
Effects of Ischemic Preconditioning on Sport-Specific Performance in Highly Trained Taekwondo Athletes

 , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
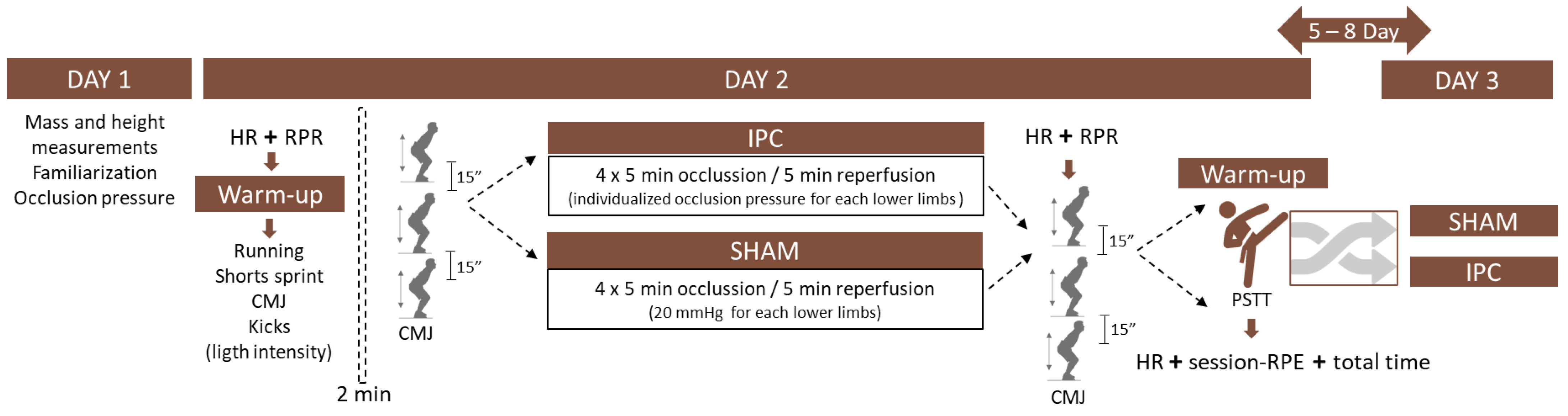
2.1. Study 1
2.1.1. Participants
2.1.2. Study Design
2.1.3. Procedures
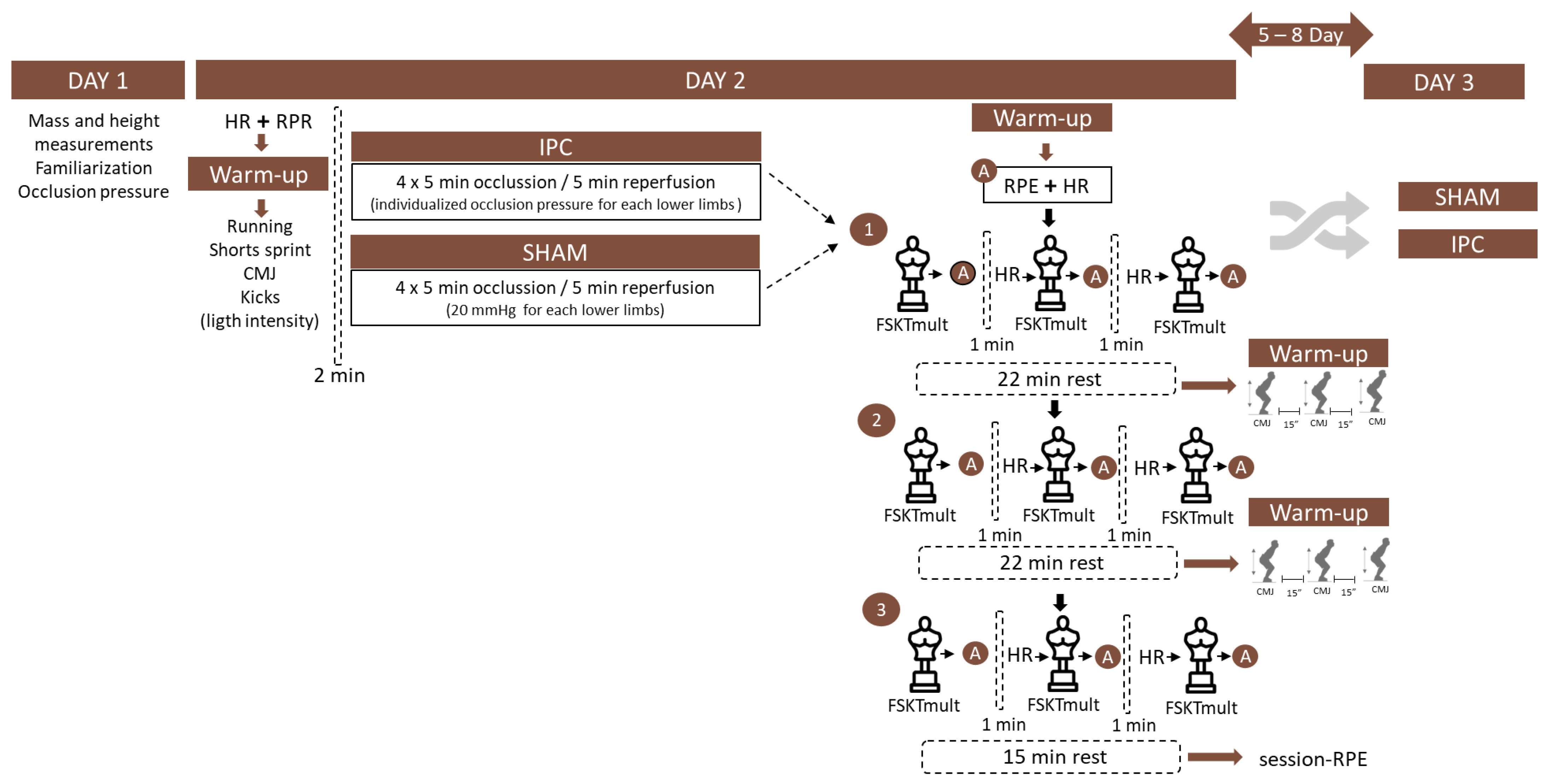
2.2. Study 2
2.2.1. Participants
2.2.2. Study Design
2.2.3. Procedures
2.2.4. Statistical Analysis
3. Results
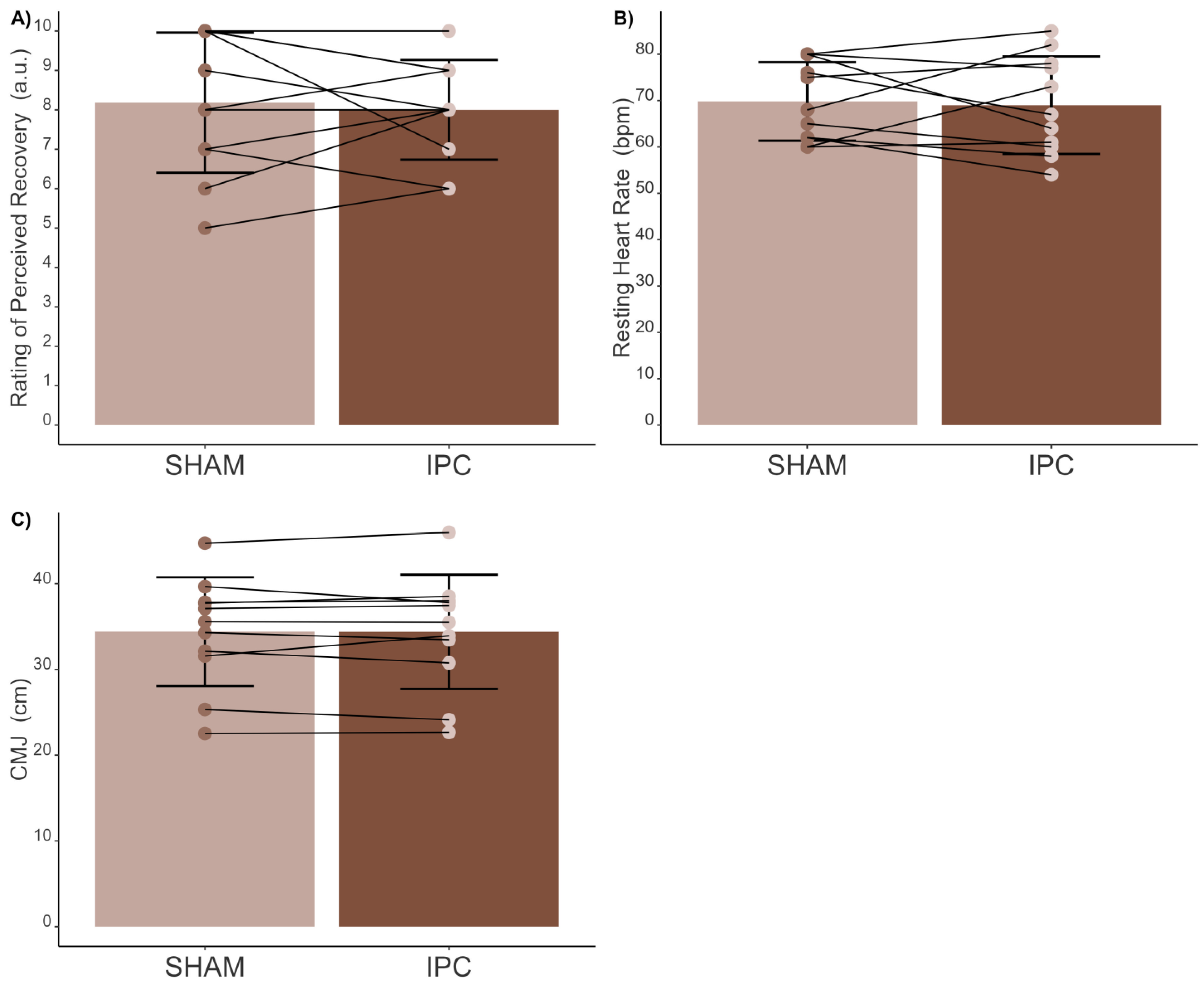
3.1. Study 1
3.1.1. Pre-Intervention
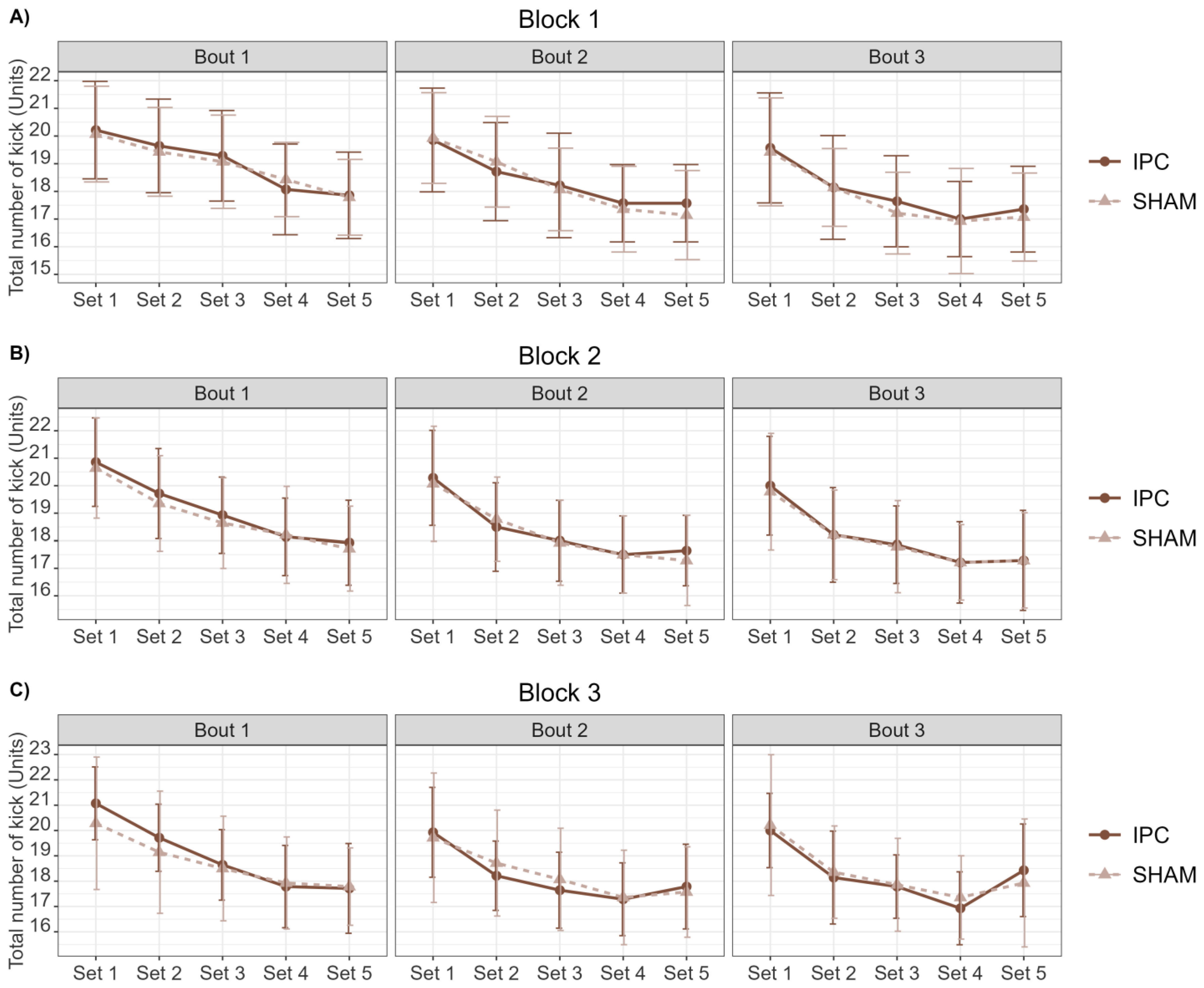
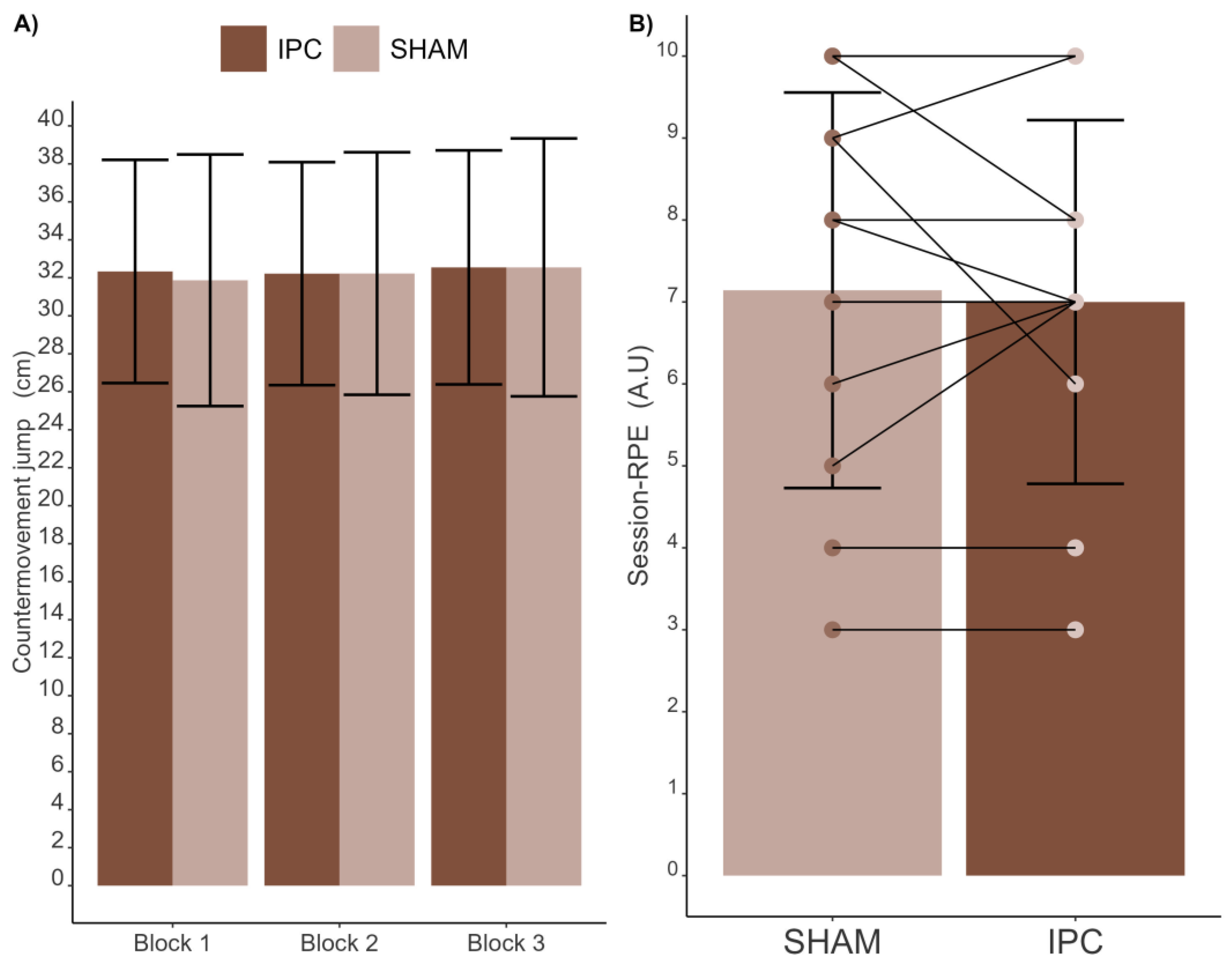
3.1.2. Intervention
3.1.3. Post-Intervention
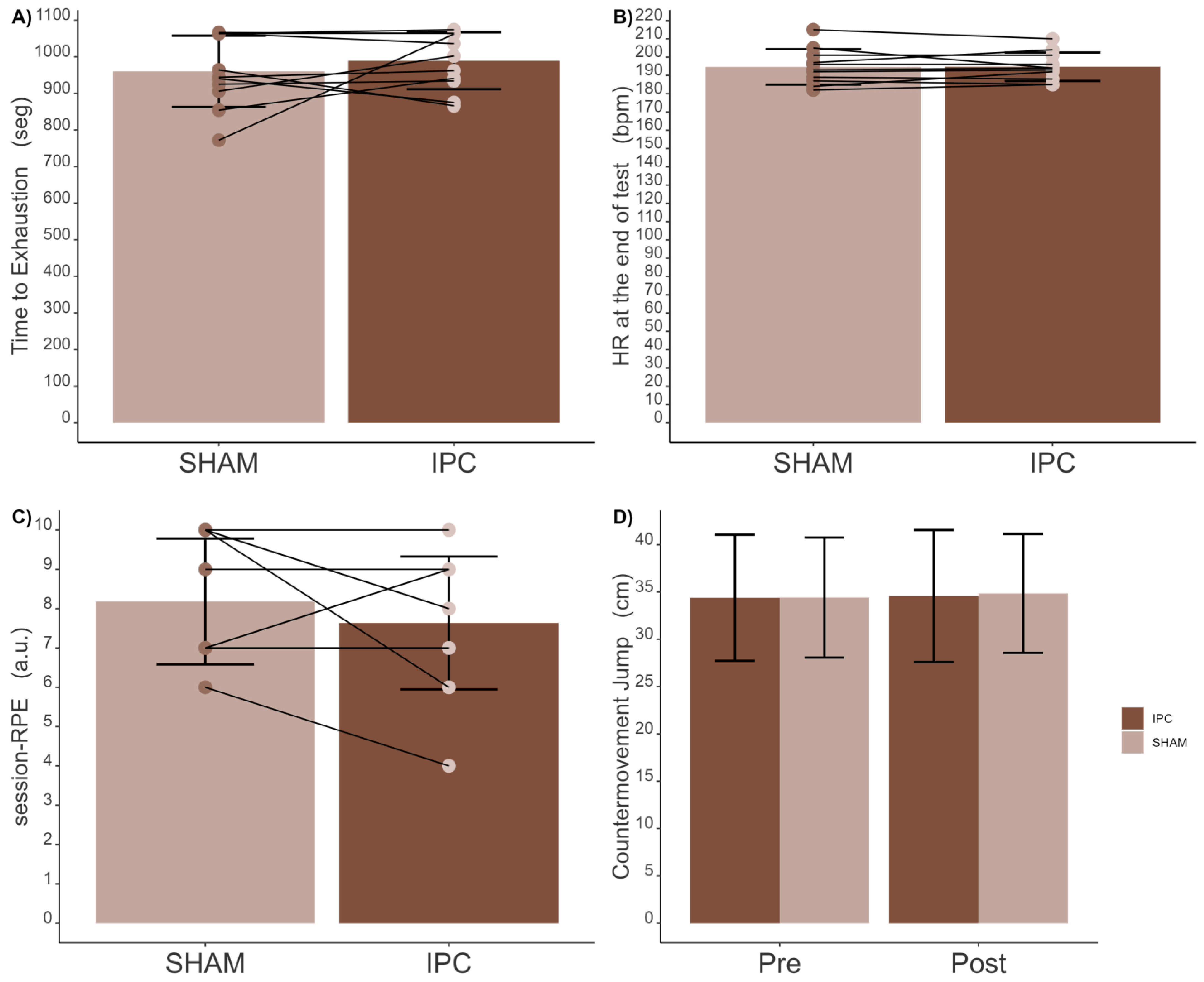
3.2. Study 2
3.2.1. Pre-Intervention
3.2.2. Intervention
3.2.3. Post-Intervention
4. Discussion
5. Conclusions
6. Practical Applications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bridge, C.A.; Santos, J.F.d.S.; Chaabène, H.; Pieter, W.; Franchini, E. Physical and Physiological Profiles of Taekwondo Athletes. Sports Med. 2014, 44, 713–733. [Google Scholar] [CrossRef]
- Santos, J.F.d.S.; Wilson, V.D.; Herrera-Valenzuela, T.; Machado, F.S.M. Time-Motion Analysis and Physiological Responses to Taekwondo Combat in Juvenile and Adult Athletes: A Systematic Review. Strength Cond. J. 2020, 42, 103–121. [Google Scholar] [CrossRef]
