Condition Changes Before and After the Coronavirus Disease 2019 Pandemic in Adolescent Athletes and Development of a Non-Contact Medical Checkup Application

 , , , , ,
, , , , ,
Abstract

1. Introduction
2. Materials and Methods
2.1. Ethical Approval and Informed Consent
2.2. Study Design and Setting
2.2.1. Questionnaire to Assess Pain
2.2.2. Physical Examination
2.2.3. Assessment of Pre- and Post-Pandemic Physical Condition and Statistical Analysis
2.2.4. Development of a Smartphone Application for Self-Checkup
2.2.5. Assessment of the Developed Smartphone Application for Self-Checkup
3. Results
3.1. Participant Characteristics
3.2. Pre- and Post-Pandemic Physical Condition
3.3. Discrepancies Between Physician-Conducted Medical Checkup Results and Self-Checked Results Using the App
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| COVID-19 | Coronavirus disease 2019 |
| ICC | Intraclass correlation coefficient |
References
- Zu, Z.Y.; Jiang, M.D.; Xu, P.P.; Chen, W.; Ni, Q.Q.; Lu, G.M.; Zhang, L.J. Coronavirus disease 2019 (COVID-19): A perspective from China. Radiology 2020, 296, E15–E25. [Google Scholar] [CrossRef]
- World Health Organization. General’s Opening Remarks at the Media Briefing on COVID-19. Published Online 2020, WHO, Dirs. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 1 July 2025).
- Liu, J.; Lou, J.; Wang, Y.; Zhang, J. Risk management strategies for the 2022 Olympic winter games: The Beijing scheme. J. Sport Health Sci. 2022, 11, 545–547. [Google Scholar] [CrossRef]
- Washif, J.A.; Farooq, A.; Krug, I.; Pyne, D.B.; Verhagen, E.; Taylor, L.; Wong, D.P.; Mujika, I.; Cortis, C.; Haddad, M.; et al. Training during the COVID-19 lockdown: Knowledge, beliefs, and practices of 12,526 athletes from 142 countries and six continents. Sports Med. 2022, 52, 933–948. [Google Scholar] [CrossRef]
- Bok, D.; Chamari, K.; Foster, C. The pitch invader-COVID-19 canceled the game: What can science do for us, and what can the pandemic do for science? Int. J. Sports Physiol. Perform. 2020, 15, 917–919. [Google Scholar] [CrossRef] [PubMed]
- Martens, G.; Delvaux, F.; Forthomme, B.; Kaux, J.F.; Urhausen, A.; Bieuzen, F.; Leclerc, S.; Winkler, L.; Brocherie, F.; Nedelec, M.; et al. Exercise-based injury prevention in high-level and professional athletes: Narrative review and proposed standard operating procedure for future lockdown-like contexts after COVID-19. Front. Sports Act. Living 2021, 3, 745765. [Google Scholar] [CrossRef]
- López-Moreno, M.; López, M.T.I.; Miguel, M.; Garcés-Rimón, M. Physical and psychological effects related to food habits and lifestyle changes derived from COVID-19 home confinement in the Spanish population. Nutrients 2020, 12, 3445. [Google Scholar] [CrossRef]
