
Validity and Inter-Device Reliability of the OTBeat BurnTM Monitor to Estimate Heart Rate During Exercise



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Exercise Protocol
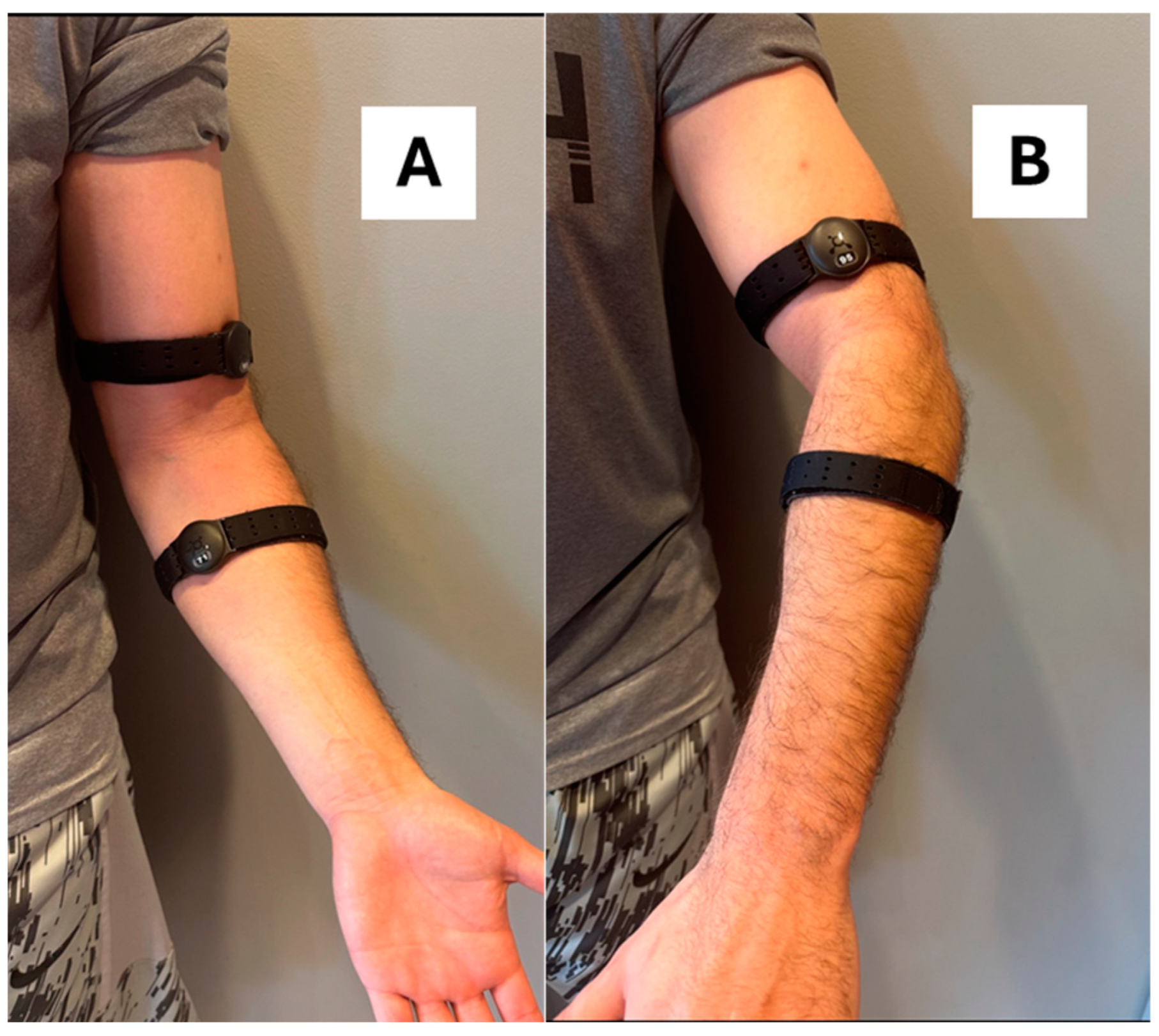
2.3. Measurement of the Heart Rate
2.4. Data Analyses
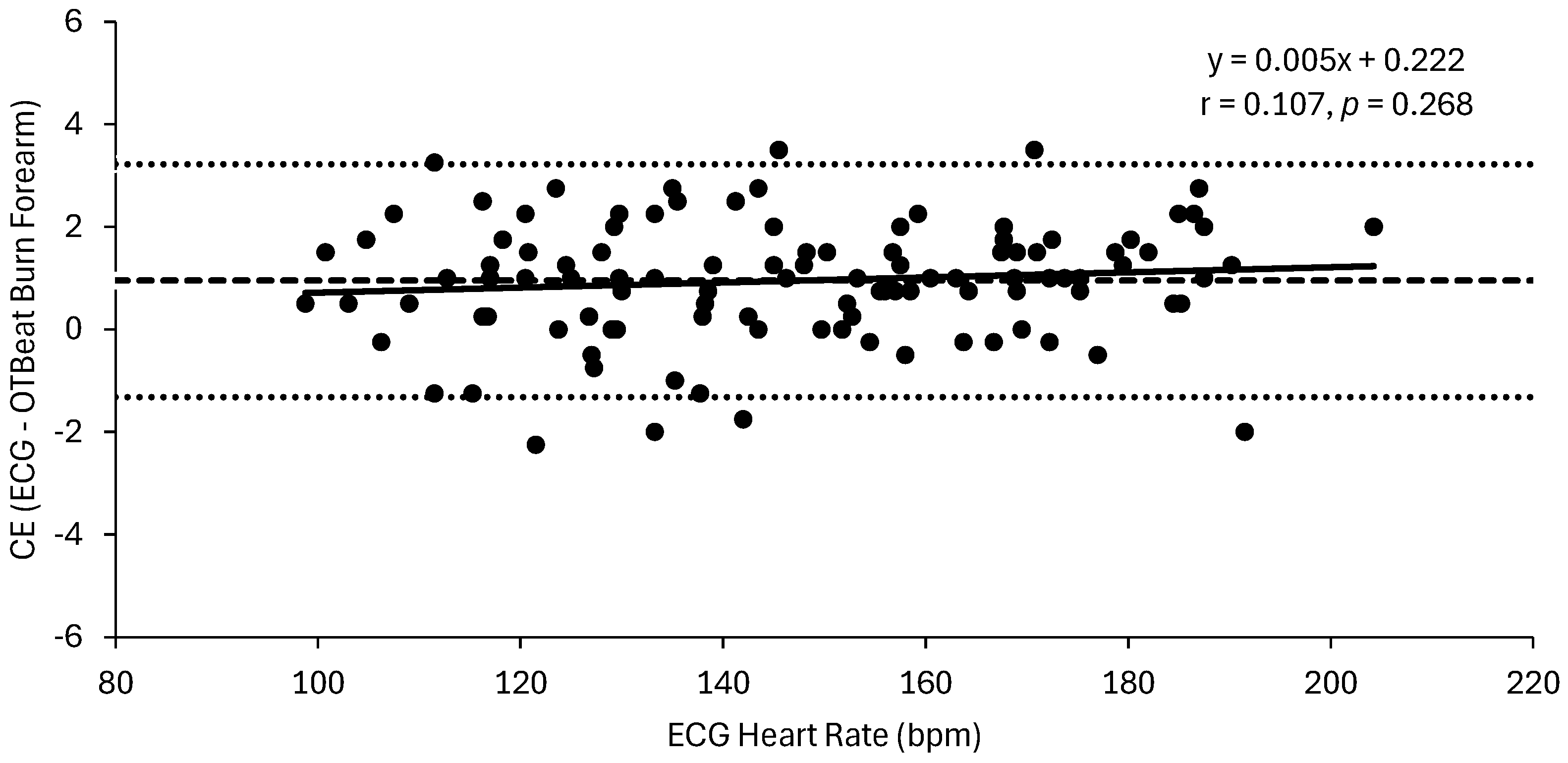
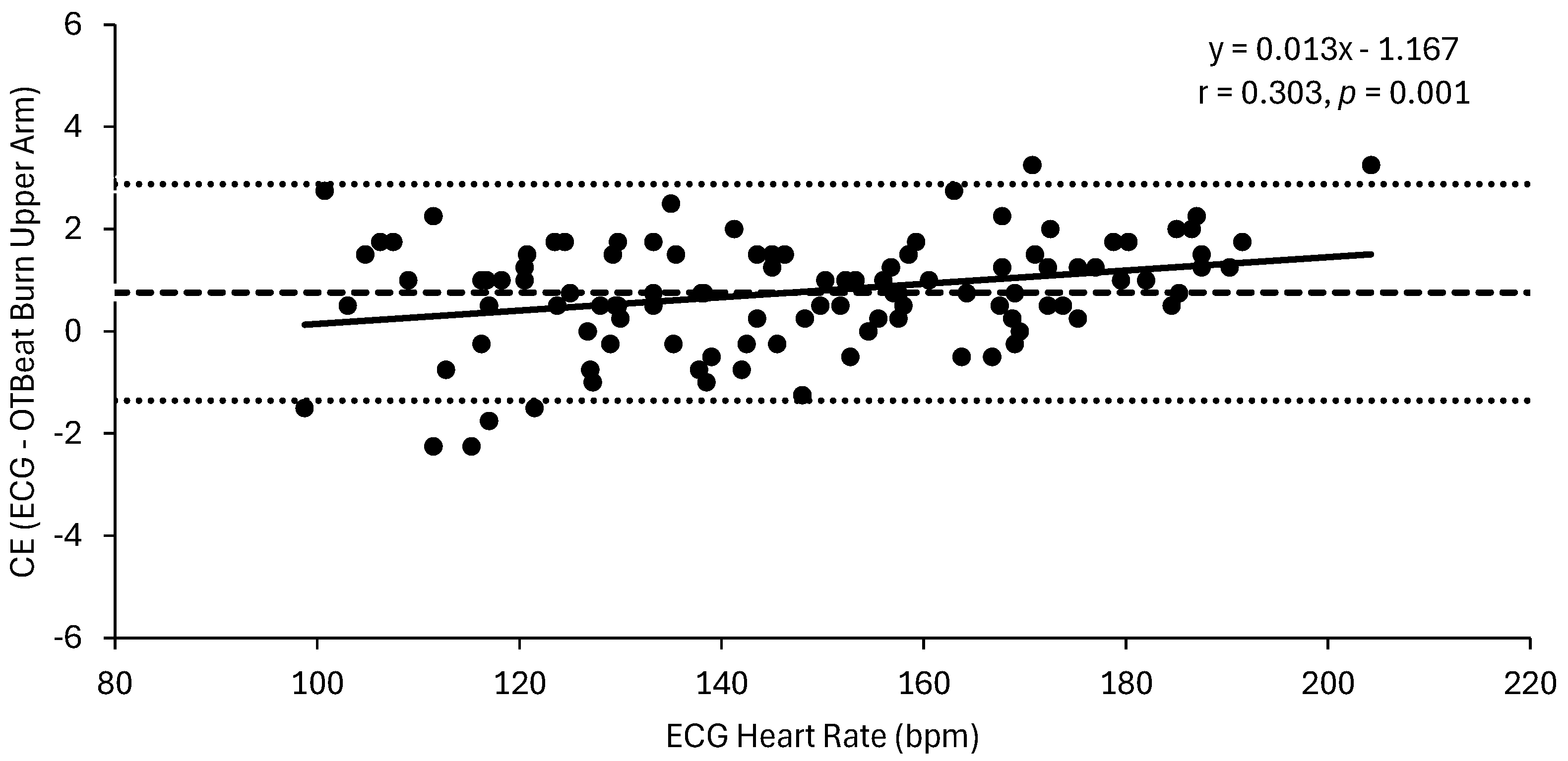
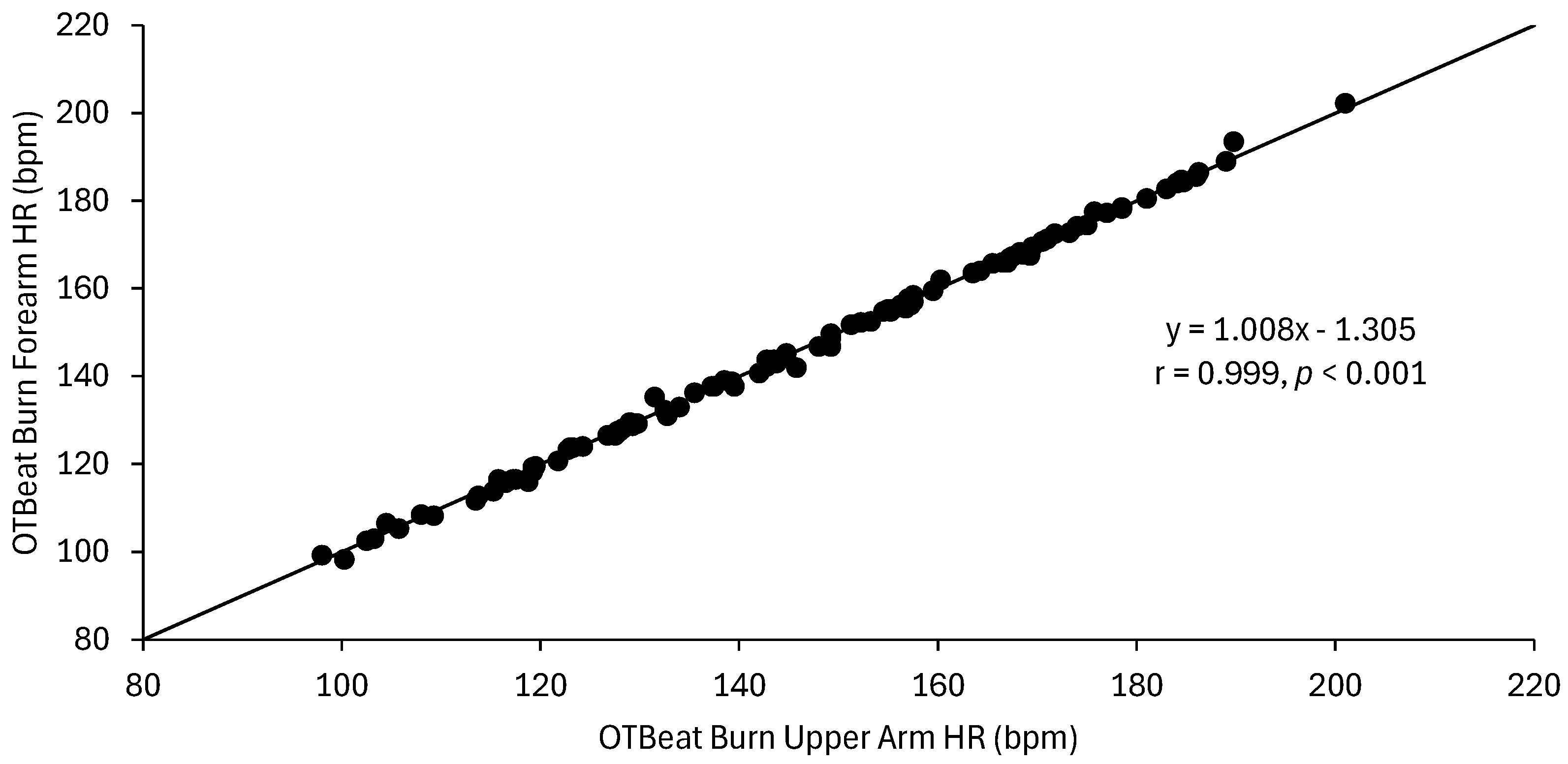
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MAPE | Mean absolute percent error |
| CCC | Lin’s concordance correlation coefficient |
| ECG | Electrocardiogram |
| ICC | Intraclass correlation coefficient |
| PPG | Photoplethysmography |
| CE | Constant error |
| AE | Absolute error |
| APE | Absolute percent error |
| SEE | Standard error of estimate |
References
- Newsome, A.M.; Batrakoulis, A.; Camhi, S.M.; Sansone, J. 2025 ACSM Worldwide Fitness Trends: Future Directions of the Health and Fitness Industry. ACSMs Health Fit. J. 2024, 28, 11–25. [Google Scholar] [CrossRef]
