Effectiveness of Manual Therapy, Customised Foot Orthoses and Combined Therapy in the Management of Plantar Fasciitis—A RCT

Abstract
1. Introduction
2. Materials and Methods
2.1. Examination Procedures
2.2. Outcome Measures
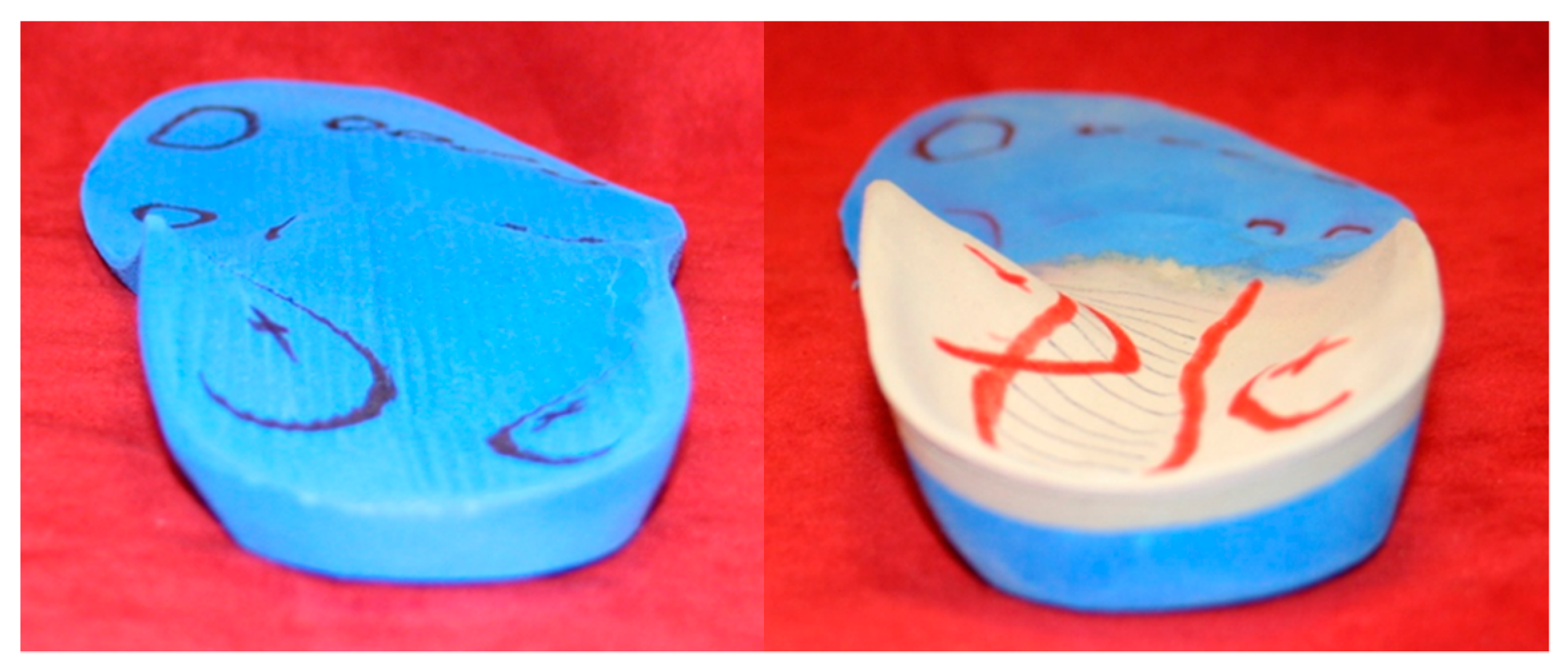
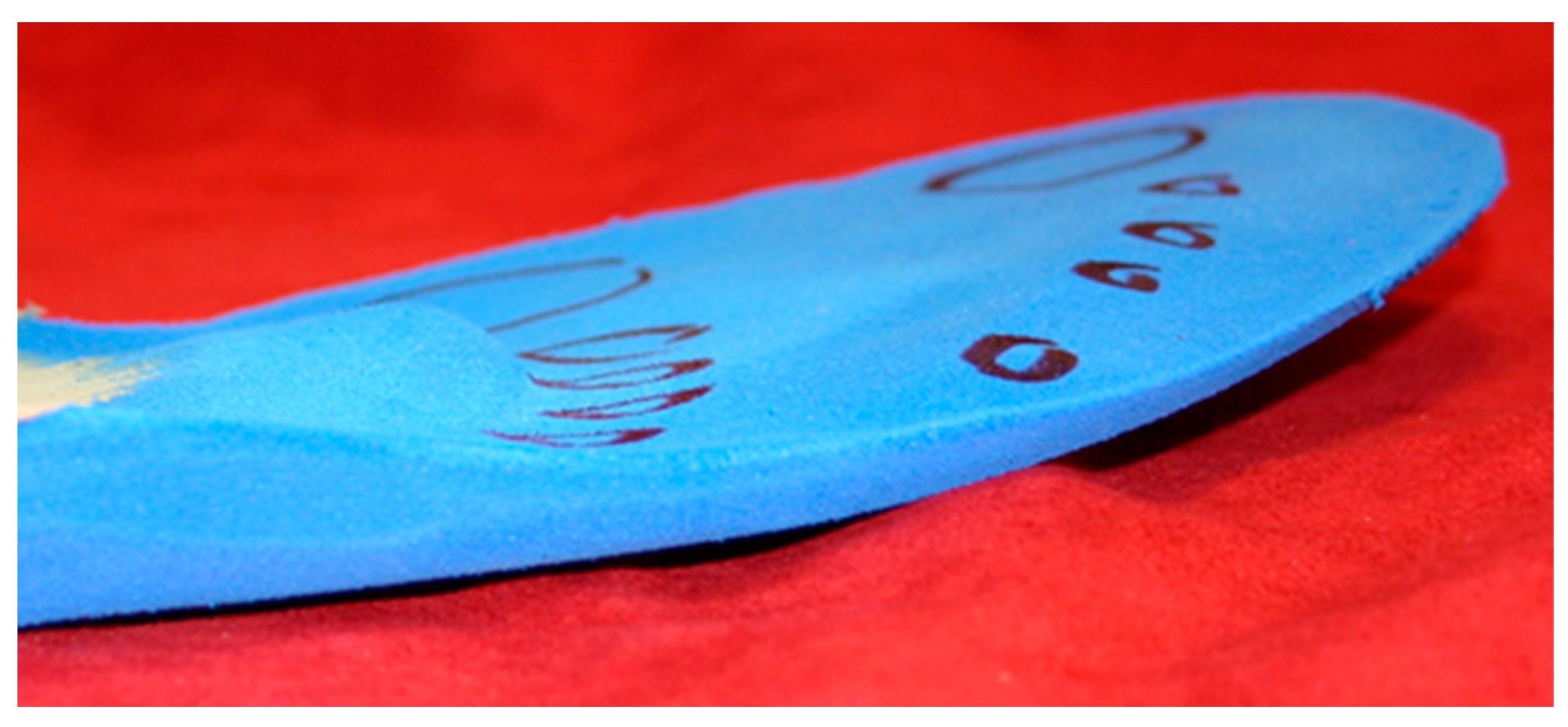
2.3. Interventions
2.4. Statistical Analysis
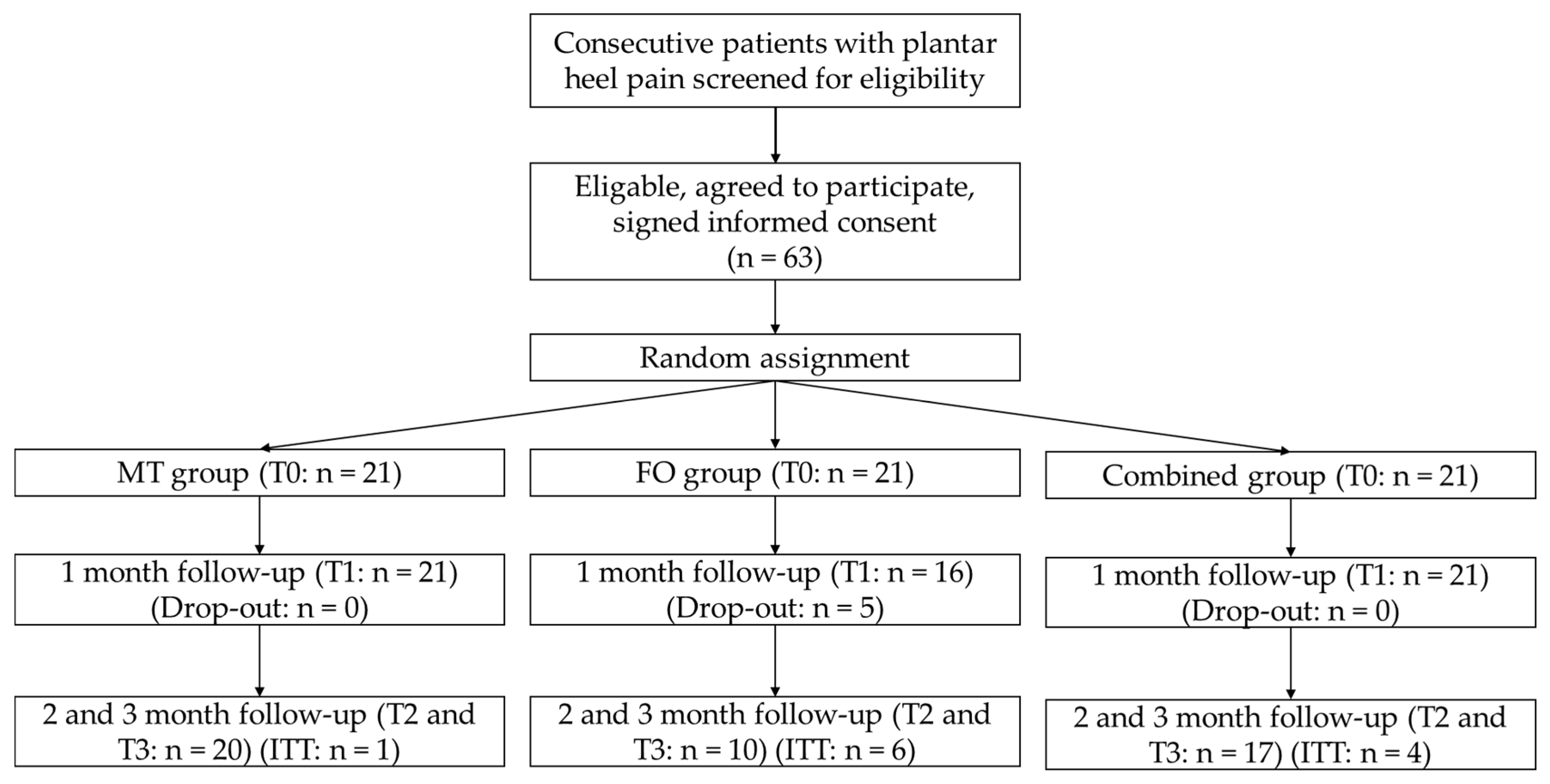
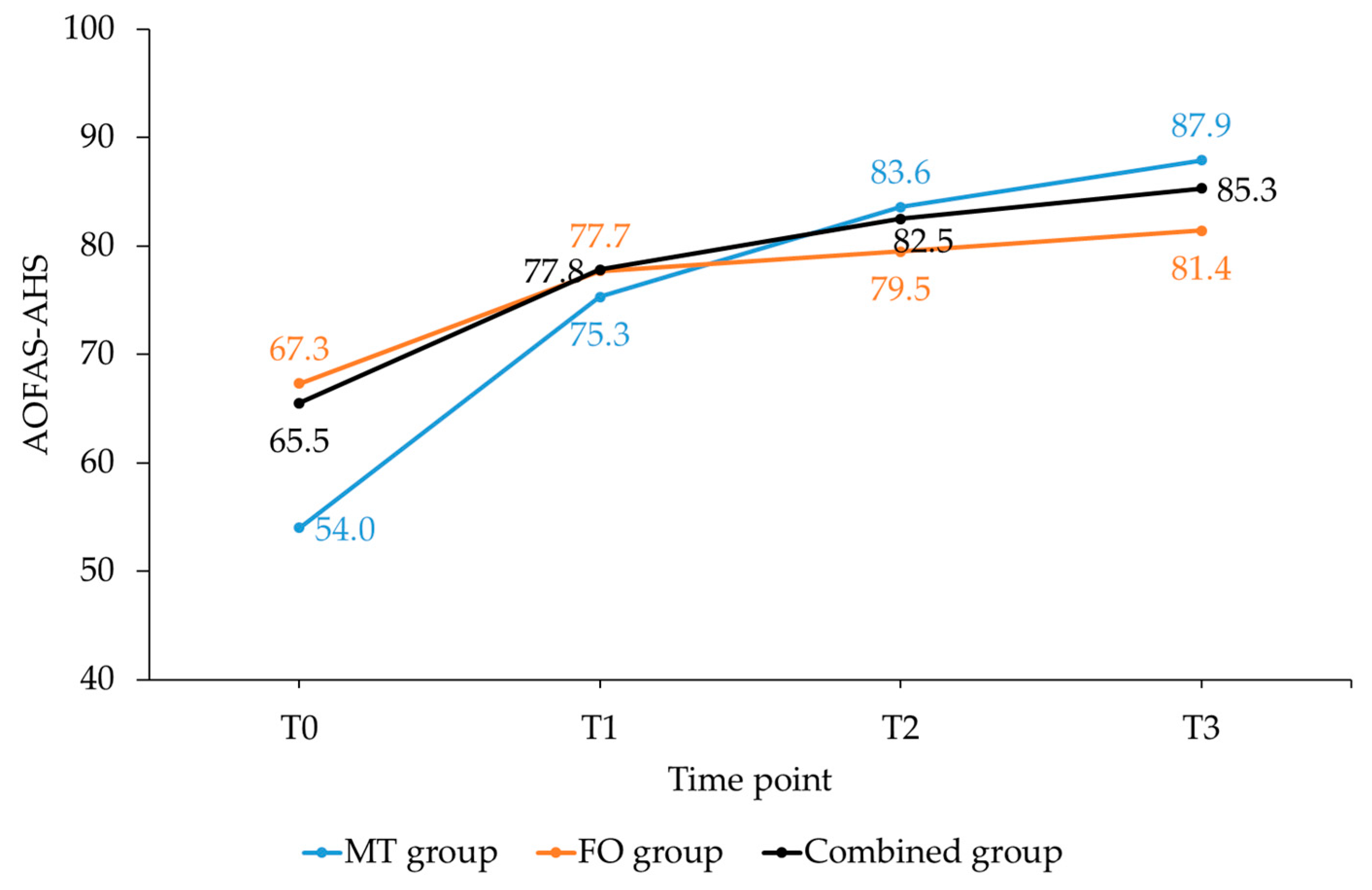
3. Results
4. Discussion
4.1. Comparison with Previous Studies
4.2. Strength and Limitations
4.3. Clinical Implications
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cleland, J.A.; Abbott, J.H.; Kidd, M.O.; Stockwell, S.; Cheney, S.; Gerrard, D.F.; Flynn, T.W. Manual physical therapy and exercise versus electrophysical agents and exercise in the management of plantar heel pain: A multicenter randomized clinical trial. J. Orthop. Sports Phys. Ther. 2009, 39, 573–585. [Google Scholar] [CrossRef] [PubMed]
- Landorf, K.B. Plantar heel pain and plantar fasciitis. BMJ Clin. Evid. 2015, 2015, 1–46. [Google Scholar]
- McMillan, A.M.; Landorf, K.B.; Barrett, J.T.; Menz, H.B.; Bird, A.R. Diagnostic imaging for chronic plantar heel pain: A systematic review and meta-analysis. J. Foot. Ankle Res. 2009, 2, 32. [Google Scholar] [CrossRef] [PubMed]
- Mischke, J.J.; Jayaseelan, D.J.; Sault, J.D.; Emerson Kavchak, A.J. The symptomatic and functional effects of manual physical therapy on plantar heel pain: A systematic review. J. Man. Manip. Ther. 2017, 25, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Pollack, Y.; Shashua, A.; Kalichman, L. Manual therapy for plantar heel pain. Foot 2018, 34, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, G.A.; Munteanu, S.E.; Menz, H.B.; Tan, J.M.; Rabusin, C.L.; Landorf, K.B. Foot orthoses for plantar heel pain: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 322–328. [Google Scholar] [CrossRef]