- Albuquerque, M.R.; Tavares, L.D.; Longo, A.R.; Caldeira Mesquita, P.H.; Franchini, E. Relationship between Indirect Measures of Aerobic and Muscle Power with Frequency Speed of Kick Test Multiple Performance in Taekwondo Athletes. Int. J. Sports Med. 2021, 43, 254–261. [Google Scholar] [CrossRef]
- Apollaro, G.; Franchini, E.; Falcó, C.; Detanico, D.; Kons, R.L. Sport-Specific Tests for Endurance in Taekwondo: A Narrative Review With Guidelines for the Assessment. Strength Cond. J. 2023, 1–19. [Google Scholar] [CrossRef]
- Chaabene, H.; Negra, Y.; Bouguezzi, R.; Capranica, L.; Franchini, E.; Prieske, O.; Hbacha, H.; Granacher, U. Tests for the Assessment of Sport-Specific Performance in Olympic Combat Sports: A Systematic Review With Practical Recommendations. Front. Physiol. 2018, 9, 386. [Google Scholar] [CrossRef]
- Weakley, J.; Black, G.; McLaren, S.; Scantlebury, S.; Suchomel, T.J.; McMahon, E.; Watts, D.; Read, D.B. Testing and Profiling Athletes: Recommendations for Test Selection, Implementation, and Maximizing Information. Strength Cond. J. 2022, 46, 159–179. [Google Scholar] [CrossRef]
