Effect of Sports and Growth on Hamstrings and Quadriceps Development in Young Female Athletes: Cross-Sectional Study

Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Participants
2.3. Instrumentations
2.4. Procedures
2.5. Data Reduction
2.6. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- US Figure Skating Fact Sheet. 2018 Fiscal Year Information. Available online: http://www.usfsa.org. (accessed on 28 July 2018).
- Nikolic, A.; Baltzer, A.W.; Kramer, R.; Liebau, C. Injuries specific to ice skating-documentation of the injuries of competitive athletes during a pre-season training camp. Sportverletz Sportschaden. 1998, 12, 142–146. [Google Scholar] [PubMed]
- Bloch, R.M. Figure skating injuries. Phys. Med. Rehabil. Clin. N Am. 1999, 10, 177–188. [Google Scholar] [CrossRef]
- Smith, A.D. The young skater. Clin. Sports Med. 2000, 19, 741–755. [Google Scholar] [CrossRef]
- Porter, E.B.; Young, C.C.; Niedfeldt, M.W.; Gottschlich, L.M. Sport-specific injuries and medical problems of figure skaters. WMJ 2007, 106, 330–334. [Google Scholar] [PubMed]
- Porter, E.B. Common injuries and medical problems in singles figure skaters. Curr. Sports Med. Rep. 2013, 12, 318–320. [Google Scholar] [CrossRef] [PubMed]
- Dubravcic-Simunjak, S.; Pecina, M.; Kuipers, H.; Moran, J.; Haspl, M. The incidence of injuries in elite junior figure skaters. Am. J. Sports Med. 2003, 31, 511–517. [Google Scholar] [CrossRef] [PubMed]
- Dubravcic-Simunjak, S.; Kuipers, H.; Moran, J.; Simunjak, B.; Pecina, M. Injuries in synchronized skating. Int. J. Sports Med. 2006, 27, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Kowalczyk, A.D.; Geminiani, E.T.; Dahlberg, B.W.; Micheli, L.J.; Sugimoto, D. Pediatric and Adolescent Figure Skating Injuries: A 15-Year Retrospective Review. Clin. J. Sport Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Hootman, J.M.; Dick, R.; Agel, J. Epidemiology of collegiate injuries for 15 sports: Summary and recommendations for injury prevention initiatives. J. Athl. Train. 2007, 42, 311–319. [Google Scholar]
