
Comparative Effects of Resistance Training Modalities on Mental Health and Quality of Life in Individuals with Spinal Cord Injury

 , ,
, ,  ,
,  ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
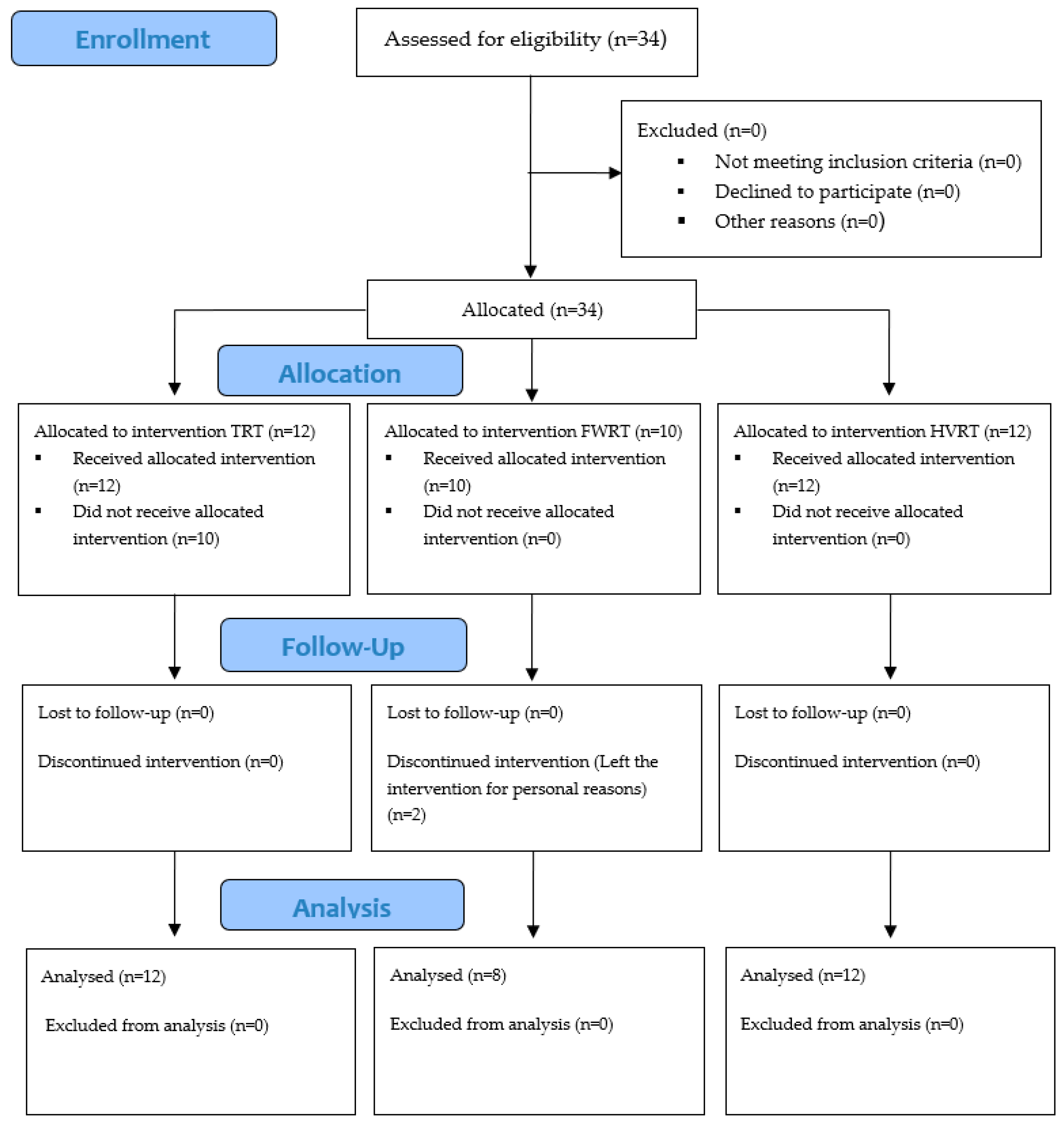
2.1. Experimental Approach to the Problem
2.2. Subjects
2.3. Procedures
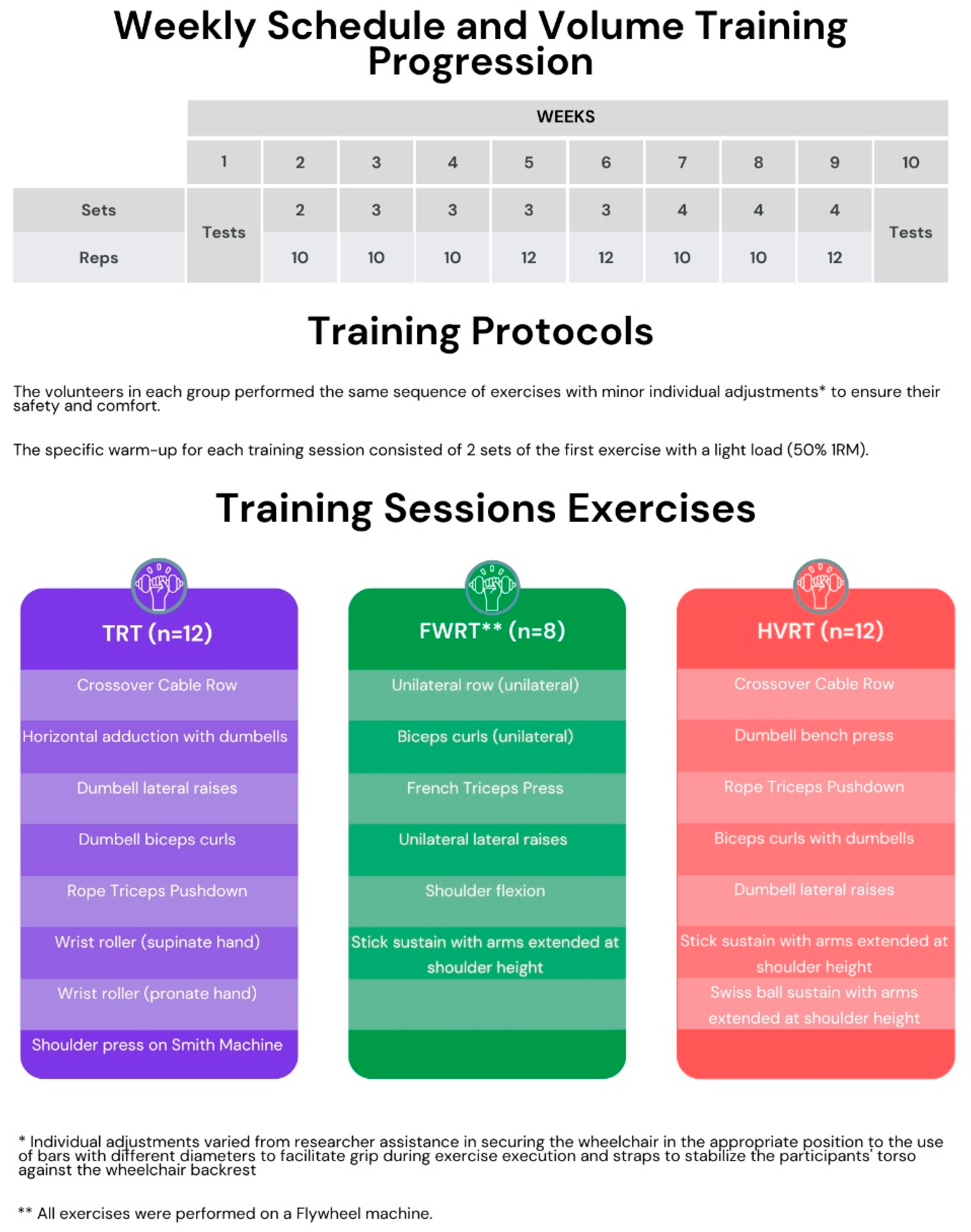
2.3.1. Training Protocols
2.3.2. Mental Health and Quality of Life Assessment
2.4. Statistics
3. Results
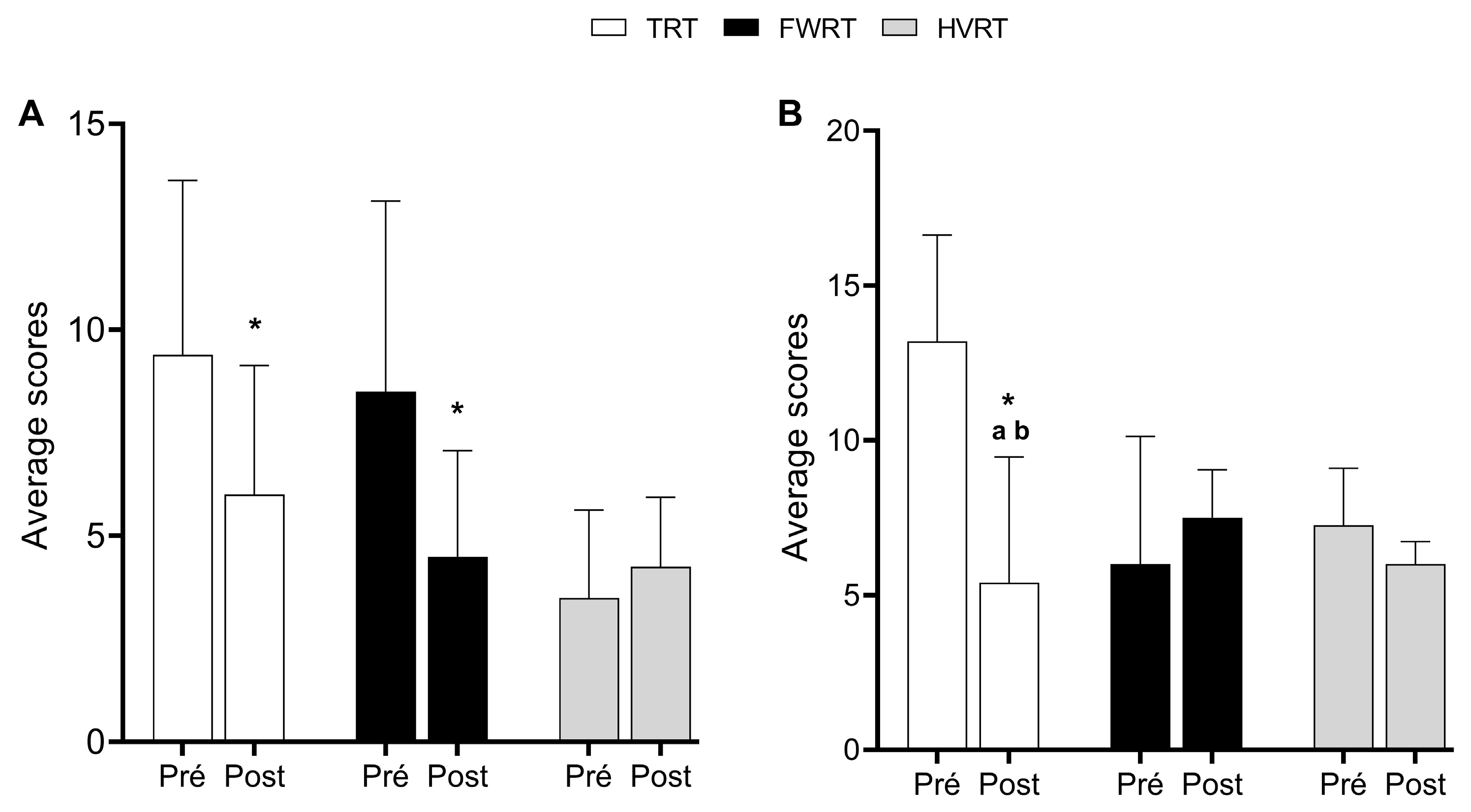
3.1. Mental Health
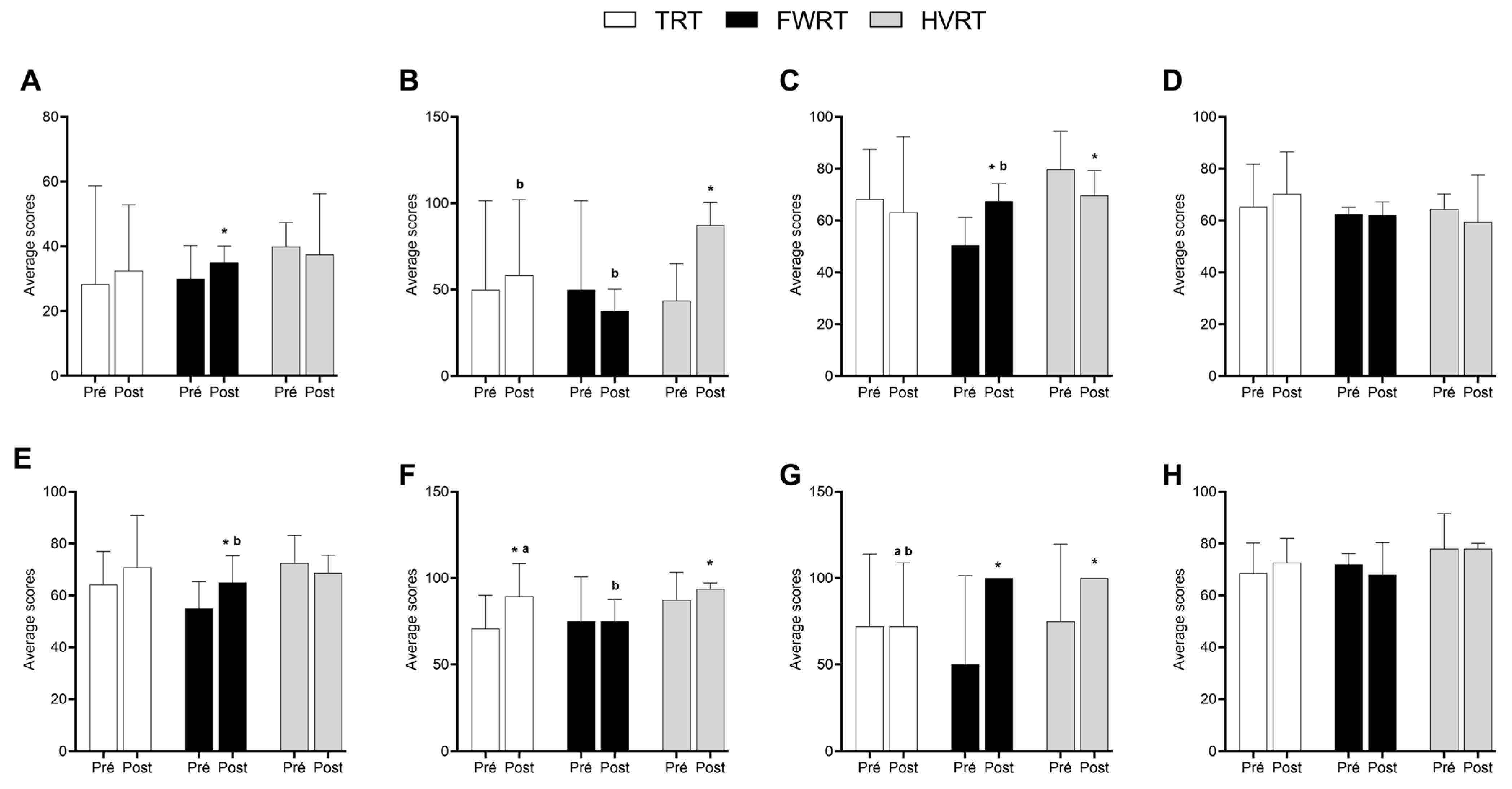
3.2. Quality of Life
4. Discussion
4.1. Mental Health
4.2. Quality of Life
4.3. Limitations and Strengths of This Study
4.4. Practical Applications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| FWRT | Flywheel Resistance Training |
| HVRT | High-Velocity Resistance Training |
| TRT | Traditional Resistance Training |
| HADS | Hospital Anxiety and Depression Scale |
| HADS-D | HADS Depression Score |
| HADS-A | HADS Anxiety Score |
References
- Cardile, D.; Calderone, A.; De Luca, R.; Corallo, F.; Quartarone, A.; Calabrò, R.S. The Quality of Life in Patients with Spinal Cord Injury: Assessment and Rehabilitation. J. Clin. Med. 2024, 13, 1820. [Google Scholar] [CrossRef]
- Leduc, B.E.; Lepage, Y. Health-related quality of life after spinal cord injury. Disabil. Rehabil. 2002, 24, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Lynch, J.; Cahalan, R. The impact of spinal cord injury on the quality of life of primary family caregivers: A literature review. Spinal Cord 2017, 55, 964–978. [Google Scholar] [CrossRef] [PubMed]
- Santos, L.V.; Pereira, E.T.; Suárez-Iglesias, D.; Ayán, C.; de Oliveira, C.E.P.; Moreira, O.C. Strength training as a non-pharmacological alternative to improve body composition and quality of life in people with spinal cord injury: A systematic review. J. Bodyw. Mov. Ther. 2024, 39, 285–292. [Google Scholar] [CrossRef]