- Ajimsha, M.S.; Binsu, D.; Chithra, S. Effectiveness of myofascial release in the management of plantar heel pain: A randomized controlled trial. Foot 2014, 24, 66–71. [Google Scholar] [CrossRef]
- Renan-Ordine, R.; Alburquerque-Sendin, F.; de Souza, D.P.; Cleland, J.A.; Fernandez-de-Las-Penas, C. Effectiveness of myofascial trigger point manual therapy combined with a self-stretching protocol for the management of plantar heel pain: A randomized controlled trial. J. Orthop. Sports Phys. Ther. 2011, 41, 43–50. [Google Scholar] [CrossRef]
- Hansen, L.; Krogh, T.P.; Ellingsen, T.; Bolvig, L.; Fredberg, U. Long-term prognosis of plantar fasciitis: A 5- to 15-year follow-up study of 174 patients with ultrasound examination. Orthop. J. Sports Med. 2018, 6, 2325967118757983. [Google Scholar] [CrossRef]
- Goff, J.D.; Crawford, R. Diagnosis and treatment of plantar fasciitis. Am. Fam. Physician 2011, 84, 676–682. [Google Scholar]
- Van Leeuwen, K.D.; Rogers, J.; Winzenberg, T.; van Middelkoop, M. Higher body mass index is associated with plantar fasciopathy/‘plantar fasciitis’: Systematic review and meta-analysis of various clinical and imaging risk factors. Br. J. Sports Med. 2016, 50, 972–981. [Google Scholar] [CrossRef] [PubMed]
