The Effect of Traditional and Stabilization-Oriented Exercises on Deep Stabilization System Function in Elite Futsal Players



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
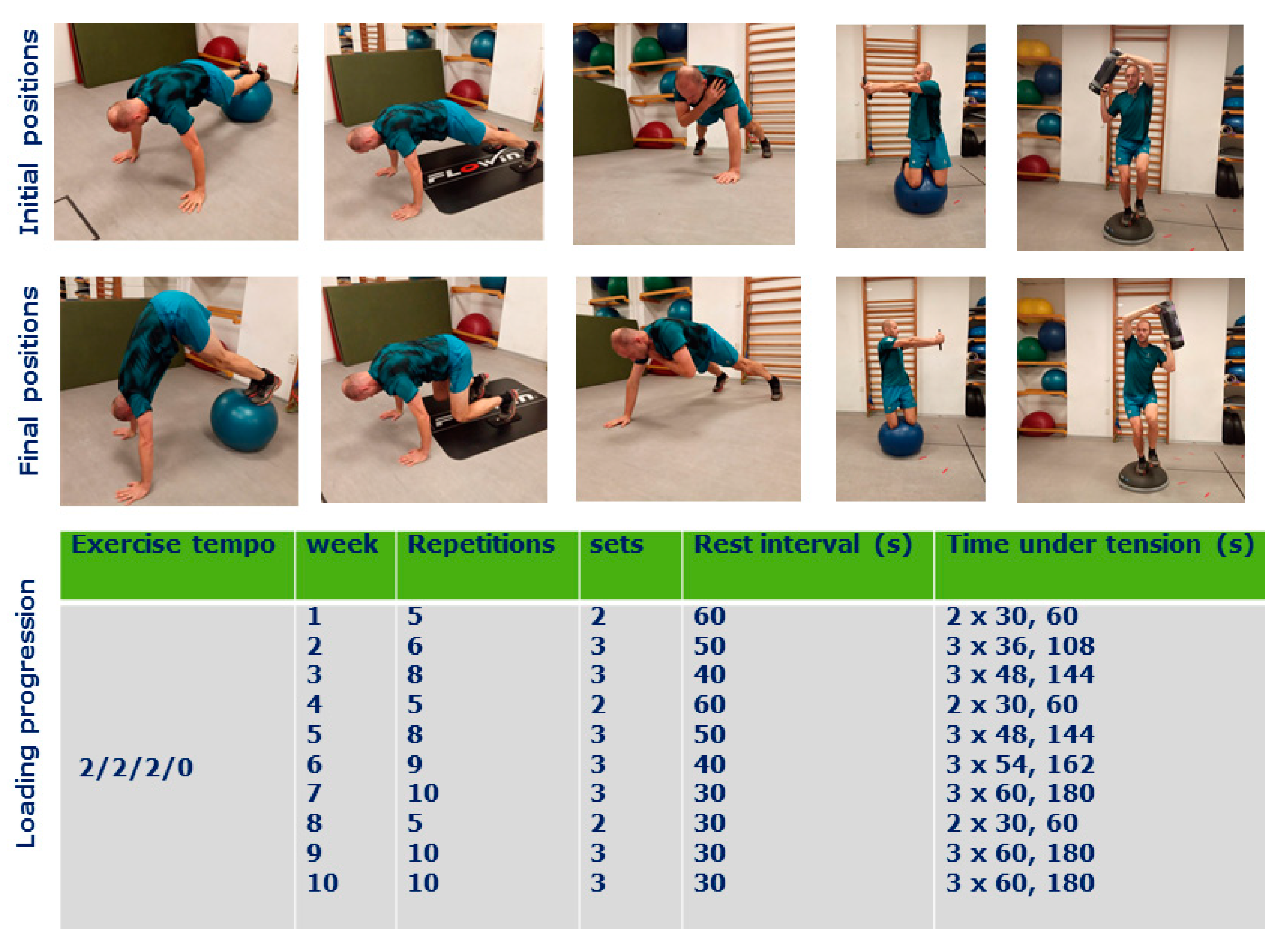
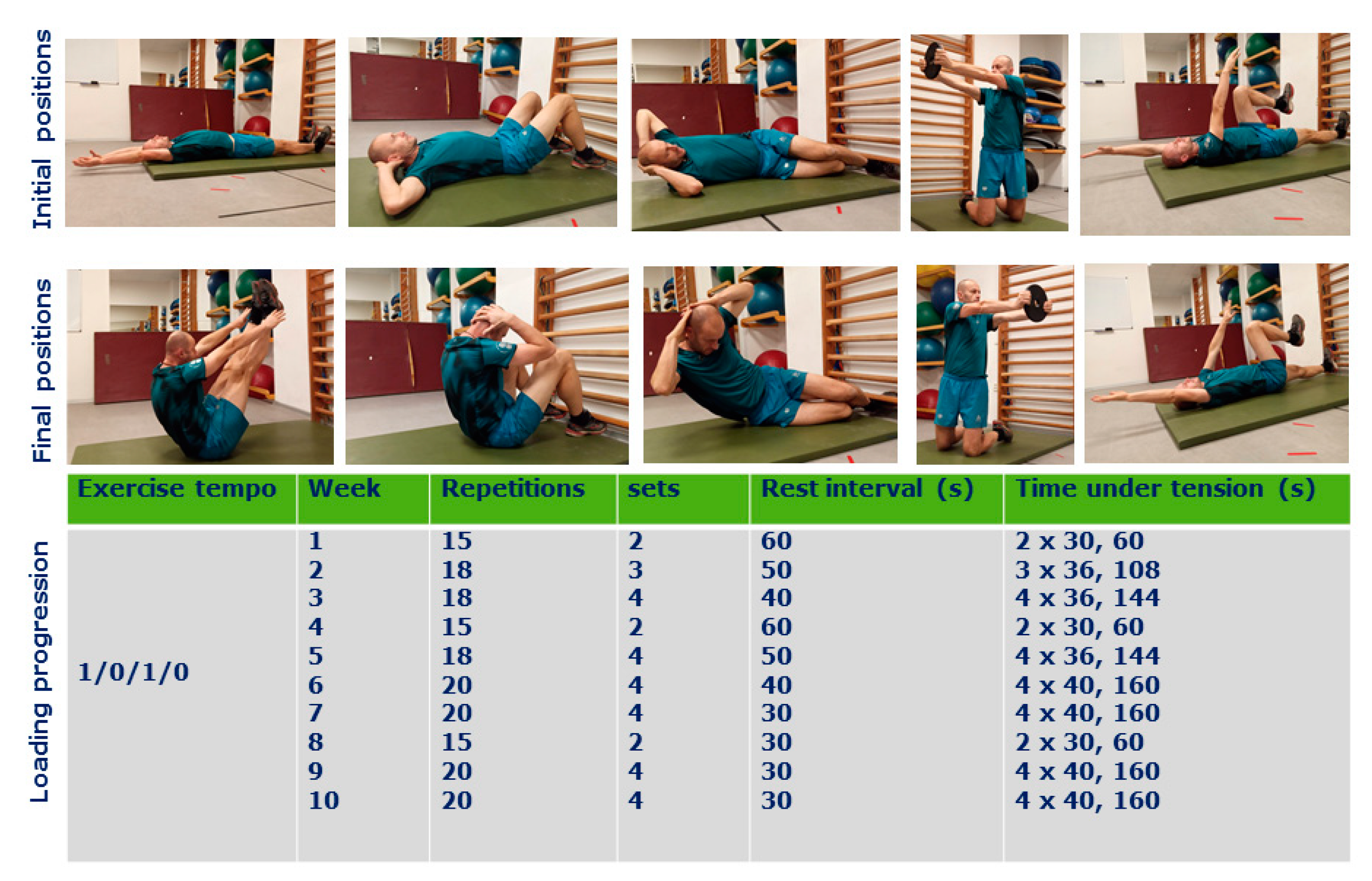
2.2. Design and Procedure
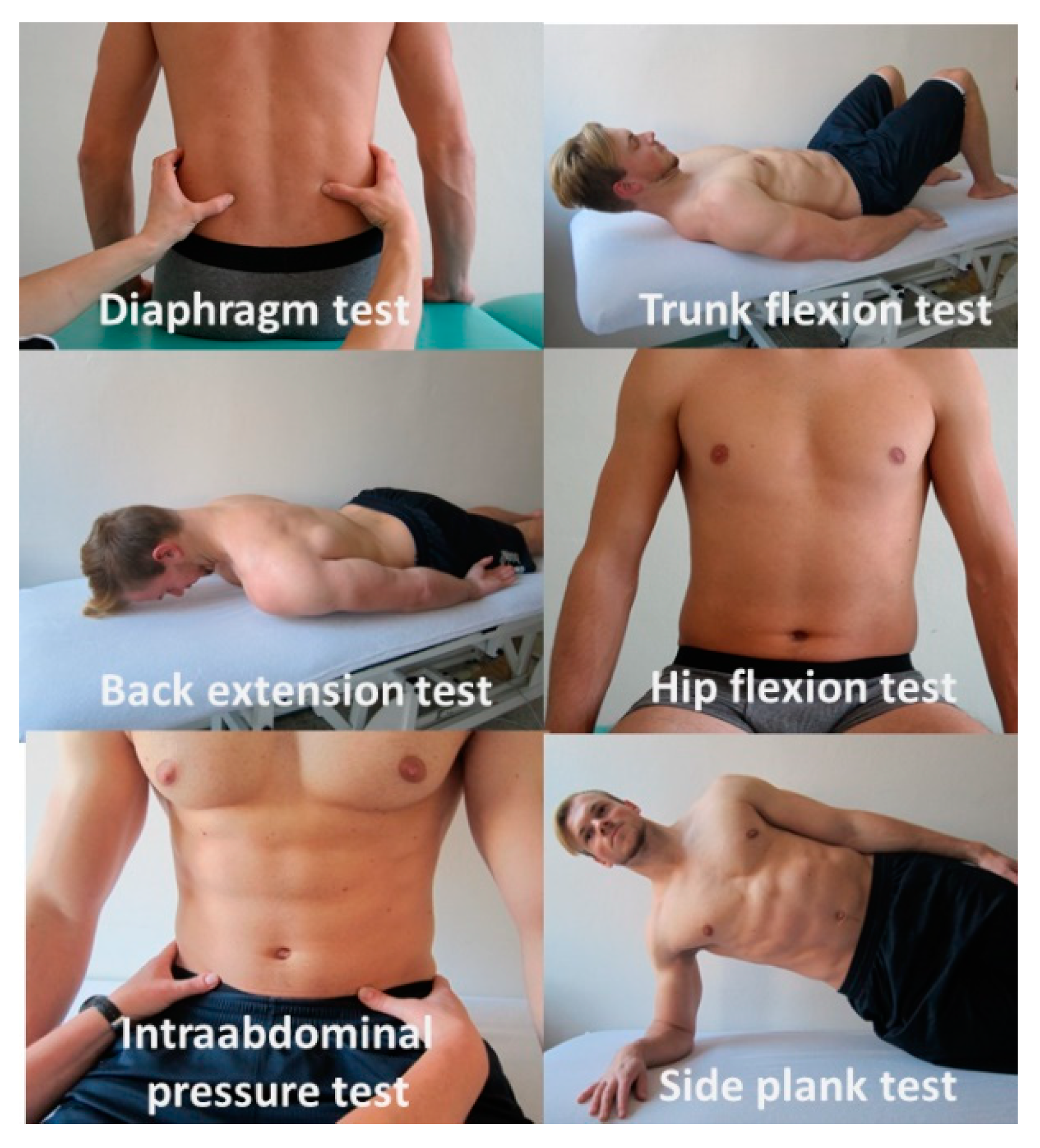
2.3. Measures of the Deep Stabilization System (DSS)
2.4. Diaphragm Test
2.5. Trunk Flexion Test
2.6. Back Extension Test
2.7. Hip Flexion Test
2.8. Intraabdominal Pressure Test (IAP Test)
2.9. Side Plank Test
2.10. Statistical Analysis
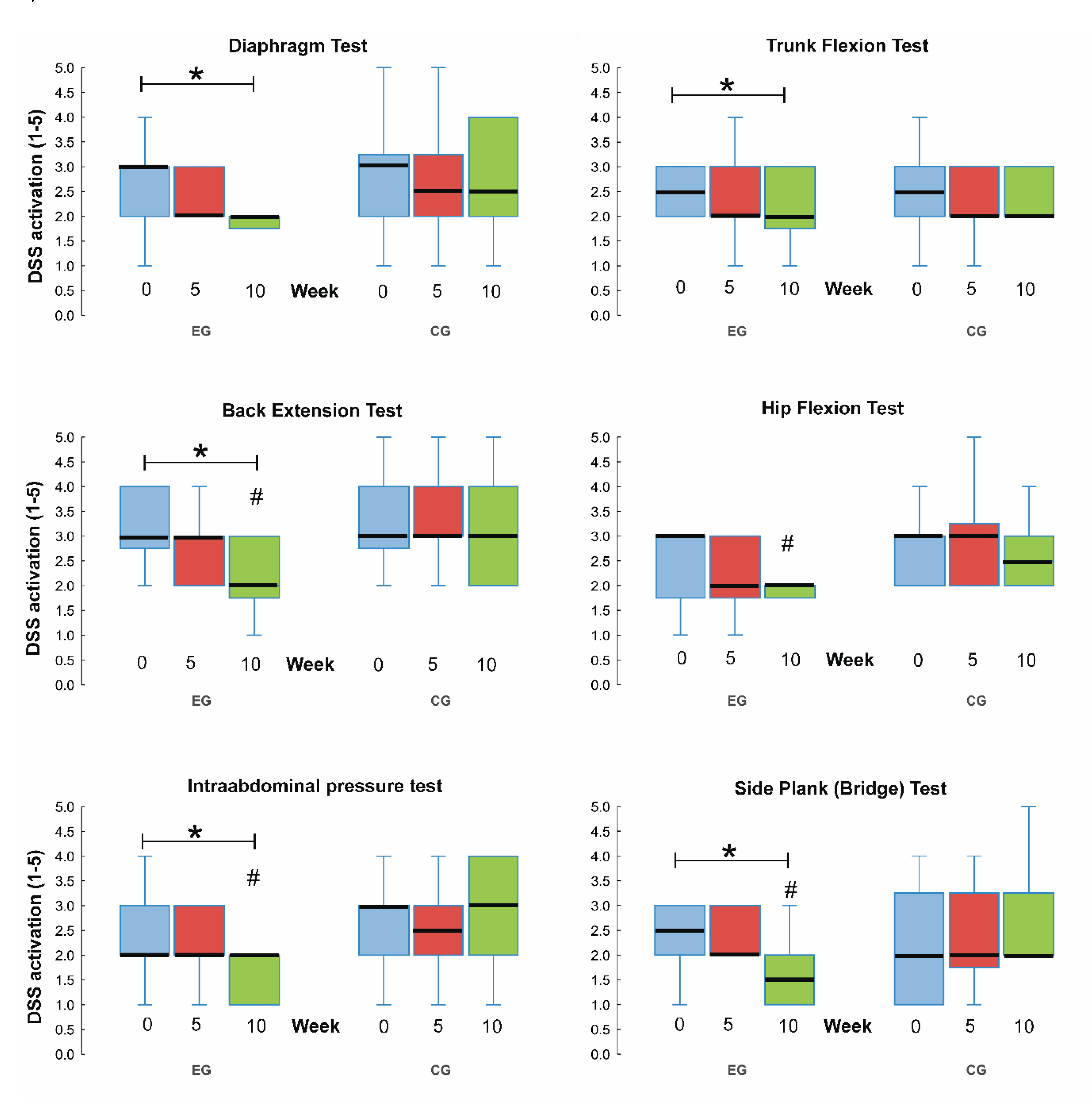
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Junge, A.; Dvorak, J. Injury risk of playing football in Futsal World Cups. Br. J. Sports Med. 2010, 44, 1089–1092. [Google Scholar] [CrossRef] [PubMed]
- Varkiani, M.E.; Alizadeh, M.H.; Pourkazemi, L. The epidemiology of futsal injuries via sport medicine federation injury surveillance system of Iran in 2010. Procedia-Soc. Behav. Sci. 2013, 82, 946–951. [Google Scholar] [CrossRef][Green Version]
- Naser, N.; Ali, A.; Macadam, P. Physical and physiological demands of futsal. J. Exerc. Sci. Fit. 2017, 15, 76–80. [Google Scholar] [CrossRef] [PubMed]
- De Freitas, V.H.; Ramos, S.d.P.; Leicht, A.; Alves, T.; Rabelo, F.; Bara-Filho, M.G.; Guarnier, F.A.; Nakamura, F.Y. Validation of the futsal-specific intermittent shuttle protocol for the simulation of the physical demands of futsal match-play. Int. J. Perform. Anal. Sport 2017, 17, 934–947. [Google Scholar] [CrossRef]
- Ayarra, R.; Nakamura, F.Y.; Iturricastillo, A.; Castillo, D.; Yanci, J. Differences in physical performance according to the competitive level in futsal players. J. Hum. Kinet. 2018, 64, 275–285. [Google Scholar] [CrossRef]
