
A Battery of Jump Tests Helps Discriminating Between Subjects With and Without Chronic Ankle Instability

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients Recruitment
2.2. Patients’ Assessment
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ventura, A.; Legnani, C. Chronic ankle instability. In Arthroscopy and Sport Injuries: Applications in High-Level Athletes; Volpi, P., Ed.; Springer: Cham, Switzerland, 2016; pp. 399–404. [Google Scholar]
- Herb, C.C.; Shank, K. Ankle kinematics during a drop-vertical jump in patients with chronic ankle instability and healthy controls: A bivariate confidence interval comparison. Gait Posture 2023, 104, 147–150. [Google Scholar] [CrossRef] [PubMed]
- Labanca, L.; Tedeschi, R.; Mosca, M.; Benedetti, M.G. Individuals With Chronic Ankle Instability Show Abnormalities in Maximal and Submaximal Isometric Strength of the Knee Extensor and Flexor Muscles. Am. J. Sports Med. 2024, 52, 1328–1335. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, U.; Hoffman, J.R.; Springer, S. Dynamic postural control in individuals with and without chronic ankle instability-do the modified star-excursion balance test and jump-landing stabilization have the same control mechanism? Phys. Ther. Sport 2023, 60, 104–111. [Google Scholar] [CrossRef]
- Taghavi Asl, A.; Shojaedin, S.S.; Hadadnezhad, M. Comparison of effect of wobble board training with and without cognitive intervention on balance, ankle proprioception and jump landing kinetic parameters of men with chronic ankle instability: A randomized control trial. BMC Musculoskelet. Disord. 2022, 23, 888. [Google Scholar] [CrossRef]
- Legnani, C.; Del Re, M.; Peretti, G.M.; Borgo, E.; Macchi, V.; Ventura, A. Limb asymmetries persist 6 months after anterior cruciate ligament reconstruction according to the results of a jump test battery. Front. Med. 2024, 11, 1303172. [Google Scholar] [CrossRef] [PubMed]
- West, T.J.; Bruder, A.M.; Crossley, K.M.; Culvenor, A.G. Unilateral tests of lower-limb function as prognostic indicators of future knee-related outcomes following anterior cruciate ligament injury: A systematic review and meta-analysis of 13,150 adolescents and adults. Br. J. Sports Med. 2023, 57, 855–863. [Google Scholar] [CrossRef]
- Baus, J.; Harry, J.R.; Yang, J. Jump and Landing Biomechanical Variables and Methods: A Literature Review. Crit. Rev. Biomed. Eng. 2020, 48, 211–222. [Google Scholar] [CrossRef]
- Kawabata, S.; Ozone, K.; Minegishi, Y.; Oka, Y.; Terada, H.; Takasu, C.; Kojima, T.; Kano, T.; Kanemura, N.; Murata, K. Chronic Ankle Joint Instability Induces Ankle Sensorimotor Dysfunction: A Controlled Laboratory Study. Am. J. Sports Med. 2024, 52, 739–749. [Google Scholar] [CrossRef]