- Anjum, A.; Yazid, M.D.I.; Fauzi Daud, M.; Idris, J.; Ng, A.M.H.; Selvi Naicker, A.; Lokanathan, Y. Spinal cord injury: Pathophysiology, multimolecular interactions, and underlying recovery mechanisms. Int. J. Mol. Sci. 2020, 21, 7533. [Google Scholar] [CrossRef]
- Hadjipavlou, G.; Cortese, A.M.; Ramaswamy, B. Spinal cord injury and chronic pain. BJA Educ. 2016, 16, 264–268. [Google Scholar] [CrossRef]
- Lee, W.; Jeong, S.; Lee, B.S.; Lim, J.C.; Kim, O. Association between functional outcomes and psychological variables in persons with spinal cord injury. Sci. Rep. 2023, 13, 23092. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Wang, H.; Deng, L.; Li, J. Exercise training promotes functional recovery after spinal cord injury. Neural Plast. 2016, 2016, 4039580. [Google Scholar] [CrossRef] [PubMed]
- Frontera, J.E.; Mollett, P. Aging with spinal cord injury: An update. Phys. Med. Rehabil. Clin. 2017, 28, 821–828. [Google Scholar] [CrossRef] [PubMed]
- Parker, M.A.; Ichikawa, J.K.; Bombardier, C.H.; Hammond, F.M. Association between anxiety symptoms, depression symptoms, and life satisfaction among individuals 1 year after spinal cord injury: Findings from the SCIRehab Project. Arch. Rehabil. Res. Clin. Transl. 2022, 4, 100211. [Google Scholar] [CrossRef]
- Hara, A.C.P.; Aching, N.C.; Marques, L.M.; Fregni, F.; Battisttella, L.R.; Simis, M. Clinical and demographic predictors of symptoms of depression and anxiety in patients with spinal cord injury. Spinal Cord 2022, 60, 1123–1129. [Google Scholar] [CrossRef] [PubMed]
- Khandelwal, A.; Shafer, L.A.; Ethans, K. Does severity of spinal cord injury predict likelihood of suffering chronically from severe depression and anxiety? Spinal Cord Ser. Cases 2022, 8, 58. [Google Scholar]