- Ribeiro, J.N.; Gonçalves, B.; Coutinho, D.; Brito, J.; Sampaio, J.; Travassos, B. Activity Profile and Physical Performance of match play in elite futsal players. Front. Psychol. 2020, 11, 1709. [Google Scholar] [CrossRef]
- Small, K.; McNaughton, L.; Greig, M.; Lovell, R. The effects of multidirectional soccer-specific fatigue on markers of hamstring injury risk. J. Sci. Med. Sport 2010, 13, 120–125. [Google Scholar] [CrossRef]
- Martuscello, J.M.; Nuzzo, J.L.; Ashley, C.D.; Campbell, B.I.; Orriola, J.J.; Mayer, J.M. Systematic review of core muscle activity during physical fitness exercises. J. Strength Cond. Res. 2013, 27, 1684–1698. [Google Scholar] [CrossRef]
- Bryan, M.; Hawson, S. The benefits of Pilates exercise in orthopaedic rehabilitation. Tech. Orthop. 2003, 18, 126–129. [Google Scholar] [CrossRef]
- Jebavý, R.; Hojka, V.; Kaplan, A. Kondiční Trénink ve Sportovních Hrách: Na Příkladu Fotbalu, Ledního Hokeje a Basketbalu; Grada Publishing a.s.: Praha 7-Holešovice, Czech Republic, 2017. [Google Scholar]
- Frank, C.; Kobesova, A.; Kolar, P. Dynamic neuromuscular stabilization & sports rehabilitation. Int. J. Sports Phys. 2013, 8, 62–73. [Google Scholar]
- Kolář, P. Rehabilitace v Klinické Praxi; 1. Vydání; Galén: Praha, Czech Republic, 2009; ISBN 978-80-7262-657-1. [Google Scholar]
- Suchomel, R.f.M.T. Stabilita v pohybovém systému a hluboký stabilizační systém. Rehabil. Fy. 2006, 13, 112–124. [Google Scholar]
- Daggfeldt, K.; Thorstensson, A. The role of intra-abdominal pressure in spinal unloading. J. Biomech. 1997, 30, 1149–1155. [Google Scholar] [CrossRef]
