
Full-Body Photobiomodulation Therapy Is Associated with Reduced Sleep Durations and Augmented Cardiorespiratory Indicators of Recovery


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Procedures
2.2. Obtained Samples
2.3. Measures
2.3.1. Cardiorespiratory Physiology
2.3.2. Sleep
2.3.3. External Training Load
2.4. Statistical Analyses
2.4.1. Intra-Night Relationships
2.4.2. External Training Load
3. Results
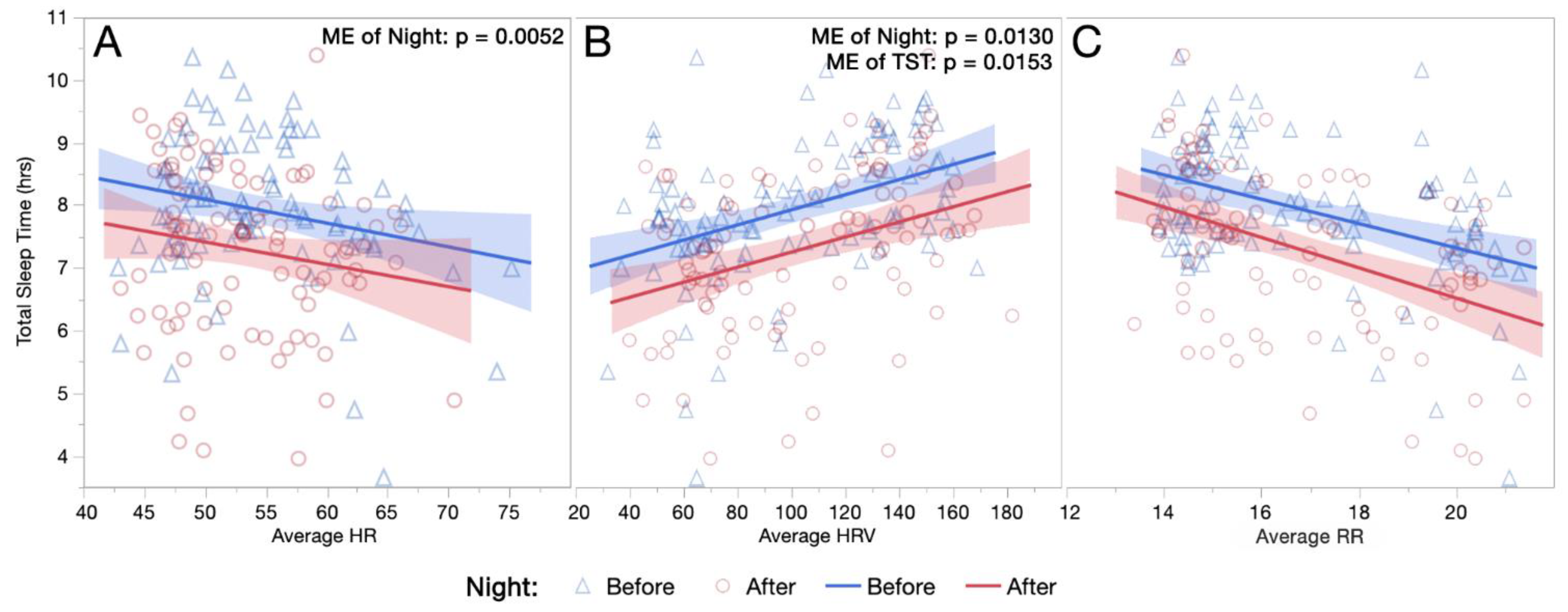
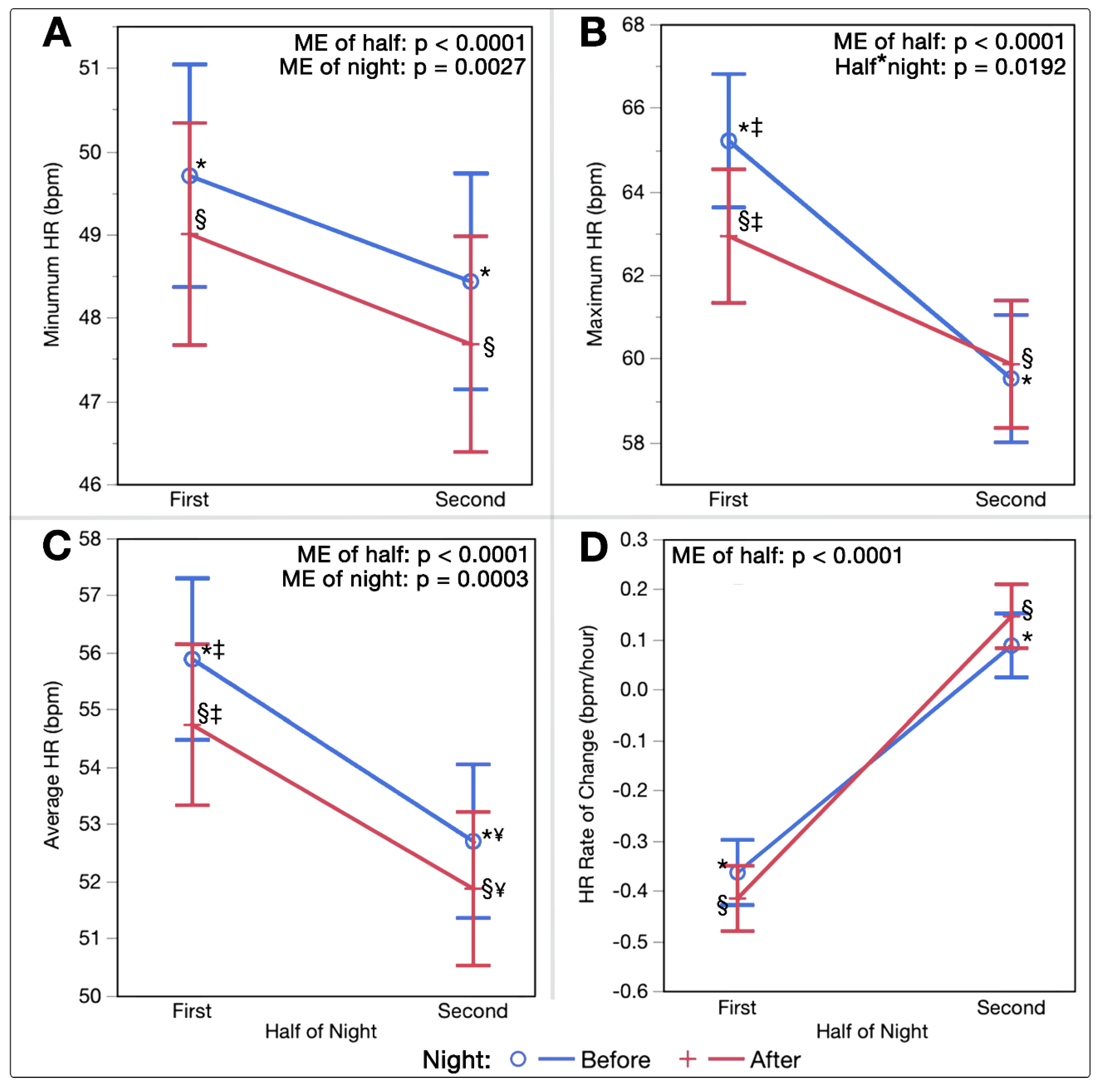
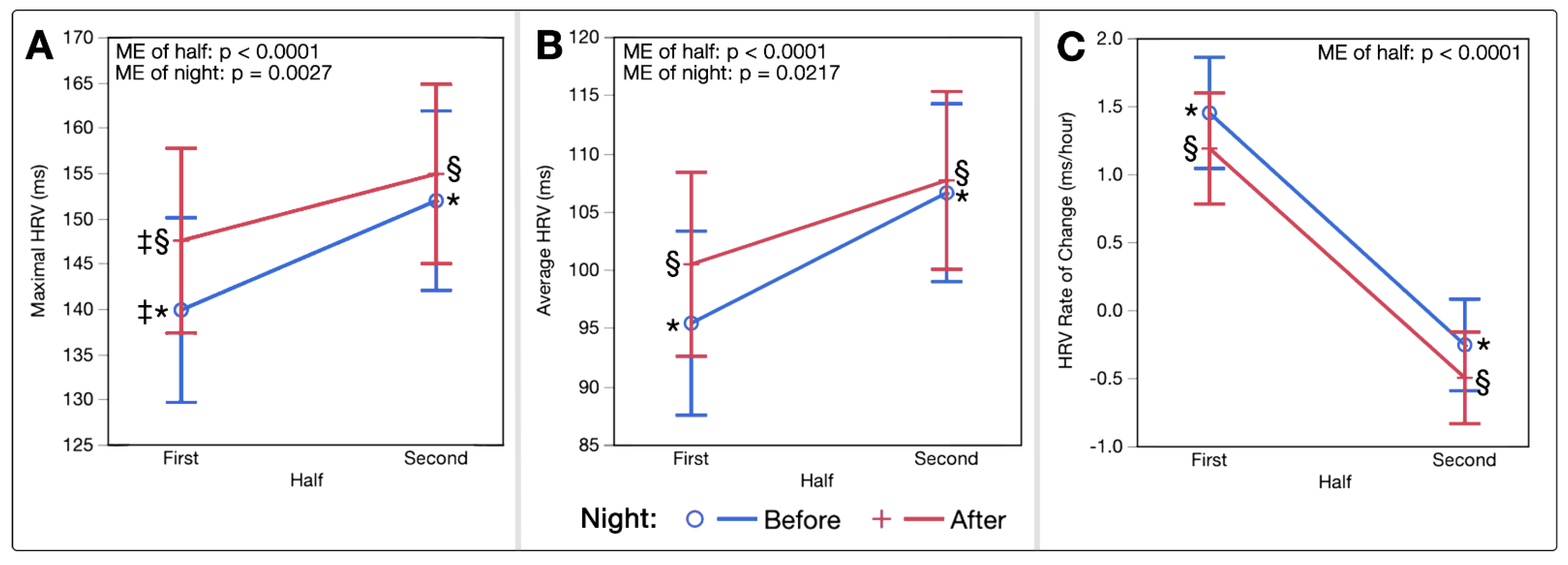
3.1. Intra-Night Relationships
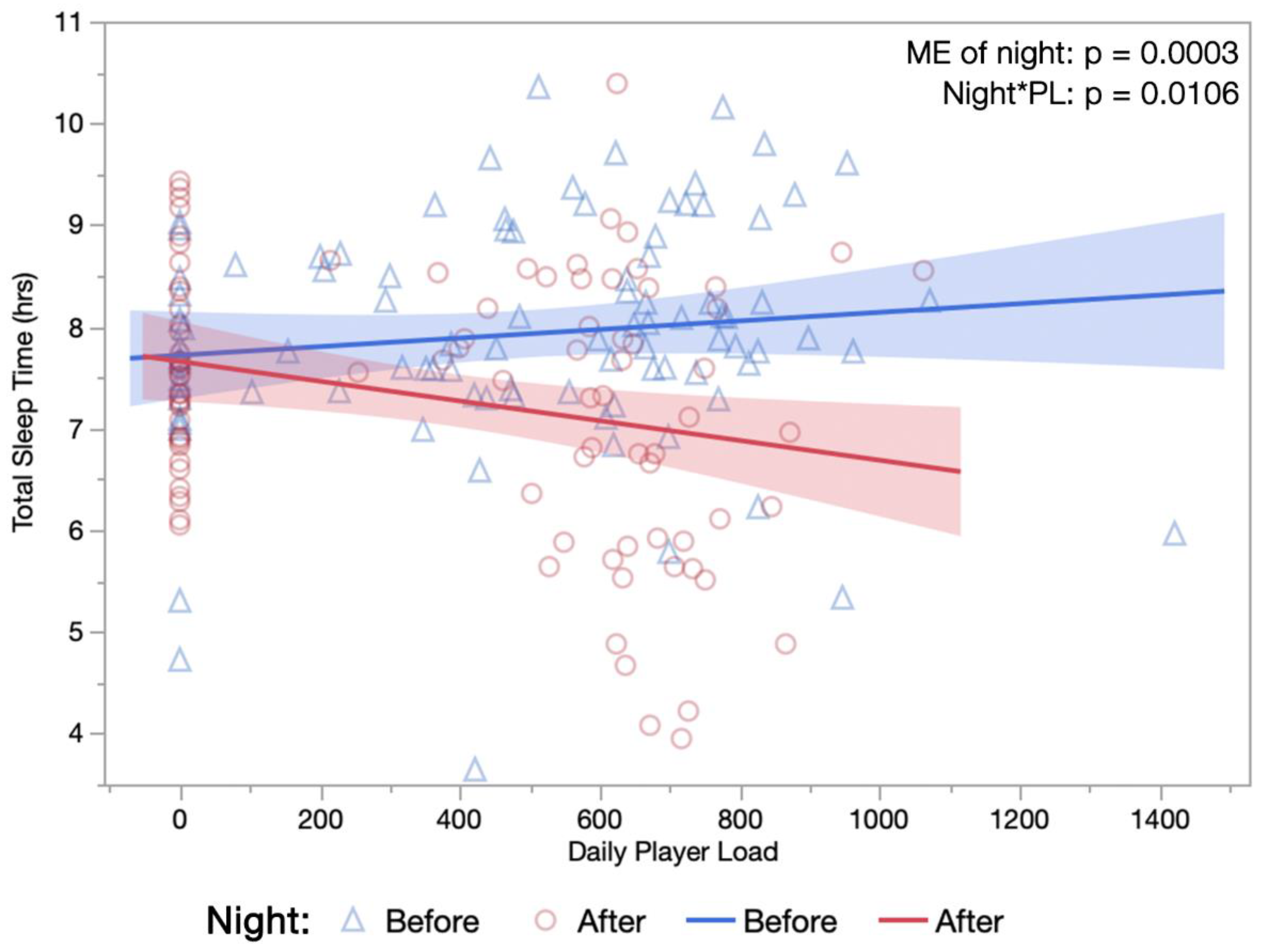
3.2. Training Load
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Humphreys, B.; Ruseski, J. The Size and Scope of the Sports Industry in the United States. In Proceedings of the 10th Annual International Association of Sports Economists Conference, Gijón, Spain, 29–31 August 2008. [Google Scholar]
- Dos Santos, M.L.; Uftring, M.; Stahl, C.A.; Lockie, R.G.; Alvar, B.; Mann, J.B.; Dawes, J.J. Stress in Academic and Athletic Performance in Collegiate Athletes: A Narrative Review of Sources and Monitoring Strategies. Front. Sports Act. Living 2020, 2, 42. [Google Scholar] [CrossRef] [PubMed]
- Ramezani, F.; Neshasteh-Riz, A.; Ghadaksaz, A.; Fazeli, S.M.; Janzadeh, A.; Hamblin, M.R. Mechanistic Aspects of Photobiomodulation Therapy in the Nervous System. Lasers Med. Sci. 2021, 37, 11–18. [Google Scholar] [CrossRef] [PubMed]
- de Freitas, L.F.; Hamblin, M.R. Proposed Mechanisms of Photobiomodulation or Low-Level Light Therapy. IEEE J. Sel. Top. Quantum Electron. 2016, 22, 348–364. [Google Scholar] [CrossRef]