- Barkley, J.E.; Lepp, A.; Glickman, E.; Farnell, G.; Beiting, J.; Wiet, R.; Dowdell, B. The acute effects of the COVID-19 pandemic on physical activity and sedentary behavior in university students and employees. Int. J. Exerc. Sci. 2020, 13, 1326–1339. [Google Scholar] [CrossRef] [PubMed]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [PubMed]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1.6 million participants. Lancet Child. Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Tison, G.H.; Avram, R.; Kuhar, P.; Abreau, S.; Marcus, G.M.; Pletcher, M.J.; Olgin, J.E. Worldwide effect of COVID-19 on physical activity: A descriptive study. Ann. Intern. Med. 2020, 173, 767–770. [Google Scholar] [CrossRef]
- Castañeda-Babarro, A.; Arbillaga-Etxarri, A.; Gutiérrez-Santamaría, B.; Coca, A. Physical activity change during COVID-19 confinement. Int. J. Environ. Res. Public Health 2020, 17, 6878. [Google Scholar] [CrossRef]
- Do, B.; Kirkland, C.; Besenyi, G.M.; Carissa Smock, M.; Lanza, K. Youth physical activity and the COVID-19 pandemic: A systematic review. Prev. Med. Rep. 2022, 29, 101959. [Google Scholar] [CrossRef]
- Kljajević, V.; Stanković, M.; Đorđević, D.; Trkulja-Petković, D.; Jovanović, R.; Plazibat, K.; Oršolić, M.; Čurić, M.; Sporiš, G. Physical activity and physical fitness among university students—A systematic review. Int. J. Environ. Res. Public Health 2021, 19, 158. [Google Scholar] [CrossRef]
- Patti, A.; Giustino, V.; Figlioli, F.; Miceli, M.; Barca, M.; Drid, P.; Palma, A.; Bianco, A. The role of school physical education on adolescents’ fitness levels during the pandemic period from COVID-19: An observational study of the Italian scientific high school-section sport and physical activity. Front. Public Health 2022, 10, 1010236. [Google Scholar] [CrossRef] [PubMed]
- Bonilla, D.A.; Cardozo, L.A.; Vélez-Gutiérrez, J.M.; Arévalo-Rodríguez, A.; Vargas-Molina, S.; Stout, J.R.; Kreider, R.B.; Petro, J.L. Exercise selection and common injuries in fitness centers: A systematic integrative review and practical recommendations. Int. J. Environ. Res. Public Health 2022, 19, 12710. [Google Scholar] [CrossRef] [PubMed]
- Washif, J.A.; Kok, L.Y.; James, C.; Beaven, C.M.; Farooq, A.; Pyne, D.B.; Chamari, K. Athlete level, sport-type, and gender influences on training, mental health, and sleep during the early COVID-19 lockdown in Malaysia. Front. Physiol. 2022, 13, 1093965. [Google Scholar] [CrossRef]
- Washif, J.A.; Mohd Kassim, S.F.A.; Lew, P.C.F.; Chong, C.S.M.; James, C. Athlete’s perceptions of a “quarantine” training camp during the COVID-19 lockdown. Front. Sports Act. Living 2021, 14, 622858. [Google Scholar] [CrossRef]