- Blazek, D.; Stastny, P.; Maszczyk, A.; Krawczyk, M.; Matykiewicz, P.; Petr, M. Systematic review of intra-abdominal and intrathoracic pressures initiated by the Valsalva manoeuvre during high-intensity resistance exercises. Biol. Sport 2019, 36, 373. [Google Scholar] [CrossRef] [PubMed]
- Hodges, P.W. Core stability exercise in chronic low back pain. Orthop. Clin. 2003, 34, 245–254. [Google Scholar] [CrossRef]
- Pysna, J.; Pysny, L.; Petru, D.; Endal, V. Evaluating activity of deep stabilising system of the spine in young elite ice-hockey players. South. Afr. J. Res. SportPhys. Educ. Recreat. 2018, 40, 73–88. [Google Scholar]
- Jalovcova, M.; Pavlů, D. Stabilizační systém a role m. transversus abdominis. Rehabil. Fyzikální Lékařství 2010, 17, 174–180. [Google Scholar]
- Long, A.; Donelson, R.; Fung, T. Does it matter which exercise? A randomized control trial of exercise for low back pain. Spine 2004, 29, 2593–2602. [Google Scholar] [CrossRef]
- Aspe, R.R.; Swinton, P.A. Electromyographic and kinetic comparison of the back squat and overhead squat. J. Strength Cond. Res. 2014, 28, 2827–2836. [Google Scholar] [CrossRef]
- Cordo, P.J.; Gurfinkel, V.S.; Smith, T.C.; Hodges, P.W.; Verschueren, S.; Brumagne, S. The sit-up: Complex kinematics and muscle activity in voluntary axial movement. J. Electromyogr. Kinesiol. 2003, 13, 239–252. [Google Scholar] [CrossRef]
- Jahoda, R.; Mitterbauer, G. ComplexCoreTM-Core Stabilisation in Training and Therapy; Jahoda Sports Publisher: Salzburg, Austria, 2013. [Google Scholar]
- Mahdieh, L.; Zolaktaf, V.; Karimi, M.T. Effects of dynamic neuromuscular stabilization (DNS) training on functional movements. Hum. Mov. Sci. 2020, 70, 102568. [Google Scholar] [CrossRef]
