
Recovery from Different High-Intensity Interval Training Protocols: Comparing Well-Trained Women and Men


 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
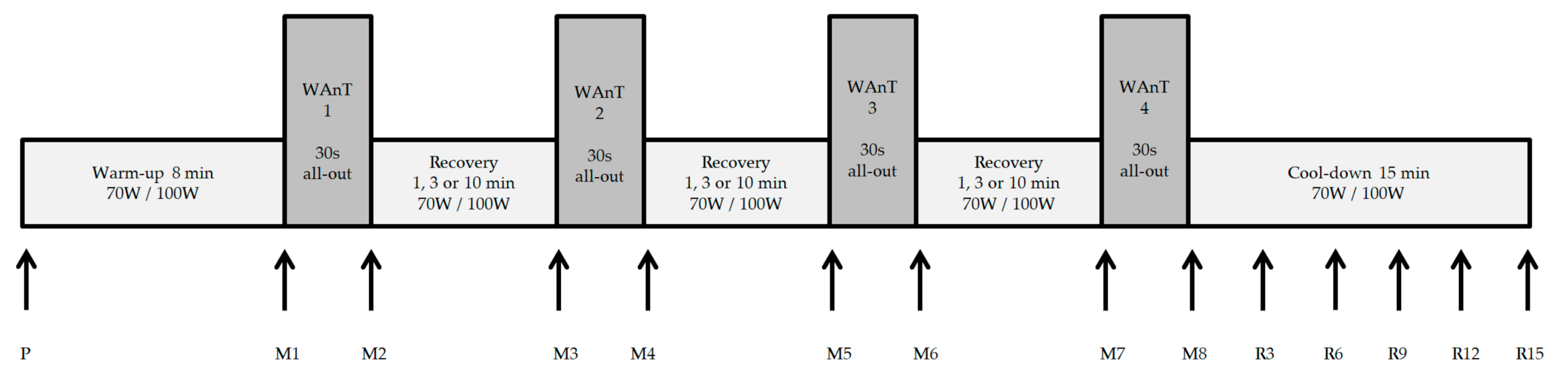
2.2. Test Protocol
2.3. Statistical Analysis
3. Results
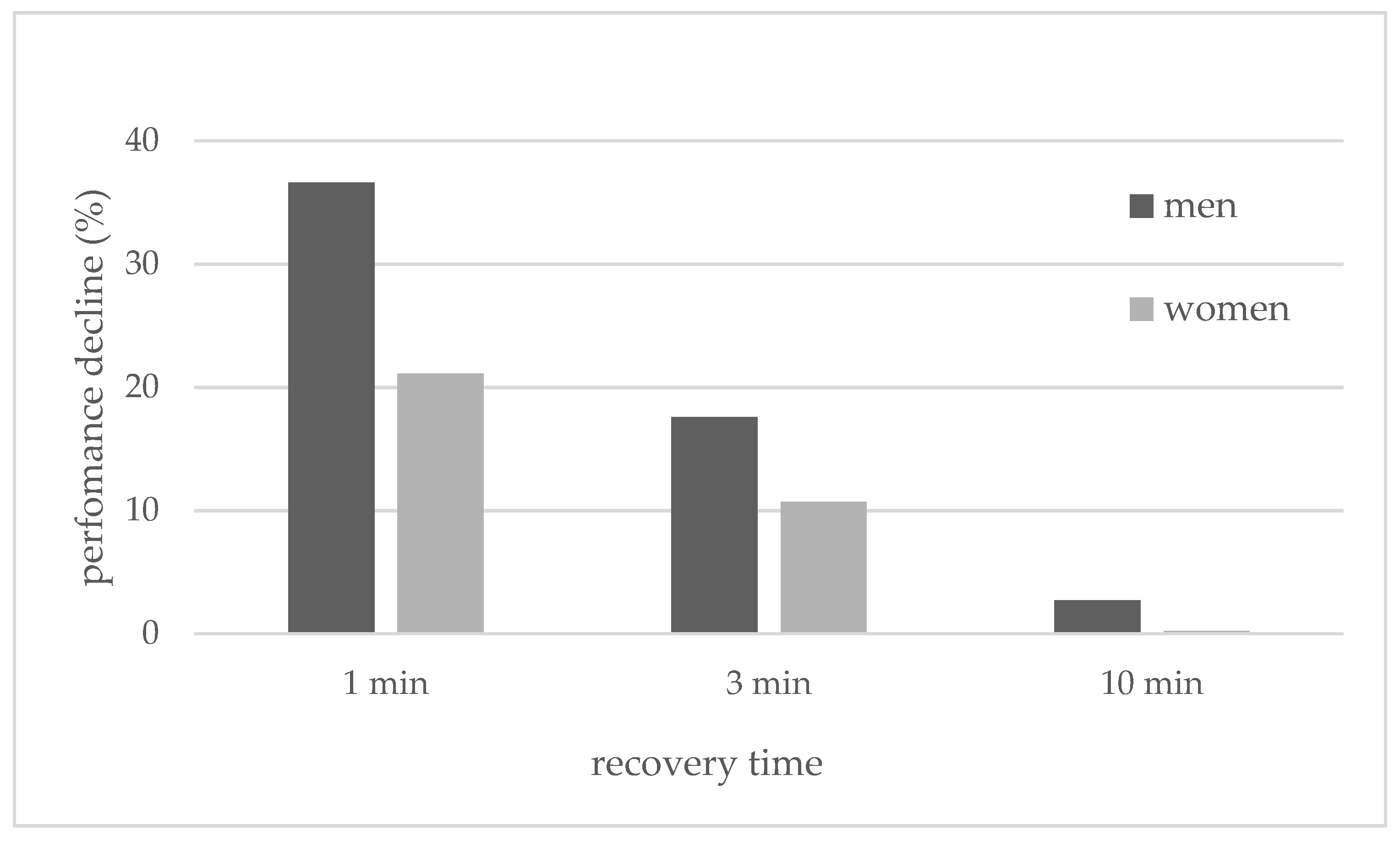
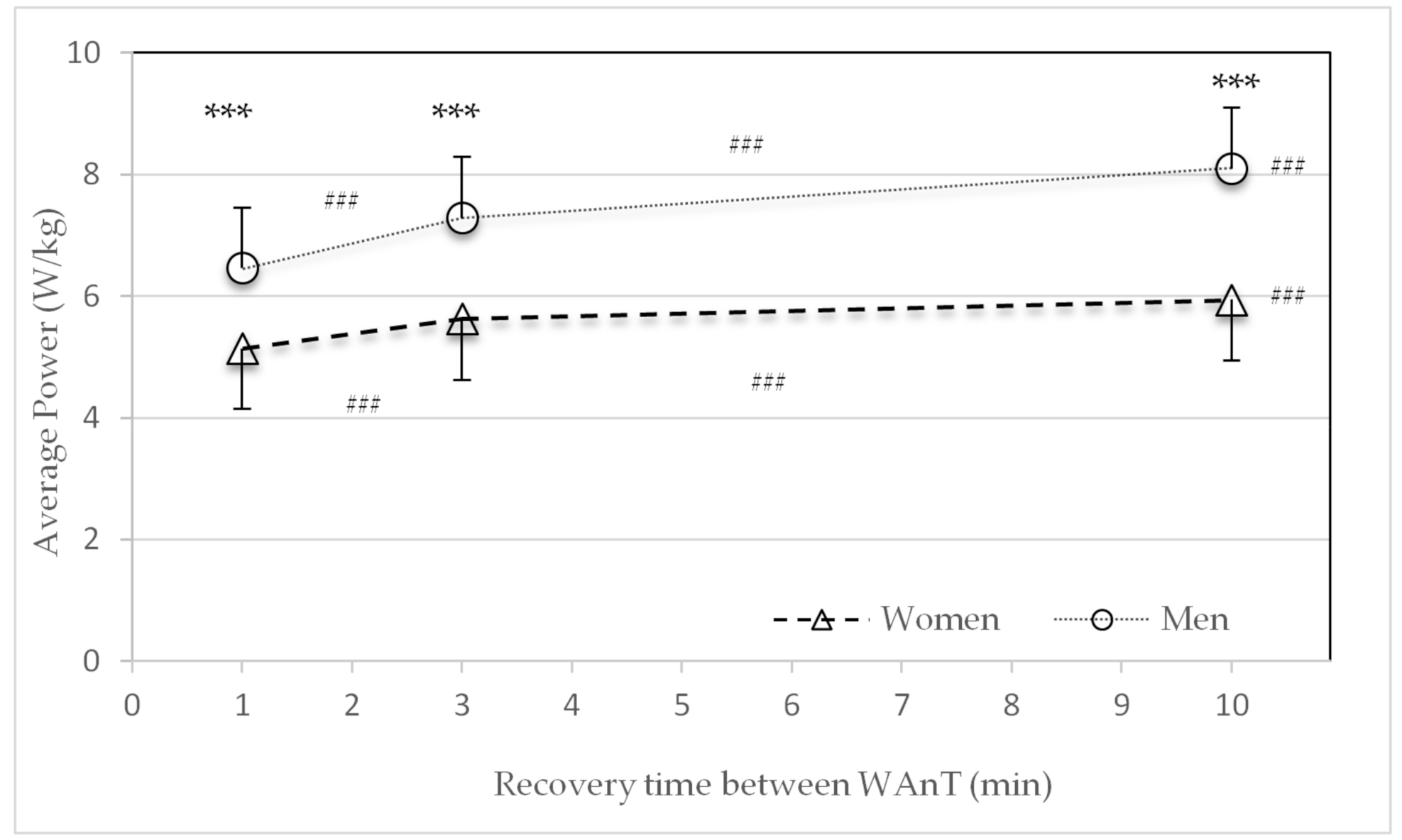
3.1. Power
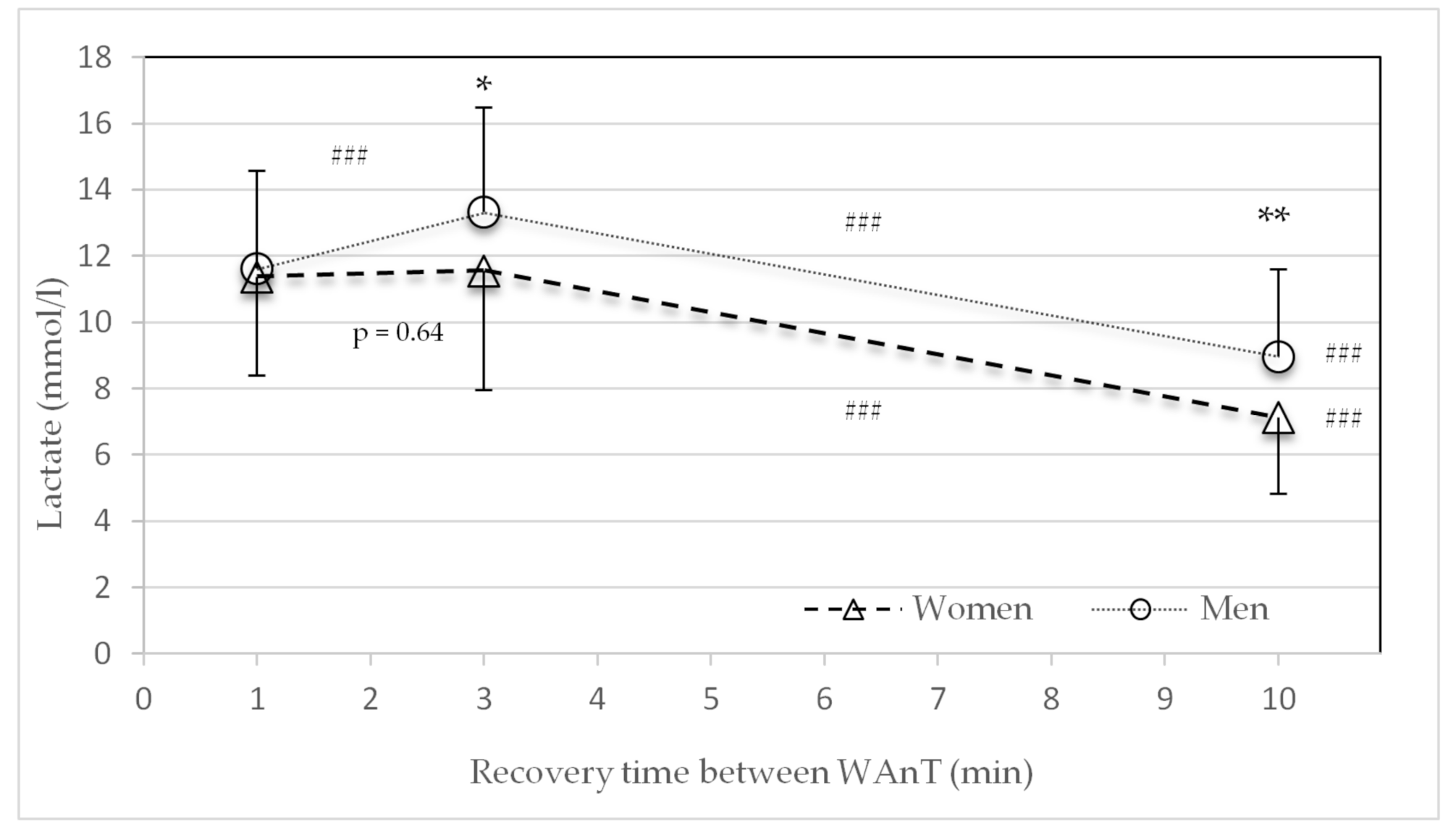
3.2. Lactate
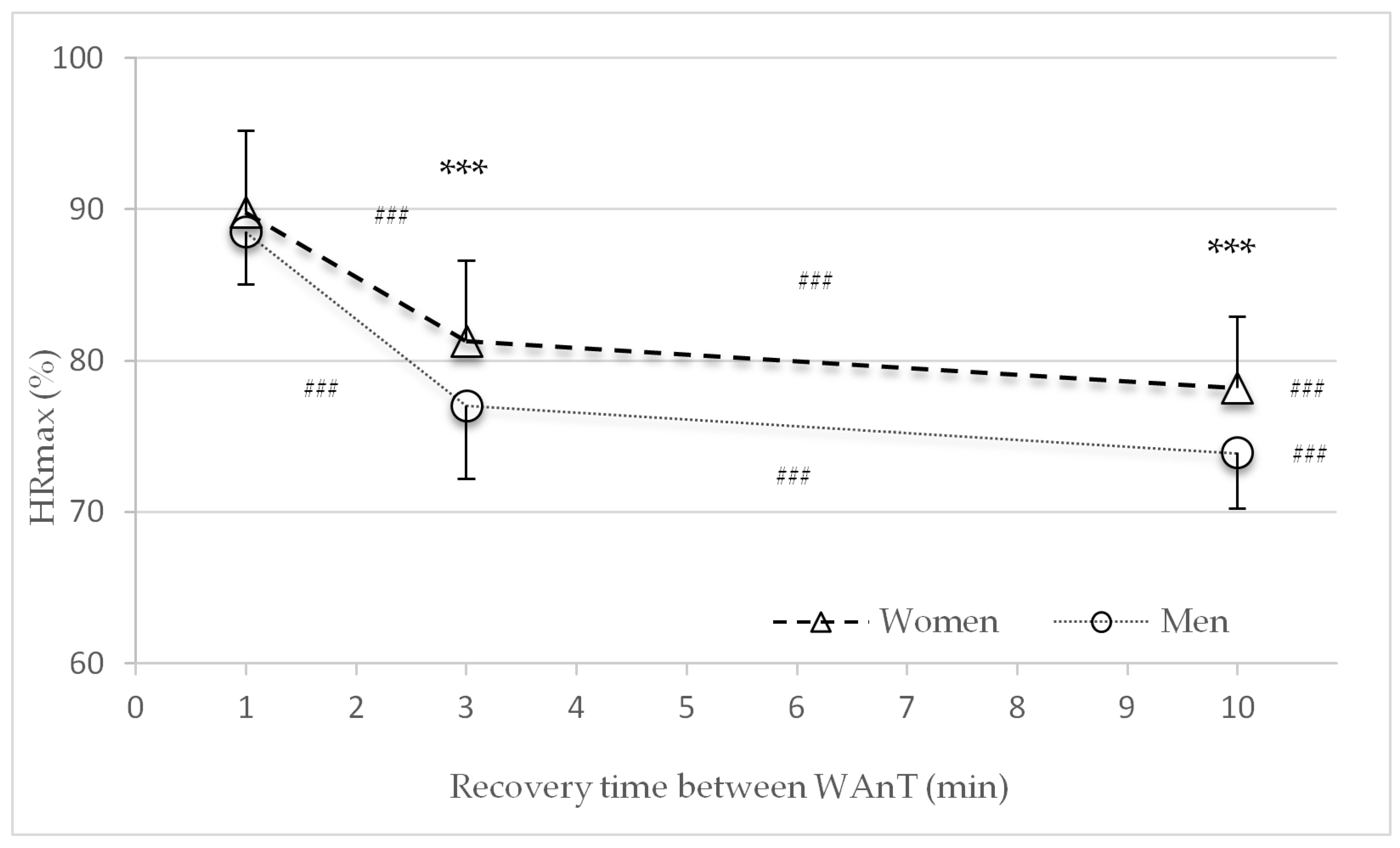
3.3. Heart Rate
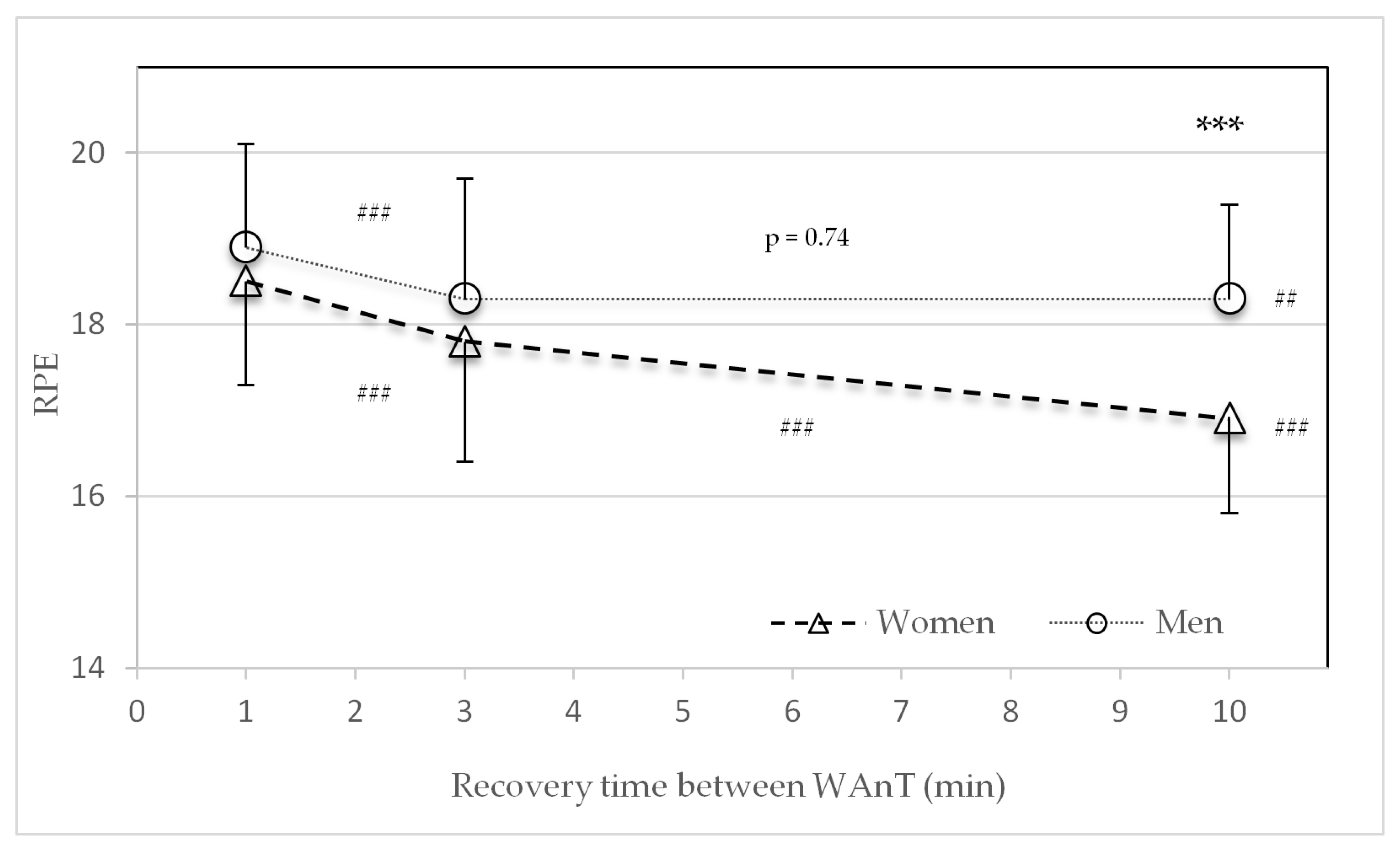
3.4. Subjective Rating of Perceived Exertion (RPE Scale)
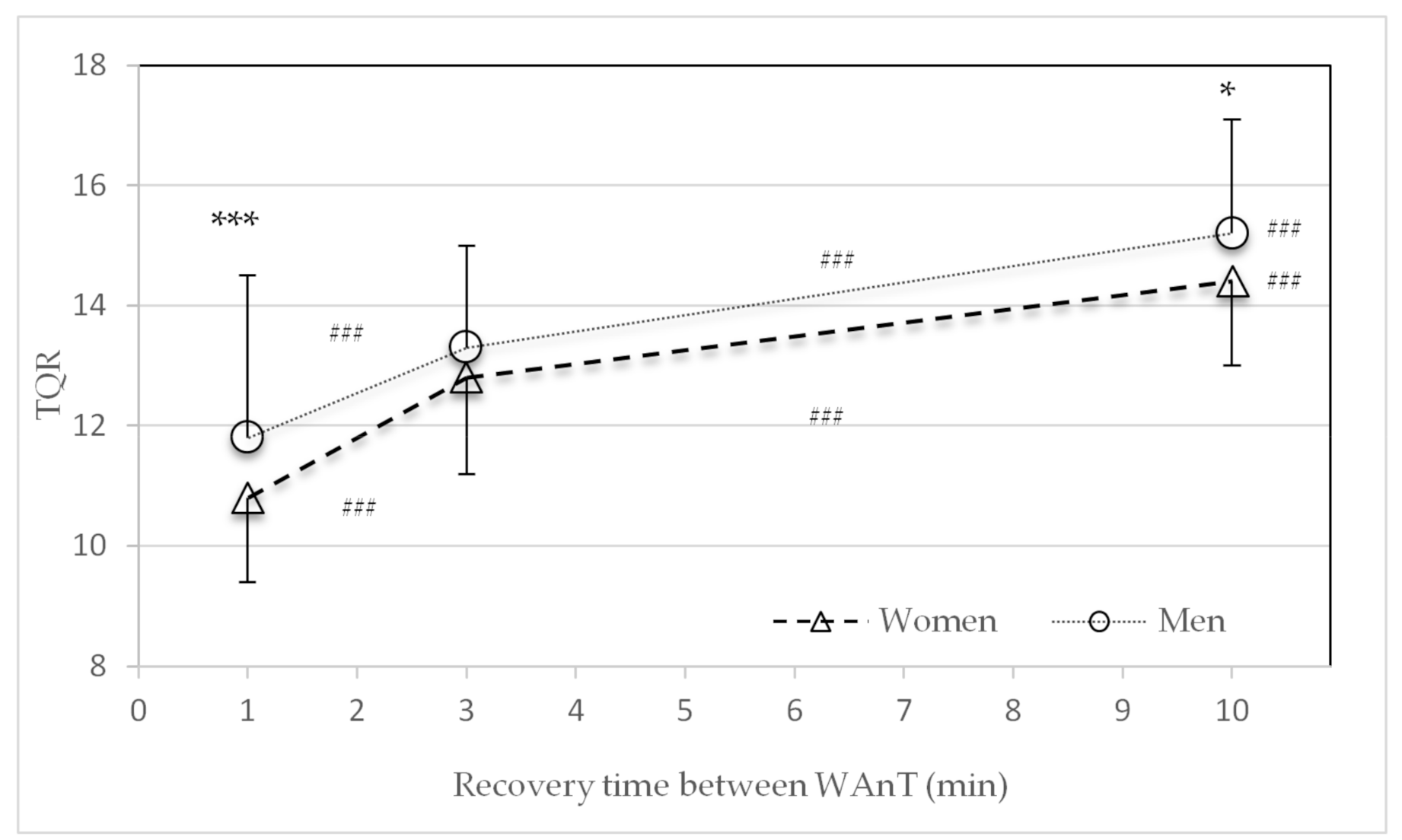
3.5. Subjective Recovery of Perceived Recovery (TQR Scale)
3.6. Ventilatory Parameter during Recovery
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Cicioni-Kolsky, D.; Lorenzen, C.; Williams, M.D.; Kemp, J.G. Endurance and sprint benefits of high-intensity and supramaximal interval training. Eur. J. Sport Sci. 2013, 13, 304–311. [Google Scholar] [CrossRef]
- Milanović, Z.; Sporiš, G.; Weston, M. Effectiveness of High-Intensity Interval Training (HIT) and Continuous Endurance Training for VO2max Improvements: A Systematic Review and Meta-Analysis of Controlled Trials. Sports Med. 2015, 45, 1469–1481. [Google Scholar] [CrossRef]
- Sloth, M.; Sloth, D.; Overgaard, K.; Dalgas, U. Effects of Sprint Interval Training on VO2max and Aerobic Exercise Performance: A Systematic Review and Meta-Analysis. Scand J. Med. Sci. Sports 2013, 23, e341–e352. [Google Scholar] [CrossRef]