- Newsome, A.M.; Sansone, J.; McAvoy, C. 2024 Worldwide Fitness Trends: Future Directions of the Health and Fitness Industry. ACSMs Health Fit. J. 2023, 28, 14–26. [Google Scholar] [CrossRef]
- Thompson, W.R. Worldwide survey of fitness trends for 2023. ACSMs Health Fit. J. 2022, 27, 9–18. [Google Scholar] [CrossRef]
- Thompson, W.R. Worldwide survey of fitness trends for 2022. ACSMs Health Fit. J. 2021, 26, 11–20. [Google Scholar] [CrossRef]
- El-Amrawy, F.; Nounou, M.I. Are currently available wearable devices for activity tracking and heart rate monitoring accurate, precise, and medically beneficial? Health Inform. Res. 2015, 21, 315–320. [Google Scholar] [CrossRef]
- Gillinov, S.; Etiwy, M.; Wang, R.; Blackburn, G.; Phelan, D.; Gillinov, A.M.; Houghtaling, P.; Javadikasgari, H.; Desai, M.Y. Variable accuracy of wearable heart rate monitors during aerobic exercise. Med. Sci. Sports Exerc. 2017, 49, 1697–1703. [Google Scholar] [CrossRef] [PubMed]
- Alugubelli, N.; Abuissa, H.; Roka, A. Wearable devices for remote monitoring of heart rate and heart rate variability-what we know and what is coming. Sensors 2022, 22, 8903. [Google Scholar] [CrossRef]