- Lago-Fuentes, C.; Rey, E.; Padrón-Cabo, A.; de Rellán-Guerra, A.S.; Fragueiro-Rodríguez, A.; García-Núñez, J. Effects of core strength training using stable and unstable surfaces on physical fitness and functional performance in professional female futsal players. J. Hum. Kinet. 2018, 65, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Pešán, F.; Jelínek, M.; Fiala, M.; Matošková, P.; Süss, V. Vliv kompenzačního programu na posturální svaly u extraligových hráčů ledního hokeje. Rehabilitácia 2015, 52, 3–10. [Google Scholar]
- Ondra, L.; Nátěsta, P.; Bizovská, L.; Kuboňová, E.; Svoboda, Z. Effect of in-season neuromuscular and proprioceptive training on postural stability in male youth basketball players. Acta Gymnica 2017, 47, 144–149. [Google Scholar] [CrossRef]
- Busara, J.; Chentanez, T.; Pintong, M.; Widjaja, W. The effects of the 11+ training programme on stability performance in adolescent futsal players. J. Sports Sci. Technol. 2015, 15, 57–65. [Google Scholar]
- Ruiz-Pérez, I.; Ayala, F.; Puerta, J.M.; Elvira, J.L.L.; De Ste Croix, M.; Hernández-Sánchez, S.; Vera-Garcia, F.J. A Bayesian Network approach to study the relationships between several neuromuscular performance measures and dynamic postural control in futsal players. PloS ONE 2019, 14, e0220065. [Google Scholar] [CrossRef] [PubMed]
- Bačová, I.; Cicholesová, T.; Dziaková, M.; Šulla, I.; Kitka, M.; Petrovičová, J. Význam Rehabilitácie Hlbokého Stabilizačného Systému Pri Liečbe Vertebrogénnych Ochorení; Rehabilitácia: Bratislava, Slovakia, 2015; Volume 52, pp. 67–77. [Google Scholar]