- Buchheit, M.; Laursen, P.B. High-Intensity Interval Training, Solutions to the Programming Puzzle: Part I: Cardiopulmonary Emphasis. Sports Med. 2013, 43, 313–338. [Google Scholar] [CrossRef] [PubMed]
- Buchheit, M.; Laursen, P. Science and application of high-intensity interval training: Solutions to the programming puzzle. In Physiological Targets of HIIT; Laursen, P., Buchheit, M., Eds.; Human Kinetics: Champaign, IL, USA, 2018; pp. 33–50. [Google Scholar]
- Kellmann, M.; Bertollo, M.; Bosquet, L.; Brink, M.; Coutts, A.J.; Duffield, R.; Erlacher, D.; Halson, S.L.; Hecksteden, A.; Heidari, J.; et al. Recovery and Performance in Sport: Consensus Statement. Int. J. Sports Physiol. Perform. 2018, 13, 240–245. [Google Scholar] [CrossRef]
- Mujika, I. Quantification of Training and Competition Loads in Endurance Sports: Methods and Applications. Int. J. Sports Physiol. Perform. 2017, 12, S2–S9. [Google Scholar] [CrossRef] [PubMed]
- Hebestreit, H.; Mimura, K.; Bar-Or, O. Recovery of muscle power after high-intensity short-term exercise: Comparing boys and men. J. Appl. Physiol. 1993, 74, 2875–2880. [Google Scholar] [CrossRef] [PubMed]
- Laursen, P.; Buchheit, M.; Vollmer, J.C. Science and application of high-intensity interval training: Solutions to the programming puzzle. In Genesis and Evolution of High-Intensity Interval Training; Laursen, P., Buchheit, M., Eds.; Human Kinetics: Champaign, IL, USA, 2018; pp. 3–15. [Google Scholar]
- Hausswirth, C.; Le Meur, Y. Physiological and nutritional aspects of post-exercise recovery: Specific recommendations for female athletes. Sports Med. 2011, 41, 861–882. [Google Scholar] [CrossRef]