- Dompe, C.; Moncrieff, L.; Matys, J.; Grzech-Leśniak, K.; Kocherova, I.; Bryja, A.; Bruska, M.; Dominiak, M.; Mozdziak, P.; Skiba, T.H.I.; et al. Photobiomodulation—Underlying Mechanism and Clinical Applications. J. Clin. Med. 2020, 9, 1724. [Google Scholar] [CrossRef] [PubMed]
- Sommer, A.P. Mitochondrial Cytochrome C Oxidase is Not the Primary Acceptor for Near Infrared Light—It is Mitochondrial Bound Water: The Principles of Low-Level Light Therapy. Ann. Transl. Med. 2019, 7, S13. [Google Scholar] [CrossRef]
- Hamblin, M.R. Mechanisms and Applications of the Anti-Inflammatory Effects of Photobiomodulation. AIMS Biophys. 2017, 4, 337–361. [Google Scholar] [CrossRef]
- Glass, G.E. Photobiomodulation: A Review of the Molecular Evidence for Low Level Light Therapy. J. Plast. Reconstr. Aesthet Surg. 2021, 74, 1050–1060. [Google Scholar] [CrossRef]
- Hamblin, M.R. Photobiomodulation for Alzheimer’s Disease: Has the Light Dawned? Photonics 2019, 6, 77. [Google Scholar] [CrossRef]
- Ravera, S.; Colombo, E.; Pasquale, C.; Benedicenti, S.; Solimei, L.; Signore, A.; Amaroli, A. Mitochondrial Bioenergetic, Photobiomodulation and Trigeminal Branches Nerve Damage, What’s the Connection? A Review. Int. J. Mol. Sci. 2021, 22, 4347. [Google Scholar] [CrossRef]
- Dos Santos, S.A.; Serra, A.J.; Stancker, T.G.; Simões, M.C.B.; Vieira, M.A.D.S.; Leal-Junior, E.C.; Prokic, M.; Vasconsuelo, A.; Santos, S.S.; Carvalho, P.D.T.C.D. Effects of Photobiomodulation Therapy on Oxidative Stress in Muscle Injury Animal Models: A Systematic Review. Oxidative Med. Cell. Longev. 2017, 2017, 5273403. [Google Scholar] [CrossRef] [PubMed]
- Toma, R.L.; Oliveira, M.X.; Renno, A.C.M.; Laakso, E.-L. Photobiomodulation (PBM) Therapy at 904 nm Mitigates Effects of Exercise-Induced Skeletal Muscle Fatigue in Young Women. Lasers Med. Sci. 2018, 33, 1197–1205. [Google Scholar] [CrossRef] [PubMed]