- Rodrigues, J.A.; Pereira, E.T.; de Oliveira, C.E.P.; Moreira, O.C. Effect of strength training on physical and mental health and quality of life of people with spinal cord injury: A literature review. Arch. Med. Deport. 2020, 37, 192–196. [Google Scholar]
- Rodrigues, J.A.; Pereira, E.T.; Lopes, J.S.; Teixeira, R.B.; da Silva, S.F.; Aidar, F.J.; Moreira, O.C. Effects of high-intensity and progressive volume resistance training on functional, mental states, and quality of life of people with spinal cord injury. Sport Sci. Health 2024, 20, 965–974. [Google Scholar] [CrossRef]
- Santos, L.V.; Pereira, E.T.; Reguera-García, M.M.; de Oliveira, C.E.P.; Moreira, O.C. Resistance Training and Muscle Strength in people with Spinal Cord Injury: A systematic review and meta-analysis. J. Bodyw. Mov. Ther. 2022, 29, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Deodato, M.; Granato, A.; Buoite Stella, A.; Martini, M.; Marchetti, E.; Lise, I.; Manganotti, P. Efficacy of a dual task protocol on neurophysiological and clinical outcomes in migraine: A randomized control trial. Neurol. Sci. 2024, 45, 4015–4026. [Google Scholar] [CrossRef] [PubMed]
- Da Silva Santos, R.; Galdino, G. Endogenous systems involved in exercise-induced analgesia. J. Physiol. Pharmacol. 2018, 69, 3–13. [Google Scholar]
- Maroto-Izquierdo, S.; García-López, D.; Fernandez-Gonzalo, R.; Moreira, O.C.; González-Gallego, J.; de Paz, J.A. Skeletal muscle functional and structural adaptations after eccentric overload flywheel resistance training: A systematic review and meta-analysis. J. Sci. Med. Sport 2017, 20, 943–951. [Google Scholar] [CrossRef]
- Suchomel, T.J.; Wagle, J.P.; Douglas, J.; Taber, C.B.; Harden, M.; Haff, G.G.; Stone, M.H. Implementing eccentric resistance training—Part 1: A brief review of existing methods. J. Funct. Morphol. Kinesiol. 2019, 4, 38. [Google Scholar] [CrossRef]