- Caru, M.; Levesque, A.; Lalonde, F.; Curnier, D. An overview of ischemic preconditioning in exercise performance: A systematic review. J. Sport Health Sci. 2019, 8, 355–369. [Google Scholar] [CrossRef]
- Marocolo, M.; Hohl, R.; Arriel, R.A.; Mota, G.R. Ischemic preconditioning and exercise performance: Are the psychophysiological responses underestimated? Eur. J. Appl. Physiol. 2023, 123, 683–693. [Google Scholar] [CrossRef]
- Salvador, A.F.; De Aguiar, R.A.; Lisbôa, F.D.; Pereira, K.L.; Cruz, R.S.d.O.; Caputo, F. Ischemic Preconditioning and Exercise Performance: A Systematic Review and Meta-Analysis. Int. J. Sports Physiol. Perform. 2016, 11, 4–14. [Google Scholar] [CrossRef]
- Latella, C.; Teo, W.-P.; Spathis, J.; van den Hoek, D. Long-Term Strength Adaptation: A 15-Year Analysis of Powerlifting Athletes. J. Strength Cond. Res. 2020, 34, 2412–2418. [Google Scholar] [CrossRef]
- Marocolo, M.; Simim, M.A.M.; Bernardino, A.; Monteiro, I.R.; Patterson, S.D.; da Mota, G.R. Ischemic preconditioning and exercise performance: Shedding light through smallest worthwhile change. Eur. J. Appl. Physiol. 2019, 119, 2123–2149. [Google Scholar] [CrossRef]
