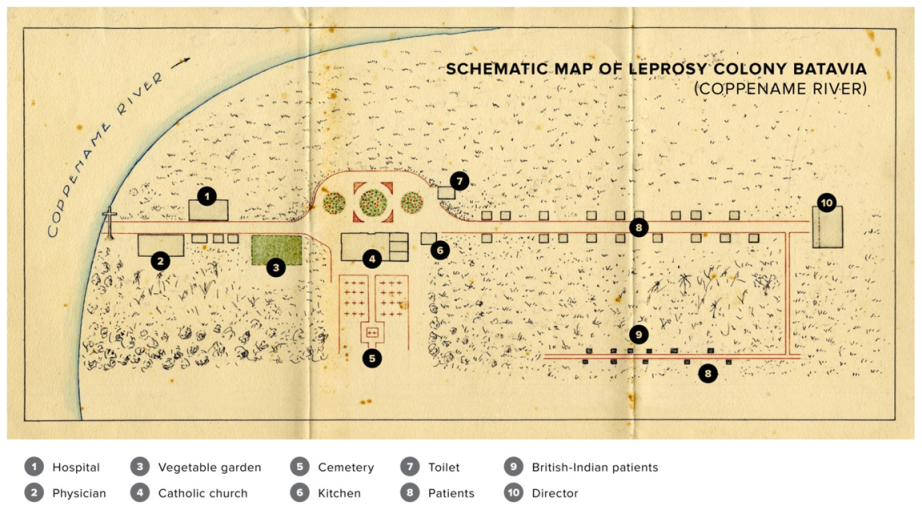
3.1.3. The Leprosaria
Anatomy of Leprosaria
The Old Leprosaria
Establishing Modern Leprosaria in a Pillarized Society
Running away was common. Inmate Hendrik from New Bethesda explains [29] (pp. 103–104):
[We] ran away in the evening, some [of us] visited a “working girl.” Yes, a young man needs a woman. So, we went to the Maagden street, Jodenbree street… the well-known streets where one can find “working girls” … I was a young [man], I could not resist it … We secretly ran away, to town.
I was 19 years old and fell in love with another inmate. I became pregnant, but a pregnant woman was not allowed at Bethesda. We were transported to Chatillon [where relations between men and women were permitted].
… the river was full of fish … I like fishing. The river [also] separated us from the rest of the world. Some of the inmates were looking for freedom. They escaped in a dugout canoe. Water entered the little boat, but they had no fear.
3.2. The Patients’ View: Entanglement of Culture and Nature
3.2.1. The Explanation of Leprosy by Patients
The Narrative of Diana (Animal Totemism, Treef, and Medical Pluralism)
My illness is not something of God. My mother did not feel well, she lay down and fell asleep. In a dream, an old woman appeared to her and said, “What you’ve done with my child will also happen to your child.” When my mother woke up, she called my dad, “Eddy, come on, did you do anything?” He replied, “That rotten iguana creeping around here, I have nothing to do with that animal. I threw stones at her, I hit her.” With a stone, my father mutilated the toes of the unborn baby iguana in the belly of mother iguana. The iguana was pregnant, just like my mother, who was at the time pregnant with me. When my fingers were crooked in my 13th year, my mom knew immediately: “Indeed, it was not good what my husband did then, throwing stones … those stones damaged the toes of the baby iguana, that’s why my child’s fingers became crooked.”
My mother said that I had a treef: pork and unscaled fish. I was lucky that these things were not prepared in Majella. They did eat salted fish there, but that is scaled fish. Maybe the nuns had spoken with the “bigi sma” (elder wise women)10, and on their advice the meals for the patients were adapted. There was a time that I did believe that you could get leprosy through treef, but later on I understood that this was a wrong idea and now I eat everything.
In her narrative, Diana also presents a modern, Western concept to explain her leprosy:
I know that leprosy is simply caused by a bacillus that comes into your body, yet I do not believe that this story of infectivity of leprosy is entirely true. The doctors who came into contact with the patients did not get leprosy anyway?