- Pinto, H.D.; Vanin, A.A.; Miranda, E.; Tomazoni, S.S.; Johnson, D.S.; Albuquerque-Pontes, G.M.; Aleixo, I.D.O.; Grandinetti, V.D.S.; Casalechi, H.L.; Carvalho, P.D.T.D.; et al. Photobiomodulation Therapy Improves Performance and Accelerates Recovery of High-Level Rugby Players in Field Test: A Randomized, Crossover, Double-Blind, Placebo-Controlled Clinical Study. J. Strength Cond. Res. 2016, 30, 3329–3338. [Google Scholar] [CrossRef] [PubMed]
- Miranda, E.F.; Vanin, A.A.; Tomazoni, S.S.; Grandinetti, V.d.S.; de Paiva, P.R.V.; Machado, C.d.S.M.; Monteiro, K.K.D.S.; Casalechi, H.L.; de Carvalho, P.d.T.C.; Leal-Junior, E.C.P. Using Pre-Exercise Photobiomodulation Therapy Combining Super-Pulsed Lasers and Light-Emitting Diodes to Improve Performance in Progressive Cardiopulmonary Exercise Tests. J. Athl. Train. 2016, 51, 129–135. [Google Scholar] [CrossRef]
- Dellagrana, R.A.; Rossato, M.; Sakugawa, R.L.; Lazzari, C.D.; Baroni, B.M.; Diefenthaeler, F. Dose-Response Effect of Photobiomodulation Therapy on Neuromuscular Economy during Submaximal Running. Lasers Med. Sci. 2018, 33, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Ferraresi, C.; Huang, Y.-Y.; Hamblin, M.R. Photobiomodulation in Human Muscle Tissue: An Advantage in Sports Performance? J. Biophotonics 2016, 9, 1273–1299. [Google Scholar] [CrossRef] [PubMed]
- De Marchi, T.; Leal-Junior, E.C.P.; Lando, K.C.; Cimadon, F.; Vanin, A.A.; Pase da Rosa, D.; Salvador, M. Photobiomodulation Therapy Before Futsal Matches Improves the Staying Time of Athletes in the Court and Accelerates Post-Exercise Recovery. Lasers Med. Sci. 2019, 34, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Malta, E.d.S.; de Lira, F.S.; Machado, F.A.; Zago, A.S.; Amaral, S.L.d.; Zagatto, A.M. Photobiomodulation by LED Does Not Alter Muscle Recovery Indicators and Presents Similar Outcomes to Cold-Water Immersion and Active Recovery. Front. Physiol. 