- Beynnon, B.D.; Vacek, P.M.; Newell, M.K.; Tourville, T.W.; Smith, H.C.; Shultz, S.J.; Johnson, R.J. The Effects of Level of Competition, Sport, and Sex on the Incidence of First-Time Noncontact Anterior Cruciate Ligament Injury. Am. J. Sports Med. 2014, 42, 1806–1812. [Google Scholar] [CrossRef] [PubMed]
- Agel, J.; Rockwood, T.; Klossner, D. Collegiate ACL Injury Rates Across 15 Sports: National Collegiate Athletic Association Injury Surveillance System Data Update (2004–2005 Through 2012–2013). Clin. J. Sport Med. 2016, 26, 518–523. [Google Scholar] [CrossRef] [PubMed]
- Hewett, T.E.; Ford, K.R.; Myer, G.D. Anterior cruciate ligament injuries in female athletes: Part 2, a meta-analysis of neuromuscular interventions aimed at injury prevention. Am. J. Sports Med. 2006, 34, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Hewett, T.E.; Myer, G.D.; Ford, K.R. Anterior cruciate ligament injuries in female athletes: Part 1, mechanisms and risk factors. Am. J. Sports Med. 2006, 34, 299–311. [Google Scholar] [CrossRef] [PubMed]
- Hewett, T.E.; Zazulak, B.T.; Myer, G.D. Effects of the menstrual cycle on anterior cruciate ligament injury risk: a systematic review. Am. J. Sports Med. 2007, 35, 659–668. [Google Scholar] [CrossRef] [PubMed]
- Alentorn-Geli, E.; Mendiguchia, J.; Samuelsson, K.; Musahl, V.; Karlsson, J.; Cugat, R.; Myer, G.D. Prevention of anterior cruciate ligament injuries in sports. Part I: Systematic review of risk factors in male athletes. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 3–15. [Google Scholar] [CrossRef]
- Hewett, T.E.; Myer, G.D.; Ford, K.R.; Heidt Jr, R.S.; Colosimo, A.J.; McLean, S.G.; Succop, P. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: A prospective study. Am. J. Sports Med. 2005, 33, 492–501. [Google Scholar] [CrossRef]
- Leppänen, M.; Pasanen, K.; Kujala, U.M.; Vasankari, T.; Kannus, P.; Äyrämö, S.; Parkkari, J. Stiff landings are associated with increased ACL injury risk in young female basketball and floorball players. Am. J. Sports Med. 2017, 45, 386–393. [Google Scholar] [CrossRef]
- Yu, B.; Garrett, W.E. Mechanisms of non-contact ACL injuries. Br. J. Sports Med. 2007, 1, 47–51. [Google Scholar] [CrossRef]