- McClinton, S.; Collazo, C.; Vincent, E.; Vardaxis, V. Impaired foot plantar flexor muscle performance in individuals with plantar heel pain and association with foot orthosis use. J. Orthop. Sports Phys. Ther. 2016, 46, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.L.; Davenport, T.E.; Reischl, S.F.; McPoil, T.G.; Matheson, J.W.; Wukich, D.K.; McDonough, C.M.; American Physical Therapy Association. Heel pain-plantar fasciitis: Revision 2014. J. Orthop. Sports Phys. Ther. 2014, 44, 1–33. [Google Scholar] [CrossRef] [PubMed]
- Huffer, D.; Hing, W.; Newton, R.; Clair, M. Strength training for plantar fasciitis and the intrinsic foot musculature: A systematic review. Phys. Ther. Sport 2017, 24, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Hotfiel, T.; Hotfiel, K.H.; Gelse, K.; Engelhardt, M.; Freiwald, J. Einlagenversorgung im leistungssport – indikationen, wirkungsweise, sportspezifische versorgungsstrategien [The use of insoles in competitive sports – Indications, effectiveness, sport specific treatment strategies]. Sports Orthop. Traumatol. 2016, 32, 250–257. [Google Scholar] [CrossRef]
- Whittaker, G.A.; Munteanu, S.E.; Menz, H.B.; Landorf, K.B. Should foot orthoses be used for plantar heel pain? Br. J. Sports Med. 2018, 52, 1224–1225. [Google Scholar] [CrossRef] [PubMed]
- Hawke, F.; Burns, J.; Radford, J.A.; du Toit, V. Custom-made foot orthoses for the treatment of foot pain. Cochrane Database Syst. Rev. 2008, 16, 1–131. [Google Scholar] [CrossRef]
- Brantingham, J.W.; Bonnefin, D.; Perle, S.M.; Cassa, T.K.; Globe, G.; Pribicevic, M.; Hicks, M.; Korporaal, C. Manipulative therapy for lower extremity conditions: Update of a literature review. J. Manipul. Physiol. Ther. 2012, 35, 127–166. [Google Scholar] [CrossRef] [PubMed]
- Brantingham, J.W.; Globe, G.; Pollard, H.; Hicks, M.; Korporaal, C.; Hoskins, W. Manipulative therapy for lower extremity conditions: Expansion of literature review. J. Manipul. Physiol. Ther. 2009, 32, 53–71. [Google Scholar] [CrossRef]