- da Silva, R.A.D.; Szmuchrowski, L.A.; Rosa, J.P.P.; Santos, M.A.P.d.; de Mello, M.T.; Savoi, L.; Porto, Y.F.; de Assis Dias Martins Júnior, F.; Drummond, M.D.M. Intermittent Fasting Promotes Weight Loss without Decreasing Performance in Taekwondo. Nutrients 2023, 15, 3131. [Google Scholar] [CrossRef]
- Schoot, R.v.d.; Miočević, M. Small Sample Size Solutions: A Guide for Applied Researchers and Practitioners, 1st ed.; Routledge: London, UK, 2020. [Google Scholar]
- Loturco, I.; Pereira, L.A.; Kobal, R.; Kitamura, K.; Cal Abad, C.C.; Marques, G.; Guerriero, A.; Moraes, J.E.; Nakamura, F.Y. Validity and Usability of a New System for Measuring and Monitoring Variations in Vertical Jump Performance. J. Strength Cond. Res. 2017, 31, 2579–2585. [Google Scholar] [CrossRef]
- Claudino, J.G.; Cronin, J.; Mezêncio, B.; McMaster, D.T.; McGuigan, M.; Tricoli, V.; Amadio, A.C.; Serrão, J.C. The countermovement jump to monitor neuromuscular status: A meta-analysis. J. Sci. Med. Sport 2017, 20, 397–402. [Google Scholar] [CrossRef]
- Laurentino, G.C.; Loenneke, J.P.; Mouser, J.G.; Buckner, S.L.; Counts, B.R.; Dankel, S.J.; Jessee, M.B.; Mattocks, K.T.; Iared, W.; Tavares, L.D.; et al. Validity of the Handheld Doppler to Determine Lower-Limb Blood Flow Restriction Pressure for Exercise Protocols. J. Strength Cond. Res. 2020, 34, 2693–2696. [Google Scholar] [CrossRef]