- Beato, M.; Dello Iacono, A. Implementing flywheel (isoinertial) exercise in strength training: Current evidence, practical recommendations, and future directions. Front. Physiol. 2020, 11, 569. [Google Scholar] [CrossRef] [PubMed]
- Stone, W.J.; Stevens, S.L.; Fuller, D.K.; Caputo, J.L. Strength and step activity after eccentric resistance training in those with incomplete spinal cord injuries. Top. Spinal Cord Inj. Rehabil. 2018, 24, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Feter, N.; Schaun, G.Z.; Smith, E.C.; Cassuriaga, J.; Alt, R.; Redig, L.; Rombaldi, A.J. High-velocity resistance training improves executive function in mobility-limited older adults. Arch. Gerontol. Geriatr. 2023, 114, 105081. [Google Scholar] [CrossRef] [PubMed]
- Lopez, P.; Rech, A.; Petropoulou, M.; Newton, R.U.; Taaffe, D.R.; Galvão, D.A.; Radaelli, R. Does high-velocity resistance exercise elicit greater physical function benefits than traditional resistance exercise in older adults? A systematic review and network meta-analysis of 79 trials. J. Gerontol. Ser. A 2023, 78, 1471–1482. [Google Scholar] [CrossRef] [PubMed]
- Botega, N.J.; Bio, M.R.; Zomignani, M.A.; Garcia Jr, C.; Pereira, W.A. Mood disorders among medical in-patients: A validation study of the hospital anxiety and depression scale (HAD). Rev. Saúde Pública 1995, 29, 359–363. [Google Scholar] [CrossRef]
- Aidar, F.J.; de Oliveira, R.J.; de Matos, D.G.; Mazini Filho, M.L.; Moreira, O.C.; de Oliveira, C.E.P.; Reis, V.M. A randomized trial investigating the influence of strength training on quality of life in ischemic stroke. Top. Stroke Rehabil. 2016, 23, 84–89. [Google Scholar] [CrossRef]
- Gordon, B.R.; McDowell, C.P.; Lyons, M.; Herring, M.P. The effects of resistance exercise training on anxiety: A meta-analysis and meta-regression analysis of randomized controlled trials. Sports Med. 2017, 47, 2521–2532. [Google Scholar] [CrossRef] [PubMed]