- Fraser, J.J.; Glaviano, N.R.; Hertel, J. Utilization of physical therapy intervention among patients with plantar fasciitis in the united states. J. Orthop. Sports Phys. Ther. 2017, 47, 49–55. [Google Scholar] [CrossRef]
- Shashua, A.; Flechter, S.; Avidan, L.; Ofir, D.; Melayev, A.; Kalichman, L. The effect of additional ankle and midfoot mobilizations on plantar fasciitis: A randomized controlled trial. J. Orthop. Sports Phys. Ther. 2015, 45, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Wynne, M.M.; Burns, J.M.; Eland, D.C.; Conatser, R.R.; Howell, J.N. Effect of counterstrain on stretch reflexes, hoffmann reflexes, and clinical outcomes in subjects with plantar fasciitis. J. Am. Osteopath. Assoc. 2006, 106, 547–556. [Google Scholar] [PubMed]
- Saban, B.; Deutscher, D.; Ziv, T. Deep massage to posterior calf muscles in combination with neural mobilization exercises as a treatment for heel pain: A pilot randomized clinical trial. Man. Ther. 2014, 19, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Burmeister, S. Osteopathie und ihr Effektivität bei Fasciitis Plantaris. Master’s Thesis, Donau Universität Krems, Krems, Germany, 2012. [Google Scholar]
- McClinton, S.; Weber, C.F.; Heiderscheit, B. Low back pain and disability in individuals with plantar heel pain. Foot 2018, 34, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Armijo-Olivo, S.; Warren, S.; Magee, D. Intention to treat analysis, compliance, drop-outs and how to deal with missing data in clinical research: A review. Phys. Ther. Rev. 2009, 14, 36–45. [Google Scholar] [CrossRef]