- Radzimiński, Ł.; Lorenzo-Martinez, M.; Konefał, M.; Chmura, P.; Andrzejewski, M.; Jastrzębski, Z.; Padrón-Cabo, A. Changes of physical match performance after the COVID-19 lockdown in professional soccer players according to their playing position. Biol. Sport 2022, 39, 1087–1093. [Google Scholar] [CrossRef]
- Seshadri, D.R.; Thom, M.L.; Harlow, E.R.; Drummond, C.K.; Voos, J.E. Case report: Return to sport following the COVID-19 lockdown and its impact on injury rates in the German soccer league. Front. Sports Act. Living 2021, 3, 604226. [Google Scholar] [CrossRef]
- Chamari, K.; Schumacher, Y.O.; Chaabane, M.; Rekik, R.N.; Chebbi, S.; Daoud, R.; Bache-Mathiesen, L.K.; Alkhelaifi, K.; Bahr, R.; Tabben, M. Impact of COVID-19 lockdown on injury risk in Qatar’s professional football. J. Sci. Med. Sport 2023, 26, 522–527. [Google Scholar] [CrossRef] [PubMed]
- Tondelli, E.; Zabaloy, S.; Comyns, T.M.; Kenny, I.C. Effect of COVID-19 lockdown on injury incidence and burden in amateur rugby union. Phys. Ther. Sport 2023, 59, 85–91. [Google Scholar] [CrossRef]
- Patel, S.R.; Uriegas, N.A.; Armstrong, T.A.; Stover, R.M.; Games, K.E.; Winkelmann, Z.K. Digital health literacy and social determinants of health affecting telehealth use by athletic trainers. J. Sport Rehabil. 2024, 34, 42–51. [Google Scholar] [CrossRef]
- Stavric, V.; Kayes, N.M.; Rashid, U.; Saywell, N.L. The effectiveness of self-guided digital intervensions to improve physical activity and exercise outcomes for people with chronic conditions: A systematic review and meta-analysis. Front. Rehabil. Sci. 2022, 3, 925620. [Google Scholar] [CrossRef]
- Maytin, L.; Maytin, J.; Agarwal, P.; Krenitsky, A.; Krenitsky, J.; Epstein, R.S. Attitudes and perceptions toward COVID-19 digital surveillance: Survey of young adults in the United States. JMIR Form. Res. 2021, 5, e23000. [Google Scholar] [CrossRef] [PubMed]
- Kijima, H.; Fujii, M.; Kawano, T.; Saito, H.; Miyakoshi, N. Characteristics of adolescent athletes with pain during sports activities: Evaluation of flexibility using ultrasound elastography. J. Phys. Fit. Sports Med. 2023, 12, 35–44. [Google Scholar] [CrossRef]
- Whitehead, N.A.; Mohammed, K.D.; Fulcher, M.L. Does the Beighton score correlate with specific measures of shoulder joint laxity? Orthop. J. Sports Med. 2018, 6, 2325967118770633. [Google Scholar] [CrossRef]
- Marijančić, V.; Grubić Kezele, T.; Peharec, S.; Dragaš-Zubalj, N.; Pavičić Žeželj, S.; Starčević-Klasan, G. Relationship between physical activity and sedentary behavior, spinal curvatures, endurance and balance of the trunk muscles—Extended physical health analysis in young adults. Int. J. Environ. Res. Public Health 2023, 20, 6938. [Google Scholar] [CrossRef]