- Myer, G.D.; Ford, K.R.; Barber Foss, K.D.; Liu, C.; Nick, T.G.; Hewett, T.E. The relationship of hamstrings and quadriceps strength to anterior cruciate ligament injury in female athletes. Clin. J. Sport Med. 2009, 19, 3–8. [Google Scholar] [CrossRef]
- Ortiz, A.; Olson, S.L.; Etnyre, B.; Trudelle-Jackson, E.E.; Bartlett, W.; Venegas-Rios, H.L. Fatigue effects on knee joint stability during two jump tasks in women. J. Strength. Cond. Res. 2010, 24, 1019–1027. [Google Scholar] [CrossRef]
- Elias, A.R.; Hammill, C.D.; Mizner, R.L. Changes in quadriceps and hamstring cocontraction following landing instruction in patients with anterior cruciate ligament reconstruction. J. Orthop. Sports Phys. Ther. 2015, 45, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Letafatkar, A.; Rajabi, R.; Tekamejani, E.E.; Minoonejad, H. Effects of perturbation training on knee flexion angle and quadriceps to hamstring cocontraction of female athletes with quadriceps dominance deficit: Pre-post intervention study. Knee 2015, 22, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Chappell, J.D.; Creighton, R.A.; Giuliani, C.; Yu, B.; Garrett, W.E. Kinematics and electromyography of landing preparation in vertical stop-jump: Risks for noncontact anterior cruciate ligament injury. Am. J. Sports Med. 2007, 35, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, D.; Mattacola, C.G.; Mullineaux, D.R.; Palmer, T.G.; Hewett, T.E. Comparison of isokinetic hip abduction and adduction peak torques and ratio between sexes. Clin. J. Sport Med. 2014, 24, 422–428. [Google Scholar] [CrossRef] [PubMed]
- El-Ashker, S.; Allardyce, J.M.; Carson, B.P. Sex-related differences in joint-angle-specific hamstring-to-quadriceps function following fatigue. Eur. J. Sport Sci. 2019. [Google Scholar] [CrossRef]
- Jayanthi, N.; Pinkham, C.; Dugas, L.; Patrick, B.; Labella, C. Sports specialization in young athletes: Evidence-based recommendations. Sports Health. 2013, 5, 251–257. [Google Scholar] [CrossRef]
- DiFiori, J.P.; Benjamin, H.J.; Brenner, J.S.; Gregory, A.; Jayanthi, N.; Landry, G.L.; Luke, A. Overuse injuries and burnout in youth sports: A position statement from the American Medical Society for Sports Medicine. Br. J. Sports Med. 2014, 48, 287–288. [Google Scholar] [CrossRef]