In 1948, when I was 11 years old, Doctor Gehr and Doctor Bueno de Mesquita brought the [new] medicine to Majella. And that’s why people could be dismissed in the 1950s. We were cured by the drug from America. [Originally] I was not treated with oso-dresi (traditional medication), my mother did not know those things. But after being dismissed from Majella she gave me Neem drink once a week. She said, “It’s something to purify blood.”
The Narrative of Kromo and Pawiro (Animal Totemism and Medical Pluralism)
Kromo, a Javanese male patient (1936) who was segregated in Chatillon from the 1960s, explains,
The Javanese people in Commewijne were afraid to go to Chatillon because they believed that a snake was living under the bridge or under the director’s house. It was told that this snake would eat them. I’ve looked around, but never saw that snake. I think it was nonsense. I was not afraid at Chatillon.
My mother had taken me to a traditional healer to protect me so that they would not send me to Chatillon. In the past, many parents were afraid to lose their children and many died in Chatillon,
where a man-eating snake lived and that’s why many Javanese went to a traditional healer … Yes, that snake eats people, living people. They say when someone wants to go home, they jail that person in a guardhouse rather than taking the person home. Then the snake comes to eat that person in the night.
The Narrative of Losita (Sand is the Tyina, the Taboo)
My sister fought with another woman—it was an argument related to my sister’s husband. That woman took sand and threw it on my sister. The sand also hit me. My sister got bumps, so did I. Sand is my sister’s tyina. It’s my tyina too, because we have the same father.
Discussion of the Patients’ Explanations
Treef and Tyina
3.2.2. Use of Plants for the Treatment of Leprosy
3.2.3. Neighboring Countries
3.3. Natural Environment: the Presence of Leprosy Bacterium DNA in the Soil of the Deserted Settlements
We pass the ruins of the housing of staff and inmates on the former leprosy colony Chatillon. They are overgrown with low vegetation and high trees, including palms with perilous thorns. The terrain is uneven, dotted with shallow puddles. Trunks of fallen trees litter the forest floor and as we walk through, we suffer an aerial attack by a swarm of bees and run for our lives. “Those were the deadly Brazilian bees, for sure,” our guide tells us. As he is speaking, his sharp eyes pick out a tortoise, its shell damaged with cracks running through the hard surface. Still alive, he picks it up. “The poor creature probably survived a swipe by a jaguar,” he says, “we’ll take it back to camp.” [22] (pp. 44–45).
4. Concluding Remarks: A Call for an Ecological Approach
5. Epilogue: The Future of Former Surinamese Hansen’s Disease Settlements
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zhang, G.; Li, W.; Yan, L.; Yang, Z.; Chen, X.; Zheng, T.; Ye, G. An epidemiological survey of deformities and disabilities among 14,257 cases of leprosy in 11 counties. Lepr. Rev. 1993, 64, 143–149. [Google Scholar]
- Deps, P.; Cruz, A. Why we should stop using the word leprosy. Lancet Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Vogelsang, T.M. Gerhard Henrik Armauer Hansen 1841–1912. The discoverer of the leprosy bacillus. His life and his work. Int. J. Lepr. Other Mycobact. Dis. 1978, 46, 257–332. [Google Scholar] [PubMed]
- Han, X.Y.; Seo, Y.H.; Sizer, K.C.; Schoberle, T.; May, G.S.; Spencer, J.S.; Li, W.; Nair, R.G. A new Mycobacterium species causing diffuse lepromatous leprosy. Am. J. Clin. Pathol. 2008, 130, 856–864. [Google Scholar] [CrossRef] [PubMed]
- Hatta, M.; van Beers, S.M.; Madjid, B.; Djumadi, A.; de Wit, M.Y.; Klatser, P.R. Distribution and persistence of Mycobacterium leprae nasal carriage among a population in which leprosy is endemic in Indonesia. Trans. R. Soc. Trop. Med. Hyg. 1995, 89, 381–385. [Google Scholar] [CrossRef]
- Job, C.K.; Jayakumar, J.; Kearney, M.; Gillis, T.P. Transmission of leprosy: A study of skin and nasal secretions of household contacts of leprosy patients using PCR. Am. J. Trop. Med. Hyg. 2008, 78, 518–521. [Google Scholar] [CrossRef]
- Turankar, R.P.; Lavania, M.; Singh, M.; Sengupta, U.; Siva Sai, K.; Jadhav, R.S. Presence of viable Mycobacterium leprae in environmental specimens around houses of leprosy patients. Indian J. Med. Microbiol. 2016, 34, 315–321. [Google Scholar]
- Mohanty, P.S.; Naaz, F.; Katara, D.; Misba, L.; Kumar, D.; Dwivedi, D.K.; Tiwari, A.K.; Chauhan, D.S.; Bansal, A.K.; Tripathy, S.P.; et al. Viability of Mycobacterium leprae in the environment and its role in leprosy dissemination. Indian J. Dermatol. Venereol. Leprol. 2016, 82, 23–27. [Google Scholar] [CrossRef]
- Walsh, G.P.; Storrs, E.E.; Burchfield, H.P.; Cotrell, E.H.; Vidrine, M.F.; Binford, C.H. Leprosy-like disease occurring naturally in armadillos. J. Reticuloendothel. Soc. 1975, 18, 347–351. [Google Scholar]
- Truman, R.W.; Singh, P.; Sharma, R.; Busso, P.; Rougemont, J.; Paniz-Mondolfi, A.; Kapopoulou, A.; Brisse, S.; Scollard, D.M.; Gillis, T.P.; et al. Probable zoonotic leprosy in the southern United States. N. Engl. J. Med. 2011, 364, 1626–1633. [Google Scholar] [CrossRef]
- Avanzi, C.; Del-Pozo, J.; Benjak, A.; Stevenson, K.; Simpson, V.R.; Busso, P.; McLuckie, J.; Loiseau, C.; Lawton, C.; Schoening, J.; et al. Red squirrels in the British Isles are infected with leprosy bacilli. Science 2016, 354, 744–747. [Google Scholar] [CrossRef] [PubMed]
- Plouvier, D.; Gomes, L.; Verweij, P.; Verlinden, N. Living Guianas; WWF: Gland, Switzerland, 2012; pp. 8–9. Available online: https://wwf.panda.org/?306012/The-Living-Guianas-Report (accessed on 10 December 2019).
- Helman, A. Kroniek van Eldorado. Boek I Folteraars over en Weer; Globe Pocket, In de Knipscheer: Amsterdam, The Netherlands, 1995; pp. 26–38. [Google Scholar]
- Van Andel, T.; Ruysschaert, S. Medicinale en Rituele Planten van Suriname; KIT Publishers: Amsterdam, The Netherlands, 2011; p. 7. [Google Scholar]
- Funk, V.; Hollowell, T.; Berry, P.; Kelloff, C.; Alexander, S.N. Checklist of the Plants of the Guiana Shield (Venezuela: Amazonas, Bolivar, Delta Amacuro; Guyana, Surinam, French Guiana); Contributions from the United States National Herbarium 55:1-584 (2007); Department of Botany National Museum of Natural History: Washington, DC, USA, 2007; p. 2. [Google Scholar]
- De Dijn, B. Natural History and Ecology of Suriname; LM publishers: Volendam, The Netherlands, 2018; pp. 4–480. [Google Scholar]
- Buddingh’, H. Geschiedenis van Suriname; Het Spectrum BV: Utrecht, the Netherlands, 1995; pp. 9–20. [Google Scholar]
- Van Stipriaan, A. Surinaams Contrast; KITLV Uitgeverij: Leiden, the Netherlands, 1995; pp. 33–37. [Google Scholar]
- Hoogbergen, W. ‘De Bosnegers zijn Gekomen’! Prometheus: Amsterdam, The Netherlands, 1992; pp. 1–38. [Google Scholar]
- Ankum-Houwink, J.C. Chinese kontraktarbeiders in de 19e eeuw. OSO Tijdschr. voor Surinamistiek 1985, 4, 181–186. [Google Scholar]
- Hoefte, R. Control and Resistance: Indentured Labor in Suriname. New West Indian Guide 1997, 61, 1–22. [Google Scholar] [CrossRef]
- Menke, H.; Pieters, T. Deel 1 Historische ontdekkingsreis; over kolonialisme, slavernij, een raadselachtige ziekte en een ongrijpbare bacterie. In De tenen van de Leguaan, Verhalen uit de Wereld van Surinaamse Leprapatiënten; Menke, H., Pieters, T., Reyme, M., Menke, J., Eds.; LM Publishers: Volendam, The Netherlands, 2019; pp. 11–72. [Google Scholar]
- Edmond, R. Leprosy and Empire A Medical and Cultural History; Cambridge University Press: Cambridge, UK, 2006; p. 55. [Google Scholar]
- Abernethy, D.B. The Dynamics of Global Dominance: European O zxverseas Empires. 1415–1980; Yale University Press: New Haven, CT, USA, 2001. [Google Scholar]
- Mertens, M. Van ‘Triomfalisme’ naar ‘Postkolonialisme’: Trends in de Geschiedschrijving van de Tropische Geneeskunde. Studium 2009, 2, 78–91. [Google Scholar] [CrossRef]
- Arnold, D. Introduction: Disease, Medicine and Empire. In Imperial Medicine and Indigenous Society; Arnold, D., Ed.; Manchester University Press: Manchester, UK, 1998. [Google Scholar]
- MacLeod, R. Preface. In Disease, Medicine and Empire: Perspectives on Western Medicine and the Experience of European Expansion; MacLeod, R., Lewis, M., Eds.; Routledge: London, UK, 1988. [Google Scholar]
- Menke, H.E.; Snelders, S.; Pieters, T. Leprosy Control and Contagionism in Suriname. Acad. J. Sur. 2011, 2, 168–175. [Google Scholar]
- Reyme, M.; Menke, J. Deel 2 De wereld van de Surinaamse leprapatiënt I Verhalen over liefde en haat, geloof en vloek, medeleven en uitsluiting. In De Tenen van de Leguaan Verhalen uit de Wereld van Surinaamse Leprapatiënten; Menke, H., Pieters, T., Reyme, M., Menke, J., Eds.; LM Publishers: Volendam, The Netherlands, 2019; pp. 73–134. [Google Scholar]
- Ramdas, S.; Menke, H.; Pieters, T.; Menke, J. Deel 3 De wereld van de Surinaamse leprapatiënt II Analyse: Over stigma, pluralisme, treef en tyina. In De Tenen van de Leguaan Verhalen uit de Wereld van Surinaamse Leprapatiënten; Menke, H., Pieters, T., Reyme, M., Menke, J., Eds.; LM Publishers: Volendam, The Netherlands, 2019; pp. 162–163. [Google Scholar]
- Weiss, H. Vier maanden in Suriname; G. F. Callenbach: Nijkerk, The Netherlands, 1915; pp. 61–72. [Google Scholar]
- Schuitemaker, E.P. De Lepra en de Gouvernementsleproserie in Suriname met Kaart en elf Platen; J.H. de Bussy: Amsterdam, The Netherlands, 1915. [Google Scholar]
- Snelders, S. Leprosy and Colonialism. Suriname under Dutch rule, 1750–1950; Manchester University Press: Manchester, UK, 2017. [Google Scholar]
- Proust, A. Essai sur L’hygiène Internationale, Ses Applications Contre la Peste, la Fièvre Jaune et le Choléra Asiatique (Avec une Carte Indiquant la Marche des Epidémies de Choléra); G. Masson: Paris, France, 1873; pp. 52–53. [Google Scholar]
- Weismann, G. Ebola, dynamin, and the cordon sanitaire of Dr. Adrien Proust. FASEB J. 2015, 29, 1–4. [Google Scholar] [CrossRef][Green Version]
- Leydesdorff, S. De Mensen en de Woorden; J.M. Meulenhoff: Amsterdam, The Netherlands, 2004; pp. 23–42. [Google Scholar]
- Tió-Coma, M.; Wijnands, T.; Pierneef, L.; Schilling, A.K.; Alam, K.; Roy, J.C.; Faber, W.R.; Menke, H.; Pieters, T.; Stevenson, K.; et al. Detection of Mycobacterium leprae DNA in soil: Multiple needles in the haystack. Sci. Rep. 2019, 9, 3165. [Google Scholar] [CrossRef]
- Van Dissel, J.T.; Pieters, T.; Geluk, A.; Maat, G.; Menke, H.E.; Tió-Coma, M.; Altena, E.; Laros, J.F.J.; Adhin, M.R. Archival, paleopathological and aDNA-based techniques in leprosy research and the case of Father Petrus Donders at the Leprosarium ‘Batavia’, Suriname. Int. J. Paleopathol. 2019, 27, 1–8. [Google Scholar] [CrossRef]
- Snelders, S. Leprosy and Slavery in Suriname: Godfried Schilling and the Framing of a Racial Pathology in the Eighteenth Century. Soc. Hist. Med. 2013, 26, 432–450. [Google Scholar] [CrossRef]
- Fermin, P. Traité des Maladies Fréquentes á Surinam et des Remèdes le plus Propres à les Guérir. Jacques Lekens: Maastricht, The Netherlands, 1764; p. 127. [Google Scholar]
- Schilling, G.W. Verhandeling over de Melaatschheid. Ph.D. Thesis, Utrecht University, Utrecht, The Netherlands, 1769. [Google Scholar]
- Van Hasselaar, A. Beschrijving der in de Kolonie Suriname Voorkomende Elephantiasis en Lepra (Melaatschheid). Ph.D. Thesis, Amsterdam University, Amsterdam, The Netherlands, 1835. [Google Scholar]
- Ter Beek, J.P. Dissertatio Inauguralis de Elephantiasis Surinamensis. Ph.D. Thesis, Leiden University, Leiden, The Netherlands, 1841. [Google Scholar]
- Drognat Landré, C.L. De la Contagion, Seule Cause de la Propagation de la Lèpre; Baillière: Paris, France, 1869. [Google Scholar]
- Danielssen, D.C.; Boeck, C.W. Traité de la Spédalskhed ou Elephantiasis des Grecs. Traduit du Norwégien sous les Yeux de Mr Danielssen par L. A. Cosson (de Nogaret) avec un Atlas de 24 Planches Colorées; Baillière: Paris, France, 1848. [Google Scholar]
- Report on Leprosy by the Royal College of Physicians. Prepared for, and Published by Her Majesty ´s Secretary of State for the Colonies; with an Appendix; Eyre and Spottiswoode: London, UK, 1867.
- Irgens, L.M. Leprosy in Norway: An interplay of research and public health work. Int. J. Lepr. Other Mycobact. Dis. 1973, 41, 189–198. [Google Scholar]
- Menke, H.E.; Faber, W.R.; Pieters, T. Charles Louis Drognat Landré and Gerhard Henrik Armauer Hansen. Contribution from a Dutch colony to the discovery of the leprosy bacterium. Lepr. Rev. 2010, 81, 82–86. [Google Scholar] [PubMed]
- Snelders, S.; van Bergen, L.; Huisman, M. Leprosy and the Colonial Gaze: Comparing the Dutch West and East Indies, 1750–1950. Soc. Hist. Med. 2020. Available online: https://academic.oup.com/shm/advance-article/doi/10.1093/shm/hkz079/5681883?guestAccessKey=554dd703-2e1e-4253-9328-68d6e9d1efaf (accessed on 6 January 2020).
- Ackerknecht, E.H.; Fielding, H. Garrison lecture: Anticontagionism between 1821 and 1867. Bull Hist. Med. 1948, 22, 562–593. [Google Scholar]
- Schiltkamp, J.A.; de Smidt, J.T. West Indisch Plakaatboek. Plakaten, Ordonnantiën en Andere Wetten Uitgevaardigd in Suriname II, 1761–1816; S. Emmering: Amsterdam, The Netherlands, 1973. [Google Scholar]
- Vernooij, J. Een opvallende relatie. De Rooms Katholieke kerk en lepra in Suriname. OSO Tijdschr. voor Surinamistiek 2003, 22, 62–68. [Google Scholar]
- Kapper, A. Plantages langs de Commewijnerivier, de goudkust van Suriname. Vitruvius 2011, 4, 36–42. [Google Scholar]
- Bosser, A. Beknopte Geschiedenis der Katholieke Missie in Suriname; M. Alberts: Gulpen, The Netherlands, 1884; p. 171. [Google Scholar]
- van der Aa, A.J. Aardrijkskundig Woordenboek der Nederlanden, Tweede deel B; Jacobus Noorduyn: Gorinchem, The Netherlands, 1840; p. 168. [Google Scholar]
- Foucault, M. Madness and civilization: A History of Insanity in the Age of Reason; Routledge: London, UK, 2001; pp. 38–40. [Google Scholar]
- Lens, T. Lepra in Suriname. Elsevier’s Geïllustreerd Maandschr. 1895, 5, 521–552. [Google Scholar]
- Postma, J. De leprozerie Bethesda tussen 1897 en 1928. OSO Tijdschr. voor Surinamistiek 2003, 22, 69–82. [Google Scholar]
- Zaalberg, H.H. De Melaatschen in Suriname en hun Verpleging; G.C.Visser: Den Haag, The Netherlands, 1904; pp. 18–19. [Google Scholar]
- Merritt, J.G.; Satterlee, A. Historical Dictionary of the Salvation Army; Rowman and Littlefield: London, UK, 2017; pp. 203–209. [Google Scholar]
- Hira, S. Eddy Jharap Geloof in Eigen Kunnen; Amrit Consultancy: Den Haag, The Netherlands, 2011; pp. 45–65. [Google Scholar]
- Van Hinte-Rustwijk, D.; van Steenderen-Rustwijk, G. Van bedrijfsschade tot verzuilde paria naar ex-Hansen cliënt. OSO Tijdschr. voor Surinamistiek 2003, 22, 10–20. [Google Scholar]
- Haekel, J. Totemism. in Encyclopaedia Britannica. Available online: https://www.britannica.com/topic/totemism-religion (accessed on 6 January 2020).
- Vruggink, H. Javaanse volksverhalen: Een eerste kennismaking. Oso Tijdschr. voor Surinamistiek 1989, 8, 170–183. [Google Scholar]
- Landré, C. Over de OORZAKEN der verbreiding van de lepra. Een Waarschuwend Woord Hoofdzakelijk Gericht tot de Bewoners van Suriname; Martinus Nijhoff: Den Haag, The Netherlands, 1889. [Google Scholar]
- Lampe, P.H.J. ‘Het Surinaams treefgeloof’ Een volksgeloof betreffende het ontstaan van de melaatschheid. De West-Indische Gids 1929, 10, 545–568. [Google Scholar] [CrossRef]
- Benjamins, H.D. Treef en lepra in Suriname. De West-Indische Gids 1930, 11, 187–218. [Google Scholar] [CrossRef]
- Van Andel, T. The reinvention of household medicine by enslaved Africans in Suriname. Soc. Hist. Med. 2016, 29, 676–694. [Google Scholar] [CrossRef]
- Girvan, N. Reinterpreting the Caribbean. In New Caribbean Thought; Meeks, B., Lindahl, F., Eds.; University of the West Indies Press: Kingston, Jamaica, 2001. [Google Scholar]
- Anderson, N.R. “It’s Not Catching”: Hansen Home and the Local Knowledge of Leprosy in the Federation of St. Kitts and Nevis, West Indies. Master’s Thesis, University of Tennessee, Knoxville, Tennessee, 2005. Available online: http://trace.tennessee.edu/utk_gradthes/580 (accessed on 24 March 2020).
- Gampat, R. Guyana from Slavery to the Present. Volume 2. Major Diseases; Xlibris: Bloomington, Indiana, 2015; pp. 623–648. [Google Scholar]
- De Souza-Araujo, H.C. A la lepra na Guiana Francêsa in: O problema da lepra na America do Sul. Memórias do Inst. Oswaldo Cruz 1945, 43, 583–598. [Google Scholar] [CrossRef]
- White, C. Explaining a Complex Disease Process: Talking to Patients about Hansen’s Disease (Leprosy) in Brazil. Med Anthropol. Q. 2008, 19, 310–330. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, M.B.; Portela, J.M.; Li, W.; Jackson, M.; Gonzalez-Juarrero, M.; Hidalgo, A.S.; Belisle, J.T.; Bouth, R.C.; Gobbo, A.R.; Barreto, J.G.; et al. Evidence of zoonotic leprosy in Pará, Brazilian Amazon, and risks associated with human contact or consumption of armadillos. PLoS. Negl. Trop. Dis. 2018, 12. [Google Scholar] [CrossRef] [PubMed]
- WHO Weekly Epidemiological Record 2019, 94, 389–412. Available online: https://zeroleprosy.org/wp-content/uploads/2020/02/WHO-August-2019-Leprosy-Report.pdf (accessed on 24 March 2020).
- Ploemacher, T.; Faber, W.R.; Menke, H.; Rutten, V.; Pieters, T. Reservoirs and Transmission Routes of Leprosy; A Systematic Review. PLoS. Negl. Trop. Dis. Under review.
- Sitalsing, K. Boeroes een Familiegeschiedenis van Witte Surinamers; Uitgeverij Atlas Contact: Amsterdam, The Netherlands, 2016; p. 30. [Google Scholar]
| 1 | We are fully aware of the disadvantages of the word leprosy, as explained by Deps and Cruz (2020, see reference [2]), but we have deliberately chosen to use the word in this historical article when necessary, in addition to ‘Hansen’s disease.’ |
| 2 | The transcribed interviews are kept in the National Archive of Suriname (www.nationaalarchief.sr). |
| 3 | In their paper, Snelders, et al. use the term ‘colonial gaze’ to refer to the ways in which plantation owners, colonial administrators, doctors, and surgeons legitimised compulsory segregation of leprosy sufferers who were no longer of use on the plantation or as labourers in general.). |
| 4 | Publicatie van 15 september 1830. Gouvernements Blad van Suriname No 13. |
| 5 | Landsverordening van 23 maart 1960 houdende bepalingen ter wering en bestrijding van lepra. Gouvernementsblad van Suriname no 37, 1960. |
| 6 | Peerke (Petrus) Donders became an icon of Roman Catholic missionary work and was beatified by the Pope in 1982. |
| 7 | Bueno de Mesquita, S.J. Leprosy Annual report of the year 1952. Van der Kuyp files, National Archive of Suriname (www.nationaalarchief.sr). |
| 8 | Surinamese newspaper ‘de West: nieuwsblad uit en voor Suriname’, 23-02-1948. Available online: https://www.delpher.nl/nl/kranten. |
| 9 | Tyina is the Surinamese spelling of this word. It can be found in the literature as tchina and kina. |
| 10 | These are elder female leprosy inmates (generally of African-Surinamese descent) who assisted, informed, and advised the European caretakers in the leprosaria on matters related to life in Suriname. |
| 11 | Winti is a traditional African-Surinamese religion. |
| 12 | Treef is the Dutch spelling and trefu is the Surinamese spelling of this word. |
| 13 | |
| 14 | Personal information (received on 28 October 2019) from Roxane Schaub, leprosy researcher in French Guyana. |




{kind=link}
{kind=link}
{kind=link}
| Name | Authority | Opening | Closing | Location | Distance to Paramaribo (km) |
|---|---|---|---|---|---|
| Voorzorg | Colonial government | 1791 | 1823 | Saramacca river | 90 |
| Batavia | Colonial government, Roman Catholics | 1823 | 1896 | Coppename river | 40 |
| Gerardus Majella | Roman Catholics | 1895 | 1964 | Van Sommelsdijckse Creek | 0 |
| Groot Chatillon | Colonial government | 1896 | 1972 | Suriname river | 38 |
| Bethesda | Moravians | 1899 | 1933 | Suriname river | 38 |
| New Bethesda | Moravians | 1933 | 1964 | Suriname river | 10 |
| Cause According to the Patient | Sixteen Old Patients (Had Been Segregated) | Fourteen Young Patients |
|---|---|---|
| Infected (by other leprosy patient) | 8 | 5 |
| Bad hygiene | 1 | 1 |
| Inherited | 2 | 3 |
| Punished by God | 1 | 2 |
| Violating totem animal/winti11(curse) | 4 | 4 |
| Treef | 10 | 9 |
| Eating animal (not considered treef by the patient) | 0 | 3 |
| Other (prick by a thorn of a plant) | 1 | 0 |
| Treef | |
|---|---|
| 1 | Beef, monkey, milk, chicken egg, pumpkin, rice |
| 2 | Pork, unscaled fish |
| 3 | Turtle, tomato |
| 4 | Salted beef, tomato |
| 5 | Beef, milk, rice |
| 6 | Beef, tomato, rice |
| 7 | Parrot, podosiri (açai palm) |
| 8 | Turtle, monkey, iguana |
| 9 | Turtle, unscaled fish, pork |
| Scientific Name | Local Name | Use |
|---|---|---|
| Azadirachta indica A. | Neem | Local application, drinking a tea |
| Eclipta prostrata | Rosa wiwiri | Local application |
| Senna alata | Slabriki | Local application |
| Cordia curassaviva | Blaka uma | Local application |
| Elephantopus mollis | Snekibita | Drinking a tea |
| Cecropia peltata | Busipapaya | Drinking a tea |
| Cocos nucifera | Kokos | Local application |
| Citrus aurantifolia | Lemmetje | Local application |
| Alpinia officinarum | Laos | Local application |
| Curcuma domestica | Kurkuma | Local application |
| Manihot esculenta | Bitter cassava | Local application |
| Montrichardia arborescens | Mokomoko | Local application |
| Aloe vera | Semprefisi | Local application |
| Scientific Name of Plants | Local Name | How to Use |
|---|---|---|
| Annona reticulate | kasyuma | Drinking concoction of the bark |
| Theobroma cacao | Cacao | Drinking tea from dried seeds |
| Lycopodiella cemua | Amoraman | Drinking tea from the plant |
| Zygia latifolia | Boasiman weko or Kokobe bisonki | Drinking tea of leaves; washing of the body with the same brew |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Menke, H.; Pieters, T.; Menke, J. How Colonial Power, Colonized People, and Nature Shaped Hansen’s Disease Settlements in Suriname. Societies 2020, 10, 32. https://doi.org/10.3390/soc10020032
Menke H, Pieters T, Menke J. How Colonial Power, Colonized People, and Nature Shaped Hansen’s Disease Settlements in Suriname. Societies. 2020; 10(2):32. https://doi.org/10.3390/soc10020032
Chicago/Turabian StyleMenke, Henk, Toine Pieters, and Jack Menke. 2020. "How Colonial Power, Colonized People, and Nature Shaped Hansen’s Disease Settlements in Suriname" Societies 10, no. 2: 32. https://doi.org/10.3390/soc10020032
APA StyleMenke, H., Pieters, T., & Menke, J. (2020). How Colonial Power, Colonized People, and Nature Shaped Hansen’s Disease Settlements in Suriname. Societies, 10(2), 32. https://doi.org/10.3390/soc10020032