- Perez-Gomez, J.; Rodriguez, G.V.; Ara, I.; Olmedillas, H.; Chavarren, J.; González-Henriquez, J.J.; Dorado, C.; Calbet, J.A.L. Role of Muscle Mass on Sprint Performance: Gender Differences? Eur. J. Sport Sci. 2007, 102, 685–694. [Google Scholar] [CrossRef]
- Billaut, F.; Bishop, D. Muscle fatigue in males and females during multiple-sprint exercise. Sports Med. 2009, 39, 257–278. [Google Scholar] [CrossRef]
- Hunter, S.K. Sex Differences in Human Fatigability: Mechanisms and Insight to Physiological Responses. Acta Physiol. 2014, 210, 768–789. [Google Scholar] [CrossRef] [PubMed]
- Albert, W.J.; Wrigley, A.T.; McLean, R.B.; Sleivert, G.G. Sex differences in the rate of fatigue development and recovery. Dyn. Med. 2006, 5, 2. [Google Scholar] [CrossRef] [PubMed]
- Wüst, R.C.I.; Morse, C.I.; De Haan, A.; Jones, D.A.; Degens, H. Sex Differences in Contractile Properties and Fatigue Resistance of Human Skeletal Muscle. Exp. Physiol. 2008, 93, 843–850. [Google Scholar] [CrossRef] [PubMed]
- Esbjornsson-Liljedahl, M.; Bodin, K.; Jansson, E. Smaller muscle ATP reduction in women than in men by repeated bouts of sprint exercise. J. Appl. Physiol. 2002, 93, 1075–1083. [Google Scholar] [CrossRef]
- Bar-Or, O. The Wingate Anaerobic Test: An Update on Methodology, Reliability and Validity. Sports Med. 1987, 4, 381–394. [Google Scholar] [CrossRef]
- Inbar, O.; Bar-Or, O.; Skinner, J.S. The Development of the Wingate Anaerobic Test. In The Wingate Anaerobic Test; Human Kinetics: Champaign, IL, USA, 1996; pp. 1–7. [Google Scholar]