- Feeley, B.T.; Agel, J.; LaPrade, R.F. When is it Too Early for Single Sport Specialization? Am. J. Sports Med. 2016, 44, 234–241. [Google Scholar] [CrossRef]
- Jayanthi, N.; LaBella, C.R.; Fischer, D.; Pasulka, J.; Dugas, L.R. Sports-specialized intensive training and the risk of injury in young athletes: A clinical case-control study. Am. J. Sports Med. 2015, 43, 794–801. [Google Scholar] [CrossRef]
- Hall, R.; Barber Foss, K.; Hewett, T.E.; Myer, G.D. Sport specialization’s association with an increased risk of developing anterior knee pain in adolescent female athletes. J. Sport Rehabil. 2015, 24, 31–35. [Google Scholar] [CrossRef]
- Myer, G.D.; Ford, K.R.; Divine, J.G.; Wall, E.J.; Kahanov, L.; Hewett, T.E. Longitudinal assessment of noncontact anterior cruciate ligament injury risk factors during maturation in a female athlete: A case report. J. Athl. Train. 2009, 44, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Ford, K.R.; Shapiro, R.; Myer, G.D.; Van Den Bogert, A.J.; Hewett, T.E. Longitudinal sex differences during landing in knee abduction in young athletes. Med. Sci. Sports Exerc. 2010, 42, 1923–1931. [Google Scholar] [CrossRef] [PubMed]
- Quatman-Yates, C.C.; Myer, G.D.; Ford, K.R.; Hewett, T.E. A longitudinal evaluation of maturational effects on lower extremity strength in female adolescent athletes. Pediatr. Phys. Ther. 2013, 25, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Hewett, T.E.; Myer, G.D.; Kiefer, A.W.; Ford, K.R. Longitudinal Increases in Knee Abduction Moments in Females during Adolescent Growth. Med. Sci. Sports Exerc. 2015, 47, 2579–2585. [Google Scholar] [CrossRef] [PubMed]
- Stracciolini, A.; Casciano, R.; Levey Friedman, H.; Meehan, W.P.; Micheli, L.J. Pediatric sports injuries: An age comparison of children versus adolescents. Am. J. Sports Med. 2013, 41, 1922–1929. [Google Scholar] [CrossRef] [PubMed]
