Development of a Digital-Based Instrument to Assess Perceived Motor Competence in Children: Face Validity, Test-Retest Reliability, and Internal Consistency



Abstract
:1. Introduction
2. Materials and Methods
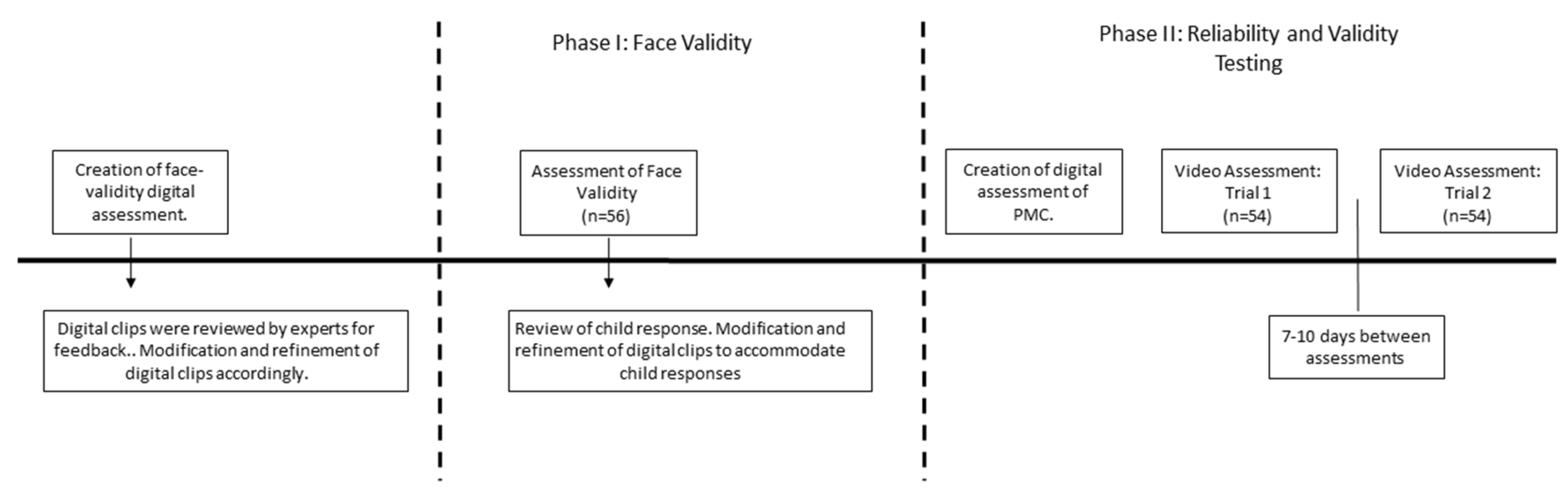
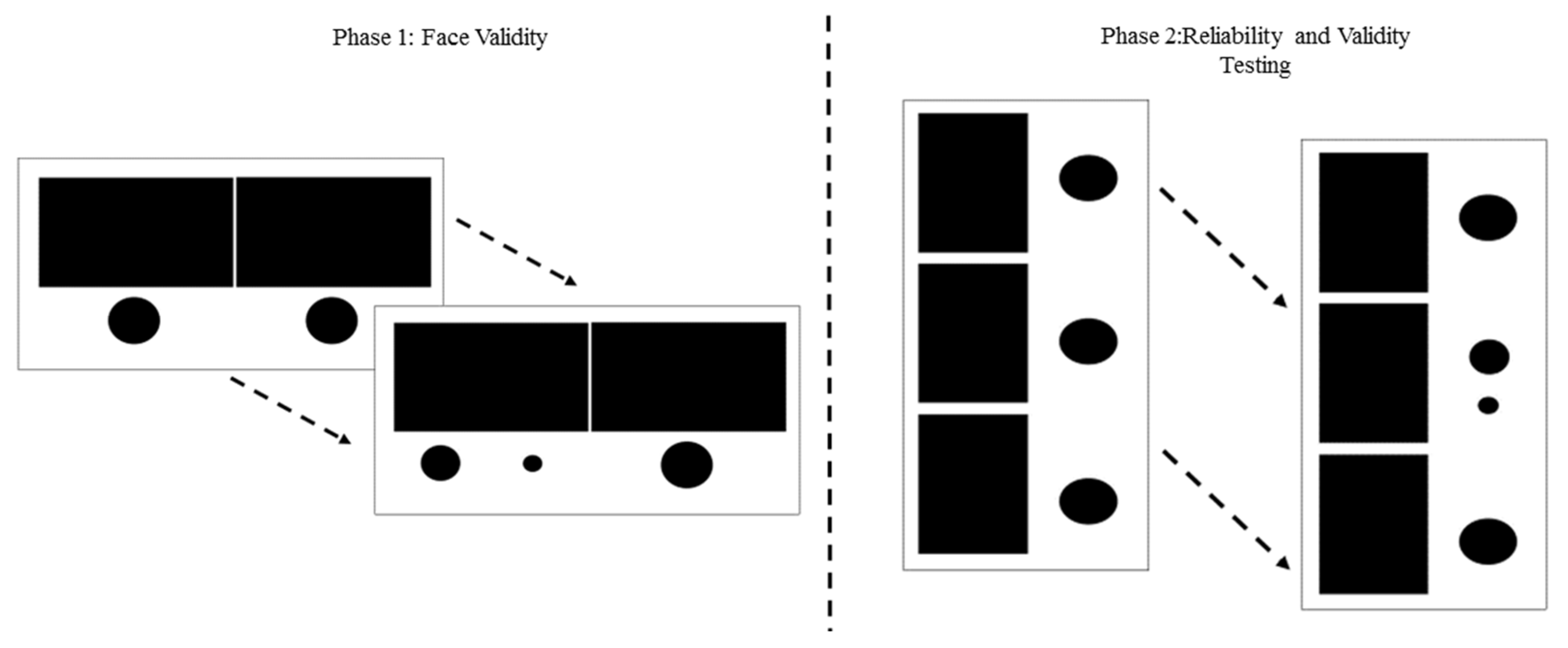
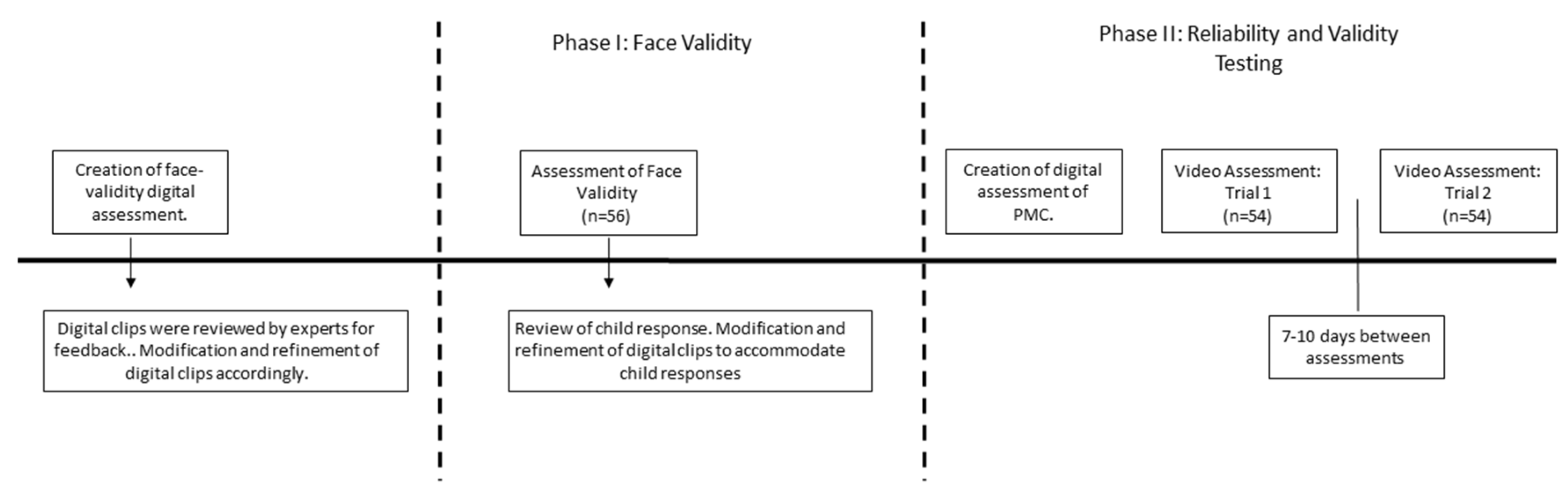
2.1. Phase I: Face Validity
2.2. Phase II: Reliability and Validity Testing
3. Results
3.1. Phase I: Face Validity
3.2. Phase II: Reliability and Validity Testing
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Robinson, L.E.; Stodden, D.F.; Barnett, L.M.; Lopes, V.P.; Logan, S.W.; Rodrigues, L.P.; D’Hondt, E. Motor competence and its effect on positive developmental trajectories of health. Sports Med. 2015, 45, 1273–1284. [Google Scholar] [CrossRef] [PubMed]
- Babic, M.J.; Morgan, P.J.; Plotnikoff, R.C.; Lonsdale, C.; White, R.L.; Lubans, D.R. Physical activity and physical self-concept in youth: Systematic review and meta-analysis. Sports Med. 2014, 44, 1589–1601. [Google Scholar] [CrossRef] [PubMed]
- Stodden, D.F.; Goodway, J.D.; Langendorfer, S.J.; Roberton, M.A.; Rudisill, M.E.; Garcia, C.; Garcia, L.E. A developmental perspective on the role of motor skill competence in physical activity: An emergent relationship. Quest 2008, 60, 290–306. [Google Scholar] [CrossRef]
- Barnett, L.M.; Morgan, P.J.; van Beurden, E.; Beard, J.R. Perceived sports competence mediates the relationship between childhood motor skill proficiency and adolescent physical activity and fitness: A longitudinal assessment. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 40–52. [Google Scholar] [CrossRef] [PubMed]
- Crane, J.R.; Naylor, P.J.; Cook, R.; Temple, V.A. Do perceptions of competence mediate the relationship between fundamental motor skill proficiency and physical activity levels of children in kindergarten? J. Phys. Act. Health 2015, 12, 954–961. [Google Scholar] [CrossRef] [PubMed]