- Graves, R.S.; Mahnken, J.D.; Perea, R.D.; Billinger, S.A.; Vidoni, E.D. Modeling Percentile Rank of Cardiorespiratory Fitness Across the Lifespan. Cardiopulm. Phys. Ther. J. 2015, 26, 108–113. [Google Scholar] [CrossRef]
- Borg, G.; Hassmén, P.; Lagerström, M. Perceived exertion related to heart rate and blood lactate during arm and leg exercise. Eur. J. Appl. Physiol. Occup. Physiol. 1987, 56, 679–685. [Google Scholar] [CrossRef]
- Kenttä, G.; Hassmén, P. Overtraining and recovery. A conceptual model. Sports Med. 1998, 26, 1–16. [Google Scholar] [CrossRef]
- Hopkins, W.G. Spreadsheets for analysis of controlled trials, with adjustment for a subject characteristic. Sport Sci. 2006, 10, 46–50. [Google Scholar]
- Laurent, C.M.; Green, J.M.; Bishop, P.A.; Sjökvist, J.; Schumacker, R.E.; Richardson, M.T.; Curtner-Smith, M. Effect of gender on fatigue and recovery following maximal intensity repeated sprint performance. J. Sports Med. Phys. Fit. 2010, 50, 243–253. [Google Scholar]
- Venables, M.C.; Achten, J.; Jeukendrup, A.E. Determinants of Fat Oxidation during Exercise in Healthy Men and Women: A Cross-Sectional Study. J. Appl. Physiol. 2005, 98, 160–167. [Google Scholar] [CrossRef]
- Hamadeh, M.J.; Devries, M.C.; Tarnopolsky, M.A. Estrogen supplementation reduces whole body leucine and carbohydrate oxidation and increases lipid oxidation in men during endurance exercise. J. Clin. Endocrinol. Metab. 2005, 90, 3592–3599. [Google Scholar] [CrossRef]