- Stracciolini, A.; Stein, C.J.; Zurakowski, D.; Meehan, W.P.; Myer, G.D.; Micheli, L.J. Anterior cruciate ligament injuries in pediatric athletes presenting to sports medicine clinic: A comparison of males and females through growth and development. Sports Health. 2015, 7, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, D.; McCartney, R.E.; Parisien, R.L.; Dashe, J.; Borg, D.R.; Meehan, W.P. Range of motion and ankle injury history association with sex in pediatric and adolescent athletes. Phys. Sports Med. 2018, 46, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Lopezosa-Reca, E.; Gijon-Nogueron, G.; Garcia-Paya, I.; Ortega-Avila, A.B. Does the type of sport practised influence foot posture and knee angle? Differences between footballers and swimmers. Res. Sports Med. 2018, 26, 345–353. [Google Scholar] [CrossRef]
- Vlachopoulos, D.; Barker, A.R.; Williams, C.A.; Arngrímsson, S.A.; Knapp, K.M.; Metcalf, B.S.; Gracia-Marco, L. The Impact of Sport Participation on Bone Mass and Geometry in Male Adolescents. Med. Sci. Sports Exerc. 2017, 49, 317–326. [Google Scholar] [CrossRef]
- Myer, G.D.; Jayanthi, N.; Difiori, J.P.; Faigenbaum, A.D.; Kiefer, A.W.; Logerstedt, D.; Micheli, L.J. Sport Specialization, Part I: Does Early Sports Specialization Increase Negative Outcomes and Reduce the Opportunity for Success in Young Athletes? Sports Health. 2015, 7, 437–442. [Google Scholar] [CrossRef]
- Myer, G.D.; Jayanthi, N.; DiFiori, J.P.; Faigenbaum, A.D.; Kiefer, A.W.; Logerstedt, D.; Micheli, L.J. Sports Specialization, Part II: Alternative Solutions to Early Sport Specialization in Youth Athletes. Sports Health. 2016, 8, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, D.; Jackson, S.S.; Howell, D.R.; Meehan, W.P.; Stracciolini, A. Association between training volume and lower extremity overuse injuries in young female athletes: Implications for early sports specialization. Phys. Sports Med. 2019, 47, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Post, E.G.; Bell, D.R.; Trigsted, S.M.; Pfaller, A.Y.; Hetzel, S.J.; Brooks, M.A.; McGuine, T.A. Association of Competition Volume, Club Sports, and Sport Specialization With Sex and Lower Extremity Injury History in High School Athletes. Sports Health. 2017, 9, 518–523. [Google Scholar] [CrossRef] [PubMed]