- Gordon, B.R.; McDowell, C.P.; Hallgren, M.; Meyer, J.D.; Lyons, M.; Herring, M.P. Association of efficacy of resistance exercise training with depressive symptoms: Meta-analysis and meta-regression analysis of randomized clinical trials. JAMA Psychiatry 2018, 75, 566–576. [Google Scholar] [CrossRef]
- Henriksson, M.; Wall, A.; Nyberg, J.; Adiels, M.; Lundin, K.; Bergh, Y.; Åberg, M. Effects of exercise on symptoms of anxiety in primary care patients: A randomized controlled trial. J. Affect. Disord. 2022, 297, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Bonanno, G.A.; Kennedy, P.; Galatzer-Levy, I.R.; Lude, P.; Elfström, M.L. Trajectories of resilience, depression, and anxiety following spinal cord injury. Rehabil. Psychol. 2012, 57, 236. [Google Scholar] [CrossRef]
- Kennedy, P.; Rogers, B.A. Anxiety and depression after spinal cord injury: A longitudinal analysis. Arch. Phys. Med. Rehabil. 2000, 81, 932–937. [Google Scholar] [CrossRef]
- Lim, S.W.; Shiue, Y.L.; Ho, C.H.; Yu, S.C.; Kao, P.H.; Wang, J.J.; Kuo, J.R. Anxiety and depression in patients with traumatic spinal cord injury: A nationwide population-based cohort study. PLoS ONE 2017, 12, e0169623. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Lan, W.; Yang, G.; Li, Y.; Ji, X.; Chen, L.; Li, S. Exercise intervention in treatment of neuropsychological diseases: A review. Front. Psychol. 2020, 11, 569206. [Google Scholar] [CrossRef] [PubMed]
- Mason, O.J.; Holt, R. Mental health and physical activity interventions: A review of the qualitative literature. J. Ment. Health 2012, 21, 274–284. [Google Scholar] [CrossRef]
- Dionigi, R. Resistance training and older adults’ beliefs about psychological benefits: The importance of self-efficacy and social interaction. J. Sport Exerc. Psychol. 2007, 29, 723–746. [Google Scholar] [CrossRef] [PubMed]