- Goyal, J.; Rakhra, G. Sedentarism and chronic health problems. Korean J. Fam. Med. 2024, 45, 239–257. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, L.G.; Zubler, C. Physical and psychological burden of bed rest on patients following free flap reconstruction of the lower limb: A systematic review and possible solutions. J. Clin. Med. 2025, 14, 705. [Google Scholar] [CrossRef] [PubMed]
- Lepers, R.; Mater, A.; Assadi, H.; Zanou, N.; Gremeaux, V.; Place, N. Effect of 12 weeks of detraining and retraining on the cardiorespiratory fitness in a competitive master athlete: A case study. Front. Physiol. 2024, 15, 1508642. [Google Scholar] [CrossRef]
- Ehresman, B.A.; Lehecka, B.J.; Hiser, D.; Koster, L.; Wietharn, J. Improved hip flexibility and gluteal function following a daily lunge-and-reach stretching intervention. Int. J. Sports Phys. Ther. 2025, 20, 814–823. [Google Scholar] [CrossRef] [PubMed]
- Solheim, E.; Rosenlund, M.; Ulsaker, K.G.; Parkar, A.P. Self-assessment of range of motion in patients undergoing surgery for a unilateral shoulder condition. Acta Orthop. Traumatol. Turc. 2023, 57, 340–347. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Before COVID | After COVID | p-Value | |
|---|---|---|---|
| Restricted finger–floor distance | 19.5% | 14.5% | 0.4940 |
| Laxity of shoulder (dominant side) | 82.0% | 88.2% | 0.3578 |
| Laxity of shoulder (nondominant side) | 55.1% | 64.7% | 0.2700 |
| Restricted range of motion—ankle | 22.5% | 23.5% | 0.8934 |
| Low back pain during lumbar extension | 9.83% | 8.82% | 0.8481 |
| Laxity of finger | 25.4% | 11.8% | 0.0730 |
| Restricted elbow flexion | 7.01% | 0% | 0.1103 |
| Restricted elbow extension | 2.08% | 2.94% | 0.7373 |
| Laxity of elbow extension | 45.8% | 29.4% | 0.0620 |
| Restricted knee flexion | 12.9% | 11.8% | 0.8443 |
| Restricted knee extension | 3.04% | 2.94% | 0.9736 |
| Laxity of knee extension | 23.8% | 17.6% | 0.4142 |
| Straight leg raising angle (dominant side) | 75.6° | 75.7° | 0.9498 |
| Straight leg raising angle (nondominant side) | 75.6° | 77.1° | 0.5710 |
| Range of hip internal rotation (dominant side) | 36.8° | 34.0° | 0.3655 |
| Range of hip internal rotation (nondominant side) | 36.8° | 36.5° | 0.9044 |
| Range of hip external rotation (dominant side) | 53.8° | 46.8° | 0.0062 * |
| Range of hip external rotation (nondominant side) | 53.5° | 48.0° | 0.0252 * |
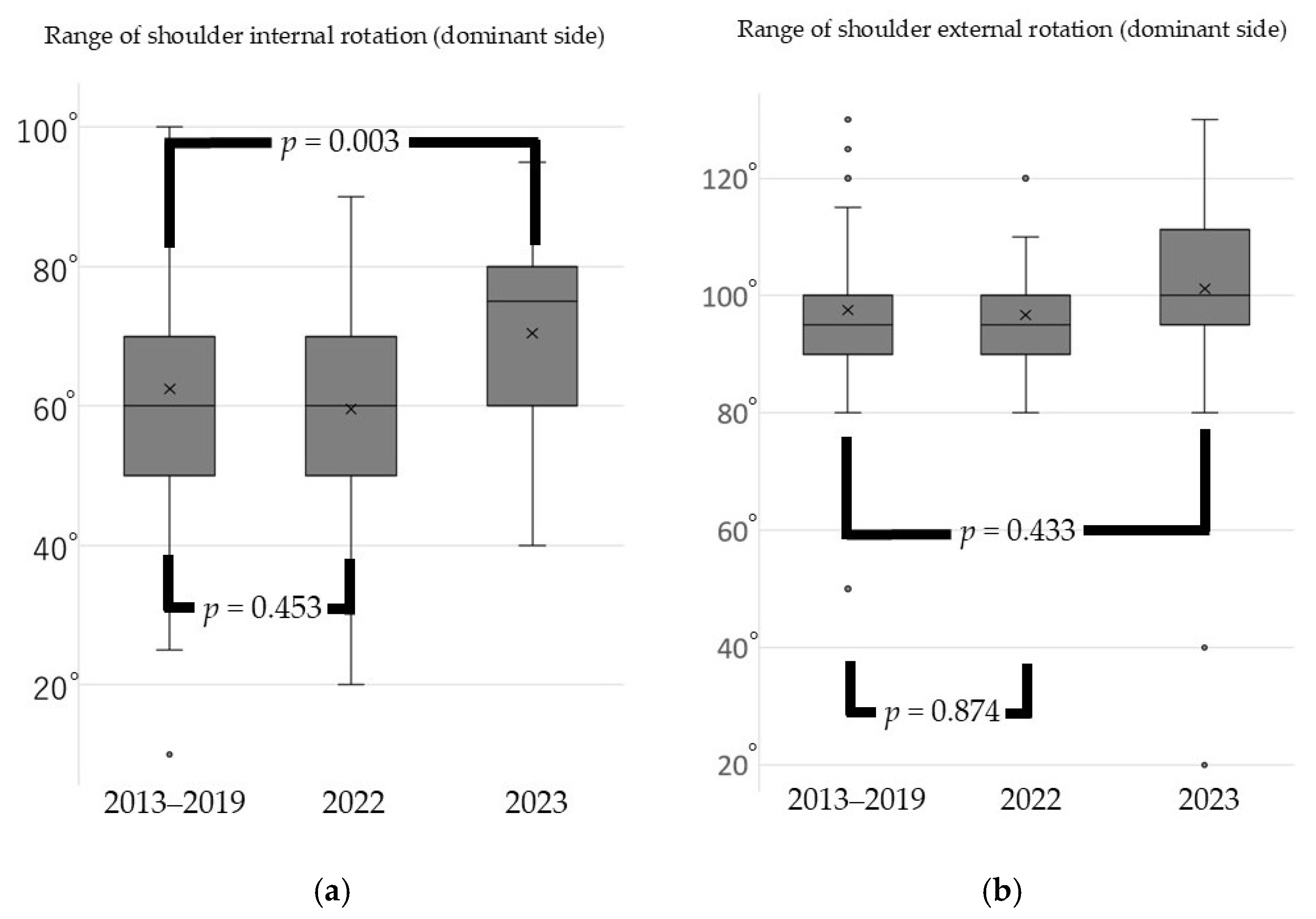
| Range of shoulder internal rotation (dominant side) | 62.5° | 54.7° | 0.0042 * |
| Range of shoulder internal rotation (nondominant side) | 66.4° | 61.9° | 0.1123 |