- Balasukumaran, T.; Gottlieb, U.; Springer, S. Spatiotemporal gait characteristics and ankle kinematics of backward walking in people with chronic ankle instability. Sci. Rep. 2020, 10, 11515. [Google Scholar] [CrossRef]
- Yen, S.C.; Qian, S.; Folmar, E.; Hasson, C.J.; Chou, C.A. Recurrence Quantification Analysis of Ankle Kinematics During Gait in Individuals With Chronic Ankle Instability. Front. Sports Act. Living 2022, 4, 893745. [Google Scholar] [CrossRef]
- Gribble, P.A.; Delahunt, E.; Bleakley, C.; Caulfield, B.; Docherty, C.L.; Fourchet, F.; Fong, D.; Hertel, J.; Hiller, C.; Kaminski, T.W.; et al. Selection criteria for patients with chronic ankle instability in controlled research: A position statement of the International Ankle Consortium. J. Orthop. Sports Phys. Ther. 2013, 43, 585–591. [Google Scholar] [CrossRef]
- Legnani, C.; Del Re, M.; Viganò, M.; Peretti, G.M.; Borgo, E.; Ventura, A. Relationships between jumping performance and psychological readiness to return to sport 6 months following anterior cruciate ligament reconstruction: A cross-sectional study. J. Clin. Med. 2023, 12, 626. [Google Scholar] [CrossRef]
- Gustavsson, A.; Neeter, C.; Thomeé, P.; Grävare Silbernagel, K.; Augustsson, J.; Thomeé, R.; Karlsson, J. A test battery for evaluating hop performance in patients with an ACL injury and patients who have undergone ACL reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2006, 14, 778–788. [Google Scholar] [CrossRef]
- Koyama, K.; Kato, T.; Yamauchi, J. The effect of ankle taping on the ground reaction force in vertical jump performance. J. Strength. Cond. Res. 2014, 28, 1411–1417. [Google Scholar] [CrossRef] [PubMed]
- Picot, B.; Hardy, A.; Terrier, R.; Tassignon, B.; Lopes, R.; Fourchet, F. Which Functional Tests and Self-Reported Questionnaires Can Help Clinicians Make Valid Return to Sport Decisions in Patients With Chronic Ankle Instability? A Narrative Review and Expert Opinion. Front. Sports Act. Living 2022, 4, 902886. [Google Scholar] [CrossRef] [PubMed]
- Legnani, C.; Del Re, M.; Peretti, G.M.; Macchi, V.; Borgo, E.; Ventura, A. Return to sport at the pre-injury level following anterior cruciate ligament reconstruction is influenced by patients’ perceived knee status and psychological readiness, and does not correlate with functional ability. J. ISAKOS 2025, 10, 100369. [Google Scholar] [CrossRef] [PubMed]