- Gupta, S.K. Intention-to-treat concept: A review. Perspect. Clin. Res. 2011, 2, 109–112. [Google Scholar] [CrossRef]
- Kitaoka, H.B.; Alexander, I.J.; Adelaar, R.S.; Nunley, J.A.; Myerson, M.S.; Sanders, M. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int. 1994, 15, 349–353. [Google Scholar] [CrossRef]
- Madeley, N.J.; Wing, K.J.; Topliss, C.; Penner, M.J.; Glazebrook, M.A.; Younger, A.S. Responsiveness and validity of the sf-36, ankle osteoarthritis scale, aofas ankle hindfoot score, and foot function index in end stage ankle arthritis. Foot Ankle Int. 2012, 33, 57–63. [Google Scholar] [CrossRef]
- Kostuj, T.; Schaper, K.; Baums, M.H.; Lieske, S. Eine Validierung des aofas-ankle-hindfoot-scale für den deutschen Sprachraum [German Validation of the AOFAS ankle hindfoot scale]. Foot Ankle 2014, 12, 100–106. [Google Scholar]
- Richter, M.; Zech, S.; Geerling, J.; Frink, M.; Knobloch, K.; Krettek, C. A new foot and ankle outcome score: Questionaire based, subjective, visual-analogue-scale, validated and computerized. Foot Ankle Surg. 2006, 12, 191–199. [Google Scholar] [CrossRef]
- Ibrahim, T.; Beiri, A.; Azzabi, M.; Best, A.J.; Taylor, G.J.; Menon, D.K. Reliability and validity of the subjective component of the american orthopaedic foot and ankle society clinical rating scales. J. Foot Ankle Surg. 2007, 46, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.Y.; Chen, J.Y.; Zainul-Abidin, S.; Ying, H.; Koo, K.; Rikhraj, I.S. Minimal clinically important differences for american orthopaedic foot & ankle society score in hallux valgus surgery. Foot Ankle Int. 2017, 38, 551–557. [Google Scholar] [PubMed]