- Hittinger, E.A.; Maher, J.L.; Nash, M.S.; Perry, A.C.; Signorile, J.F.; Kressler, J.; Jacobs, K.A. Ischemic preconditioning does not improve peak exercise capacity at sea level or simulated high altitude in trained male cyclists. Appl. Physiol. Nutr. Metab. 2015, 40, 65–71. [Google Scholar] [CrossRef]
- de Souza, H.L.R.; Arriel, R.A.; Mota, G.R.; Hohl, R.; Marocolo, M. Does ischemic preconditioning really improve performance or it is just a placebo effect? PLoS ONE 2021, 16, e0250572. [Google Scholar] [CrossRef]
- Mesquita, P.H.C.; Franchini, E.; Romano-Silva, M.A.; Lage, G.M.; Albuquerque, M.R. Transcranial Direct Current Stimulation: No Effect on Aerobic Performance, Heart Rate, or Rating of Perceived Exertion in a Progressive Taekwondo-Specific Test. Int. J. Sports Physiol. Perform. 2020, 15, 958–963. [Google Scholar] [CrossRef]
- Sant’ Ana, J.; Franchini, E.; Murias, J.M.; Diefenthaeler, F. Validity of a Taekwondo-Specific Test to Measure Vo2peak and the Heart Rate Deflection Point. J. Strength Cond. Res. 2019, 33, 2523–2529. [Google Scholar] [CrossRef]