- Harter, S.; Pike, R. The pictorial scale of perceived competence and social acceptance for young children. Child Dev. 1984, 55, 1969–1982. [Google Scholar] [CrossRef] [PubMed]
- LeGear, M.; Greyling, L.; Sloan, E.; Bell, R.I.; Williams, B.-L.; Naylor, P.-J.; Temple, V.A. A window of opportunity? Motor skills and perceptions of competence of children in kindergarten. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.E.; Rudisill, M.E.; Goodway, J.D. Instructional climates in preschool children who are at-risk. Part ii: Perceived physical competence. Res. Q. Exerc. Sport 2009, 80, 543–551. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.E. Effect of a mastery climate motor program on object control skills and perceived physical competence in preschoolers. Res. Q. Exerc. Sport 2011, 82, 355–359. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.E. The relationship between perceived physical competence and fundamental motor skills in preschool children. Child Care Health Dev. 2011, 37, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Barnett, L.M.; Ridgers, N.D.; Zask, A.; Salmon, J. Face validity and reliability of a pictorial instrument for assessing fundamental movement skill perceived competence in young children. J. Sci. Med. Sport 2015, 18, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, D.A. Test of Gross Motor Development-2; Prod-Ed: Austin, TX, USA, 2000. [Google Scholar]
- Barnett, L.M.; Vazou, S.; Abbott, G.; Bowe, S.J.; Robinson, L.E.; Ridgers, N.D.; Salmon, J. Construct validity of the pictorial scale of perceived movement skill competence. Psychol. Sport Exerc. 2016, 22, 294–302. [Google Scholar] [CrossRef]