- Etiwy, M.; Akhrass, Z.; Gillinov, L.; Alashi, A.; Wang, R.; Blackburn, G.; Gillinov, S.M.; Phelan, D.; Gillinov, A.M.; Houghtaling, P.L.; et al. Accuracy of wearable heart rate monitors in cardiac rehabilitation. Cardiovasc. Diagn. Ther. 2019, 9, 262–271. [Google Scholar] [CrossRef]
- Shin, G.; Jarrahi, M.H.; Fei, Y.; Karami, A.; Gafinowitz, N.; Byun, A.; Lu, X. Wearable activity trackers, accuracy, adoption, acceptance and health impact: A systematic review. J. Biomed. Inform. 2019, 93, 103153. [Google Scholar] [CrossRef]
- Wang, R.; Blackburn, G.; Desai, M.; Phelan, D.; Gillinov, L.; Houghtaling, P.; Gillinov, M. Accuracy of wrist-worn heart rate monitors. JAMA Cardiol. 2016, 2, 104–106. [Google Scholar] [CrossRef] [PubMed]
- Hettiarachchi, I.T.; Hanoun, S.; Nahavandi, D.; Navahandi, S. Validation of Polar OH1 optical heart rate sensor for moderate and high intensity physical activities. PLoS ONE 2019, 14, e0217288. [Google Scholar] [CrossRef]