2019, 9, 1948. [Google Scholar] [CrossRef] [PubMed]
- Zagatto, A.M.; Dutra, Y.M.; Santos Lira, F.; Antunes, B.M.; Faustini, J.B.; Malta, E.d.S.; Lopes, V.H.F.; de Poli, R.A.B.; Brisola, G.M.P.; dos Santos, G.V.; et al. Full Body Photobiomodulation Therapy to Induce Faster Muscle Recovery in Water Polo Athletes: Preliminary Results. Photobiomodul. Photomed. Laser Surg. 2020, 38, 766–772. [Google Scholar] [CrossRef]
- Heiskanen, V.; Hamblin, M.R. Photobiomodulation: Lasers vs. light emitting diodes? Photochem. Photobiol. Sci. 2018, 17, 1003–1017. [Google Scholar] [CrossRef] [PubMed]
- Lima, A.C.; Fernandes, G.A.; Gonzaga, I.C.; de Barros Araujo, R.; de Oliveira, R.A.; Nicolau, R.A. Low-Level Laser and Light-Emitting Diode Therapy for Pain Control in Hyperglycemic and Normoglycemic Patients Who Underwent Coronary Bypass Surgery with Internal Mammary Artery Grafts: A Randomized, Double-Blind Study with Follow-Up. Photomed. Laser Surg. 2016, 34, 244–251. [Google Scholar] [CrossRef]
- Ammar, T.A. Monochromatic Infrared Photo Energy versus Low Level Laser Therapy in Patients with Knee Osteoarthritis. J. Lasers Med. Sci. 2014, 5, 176–182. [Google Scholar] [PubMed]
- Leal, E.C.P.; Lopes-Martins, R.A.B.; Baroni, B.M.; De Marchi, T.; Rossi, R.P.; Grosselli, D.; Generosi, R.A.; de Godoi, V.; Basso, M.; Mancalossi, J.L.; et al. Comparison Between Single-Diode Low-Level Laser Therapy (LLLT) and LED Multi-Diode (Cluster) Therapy (LEDT) Applications Before High-Intensity Exercise. Photomed. Laser Surg. 2009, 27, 617–623. [Google Scholar] [CrossRef] [PubMed]