- Dawson, J.; Doll, H.; Coffey, J.; Jenkinson, C. Responsiveness and minimally important change for the manchester-oxford foot questionnaire (moxfq) compared with aofas and sf-36 assessments following surgery for hallux valgus. Osteoarthr. Cartil. 2007, 15, 918–931. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.; Melzack, R. Measurement of pain. Surg. Clin. North Am. 1999, 79, 231–252. [Google Scholar] [CrossRef]
- Olsen, M.F.; Bjerre, E.; Hansen, M.D.; Hilden, J.; Landler, N.E.; Tendal, B.; Hrobjartsson, A. Pain relief that matters to patients: Systematic review of empirical studies assessing the minimum clinically important difference in acute pain. BMC Med. 2017, 15, 35. [Google Scholar] [CrossRef]
- Farrar, J.T.; Young, J.P., Jr.; LaMoreaux, L.; Werth, J.L.; Poole, R.M. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 2001, 94, 149–158. [Google Scholar] [CrossRef]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual analog scale for pain (vas pain), numeric rating scale for pain (nrs pain), mcgill pain questionnaire (mpq), short-form mcgill pain questionnaire (sf-mpq), chronic pain grade scale (cpgs), short form-36 bodily pain scale (sf-36 bps), and measure of intermittent and constant osteoarthritis pain (icoap). Arthrit. Care Res. 2011, 63 (Suppl. 11), S240–S252. [Google Scholar]
- Katz, N.P.; Paillard, F.C.; Ekman, E. Determining the clinical importance of treatment benefits for interventions for painful orthopedic conditions. J. Orthop. Surg. Res. 2015, 10, 24. [Google Scholar] [CrossRef]
- Dimou, E.; Brantingham, J.; Wood, T. A randomized, controlled trial (with blinded observer) of chiropractic manipulation and achilles stretching vs orthotics for the treatment of plantar fasciitis. J. Am. Chiropr. Assoc. 2004, 41, 32–42. [Google Scholar]