- Navalta, J.W.; Montes, J.; Bodell, N.G.; Salatto, R.W.; Manning, J.W.; DeBeliso, M. Concurrent heart rate validity of wearable technology devices during trail running. PLoS ONE 2020, 15, e0238569. [Google Scholar] [CrossRef] [PubMed]
- Thiebaud, R.S.; Funk, M.D.; Patton, J.C.; Massey, B.L.; Shay, T.E.; Schmidt, M.G.; Giovannitti, N. Validity of wrist-worn consumer products to measure heart rate and energy expenditure. Digit. Health 2018, 4, 2055207618770322. [Google Scholar] [CrossRef] [PubMed]
- Jachymek, M.; Jachymek, M.T.; Kiedrowicz, R.M.; Kaźmierczak, J.; Płońska-Gościniak, E.; Peregud-Pogorzelska, M. Wristbands in home-based rehabilitation-validation of heart rate measurement. Sensors 2021, 22, 60. [Google Scholar] [CrossRef]
- Jagim, A.R.; Koch-Gallup, N.; Camic, C.L.; Kroening, L.; Nolte, C.; Schroeder, C.; Gran, L.; Erickson, J.L. The accuracy of fitness watches for the measurement of heart rate and energy expenditure during moderate intensity exercise. J. Sports Med. Phys. Fitness 2021, 61, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Jo, E.; Lewis, K.; Directo, D.; Kim, M.J.; Dolezal, B.A. Validation of biofeedback wearables for photoplethysmographic heart rate tracking. J. Sports Sci. Med. 2016, 15, 540–547. [Google Scholar] [PubMed]
- Shumate, T.; Link, M.; Furness, J.; Kemp-Smith, K.; Simas, V.; Climstein, M. Validity of the Polar Vantage M watch when measuring heart rate at different exercise intensities. Peer J. 2021, 9, e10893. [Google Scholar] [CrossRef] [PubMed]
- Montalvo, S.; Martinez, A.; Arias, S.; Lozano, A.; Gonzalez, M.P.; Dietze-Hermosa, M.S.; Boyea, B.; Dorgo, S. Smartwatches and commercial heart rate monitors: A concurrent validity analysis. J. Strength. Cond. Res. 2023, 37, 1802–1808. [Google Scholar] [CrossRef] [PubMed]
- Reece, J.D.; Bunn, J.A.; Choi, M.; Navalta, J.W. Assessing heart rate using consumer technology association standards. Technologies 2021, 9, 46. [Google Scholar] [CrossRef]
- Orangetheory.com. Available online: https://www.orangetheory.com/en-us/international-opportunities (accessed on 1 December 2024).