- Pettigrew, S.; Burton, E.; Farrier, K.; Hill, A.M.; Bainbridge, L.; Airey, P.; Hill, K.D. Encouraging older people to engage in resistance training: A multi-stakeholder perspective. Ageing Soc. 2019, 39, 1806–1825. [Google Scholar] [CrossRef]
- Rhodes, R.E.; Lubans, D.R.; Karunamuni, N.; Kennedy, S.; Plotnikoff, R. Factors associated with participation in resistance training: A systematic review. Br. J. Sports Med. 2017, 51, 1466–1472. [Google Scholar] [CrossRef]
- Raya-González, J.; de Keijzer, K.L.; Bishop, C.; Beato, M. Effects of flywheel training on strength-related variables in female populations: A systematic review. Res. Sports Med. 2022, 30, 353–370. [Google Scholar] [CrossRef] [PubMed]
- Sañudo, B.; de Hoyo, M.; McVeigh, J.G. Improved muscle strength, muscle power, and physical function after flywheel resistance training in healthy older adults: A randomized controlled trial. J. Strength Cond. Res. 2022, 36, 252–258. [Google Scholar] [CrossRef]
- Ramírez-Campillo, R.; Castillo, A.; de la Fuente, C.I.; Campos-Jara, C.; Andrade, D.C.; Álvarez, C.; Izquierdo, M. High-speed resistance training is more effective than low-speed resistance training to increase functional capacity and muscle performance in older women. Exp. Gerontol. 2014, 58, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Ramirez-Campillo, R.; Alvarez, C.; Garcìa-Hermoso, A.; Celis-Morales, C.; Ramirez-Velez, R.; Gentil, P.; Izquierdo, M. High-speed resistance training in elderly women: Effects of cluster training sets on functional performance and quality of life. Exp. Gerontol. 2018, 110, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Rivers, C.S.; Fallah, N.; Noonan, V.K.; Whitehurst, D.G.; Schwartz, C.E.; Finkelstein, J.A.; Noreau, L. Health conditions: Effect on function, health-related quality of life, and life satisfaction after traumatic spinal cord injury. A prospective observational registry cohort study. Arch. Phys. Med. Rehabil. 