- Post, E.G.; Trigsted, S.M.; Riekena, J.W.; Hetzel, S.; McGuine, T.A.; Brooks, M.A.; Bell, D.R. The Association of Sport Specialization and Training Volume with Injury History in Youth Athletes. Am. J. Sports Med. 2017, 45, 1405–1412. [Google Scholar] [CrossRef] [PubMed]
- Weinhandl, J.T.; Earl-Boehm, J.E.; Ebersole, K.T.; Huddleston, W.E.; Armstrong, B.S.; O’Connor, K.M. Reduced hamstring strength increases anterior cruciate ligament loading during anticipated sidestep cutting. Clin. Biomech. 2014, 29, 752–759. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, E.M.; Greenberg, E.T.; Ganley, T.J.; Lawrence, J.T. Strength and functional performance recovery after anterior cruciate ligament reconstruction in preadolescent athletes. Sports Health. 2014, 6, 309–312. [Google Scholar] [CrossRef] [PubMed]
- Lynch, A.D.; Logerstedt, D.S.; Grindem, H.; Eitzen, I.; Hicks, G.E.; Axe, M.J.; Snyder-Mackler, L. Consensus criteria for defining ‘successful outcome’ after ACL injury and reconstruction: A Delaware-Oslo ACL cohort investigation. Br. J. Sports Med. 2015, 49, 335–342. [Google Scholar] [CrossRef]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Application to Practice; Prentice Hall Health: Upper Saddle River, NJ, USA, 2008. [Google Scholar]
- Kim, S.G.; Lee, Y.S. The intra- and inter-rater reliabilities of lower extremity muscle strength assessment of healthy adults using a hand held dynamometer. J. Phys. Ther. Sci. 2015, 27, 1799–1801. [Google Scholar] [CrossRef]
- Mentiplay, B.F.; Perraton, L.G.; Bower, K.J.; Adair, B.; Pua, Y.H.; Williams, G.P.; Clark, R.A. Assessment of Lower Limb Muscle Strength and Power Using Hand-Held and Fixed Dynamometry: A Reliability and Validity Study. PLoS ONE 2015, 10, e0140822. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Demographics | Figure Skaters (N = 73) | Soccer Players (N = 115) | p-Value |
|---|---|---|---|
| Age (years) | 13.8 ± 3.3 | 13.8 ± 1.9 | 0.937 |
| Height (cm) | 154.7 ± 15.7 | 161.4 ± 10.5 | 0.007* |
| Body Mass (kg) | 49.7 ± 14.0 | 54.1 ± 10.7 | 0.016* |
| BMI | 19.9 ± 3.4 | 20.9 ± 4.9 | 0.395 |
| Strength and Ratio by Age | Figure Skaters (N = 73) | Soccer Players (N = 115) | p-Value | Effect Size | |
|---|---|---|---|---|---|