- Esbjornsson-Liljedahl, M.; Sundberg, C.J.; Norman, B.; Jansson, E. Metabolic response in type I and type II muscle fibers during a 30-s cycle sprint in men and women. J. Appl. Physiol. 1999, 87, 1326–1332. [Google Scholar] [CrossRef]
- Gratas-Delamarche, A.; Le Cam, R.; Delamarche, P.; Monnier, M.; Koubi, H. Lactate and catecholamine responses in male and female sprinters during a Wingate test. Eur. J. Appl. Physiol. Occup. Physiol. 1994, 68, 362–366. [Google Scholar] [CrossRef]
- Jaworowski, A.; Porter, M.M.; Holmback, A.M.; Downham, D.; Lexell, J. Enzyme Activities in the Tibialis Anterior Muscle of Young Moderately Active Men and Women: Relationship with Body Composition, Muscle Cross-Sectional Area and Fibre Type Composition. Acta Physiol. Scand. 2002, 176, 215–225. [Google Scholar] [CrossRef]
- Vincent, S.; Berthon, P.; Zouhal, H.; Moussa, E.; Catheline, M.; Bentu-Ferrer, D.; Gratas-Delamarche, A.; Vincent, S.; Berthon, P. Plasma Glucose, Insulin and Catecholamine Responses to a Wingate Test in Physically Active Women and Men. Eur. J. Sport Sci. 2004, 91, 15–21. [Google Scholar] [CrossRef]
- Lievens, E.; Klass, M.; Bex, T.; Derave, W. Muscle Fiber Typology Substantially Influences Time to Recover from High-Intensity Exercise. J. Appl. Physiol. 2020, 128, 648–659. [Google Scholar] [CrossRef] [PubMed]
- Haizlip, K.M.; Harrison, B.C.; Leinwand, L.A. Sex-Based Differences in Skeletal Muscle Kinetics and Fiber-Type Composition. Physiology 2015, 30, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Dar, D.E.; Zinder, O. Short-term effect of steroids on catecholamines secretion from bovine adrenal medulla chromaffin cells. Neuropharmacology 1997, 36, 1783–1788. [Google Scholar] [CrossRef]