- Esper, M.A.L.R.; Nicolau, R.A.; Arisawa, E.A.L. The effect of two phototherapy protocols on pain control in orthodontic procedure-a preliminary clinical study. Lasers Med. Sci. 2011, 26, 657–663. [Google Scholar] [CrossRef] [PubMed]
- Freitas, A.C.C.; Campos, L.; Brandao, T.B.; Cristofaro, M.; Eduardo, F.D.; Luiz, A.C.; Marques, M.M.; Eduardo, C.D.; Simoes, A. Chemotherapy-Induced Oral Mucositis: Effect of LED and Laser Phototherapy Treatment Protocols. Photomed. Laser Surg. 2014, 32, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Dellagrana, R.A.; Rossato, M.; Sakugawa, R.L.; Baroni, B.M.; Diefenthaeler, F. Photobiomodulation Therapy on Physiological and Performance Parameters During Running Tests: Dose–Response Effects. J. Strength Cond. Res. 2018, 32, 2807–2815. [Google Scholar] [CrossRef] [PubMed]
- Rossato, M.; Dellagrana, R.A.; Sakugawa, R.L.; Baroni, B.M.; Diefenthaeler, F. Dose–Response Effect of Photobiomodulation Therapy on Muscle Performance and Fatigue During a Multiple-Set Knee Extension Exercise: A Randomized, Crossover, Double-Blind Placebo Controlled Trial. Photobiomodul. Photomed. Laser Surg. 2020, 38, 758–765. [Google Scholar] [CrossRef]
- Tuner, J. Photobiomodulation: How Many Sessions and How Often? Photomed. Laser Surg. 2018, 36, 59–60. [Google Scholar] [CrossRef] [PubMed]
- Dutra, Y.M.; Claus, G.M.; Malta, E.d.S.; Brisola, G.M.P.; Esco, M.R.; Ferraresi, C.; Zagatto, A.M. Acute Photobiomodulation by LED Does Not Alter Muscle Fatigue and Cycling Performance. Med. Sci. Sports Exerc. 2020, 52, 2448–2458. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Tian, Y.; Nie, J.; Xu, J.; Liu, D. Red Light and the Sleep Quality and Endurance Performance of Chinese Female Basketball Players. J. Athl. Train. 2012, 47, 673–678. [Google Scholar] [CrossRef]