- Šorfová, M.; Tlapáková, E.; Matějková, A. Funkce svalů pánevního dna ve vztahu k poloze těla a k typu dýchání. Rehabil. Phys. Med./Rehabil. Fyzikalni Lek. 2018, 25, 171–177. [Google Scholar]
- Siff, M. Supertraining, 6th ed.; Supertraining Institute: Denver, CO, USA, 2003; Volume 290. [Google Scholar]
- Zatsiorsky, V.; Kraemer, W. Science and Practice of Strength Training; Human Kinetics: Champaign, IL, USA, 2006. [Google Scholar]
- Willardson, J.M. Core stability training: Applications to sports conditioning programs. J. Strength Cond. Res. 2007, 21, 979–985. [Google Scholar] [CrossRef]
- Lopes, M.; Lopes, S.; Patinha, T.; Araújo, F.; Rodrigues, M.; Costa, R.; Oliveira, J.; Ribeiro, F. Balance and proprioception responses to FIFA 11+ in amateur futsal players: Short and long-term effects. J. Sports Sci. 2019, 37, 2300–2308. [Google Scholar] [CrossRef]
- Stastny, P.; Lehnert, M.; De Ste Croix, M.; Petr, M.; Svoboda, Z.; Maixnerova, E.; Varekova, R.; Botek, M.; Petrek, M.; Kocourkova, L.; et al. Effect of COL5A1, GDF5, and PPARA Genes on a Movement Screen and Neuromuscular Performance in Adolescent Team Sport Athletes. J. Strength Cond. Res. 2019, 33, 2057–2065. [Google Scholar] [CrossRef]
- Bompa, T.; Buzzichelli, C. Periodization Training for Sports, 3E; Human kinetics: Champaign, IL, USA, 2015. [Google Scholar]
- Cejudo, A.; de Baranda, P.S.; Ayala, F.; Santonja, F. Test-retest reliability of seven common clinical tests for assessing lower extremity muscle flexibility in futsal and handball players. Phys. Sport 2015, 16, 107–113. [Google Scholar] [CrossRef]