- Arena, R.; Arrowood, J.A.; Fei, D.; Shelar, S.; Helm, S.; Kraft, K.A. The influence of sex on the relationship between heart rate recovery and other cardiovascular risk factors in apparently healthy subjects. Scand. J. Med. Sci. Sports 2010, 20, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Kappus, R.M.; Ranadive, S.M.; Yan, H.; Lane-Cordova, A.D.; Cook, M.D.; Sun, P.; Fernhall, B. Sex differences in autonomic function following maximal exercise. Biol. Sex Differ. 2015, 6, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Mendonca, G.V.; Heffernan, K.S.; Rossow, L.; Guerra, M.; Pereira, F.D.; Fernhall, B. Sex differences in linear and nonlinear heart rate variability during early recovery from supramaximal exercise. Appl. Physiol. Nutr. Metab. 2010, 35, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Gibala, M.J.; Gillen, J.B.; Percival, M.E. Physiological and health-related adaptations to low-volume interval training: Influences of nutrition and sex. Sports Med. 2014, 44, 127–137. [Google Scholar] [CrossRef]
- Schmitz, B.; Niehues, H.; Thorwesten, L.; Klose, A.; Krüger, M.; Brand, S.M. Sex Differences in High-Intensity Interval Training–Are HIIT Protocols Interchangeable Between Females and Males? Front. Physiol. 2020, 11, 38. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Women (n = 11) | Men (n = 11) | p-Values |
|---|---|---|---|
| Age (years) | 31.7 ± 10.0 | 33.5 ± 10.2 | 0.69 |
| Height (m) | 1.66 ± 0.06 | 1.80 ± 0.05 | <0.001 |
| Body mass (kg) | 57.2 ± 6.3 | 75.2 ± 4.3 | <0.001 |