- Orangetheory.com. Available online: https://www.orangetheory.com/files/otbeat/user-guide.pdf (accessed on 1 December 2024).
- Moraes, J.L.; Rocha, M.X.; Vasconcelos, G.G.; Vasconcelos Filho, J.E.; de Albuquerque, V.H.C.; Alexandria, A.R. Advances in photoplethysmography signal analysis for biomedical applications. Sensors 2018, 18, 1894. [Google Scholar] [CrossRef] [PubMed]
- Estepp, J.R.; Blackford, E.B.; Meier, C.M. Recovering pulse rate during motion artifact with a multi-imager array for non-contact imaging photoplethysmography. In Proceedings of the 2014 IEEE International Conference on Systems, Man and Cybernetics—SMC, San Diego, CA, USA, 5–8 October 2014; pp. 1462–1469. [Google Scholar]
- Mühlen, J.M.; Stang, J.; Lykke Skovgaard, E.; Judice, P.B.; Molina-Garcia, P.; Johnston, W.; Sardinha, L.B.; Ortega, F.B.; Caulfield, B.; Bloch, W.; et al. Recommendations for determining the validity of consumer wearable heart rate devices: Expert statement and checklist of the INTERLIVE Network. Br. J. Sports Med. 2021, 55, 767–779. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Wang, Z.; Zhang, W.; Kong, W.; Jiang, J.; Zhao, R.; Wang, D.; Feng, L.; Ni, G. Estimation of heart rate and energy expenditure using smart bracelet during different exercise intensities: A reliability and validity study. Sensors 2022, 22, 4661. [Google Scholar] [CrossRef] [PubMed]
- Ceugniez, M.; Devanne, H.; Hermand, E. Reliability and accuracy of the Fitbit charge 4 photoplethysmography heart rate sensor in ecological conditions: Validation study. JMIR Mhealth Uhealth 2025, 13, e54871. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Vicente, A.; Hernando, D.; Marín-Puyalto, J.; Vicente-Rodríguez, G.; Garatachea, N.; Pueyo, E.; Bailón, R. Validity of the Polar H7 heart rate sensor for heart rate variability analysis during exercise in different age, body composition and fitness level groups. Sensors 2021, 21, 902. [Google Scholar] [CrossRef] [PubMed]
- Muggeridge, D.J.; Hickson, K.; Davies, A.V.; Giggins, O.M.; Megson, I.L.; Gorely, T.; Crabtree, D.R. Measurement of heart rate using the Polar OH1 and Fitbit Charge 3 wearable devices in healthy adults during light, moderate, vigorous, and sprint-based exercise: Validation study. JMIR Mhealth Uhealth 2021, 9, e25313. [Google Scholar] [CrossRef]
- Navalta, J.W.; Davis, D.W.; Malek, E.M.; Carrier, B.; Bodell, N.G.; Manning, J.W.; Cowley, J.; Funk, M.; Lawrence, M.M.; DeBeliso, M. Heart rate processing algorithms and exercise duration on reliability and validity decisions in biceps-worn Polar Verity Sense and OH1 wearables. Sci. Rep. 2023, 13, 11736. [Google Scholar] [CrossRef] [PubMed]
- Neudorfer, M.; Kumar, D.; Smeddinck, J.D.; Kulnik, S.T.; Niebauer, J.; Treff, G.; Sareban, M. Validity of four consumer-grade optical heart rate sensors for assessing volume and intensity distribution of physical activity. Scand. J. Med. Sci. Sports 2024, 34, e14756. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W.G. Validity thresholds and error rates for test measures used to assess individuals. In Proceedings of the 21st Annual Congress of the European College of Sport Science, Vienna, Austria, 6–9 July 2016. [Google Scholar]