| Range of shoulder external rotation (dominant side) | 97.6° | 93.5° | 0.0282 * |
| Range of shoulder external rotation (nondominant side) | 95.9° | 92.9° | 0.0890 |
| Heel–buttock distance | 4.0 cm | 10.4 cm | <0.0001 * |
| Growth of body height in 1 year | 4.9 cm | 4.1 cm | 0.4170 |
| Positive rate of “too many toes” sign | 22.5% | 23.5% | 0.889 |
| Reports pain during sports activity | 28.6% | 32.4% | 0.6394 |
| Percentage | |
|---|---|
| Restricted finger—floor distance | 23.3% |
| Laxity of shoulder | 33.3% |
| Restricted range of motion—ankle | 16.7% |
| Low back pain during lumbar extension | 10.0% |
| Laxity of finger | 16.7% |
| Estimation of elbow flexion angle | 0% |
| Estimation of elbow extension angle | 50.0% |
| Estimation of knee flexion angle | 13.3% |
| Estimation of knee extension angle | 33.3% |
| Straight leg raising angle | 31.7% (>20°) |
| Range of hip internal rotation | 45.0% (>20°) |
| Range of hip external rotation | 25.0% (>20°) |
| Range of shoulder internal rotation | 83.3% (>20°) |
| Range of shoulder external rotation | 41.7% (>20°) |
| Heel–buttock distance | 50.0% (>5 cm) |
| Positive rate of “too many toes” sign | 33.3% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kijima, H.; Segawa, T.; Saito, K.; Tsukamoto, H.; Kimura, R.; Sasaki, K.; Murata, S.; Tominaga, K.; Morishita, Y.; Asaka, Y.; et al. Condition Changes Before and After the Coronavirus Disease 2019 Pandemic in Adolescent Athletes and Development of a Non-Contact Medical Checkup Application. Sports 2025, 13, 256. https://doi.org/10.3390/sports13080256
Kijima H, Segawa T, Saito K, Tsukamoto H, Kimura R, Sasaki K, Murata S, Tominaga K, Morishita Y, Asaka Y, et al. Condition Changes Before and After the Coronavirus Disease 2019 Pandemic in Adolescent Athletes and Development of a Non-Contact Medical Checkup Application. Sports. 2025; 13(8):256. https://doi.org/10.3390/sports13080256
Chicago/Turabian StyleKijima, Hiroaki, Toyohito Segawa, Kimio Saito, Hiroaki Tsukamoto, Ryota Kimura, Kana Sasaki, Shohei Murata, Kenta Tominaga, Yo Morishita, Yasuhito Asaka, and et al. 2025. "Condition Changes Before and After the Coronavirus Disease 2019 Pandemic in Adolescent Athletes and Development of a Non-Contact Medical Checkup Application" Sports 13, no. 8: 256. https://doi.org/10.3390/sports13080256
APA StyleKijima, H., Segawa, T., Saito, K., Tsukamoto, H., Kimura, R., Sasaki, K., Murata, S., Tominaga, K., Morishita, Y., Asaka, Y., Saito, H., & Miyakoshi, N. (2025). Condition Changes Before and After the Coronavirus Disease 2019 Pandemic in Adolescent Athletes and Development of a Non-Contact Medical Checkup Application. Sports, 13(8), 256. https://doi.org/10.3390/sports13080256