| BMI (kg/m2) | 21.2 ± 2.3 | 23.5 ± 2.2 | 0.03 |
| Body fat (%) | 15.6 ± 6.8 | 10.9 ± 6.6 | <0.001 |
| FFM (kg) | 45.9 ± 10.0 | 67.9 ± 4.0 | <0.001 |
| VO2max (mL/min/kg) | 47.7 ± 5.8 | 56.0 ± 5.9 | <0.001 |
| HRmax (min−1) | 180.6 ± 11.5 | 178.9 ± 12.6 | 0.75 |
| Peak Power (W/kg) | 4.69 ± 0.43 | 5.07 ± 0.50 | 0.07 |
| Peak Power (W/kgFFM) | 5.57 ± 0.56 | 5.63 ± 0.61 | 0.63 |
| VO2max-percentile (%) | 91.8 ± 5.5 | 94.6 ± 5.4 | 0.23 |
| Training (h/week) | 9.6 ± 3.3 | 8.2 ± 1.9 | 0.87 |
| Parameter | Recovery | Sex | WAnT 1 | WAnT 2 | WAnT 3 | WAnT 4 | T1–T4 |
|---|---|---|---|---|---|---|---|
| Peak Power (W) | 1 min | w m | 532.6 ± 110.9 843.8 ± 174.2 | 439.2 ± 67.4 *** 673.4 ± 78.7 ** | 454.8 ± 72.2 625.8 ± 90.7 * | 426.8 ± 67.7 573.7 ± 78.7 *** | p = 0.006 p < 0.001 |
| Av. Power (W) | w m | 345.6 ± 54.9 608.0 ± 93.5 | 302.3 ± 46.2 *** 517.7 ± 69.3 ** | 292.9 ± 51.7 * 482.5 ± 63.7 *** | 287.4 ± 49.5 454.0 ± 66.6 *** | p < 0.001 p < 0.001 | |
| Fatigue (%) | w m | 33.6 ± 11.7 27.6 ± 8.0 | 30.6 ± 10.1 22.9 ± 7.7 * | 35.4 ± 7.3 * 22.6 ± 6.1 | 32.4 ± 8.2 * 20.2 ± 5.9 * | p = 0.67 p = 0.002 | |
| Peak Power (W) | 3 min | w m | 580.0 ± 98.2 840.5 ± 149.5 | 555.3 ± 102.7 * 762.8 ± 88.1 * | 514.9 ± 97.2 700.7 ± 86.5 *** | 505.8 ± 96.1 680.8 ± 83.9 | p = 0.026 p = 0.002 |
| Av. Power (W) | w m | 347.9 ± 63.5 622.7 ± 79.7 | 333.3 ± 53.8 ** 572.4 ± 73.4 *** | 319.1 ± 93.5 ** 541.8 ± 70.8 ** | 313.5 ± 47.2 532.2 ± 71.4 * | p = 0.64 p = 0.02 | |
| Fatigue (%) | w m | 39.4 ± 9.3 24.9 ± 9.2 | 38.9 ± 10.6 24.8 ± 7.3 | 37.3 ± 8.4 22.6 ± 5.8 | 37.0 ± 9.6 21.8 ± 5.2 | p = 0.29 p = 0.14 | |