- Barnett, L.M.; Robinson, L.E.; Webster, E.K.; Ridgers, N.D. Reliability of the pictorial scale of perceived movement skill competence in 2 diverse samples of young children. J. Phys. Act. Health. 2015, 12, 1045–1051. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.E.; Palmer, K.K.; Irwin, J.M.; Webster, E.K.; Dennis, A.L.; Brock, S.J.; Rudisill, M.E. The use of multimedia demonstration on the test of gross motor development–second edition: Performance and participant preference. J. Mot. Learn. Dev. 2015, 3, 110–122. [Google Scholar] [CrossRef]
- Kirchner, G.; Fishburne, G.J. Physical Education for Elementary School Children; Brown & Benchmark: Madison, WI, USA, 1995. [Google Scholar]
- Graham, G. Teaching Children Physical Education: Becoming A Master Teacher; Human Kinetics: Champaign, IL, USA, 2008. [Google Scholar]
- Sim, J.; Wright, C. Research in Health Care: Concepts, Designs and Methods; Nelson Thornes: Chelgenham, UK, 2000. [Google Scholar]
- Nunnally, J.C.; Bernstein, I. Psychological theory; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Maione, L.; Mirenda, P. Effects of video modeling and video feedback on peer-directed social language skills of a child with autism. J. Posit. Behav. Interv. 2006, 8, 106–118. [Google Scholar] [CrossRef]
- Nikopoulos, C.K.; Keenan, M. Promoting social initiation in children with autism using video modeling. Behav. Interv. 2003, 18, 87–108. [Google Scholar] [CrossRef]
- Ihrig, K.; Wolchik, S.A. Peer versus adult models and autistic children’s learning: Acquisition, generalization, and maintenance. J. Autism Dev. Disord. 1988, 18, 67–79. [Google Scholar] [CrossRef] [PubMed]
- VanderBorght, M.; Jaswal, V.K. Who knows best? Preschoolers sometimes prefer child informants over adult informants. Infant Child Dev. 2009, 18, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Jaswal, V.K.; Neely, L.A. Adults don’t always know best preschoolers use past reliability over age when learning new words. Psychol. Sci. 2006, 17, 757–758. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Object Control Skills | % Correct | Locomotor Skills | % Correct |