- Rossato, M.; Dellagrana, R.A.; Sakugawa, R.L.; Lazzari, C.D.; Baroni, B.M.; Diefenthaeler, F. Time Response of Photobiomodulation Therapy on Muscular Fatigue in Humans. J. Strength Cond. Res. 2018, 32, 3285–3293. [Google Scholar] [CrossRef]
- Ghigiarelli, J.J.; Fulop, A.M.; Burke, A.A.; Ferrara, A.J.; Sell, K.M.; Gonzalez, A.M.; Pelton, L.M.; Zimmerman, J.A.; Coke, S.G.; Marshall, D.G. The Effects of Whole-Body Photobiomodulation Light-Bed Therapy on Creatine Kinase and Salivary Interleukin-6 in a Sample of Trained Males: A Randomized, Crossover Study. Front. Sports Act. Living 2020, 2, 48. [Google Scholar] [CrossRef] [PubMed]
- Kiviniemi, A.M.; Hautala, A.J.; Kinnunen, H.; Tulppo, M.P. Endurance Training Guided Individually by Daily Heart Rate Variability Measurements. Eur. J. Appl. Physiol. 2007, 101, 743–751. [Google Scholar] [CrossRef] [PubMed]
- Buchheit, M. Monitoring Training Status with HR Measures: Do All Roads Lead to Rome? Front. Physiol. 2014, 5, 73. [Google Scholar] [CrossRef]
- Al Haddad, H.; Laursen, P.B.; Chollet, D.; Ahmaidi, S.; Buchheit, M. Reliability of Resting and Postexercise Heart Rate Measures. Int. J. Sports Med. 2011, 32, 598–605. [Google Scholar] [CrossRef]
- Eyal, S.; Altman, Y.; Baharav, A. 1010 Sleep Related Recovery in Athletes: The Role of Heart Rate Variability Parameters. Sleep 2019, 42, A406–A407. [Google Scholar] [CrossRef]
- Chokroverty, S.; Cortelli, P. (Eds.) Autonomic Nervous System and Sleep: Order and Disorder; Springer Nature: New York, NY, USA, 2021. [Google Scholar]