- Kobesova, A.; Davidek, P.; Morris, C.E.; Andel, R.; Maxwell, M.; Oplatkova, L.; Safarova, M.; Kumagai, K.; Kolar, P. Functional postural-stabilization tests according to Dynamic Neuromuscular Stabilization approach: Proposal of novel examination protocol. J. Bodyw. Mov. 2020, 24, 84–95. [Google Scholar] [CrossRef] [PubMed]
- Richardson, C.A.; Hodges, P.; Hides, J.A. Therapeutic exercise for lumbopelvic stabilization: A motor control approach for the treatment and prevention of low back pain. Phys. Ther. 2004, 85, 470. [Google Scholar]
- Arokoski, J.P.; Valta, T.; Airaksinen, O.; Kankaanpää, M. Back and abdominal muscle function during stabilization exercises. Arch. Phys. Med. Rehabil. 2001, 82, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Dallas, G.; Mavvidis, A.; Kirialanis, P.; Papouliakos, S. The effect of 8 weeks of whole body vibration training on static balance and explosive strength of lower limbs in physical education students. Acta Gymnica 2017, 47, 153–160. [Google Scholar] [CrossRef]
- Stephenson, J.; Swank, A.M. Core training: Designing a program for anyone. Strength Cond. J. 2004, 26, 34. [Google Scholar] [CrossRef]
- Willardson, J.M. Core stability training for healthy athletes: A different paradigm for fitness professionals. Strength Cond. J. 2007, 29, 42. [Google Scholar] [CrossRef]
- Gritsanadilok, W.; Chentanez, T.; Hirunrat, S.; Sinphurmuksakul, O. The effect of “The FIFA 11+” Warm-up training on balance and proprioception in adolescent futsall players. J. Sports Sci. Technol. 2013, 13, 19–29. [Google Scholar]
- Wahl, M.J.; Behm, D.G. Not all instability training devices enhance muscle activation in highly resistance-trained individuals. J. Strength Cond. Res. 2008, 22, 1360–1370. [Google Scholar] [CrossRef]