- McCabe, L.H.; Greer, B.D. Evaluations of heart rate during functional analyses of destructive behavior. J. Appl. Behav. Anal. 2023, 56, 777–786. [Google Scholar] [CrossRef]
- Santos, J.F.d.S.; Franchini, E. Frequency Speed of Kick Test Performance Comparison Between Female Taekwondo Athletes of Different Competitive Levels. J. Strength Cond. Res. 2018, 32, 2934–2938. [Google Scholar] [CrossRef]
- Santos, J.F.d.S.; Franchini, E. Trainers’ understanding of chosing the frequency speed of kick test (FSKT) for taekwondo practitioners. Ido Mov. Culture. J. Martial Arts Anthropol. 2021, 21, 1–5. [Google Scholar]
- Antonaccio, R.F.; Machado, F.S.M.; Santos, J.F.d.S. Intra- and Inter-rater Objectivity of the Frequency Speed of Kick Test. Ido Mov. Culture. J. Martial Arts Anthropol. 2022, 22, 1–5. [Google Scholar]
- Santos, J.F.d.S.; Franchini, E. Is frequency speed of kick test responsive to training? A study with taekwondo athletes. Sport Sci. Health 2016, 12, 377–382. [Google Scholar] [CrossRef]
- Torchiano, M. Effsize: Efficient Effect Size Computation. Available online: https://CRAN.R-project.org/package=effsize (accessed on 27 February 2024).