- de Zambotti, M.; Trinder, J.; Silvani, A.; Colrain, I.M.; Baker, F.C. Dynamic Coupling Between the Central and Autonomic Nervous Systems During Sleep: A Review. Neurosci. Biobehav. Rev. 2018, 90, 84–103. [Google Scholar] [CrossRef] [PubMed]
- Roche, F.; Gaspoz, J.-M.; Court-Fortune, I.; Minini, P.; Pichot, V.; Duverney, D.; Costes, F.; Lacour, J.-R.; Barthélémy, J.-C. Screening of Obstructive Sleep Apnea Syndrome by Heart Rate Variability Analysis. Circulation 1999, 100, 1411–1415. [Google Scholar] [CrossRef] [PubMed]
- Otzenberger, H.; Gronfier, C.; Simon, C.; Charloux, A.; Ehrhart, J.; Piquard, F.; Brandenberger, G. Dynamic Heart Rate Variability: A Tool for Exploring Sympathovagal Balance Continuously During Sleep in Men. Am. J. Physiol. Heart Circ. Physiol. 1998, 275, H946–H950. [Google Scholar] [CrossRef]
- Waldeck, M.R.; Lambert, M.I. Heart Rate During Sleep: Implications for Monitoring Training Status. J. Sports Sci. Med. 2003, 2, 133–138. [Google Scholar]
- Burton, A.R.; Rahman, K.; Kadota, Y.; Lloyd, A.; Vollmer-Conna, U. Reduced Heart Rate Variability Predicts Poor Sleep Quality in a Case–Control Study of Chronic Fatigue Syndrome. Exp. Brain Res. 2010, 204, 71–78. [Google Scholar] [CrossRef]
- Pichot, V.; Roche, F.; Gaspoz, J.-M.; Enjolras, F.; Antoniadis, A.; Minini, P.; Costes, F.; Busso, T.; Lacour, J.-R.; Barthelemy, J.C. Relation Between Heart Rate Variability and Training Load in Middle-Distance Runners. Med. Sci. Sports Exerc. 2000, 32, 1729–1736. [Google Scholar] [CrossRef]