- Broman, D.; Piussi, R.; Thomeé, R.; Hamrin Senorski, E. A clinician-friendly test battery with a passing rate similar to a ‘gold standard’ return-to-sport test battery 1 year after ACL reconstruction: Results from a rehabilitation outcome registry. Phys. Ther. Sport 2023, 59, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Shankar, D.S.; Milton, H.A.; Mojica, E.S.; Buzin, S.; Strauss, E.J.; Campbell, K.A.; Alaia, M.J.; Gonzalez-Lomas, G.; Jazrawi, L.M. Force plate jump testing metrics are predictive of performance on a multimodal return to sport testing protocol among anterior cruciate ligament reconstruction patients at minimum six-month follow-up. J. Sports Med. Phys. Fit. 2023, 63, 1208–1217. [Google Scholar] [CrossRef]
- Zarro, M.J.; Stitzlein, M.G.; Lee, J.S.; Rowland, R.W.; Gray, V.L.; Taylor, J.B.; Meredith, S.J.; Packer, J.D.; Nelson, C.M. Single-Leg Vertical Hop Test Detects Greater Limb Asymmetries Than Horizontal Hop Tests After Anterior Cruciate Ligament Reconstruction in NCAA Division 1 Collegiate Athletes. Int. J. Sports Phys. Ther. 2021, 16, 1405–1414. [Google Scholar] [CrossRef]
- Augustsson, S.R.; Erik Sjöstedt, E. A test battery for evaluation of muscle strength, balance and functional performance in subjects with chronic ankle instability: A cross-sectional study. BMC Sports Sci. Med. Rehabil. 2023, 15, 55. [Google Scholar] [CrossRef]
- Park, Y.H.; Park, S.H.; Kim, S.H.; Choi, G.W.; Kim, H.J. Relationship between isokinetic muscle strength and functional tests in chronic ankle instability. J. Foot Ankle Surg. 2019, 58, 1187–1191. [Google Scholar] [CrossRef] [PubMed]
- Linens, S.W.; Ross, S.E.; Arnold, B.L.; Gayle, R.; Pidcoe, P. Postural-stability tests that identify individuals with chronic ankle instability. J. Athl. Train. 2014, 49, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Hiller, C.E.; Refshauge, K.M.; Herbert, R.D.; Kilbreath, S.L. Balance and recovery from a perturbation are impaired in people with functional ankle instability. Clin. J. Sport. Med. 2007, 17, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.; Zhang, T.; Yu, R.; Ganderton, C.; Adams, R.; Han, J. Effect of Different Landing Heights and Loads on Ankle Inversion Proprioception during Landing in Individuals with and without Chronic Ankle Instability. Bioengineering 2022, 9, 743. [Google Scholar] [CrossRef]
- Rosen, A.B.; Needle, A.R.; Ko, J. Ability of Functional Performance Tests to Identify Individuals With Chronic Ankle Instability: A Systematic Review With Meta-Analysis. Clin. J. Sport. Med. 2019, 29, 509–522. [Google Scholar] [CrossRef]
- Healy, A.; Linyard-Tough, K.; Chockalingam, N. Agreement Between the Spatiotemporal Gait Parameters of Healthy Adults From the OptoGait System and a Traditional Three-Dimensional Motion Capture System. J. Biomech. Eng. 2019, 141, 014501. [Google Scholar] [CrossRef]