2018, 99, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Ditor, D.S.; Latimer, A.E.; Martin Ginis, K.A.; Arbour, K.P.; McCartney, N.; Hicks, A.L. Maintenance of exercise participation in individuals with spinal cord injury: Effects on quality of life, stress, and pain. Spinal Cord 2003, 41, 446–450. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos, L.V.; Freitas, K.R.d.S.R.; Pereira, E.T.; Leite, L.B.; Forte, P.; de Oliveira, C.E.P.; Moreira, O.C. Comparative Effects of Resistance Training Modalities on Mental Health and Quality of Life in Individuals with Spinal Cord Injury. Sports 2025, 13, 60. https://doi.org/10.3390/sports13020060
Santos LV, Freitas KRdSR, Pereira ET, Leite LB, Forte P, de Oliveira CEP, Moreira OC. Comparative Effects of Resistance Training Modalities on Mental Health and Quality of Life in Individuals with Spinal Cord Injury. Sports. 2025; 13(2):60. https://doi.org/10.3390/sports13020060
Chicago/Turabian StyleSantos, Lucas Vieira, Karla Raphaela da Silva Ramos Freitas, Eveline Torres Pereira, Luciano Bernardes Leite, Pedro Forte, Claudia Eliza Patrocínio de Oliveira, and Osvaldo Costa Moreira. 2025. "Comparative Effects of Resistance Training Modalities on Mental Health and Quality of Life in Individuals with Spinal Cord Injury" Sports 13, no. 2: 60. https://doi.org/10.3390/sports13020060
APA StyleSantos, L. V., Freitas, K. R. d. S. R., Pereira, E. T., Leite, L. B., Forte, P., de Oliveira, C. E. P., & Moreira, O. C. (2025). Comparative Effects of Resistance Training Modalities on Mental Health and Quality of Life in Individuals with Spinal Cord Injury. Sports, 13(2), 60. https://doi.org/10.3390/sports13020060