- Jebavy, R.; Balas, J.; Jalovcova, M. Komparace silových cvičení na nestabilních a stabilních plochách jako prostředek pro zlepšení činností hlubokého stabilizačního systému. Rehabilitácia 2016, 53, 85–92. [Google Scholar]
- Jebavý, R.; Perič, T.; Baláš, J.; Šťastný, P. Stimulation a strength endurance through exercises on the unstable surfaces. Studia KinanthropologicaUniv. Bohem. Merid. Budvicensis 2013, 14, 93–99. [Google Scholar]
- Yaggie, J.A.; Campbell, B.M. Effects of balance training on selected skills. J. Strength Cond. Res. 2006, 20, 422–428. [Google Scholar] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jebavy, R.; Baláš, J.; Vomackova, H.; Szarzec, J.; Stastny, P. The Effect of Traditional and Stabilization-Oriented Exercises on Deep Stabilization System Function in Elite Futsal Players. Sports 2020, 8, 153. https://doi.org/10.3390/sports8120153
Jebavy R, Baláš J, Vomackova H, Szarzec J, Stastny P. The Effect of Traditional and Stabilization-Oriented Exercises on Deep Stabilization System Function in Elite Futsal Players. Sports. 2020; 8(12):153. https://doi.org/10.3390/sports8120153
Chicago/Turabian StyleJebavy, Radim, Jiří Baláš, Helena Vomackova, Jakub Szarzec, and Petr Stastny. 2020. "The Effect of Traditional and Stabilization-Oriented Exercises on Deep Stabilization System Function in Elite Futsal Players" Sports 8, no. 12: 153. https://doi.org/10.3390/sports8120153
APA StyleJebavy, R., Baláš, J., Vomackova, H., Szarzec, J., & Stastny, P. (2020). The Effect of Traditional and Stabilization-Oriented Exercises on Deep Stabilization System Function in Elite Futsal Players. Sports, 8(12), 153. https://doi.org/10.3390/sports8120153