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Kassambara, A. Rstatix: Pipe-Friendly Framework for Basic Statistical Tests. Available online: https://CRAN.R-project.org/package=rstatix (accessed on 27 February 2024).
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 3rd ed.; SAGE: London, UK, 2009. [Google Scholar]
- Morey, R.D.; Roude, J.N. BayesFactor: Computation of Bayes Factors for Common Designs. Available online: https://CRAN.R-project.org/package=BayesFactor (accessed on 27 February 2024).
- Kelter, R. Bayesian alternatives to null hypothesis significance testing in biomedical research: A non-technical introduction to Bayesian inference with JASP. BMC Med. Res. Methodol. 2020, 20, 142. [Google Scholar] [CrossRef]
- Campos, F.A.D.; Bertuzzi, R.; Dourado, A.C.; Santos, V.G.F.; Franchini, E. Energy demands in taekwondo athletes during combat simulation. Eur. J. Appl. Physiol. 2012, 112, 1221–1228. [Google Scholar] [CrossRef]
- Cruz, R.S.d.O.; Aguiar, R.A.d.; Turnes, T.; Pereira, K.L.; Caputo, F. Effects of ischemic preconditioning on maximal constant-load cycling performance. J. Appl. Physiol. 2015, 119, 961–967. [Google Scholar] [CrossRef]
- Kido, K.; Suga, T.; Tanaka, D.; Honjo, T.; Homma, T.; Fujita, S.; Hamaoka, T.; Isaka, T. Ischemic preconditioning accelerates muscle deoxygenation dynamics and enhances exercise endurance during the work-to-work test. Physiol. Rep. 2015, 3, e12395. [Google Scholar] [CrossRef]
- de Groot, P.C.E.; Thijssen, D.H.J.; Sanchez, M.; Ellenkamp, R.; Hopman, M.T.E. Ischemic preconditioning improves maximal performance in humans. Eur. J. Appl. Physiol. 2010, 108, 141–146. [Google Scholar] [CrossRef]
- Goulart, K.; Corgosinho, R.; Rodrigues, S.; Drummond, M.; Flôr, C.; Gonçalves, R.; Szmuchrowski, L.; Couto, B. Correlation between roundhouse kick and countermovement jump performance. Arch. Budo 2016, 12. [Google Scholar]
- Beaven, C.M.; Cook, C.J.; Kilduff, L.; Drawer, S.; Gill, N. Intermittent lower-limb occlusion enhances recovery after strenuous exercise. Appl. Physiol. Nutr. Metab. 2012, 37, 1132–1139. [Google Scholar] [CrossRef] [PubMed]
- Ceylan, B.; Franchini, E. Ischemic preconditioning does not improve judo-specific performance but leads to better recovery in elite judo athletes. Sci. Sports 2022, 37, 322.e1–322.e7. [Google Scholar] [CrossRef]
- Ceylan, B.; Taşkın, H.B.; Šimenko, J. Effect of Ischemic Preconditioning on Acute Recovery in Elite Judo Athletes: A Randomized, Single-Blind, Crossover Trial. Int. J. Sports Physiol. Perform. 2023, 18, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Mesquita, P.H.C.; Lage, G.M.; Franchini, E.; Romano-Silva, M.A.; Albuquerque, M.R. Bi-hemispheric anodal transcranial direct current stimulation worsens taekwondo-related performance. Hum. Mov. Sci. 2019, 66, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Cocking, S.; Wilson, M.G.; Nichols, D.; Cable, N.T.; Green, D.J.; Thijssen, D.H.J.; Jones, H. Is There an Optimal Ischemic-Preconditioning Dose to Improve Cycling Performance? Int. J. Sports Physiol. Perform. 2018, 13, 274–282. [Google Scholar] [CrossRef]
- Ribeiro, A.; Franchini, E.; Mesquita, P.H.C.; Amaral-Junior, P.; Albuquerque, M.R. Development and reliability of a kick test system for taekwondo athletes. Ido Mov. Culture. J. Martial Arts Anthropol. 2020, 20, 31–39. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Repeated Measure ANOVA | Bayes Factor Analysis | |||||||