| Peak Power (W) | 10 min | w m | 565.4 ± 99.8 850.6 ± 137.7 | 522.5 ± 88.2 * 824.5 ± 147.7 | 517.6 ± 98.2 783.9 ± 124.7 | 536.9 ± 103.3 781.9 ± 98.0 | p = 0.06 p = 0.09 |
| Av. Power (W) | w m | 341.3 ± 59.6 622.1 ± 80.1 | 340.2 ± 56.5 617.1 ± 81.5 | 342.9 ± 56.4 603.7 ± 76.9 * | 340.1 ± 56.5 605.6 ± 75.1 | p = 0.80 p = 0.25 | |
| Fatigue (%) | w m | 39.0 ± 9.0 26.1 ± 7.9 | 34.2 ± 9.1 *** 24.2 ± 9.2 | 33.0 ± 8.7 22.5 ± 5.1 | 35.8 ± 8.2 22.3 ± 5.9 | p = 0.06 p = 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hottenrott, L.; Möhle, M.; Ide, A.; Ketelhut, S.; Stoll, O.; Hottenrott, K. Recovery from Different High-Intensity Interval Training Protocols: Comparing Well-Trained Women and Men. Sports 2021, 9, 34. https://doi.org/10.3390/sports9030034
Hottenrott L, Möhle M, Ide A, Ketelhut S, Stoll O, Hottenrott K. Recovery from Different High-Intensity Interval Training Protocols: Comparing Well-Trained Women and Men. Sports. 2021; 9(3):34. https://doi.org/10.3390/sports9030034
Chicago/Turabian StyleHottenrott, Laura, Martin Möhle, Alexander Ide, Sascha Ketelhut, Oliver Stoll, and Kuno Hottenrott. 2021. "Recovery from Different High-Intensity Interval Training Protocols: Comparing Well-Trained Women and Men" Sports 9, no. 3: 34. https://doi.org/10.3390/sports9030034
APA StyleHottenrott, L., Möhle, M., Ide, A., Ketelhut, S., Stoll, O., & Hottenrott, K. (2021). Recovery from Different High-Intensity Interval Training Protocols: Comparing Well-Trained Women and Men. Sports, 9(3), 34. https://doi.org/10.3390/sports9030034