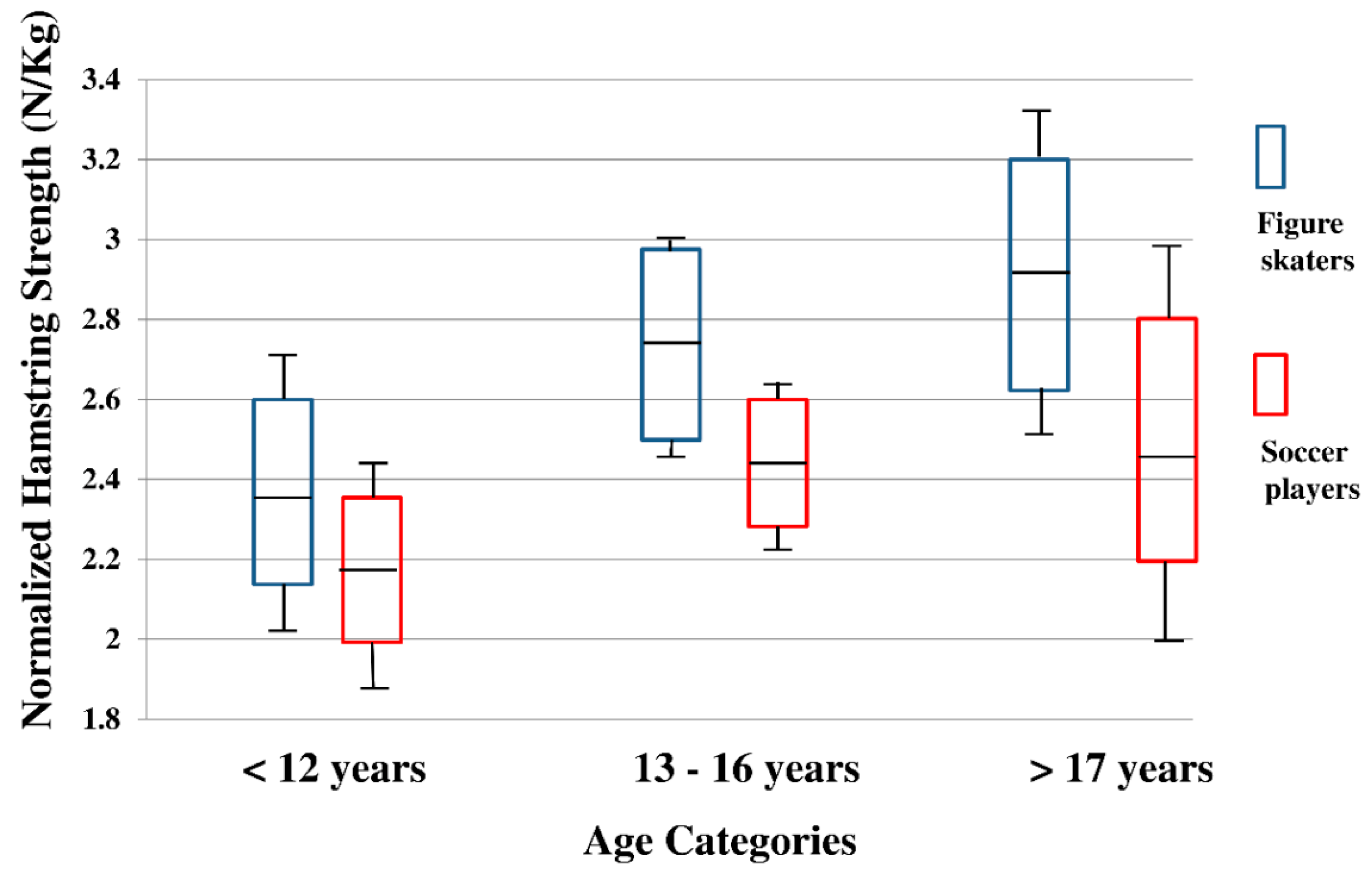
| Hamstrings Strength (N/Kg) | 2.67 (2.55, 2.79) | 2.38 (2.26, 2.50) | 0.001* | 0.061† | |
| Age§ | <12 years | 2.37 (2.15, 2.59) | 2.17 (1.99, 2.36) | 0.003* | 0.062† |
| 13–16 years | 2.72 (2.55, 2.90) | 2.46 (2.34, 2,58) | |||
| >17 years | 2.93 (2.66, 3.19) | 2.49 (2.19, 2.80) | |||
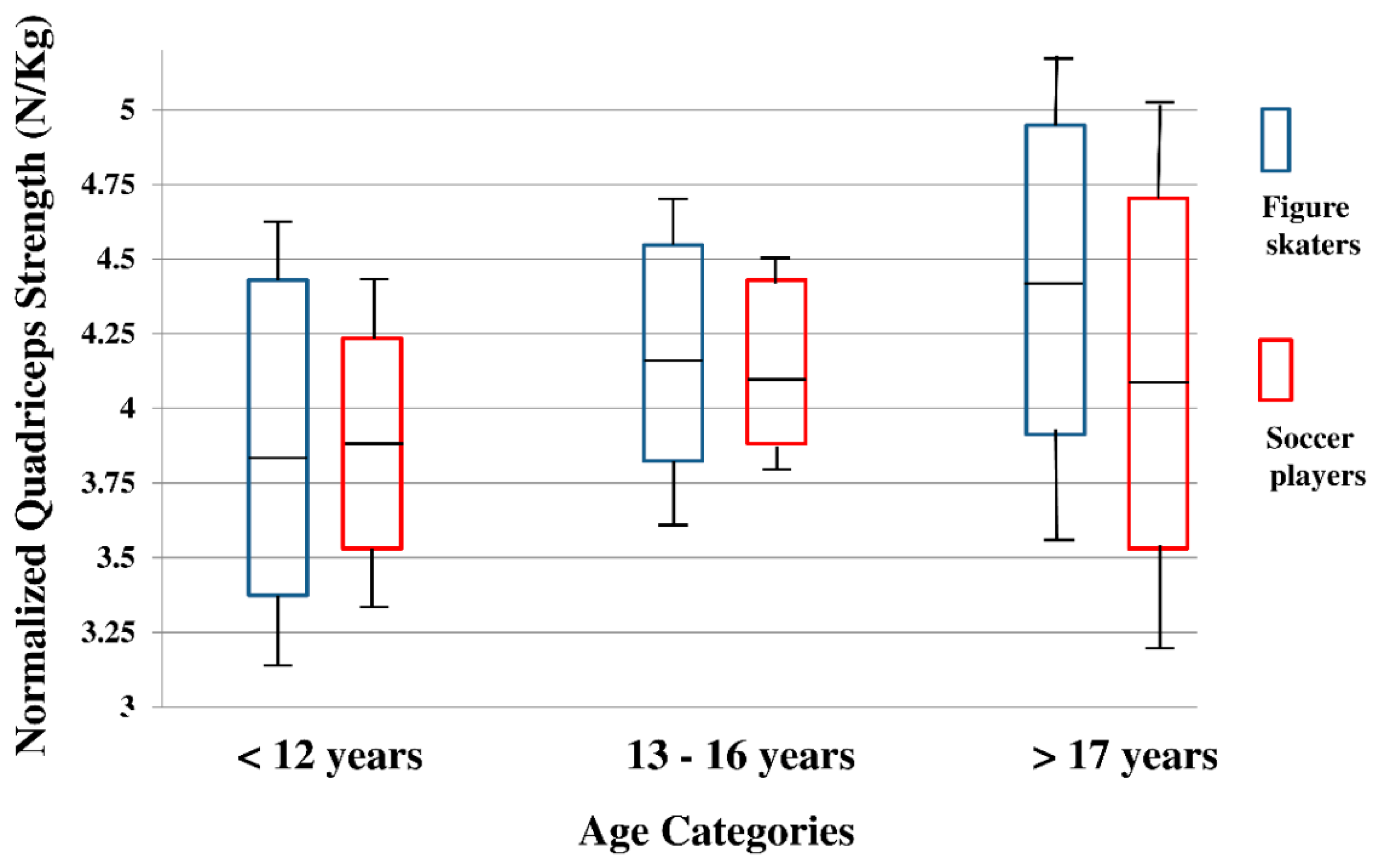
| Quadriceps Strength (N/Kg) | 4.12 (3.88, 4,36) | 4.05 (3.82, 4.29) | 0.700 | 0.001 | |
| Age | <12 years | 3.83 (3.38, 4,38) | 3.90 (3.53, 4.23) | 0.317 | 0.013‡ |
| 13–16 years | 4.17 (3.82, 4.52) | 4.14 (3.90, 4.37) | |||
| >17 years | 4.36 (3.84, 4.88) | 4.13 (3.54, 4.73) | |||
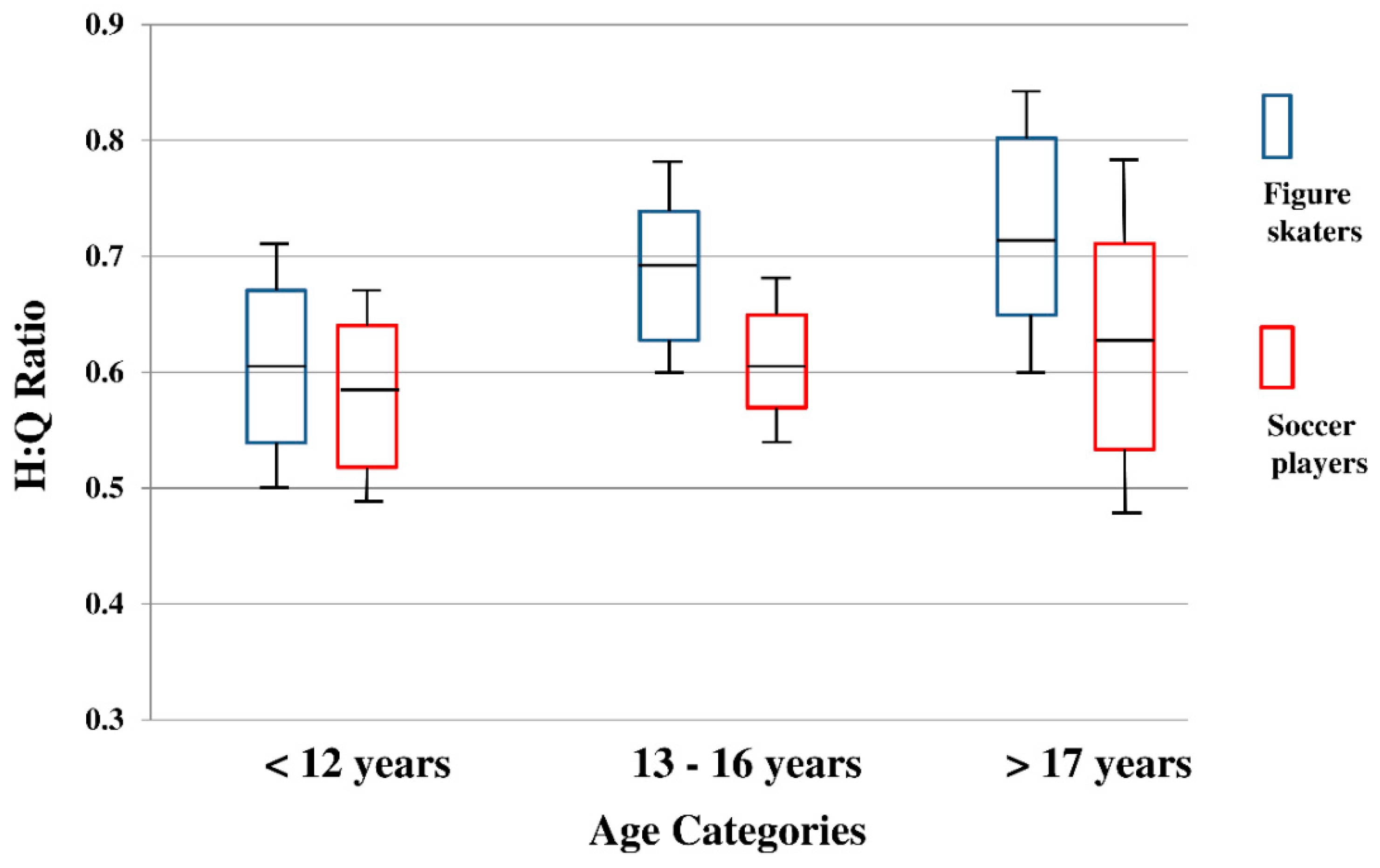
| H:Q Ratio | 0.61 (0.54, 0.68) | 0.58 (0.52, 0.64) | 0.022* | 0.029‡ | |
| Age | < 12 years | 0.61 (0.54, 0.68) | 0.58 (0.52, 0.64) | 0.161 | 0.020‡ |
| 13-16 years | 0.69 (0.63, 0.74) | 0.61 (0.58, 0.65) | |||
| > 17 years | 0.72 (0.64, 0.80) | 0.63 (0.53, 0.72) | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sugimoto, D.; Borg, D.R.; Brilliant, A.N.; Meehan, W.P., III; Micheli, L.J.; Geminiani, E.T. Effect of Sports and Growth on Hamstrings and Quadriceps Development in Young Female Athletes: Cross-Sectional Study. Sports 2019, 7, 158. https://doi.org/10.3390/sports7070158
Sugimoto D, Borg DR, Brilliant AN, Meehan WP III, Micheli LJ, Geminiani ET. Effect of Sports and Growth on Hamstrings and Quadriceps Development in Young Female Athletes: Cross-Sectional Study. Sports. 2019; 7(7):158. https://doi.org/10.3390/sports7070158
Chicago/Turabian StyleSugimoto, Dai, Dennis R. Borg, Anna N. Brilliant, William P. Meehan, III, Lyle J. Micheli, and Ellen T. Geminiani. 2019. "Effect of Sports and Growth on Hamstrings and Quadriceps Development in Young Female Athletes: Cross-Sectional Study" Sports 7, no. 7: 158. https://doi.org/10.3390/sports7070158
APA StyleSugimoto, D., Borg, D. R., Brilliant, A. N., Meehan, W. P., III, Micheli, L. J., & Geminiani, E. T. (2019). Effect of Sports and Growth on Hamstrings and Quadriceps Development in Young Female Athletes: Cross-Sectional Study. Sports, 7(7), 158. https://doi.org/10.3390/sports7070158