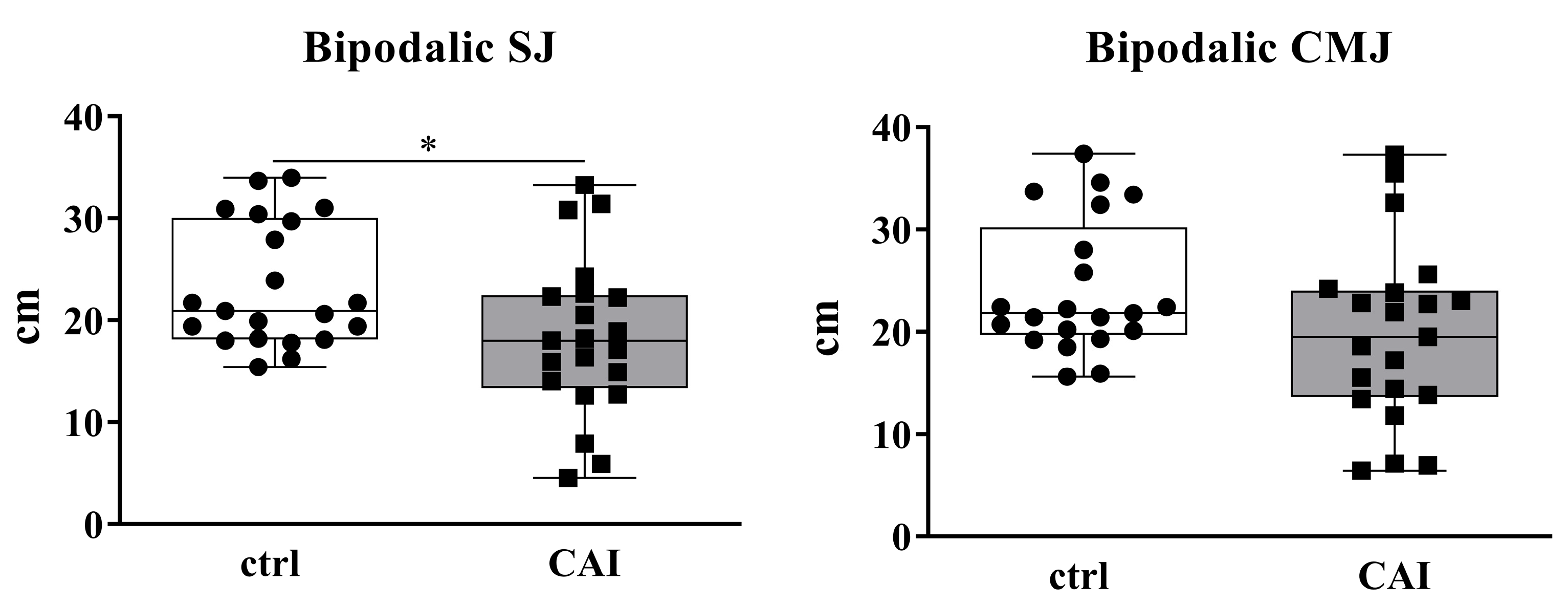

{kind=link}
{kind=link}
| CAI Patients | Control Group | p-Value | |
|---|---|---|---|
| No. of patients | 21 | 21 | |
| M:F ratio | 16:5 | 16:5 | >0.999 |
| Mean age at surgery ± SD (yr) | 33.1 ± 8.2 | 32.8 ± 7.6 | 0.945 |
| Mean BMI ± SD (kg/m2) | 23.0 ± 2.3 | 23.3 ± 2.7 | 0.916 |
| CAI Patients (n = 21) | Control Group (n = 21) | |||||||
|---|---|---|---|---|---|---|---|---|
| Uninjured Limb | Pathological Limb | p-Value | Dominant Limb | Non-Dominant Limb | p-Value | p-Value of Dominant Limb Control Group vs. Uninjured Limb CAI | p-Value of Non-Dominant Limb Control Group vs. Pathological Limb CAI | |
| Monopodalic CMJ (cm) | 9.59 ± 4.12 9.60 (7.00–12.30) | 8.31 ± 4.18 9.20 (5.40–10.40) | 0.327 | 12.50 ± 3.83 12.00 (10.05–16.05) | 11.95 ± 3.80 10.50 (8.65–15.80) | 0.644 | 0.023 | 0.005 |
| Monopodalic DJ (cm) | 11.08 ± 5.91 10.70 (8.75–14.95) | 9.28 ± 5.74 8.10 (4.35–13.60) | 0.157 | 13.86 ± 5.02 12.70 (9.70–17.95) | 12.90 ± 4.18 10.80 (10.20–16.30) | 0.504 | 0.247 | 0.025 |
| Monopodalic side-hop (cm) | 43.90 ± 17.30 41.00 (30.00–58.50) | 37.19 ± 19.37 33.00 (24.00–55.00) | 0.243 | 51.00 ± 18.01 49.00 (40.00–56.00) | 49.71 ± 19.30 43.00 (38.50–59.50) | 0.824 | 0.200 | 0.042 |
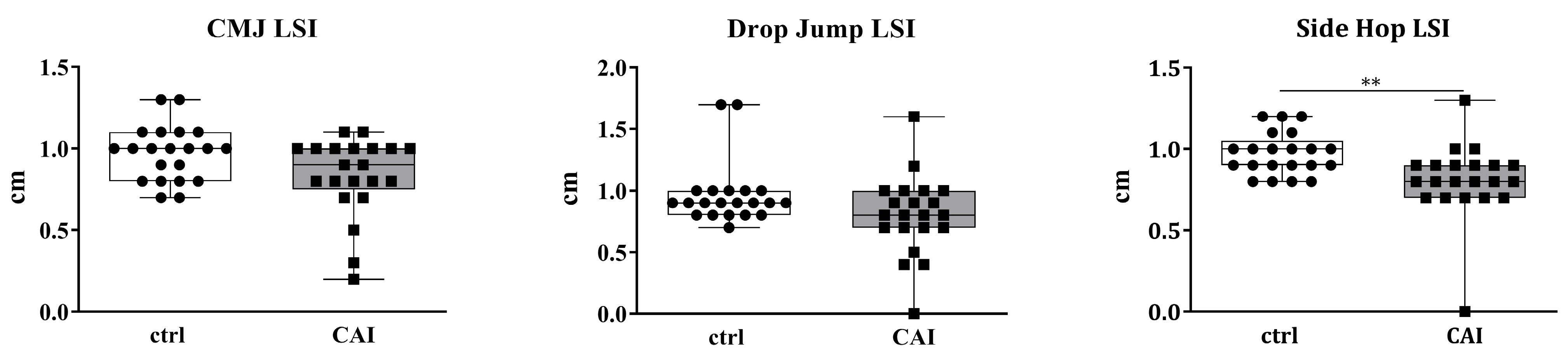
| CAI Patients (n = 21) | Control Group (n = 21) | p-Value | |
|---|---|---|---|
| CMJ LSI | 0.83 ± 0.24 0.90 (0.75–1.00) | 0.97 ± 0.17 1.00 (0.80–1.10) | 0.072 |
| DJ LSI | 0.80 ± 0.32 0.80 (0.70–1.00) | 0.97 ± 0.26 0.90 (0.80–1.00) | 0.071 |
| Side-hop LSI | 0.81 ± 0.23 0.80 (0.70–0.90) | 0.97 ± 0.13 1.00 (0.90–1.05) | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Legnani, C.; Saladini, M.; Faraldi, M.; Peretti, G.M.; Ventura, A. A Battery of Jump Tests Helps Discriminating Between Subjects With and Without Chronic Ankle Instability. Sports 2025, 13, 171. https://doi.org/10.3390/sports13060171
Legnani C, Saladini M, Faraldi M, Peretti GM, Ventura A. A Battery of Jump Tests Helps Discriminating Between Subjects With and Without Chronic Ankle Instability. Sports. 2025; 13(6):171. https://doi.org/10.3390/sports13060171
Chicago/Turabian StyleLegnani, Claudio, Matteo Saladini, Martina Faraldi, Giuseppe M. Peretti, and Alberto Ventura. 2025. "A Battery of Jump Tests Helps Discriminating Between Subjects With and Without Chronic Ankle Instability" Sports 13, no. 6: 171. https://doi.org/10.3390/sports13060171
APA StyleLegnani, C., Saladini, M., Faraldi, M., Peretti, G. M., & Ventura, A. (2025). A Battery of Jump Tests Helps Discriminating Between Subjects With and Without Chronic Ankle Instability. Sports, 13(6), 171. https://doi.org/10.3390/sports13060171