- Myllymaki, T.; Rusko, H.; Syvaoja, H.; Juuti, T.; Kinnunen, M.-L. Effects of Exercise Intensity and Duration on Nocturnal Heart Rate Variability and Sleep Quality. Eur. J. Appl. Physiol. 2012, 112, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Costa, J.; Figueiredo, P.; Nakamura, F.; Rago, V.; Rebelo, A.; Brito, J. Intra-Individual Variability of Sleep and Nocturnal Cardiac Autonomic Activity in Elite Female Soccer Players During an International Tournament. PLoS ONE 2019, 14, e0218635. [Google Scholar] [CrossRef] [PubMed]
- Watson, A.M. Sleep and Athletic Performance. Curr. Sports Med. Rep. 2017, 16, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Hainline, B.; Derman, W.; Vernec, A.; Budgett, R.; Deie, M.; Dvorak, J.; Harle, C.; Herring, S.A.; McNamee, M.; Meeuwisse, W.; et al. International Olympic Committee Consensus Statement on Pain Management in Elite Athletes. Br. J. Sports Med. 2017, 51, 1245–1258. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, P.A.; Carroll, J.D. How to report low-level laser therapy (LLLT)/photomedicine dose and beam parameters in clinical and laboratory studies. Photomed. Laser Surg. 2011, 29, 785–787. [Google Scholar] [CrossRef] [PubMed]
- Burgess, H.J.; Holmes, A.L.; Dawson, D. The Relationship Between Slow-wave Activity, Body Temperature, and Cardiac Activity During Nighttime Sleep. Sleep 2001, 24, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Brandenberger, G.; Buchheit, M.; Ehrhart, J.; Simon, C.; Piquard, F. Is Slow Wave Sleep an Appropriate Recording Condition for Heart Rate Variability Analysis? Auton. Neurosci. 2005, 121, 81–86. [Google Scholar] [CrossRef]
- Costa, J.A.; Figueiredo, P.; Nakamura, F.Y.; Rebelo, A.; Brito, J. Monitoring Individual Sleep and Nocturnal Heart Rate Variability Indices: The Impact of Training and Match Schedule and Load in High-Level Female Soccer Players. Front. Physiol. 2021, 12, 678462. [Google Scholar] [CrossRef] [PubMed]
- Thornton, H.; