
Effect of Uphill Running on VO2, Heart Rate and Lactate Accumulation on Lower Body Positive Pressure Treadmills

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Protocol and Test Design
2.3. Data Analysis
2.4. Statistics
3. Results
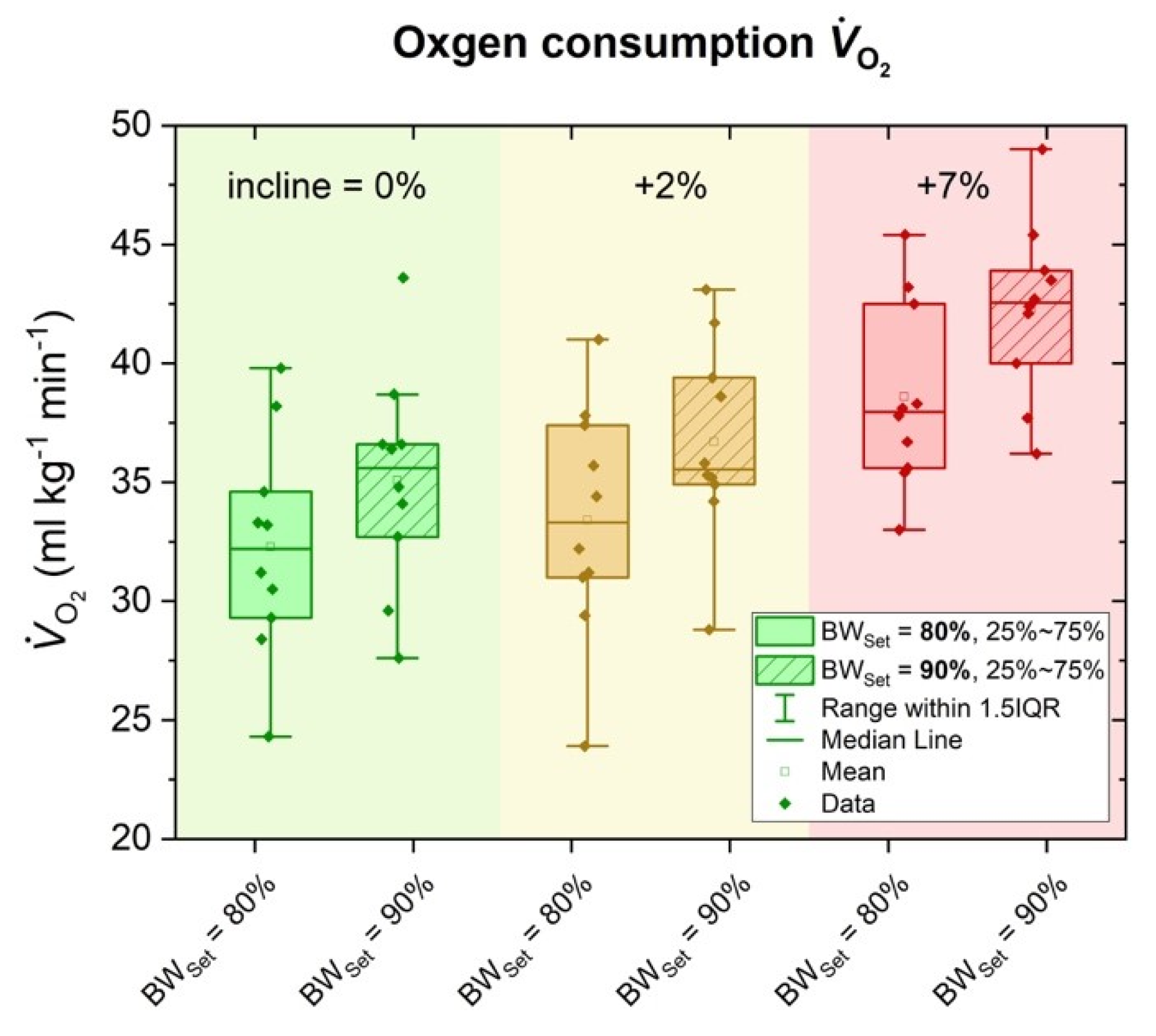
3.1. Oxygen Consumption (VO2)
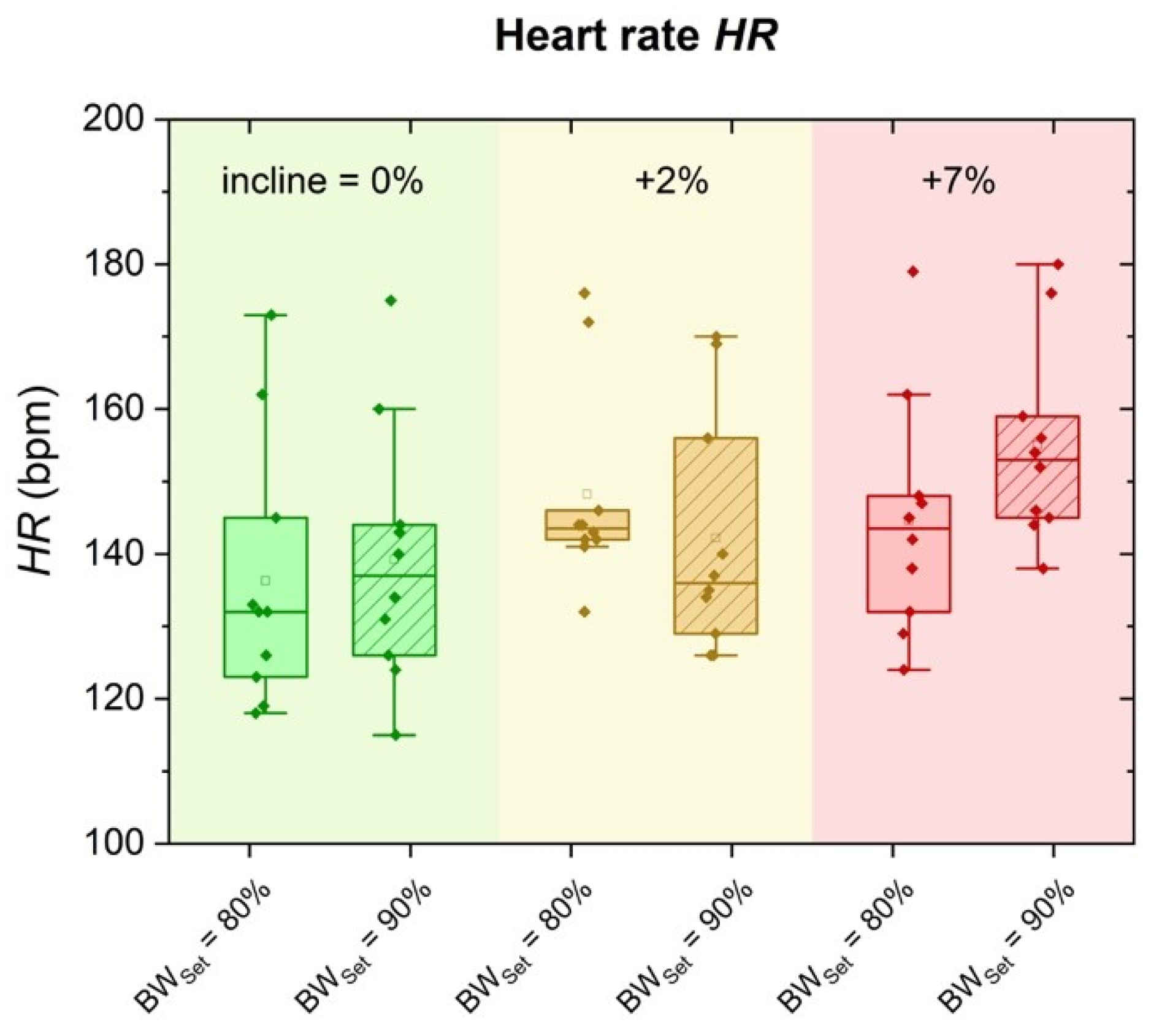
3.2. Heart Rate (HR)
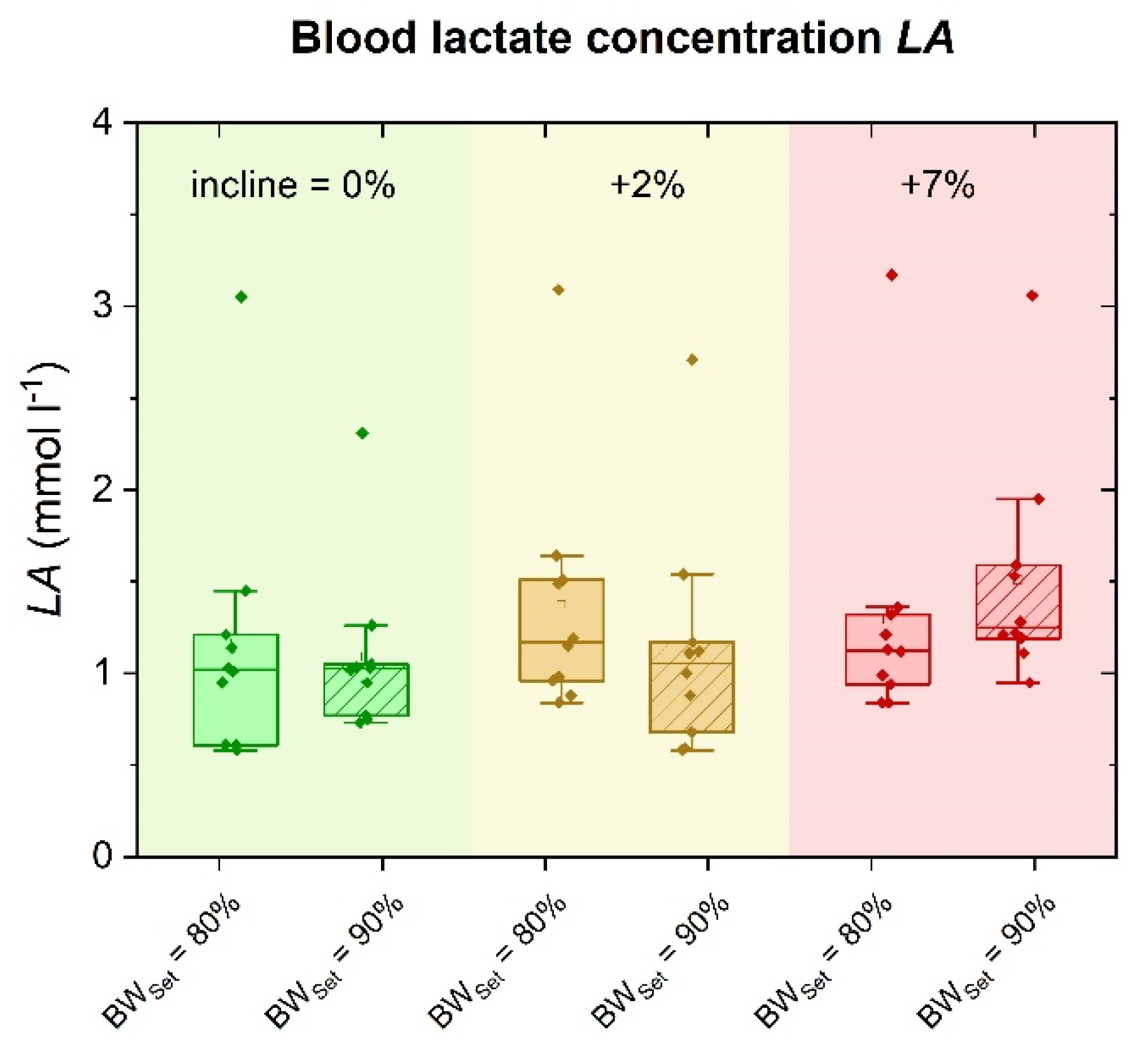
3.3. Blood Lactate Concentration (LA)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McNeill, D.K.; Kline, J.R.; de Heer, H.D.; Coast, J.R. Oxygen consumption of elite distance runners on an anti-gravity treadmill(R). J. Sports Sci. Med. 2015, 14, 333–339. [Google Scholar]
- Fleckenstein, D.; Ueberschär, O.; Wüstenfeld, J.C.; Wolfarth, B. Physiological and Metabolic Reaction to Lower Body Positive Pressure Treadmill Running. Dtsch. Z. Sportmed. 2020, 71, 11–18. [Google Scholar] [CrossRef]
- Raffalt, P.C.; Hovgaard-Hansen, L.; Jensen, B.R. Running on a Lower-Body Positive Pressure Treadmill: VO2max, Respiratory Response, and Vertical Ground Reaction Force. Res. Q. Exerc. Sport 2013, 84, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Farina, K.A.; Wright, A.A.; Ford, K.R.; Wirfel, L.A.; Smoliga, J.M. Physiological and Biomechanical Responses to Running on Lower Body Positive Pressure Treadmills in Healthy Populations. Sports Med. 2016, 47, 261–275. [Google Scholar] [CrossRef] [PubMed]
- Barnes, K.R.; Janecke, J.N. Physiological and Biomechanical Responses of Highly Trained Distance Runners to Lower-Body Positive Pressure Treadmill Running. Sports Med. Open 2017, 3, 41. [Google Scholar] [CrossRef] [PubMed]
- McNeill, D.K.P.; De Heer, H.D.; Williams, C.P.; Coast, J.R. Metabolic accommodation to running on a body weight-supported treadmill. Graefe’s Arch. Clin. Exp. Ophthalmol. 2015, 115, 905–910. [Google Scholar] [CrossRef] [PubMed]
- Kline, J.R.; Raab, S.; Coast, J.R.; Bounds, R.G.; McNeill, D.K.; de Heer, H.D. Conversion Table for Running on Lower Body Positive Pressure Treadmills. J. Strength Cond. Res. 2015, 29, 854–862. [Google Scholar] [CrossRef]
- Stucky, F.; Vesin, J.-M.; Kayser, B.; Uva, B. The Effect of Lower-Body Positive Pressure on the Cardiorespiratory Response at Rest and during Submaximal Running Exercise. Front. Physiol. 2018, 9, 34. [Google Scholar] [CrossRef] [PubMed]
- Gojanovic, B.; Cutti, P.; Shultz, R.; Matheson, G.O. Maximal Physiological Parameters during Partial Body-Weight Support Treadmill Testing. Med. Sci. Sports Exerc. 2012, 44, 1935–1941. [Google Scholar] [CrossRef]
- Grabowski, A.M. Metabolic and Biomechanical Effects of Velocity and Weight Support Using a Lower-Body Positive Pressure Device during Walking. Arch. Phys. Med. Rehabil. 2010, 91, 951–957. [Google Scholar] [CrossRef]
- Grabowski, A.M.; Kram, R. Effects of Velocity and Weight Support on Ground Reaction Forces and Metabolic Power during Running. J. Appl. Biomech. 2008, 24, 288–297. [Google Scholar] [CrossRef]
- Hoffman, M.D.; Donaghe, H.E. Physiological Responses to Body Weight–Supported Treadmill Exercise in Healthy Adults. Arch. Phys. Med. Rehabil. 2011, 92, 960–966. [Google Scholar] [CrossRef]
- Sainton, P.; Nicol, C.; Cabri, J.; Barthelemy-Montfort, J.; Berton, E.; Chavet, P. Influence of short-term unweighing and reloading on running kinetics and muscle activity. Graefe’s Arch. Clin. Exp. Ophthalmol. 2015, 115, 1135–1145. [Google Scholar] [CrossRef]
- Barnes, K.R.; Hopkins, W.G.; McGuigan, M.R.; Kilding, A.E. Effects of Different Uphill Interval-Training Programs on Running Economy and Performance. Int. J. Sports Physiol. Perform. 2013, 8, 639–647. [Google Scholar] [CrossRef]
- Midgley, A.W.; McNaughton, L.R.; Jones, A.M. Training to Enhance the Physiological Determinants of Long-Distance Running Performance. Sports Med. 2007, 37, 857–880. [Google Scholar] [CrossRef]
- Seiler, S. What is Best Practice for Training Intensity and Duration Distribution in Endurance Athletes? Int. J. Sports Physiol. Perform. 2010, 5, 276–291. [Google Scholar] [CrossRef]
- Tjelta, L.I. The training of international level distance runners. Int. J. Sports Sci. Coach. 2016, 11, 122–134. [Google Scholar] [CrossRef]
- Hollander, K.; Riebe, D.; Campe, S.; Braumann, K.-M.; Zech, A. Effects of footwear on treadmill running biomechanics in preadolescent children. Gait Posture 2014, 40, 381–385. [Google Scholar] [CrossRef]
- Squadrone, R.; Gallozzi, C. Biomechanical and physiological comparison of barefoot and two shod conditions in experienced barefoot runners. J. Sports Med. Phys. Fit. 2009, 49, 6–13. [Google Scholar]
- Borg, G. Perceived exertion as an indicator of somatic stress. Scand. J. Rehabil. Med. 1970, 2, 92–98. [Google Scholar] [PubMed]
- Robergs, R.A.; Dwyer, D.; Astorino, T. Recommendations for Improved Data Processing from Expired Gas Analysis Indirect Calorimetry. Sports Med. 2010, 40, 95–111. [Google Scholar] [CrossRef] [PubMed]
- Billat, V.L.; Slawinski, J.; Bocquet, V.; Demarle, A.; Lafitte, L.; Chassaing, P.; Koralsztein, J.-P. Intermittent runs at the velocity associated with maximal oxygen uptake enables subjects to remain at maximal oxygen uptake for a longer time than intense but submaximal runs. Graefe’s Arch. Clin. Exp. Ophthalmol. 2000, 81, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Kuipers, H.; Verstappen, F.T.J.; Keizer, H.A.; Geurten, P.; Van Kranenburg, G. Variability of Aerobic Performance in the Laboratory and Its Physiologic Correlates. Int. J. Sports Med. 1985, 6, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Xu, M.; Tu, J.; Wang, H.; Niu, X. Relationship between Omnibus and Post-hoc Tests: An Investigation of performance of the F test in ANOVA. Shanghai Arch Psychiatry 2018, 30, 60–64. [Google Scholar] [PubMed]
- Padulo, J.; Powell, U.; Milia, R.; Ardigò, L.P. A Paradigm of Uphill Running. PLoS ONE 2013, 8, e69006. [Google Scholar] [CrossRef]
- Goodwin, M.L.; Harris, J.E.; Hernández, A.; Gladden, L.B. Blood Lactate Measurements and Analysis during Exercise: A Guide for Clinicians. J. Diabetes Sci. Technol. 2007, 1, 558–569. [Google Scholar] [CrossRef]
- Davis, J.A. Anaerobic threshold: Review of the concept and directions for future research. Med. Sci. Sports Exerc. 1985, 17, 6–21. [Google Scholar] [CrossRef]
- Jensen, B.R.; Hovgaard-Hansen, L.; Cappelen, K.L. Muscle Activation and Estimated Relative Joint Force during Running with Weight Support on a Lower-Body Positive-Pressure Treadmill. J. Appl. Biomech. 2016, 32, 335–341. [Google Scholar] [CrossRef]
- Ueberschär, O.; Fleckenstein, D.; Wüstenfeld, J.C.; Warschun, F.; Falz, R.; Wolfarth, B. Running on the hypogravity treadmill AlterG® does not reduce the magnitude of peak tibial impact accelerations. Sports Orthop. Traumatol. 2019, 35, 423–434. [Google Scholar] [CrossRef]
- Moran, M.F.; Rickert, B.J.; Greer, B.K. Tibial Acceleration and Spatiotemporal Mechanics in Distance Runners during Reduced-Body-Weight Conditions. J. Sport Rehabil. 2017, 26, 221–226. [Google Scholar] [CrossRef]
- Vernillo, G.; Giandolini, M.; Edwards, W.B.; Morin, J.-B.; Samozino, P.; Horvais, N.; Millet, G.Y. Biomechanics and Physiology of Uphill and Downhill Running. Sports Med. 2017, 47, 615–629. [Google Scholar] [CrossRef] [PubMed]
- Gottschall, J.S.; Kram, R. Ground reaction forces during downhill and uphill running. J. Biomech. 2005, 38, 445–452. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Measure | Male (n = 10) (min–max) |
|---|---|
| Age (years) | 30.2 ± 3.4 (25.7–37.1) |
| Body mass (kg) | 73.1 ± 6.1 (63.7–82.2) |
| Body height (cm) | 178 ± 6 (166–185) |
| VO2max (mL min−1 kg−1) | 60.4 ± 4.2 (54.9–68.4) |
| vVO2max (km h−1) | 18.0 ± 1.6 (16.0–20.0) |
| HRmax (beats min−1) | 193 ± 8 (184–209) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fleckenstein, D.; Ueberschär, O.; Wüstenfeld, J.C.; Rüdrich, P.; Wolfarth, B. Effect of Uphill Running on VO2, Heart Rate and Lactate Accumulation on Lower Body Positive Pressure Treadmills. Sports 2021, 9, 51. https://doi.org/10.3390/sports9040051
Fleckenstein D, Ueberschär O, Wüstenfeld JC, Rüdrich P, Wolfarth B. Effect of Uphill Running on VO2, Heart Rate and Lactate Accumulation on Lower Body Positive Pressure Treadmills. Sports. 2021; 9(4):51. https://doi.org/10.3390/sports9040051
Chicago/Turabian StyleFleckenstein, Daniel, Olaf Ueberschär, Jan C. Wüstenfeld, Peter Rüdrich, and Bernd Wolfarth. 2021. "Effect of Uphill Running on VO2, Heart Rate and Lactate Accumulation on Lower Body Positive Pressure Treadmills" Sports 9, no. 4: 51. https://doi.org/10.3390/sports9040051
APA StyleFleckenstein, D., Ueberschär, O., Wüstenfeld, J. C., Rüdrich, P., & Wolfarth, B. (2021). Effect of Uphill Running on VO2, Heart Rate and Lactate Accumulation on Lower Body Positive Pressure Treadmills. Sports, 9(4), 51. https://doi.org/10.3390/sports9040051