- Hajj-Boutros, G.; Landry-Duval, M.A.; Comtois, A.S.; Gouspillou, G.; Karelis, A.D. Wrist-worn devices for the measurement of heart rate and energy expenditure: A validation study for the Apple Watch 6, Polar Vantage V, and Fitbit Sense. Eur. J. Sport. Sci. 2023, 23, 165–177. [Google Scholar] [CrossRef]
- Hermand, E.; Cassirame, J.; Ennequin, G.; Hue, O. Validation of a photoplethysmographic heart rate monitor: Polar OH1. Int. J. Sports Med. 2019, 40, 462–467. [Google Scholar] [CrossRef]
- Navalta, J.W.; Carrier, B.; Blank, M.; Zarei, S.; Davis, D.W.; Craig, M.; Perez, O.R.; Baca, J.; Sweder, T.S.; Carballo, T.; et al. Validity and reliability of wearable technology devices during simulated pickleball game play. Sports 2024, 12, 234. [Google Scholar] [CrossRef]
- Stahl, S.E.; An, H.S.; Dinkel, D.M.; Noble, J.M.; Lee, J.M. How accurate are the wrist-based heart rate monitors during walking and running activities? Are they accurate enough? BMJ Open Sport. Exerc. Med. 2016, 2, e000106. [Google Scholar] [CrossRef] [PubMed]
- Hermans, F.; Arents, E.; Blondeel, A.; Janssens, W.; Cardinaels, N.; Calders, P.; Troosters, T.; Derom, E.; Demeyer, H. Validity of a consumer-based wearable to measure clinical parameters in patients with chronic obstructive pulmonary disease and healthy controls: Observational study. JMIR Mhealth Uhealth 2024, 12, e56027. [Google Scholar] [CrossRef]
- Abt, G.; Bray, J.; Benson, A.C. The validity and inter-device variability of the Apple Watch™ for measuring maximal heart rate. J. Sports Sci. 2017, 36, 1447–1452. [Google Scholar] [CrossRef] [PubMed]
- Climstein, M.; Alder, J.L.; Brooker, A.M.; Cartwright, E.J.; Kemp-Smith, K.; Simas, V.; Furness, J. Reliability of the Polar Vantage M sports watch when measuring heart rate at different treadmill exercise intensities. Sports 2020, 8, 117. [Google Scholar] [CrossRef]
- Khushhal, A.; Nichols, S.; Evans, W.; Gleadall-Siddall, D.O.; Page, R.; O’Doherty, A.F.; Carroll, S.; Ingle, L.; Abt, G. Validity and reliability of the Apple Watch for measuring heart rate during exercise. Sports Med. Int. Open 2017, 1, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Paradiso, C.; Colino, F.; Liu, S. The validity and reliability of the Mi band wearable device for measuring steps and heart rate. Int. J. Exerc. Sci. 2020, 13, 689–701. [Google Scholar] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Leon, M.F.; Camic, C.L.; Herring, M.J.; Hill, C.M. Validity and Inter-Device Reliability of the OTBeat BurnTM Monitor to Estimate Heart Rate During Exercise. Sports 2025, 13, 49. https://doi.org/10.3390/sports13020049
de Leon MF, Camic CL, Herring MJ, Hill CM. Validity and Inter-Device Reliability of the OTBeat BurnTM Monitor to Estimate Heart Rate During Exercise. Sports. 2025; 13(2):49. https://doi.org/10.3390/sports13020049
Chicago/Turabian Stylede Leon, Matteo F., Clayton L. Camic, Matthew J. Herring, and Christopher M. Hill. 2025. "Validity and Inter-Device Reliability of the OTBeat BurnTM Monitor to Estimate Heart Rate During Exercise" Sports 13, no. 2: 49. https://doi.org/10.3390/sports13020049
APA Stylede Leon, M. F., Camic, C. L., Herring, M. J., & Hill, C. M. (2025). Validity and Inter-Device Reliability of the OTBeat BurnTM Monitor to Estimate Heart Rate During Exercise. Sports, 13(2), 49. https://doi.org/10.3390/sports13020049