|---|---|---|---|
| Catch | 94.8 | Gallop | 91.4 |
| Dribble | 87.9 | Hop | 77.6 |
| Kick | 77.6 | Jump | 96.6 |
| Roll | 91.4 | Leap | 93.1 |
| Strike | 96.6 | Run | 94.8 |
| Throw | 58.6 | Slide | 94.8 |
| Total | 87.5 | Total | 94.6 |
| Subtest | Sex | Alphas Test 1 | ICC (LCI-UCI) |
|---|---|---|---|
| Object control | All | 0.48 | 0.79 (0.64–0.88) |
| Girls | 0.55 | 0.80 (0.56–0.91) | |
| Boys | 0.42 | 0.77 (0.50–0.89) | |
| Locomotor | All | 0.49 | 0.77 (0.61–0.87) |
| Girls | 0.68 | 0.79 (0.53–0.91) | |
| Boys | 0.58 | 0.75 (0.46–0.88) | |
| Total | All | 0.62 | 0.83 (0.71–0.90) |
| Girls | 0.58 | 0.82 (0.61–0.92) | |
| Boys | 0.64 | 0.83 (0.65–0.92) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Robinson, L.E.; Palmer, K.K. Development of a Digital-Based Instrument to Assess Perceived Motor Competence in Children: Face Validity, Test-Retest Reliability, and Internal Consistency. Sports 2017, 5, 48. https://doi.org/10.3390/sports5030048
Robinson LE, Palmer KK. Development of a Digital-Based Instrument to Assess Perceived Motor Competence in Children: Face Validity, Test-Retest Reliability, and Internal Consistency. Sports. 2017; 5(3):48. https://doi.org/10.3390/sports5030048
Chicago/Turabian StyleRobinson, Leah E., and Kara K. Palmer. 2017. "Development of a Digital-Based Instrument to Assess Perceived Motor Competence in Children: Face Validity, Test-Retest Reliability, and Internal Consistency" Sports 5, no. 3: 48. https://doi.org/10.3390/sports5030048
APA StyleRobinson, L. E., & Palmer, K. K. (2017). Development of a Digital-Based Instrument to Assess Perceived Motor Competence in Children: Face Validity, Test-Retest Reliability, and Internal Consistency. Sports, 5(3), 48. https://doi.org/10.3390/sports5030048