- Stecco, C.; Corradin, M.; Macchi, V.; Morra, A.; Porzionato, A.; Biz, C.; De Caro, R. Plantar fascia anatomy and its relationship with achilles tendon and paratenon. J. Anat. 2013, 223, 665–676. [Google Scholar] [CrossRef]
- Childs, J.D.; Piva, S.R.; Fritz, J.M. Responsiveness of the numeric pain rating scale in patients with low back pain. Spine 2005, 30, 1331–1334. [Google Scholar] [CrossRef] [PubMed]
- Michener, L.A.; Snyder, A.R.; Leggin, B.G. Responsiveness of the numeric pain rating scale in patients with shoulder pain and the effect of surgical status. J. Sport Rehabil. 2011, 20, 115–128. [Google Scholar] [CrossRef] [PubMed]
- Garrison, C.; Cook, C. Clinimetrics corner: The global rating of change score (groc) poorly correlates with functional measures and is not temporally stable. J. Man. Manip. Ther. 2012, 20, 178–181. [Google Scholar] [CrossRef] [PubMed][Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | MT Group (n = 21) | FO Group (n = 21) | Combined Group (n = 21) | p-Value |
|---|---|---|---|---|
| Female sex, n (%) | 16 (76.2) | 14 (66.7) | 14 (66.7) | 0.741 |
| BMI (kg/m2) | 28.3 ± 6.2 | 30.4 ± 4.8 | 29.4 ± 4.2 | 0.432 |
| Duration of PF symptoms (month) | 5.3 ± 0.8 | 2.9 ± 1.8 | 5.0 ± 1.2 | <0.012 |
| Back pain, n (%) | 19 (90.5) | 6 (28.6) | 17 (81.0) | <0.012 |
| Duration of back pain (years) | 11.0 ± 8.1 | 2.5 ± 6.0 | 9.0 ± 8.6 | <0.012 |
| Work: Standing, weight bearing, n (%) | 11 (52.4) | 7 (43.7) | 13 (61.9) | 0.022 |
| Sporting activities, n (%) | 17 (81.0) | 12 (57.1) | 18 (85.7) | 0.082 |
| Therapy pre-study, n (%) | 17 (81.0) | 8 (38.1) | 17 (81.0) | <0.011 |