|---|---|---|---|---|---|---|---|---|
| Condition | Set | Interaction | Model 1 | Model 2 | Model 3 | Model 4 | ||
| Block 1 | Bout 1 | F1;13 = 0.055; p = 0.818 ηp2 = 0.004 | F2.05;26.71 = 68.192; p < 0.001 ηp2 = 0.840 | F4;52 = 1.677; p = 0.169 ηp2 = 0.114 | BF10: 0.22 | BF10: 6.29 × 1021 | BF10: 1.23 × 1021 | 1.90 × 1020 |
| Bout 2 | F1;13 = 0.079; p = 0.784 ηp2 = 0.006 | F2.56;33.34 = 89.136; p < 0.001 ηp2 = 0.873 | F4;52 = 2.642; p = 0.044 ηp2 = 0.169 | BF10: 0.19 | BF10: 6.60 × 1021 | BF10: 1.36 × 1021 | 3.40 × 1020 | |
| Bout 3 | F1;13 = 0.657; p = 0.432 ηp2 = 0.048 | F2.32;30.18 = 56.041; p < 0.001 ηp2 = 0.812 | F4;52 = 0.457; p = 0.767 ηp2 = 0.034 | BF10: 0.25 | BF10: 2.67 × 1020 | BF10: 1.14 × 1020 | 9.92 × 1018 | |
| Block 2 | Bout 1 | F1;13 = 0.978; p = 0.341 ηp2 = 0.070 | F1.52;19.71 = 54.030; p < 0.001 ηp2 = 0.806 | F4;52 = 0.858; p = 0.495 ηp2 = 0.062 | BF10: 0.25 | BF10: 4.72 × 1026 | BF10: 2.59 × 1026 | 2.22 × 1025 |
| Bout 2 | F1;13 = 0.127; p = 0.728 ηp2 = 0.010 | F1.75;22.76 = 39.205; p < 0.001 ηp2 = 0.751 | F2.34;30.40 = 1.163; p = 0.332 ηp2 = 0.082 | BF10: 0.18 | BF10: 6.32 × 1021 | BF10: 1.22 × 1021 | 1.51 × 1020 | |
| Bout 3 | F1;13 = 0.054; p = 0.820 ηp2 = 0.004 | F1.90;24.76 = 32.660; p < 0.001 ηp2 = 0.715 | F1.91;24.85 = 0.127; p = 0.873 ηp2 = 0.010 | BF10: 0.19 | BF10: 3.85 × 1017 | BF10: 7.46 × 1016 | 4.70 × 1015 | |
| Block 3 | Bout 1 | F1;13 = 0.843; p = 0.375 ηp2 = 0.061 | F1.84;23.94 = 61.972; p < 0.001 ηp2 = 0.827 | F1.98;25.80 = 0.797; p = 0.186 ηp2 = 0.121 | BF10: 0.29 | BF10: 1.62 × 1020 | BF10: 9.21 × 1019 | 2.60 × 1028 |
| Bout 2 | F1;13 = 0.185; p = 0.674 ηp2 = 0.014 | F1.98;25.76 = 21.387; p < 0.001 ηp2 = 0.622 | F4;52 = 1.830; p = 0.137 ηp2 = 0.123 | BF10: 0.19 | BF10: 6.33 × 1012 | BF10: 1.36 × 1012 | 2.08 × 1011 | |
| Bout 3 | F1;13 = 0.079; p = 0.783 ηp2 = 0.006 | F2.34;30.38 = 23.807; p < 0.001 ηp2 = 0.647 | F4;52 = 0.1.243; p = 0.304 ηp2 = 0.087 | BF10: 0.19 | BF10: 7.25 × 1012 | BF10: 1.38 × 1012 | 1.84 × 1011 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albuquerque, M.R.; Flôr, C.A.G.; Ribeiro, A.I.S.; Mesquita, P.H.C.; Franchini, E.; Laurentino, G.C. Effects of Ischemic Preconditioning on Sport-Specific Performance in Highly Trained Taekwondo Athletes. Sports 2024, 12, 179. https://doi.org/10.3390/sports12070179
Albuquerque MR, Flôr CAG, Ribeiro AIS, Mesquita PHC, Franchini E, Laurentino GC. Effects of Ischemic Preconditioning on Sport-Specific Performance in Highly Trained Taekwondo Athletes. Sports. 2024; 12(7):179. https://doi.org/10.3390/sports12070179
Chicago/Turabian StyleAlbuquerque, Maicon Rodrigues, Cristiano Arruda Gomes Flôr, Amanda Isadora Santos Ribeiro, Paulo Henrique Caldeira Mesquita, Emerson Franchini, and Gilberto Candido Laurentino. 2024. "Effects of Ischemic Preconditioning on Sport-Specific Performance in Highly Trained Taekwondo Athletes" Sports 12, no. 7: 179. https://doi.org/10.3390/sports12070179
APA StyleAlbuquerque, M. R., Flôr, C. A. G., Ribeiro, A. I. S., Mesquita, P. H. C., Franchini, E., & Laurentino, G. C. (2024). Effects of Ischemic Preconditioning on Sport-Specific Performance in Highly Trained Taekwondo Athletes. Sports, 12(7), 179. https://doi.org/10.3390/sports12070179