| Duration of therapy pre-study (month) | 3.4 ± 2.4 | 1.2 ± 2.1 | 3.5 ± 2.4 | <0.012 |
| Medications at the start of the study, n (%) | 12 (57.1) | 6 (28.6) | 14 (66.7) | 0.021 |
| Variable | MT Group (n = 21) | FO Group (n = 16) | Combined Group (n = 21) |
|---|---|---|---|
| AOFAS-AHS | 33.9* | 14.1 | 19.1 |
| Pain subscale | 48.8* | 26.3 | 26.3 |
| Function subscale | 24.5* | 6.1 | 6.1 |
| FPFS | 37.2* | 14.6 | 22.9 |
| Pain subscale | 48.4* | 28.4 | 28.4 |
| Function subscale | 32.8* | 19.0 | 19.0 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grim, C.; Kramer, R.; Engelhardt, M.; John, S.M.; Hotfiel, T.; Hoppe, M.W. Effectiveness of Manual Therapy, Customised Foot Orthoses and Combined Therapy in the Management of Plantar Fasciitis—A RCT. Sports 2019, 7, 128. https://doi.org/10.3390/sports7060128
Grim C, Kramer R, Engelhardt M, John SM, Hotfiel T, Hoppe MW. Effectiveness of Manual Therapy, Customised Foot Orthoses and Combined Therapy in the Management of Plantar Fasciitis—A RCT. Sports. 2019; 7(6):128. https://doi.org/10.3390/sports7060128
Chicago/Turabian StyleGrim, Casper, Ruth Kramer, Martin Engelhardt, Swen Malte John, Thilo Hotfiel, and Matthias Wilhelm Hoppe. 2019. "Effectiveness of Manual Therapy, Customised Foot Orthoses and Combined Therapy in the Management of Plantar Fasciitis—A RCT" Sports 7, no. 6: 128. https://doi.org/10.3390/sports7060128
APA StyleGrim, C., Kramer, R., Engelhardt, M., John, S. M., Hotfiel, T., & Hoppe, M. W. (2019). Effectiveness of Manual Therapy, Customised Foot Orthoses and Combined Therapy in the Management of Plantar Fasciitis—A RCT. Sports, 7(6), 128. https://doi.org/10.3390/sports7060128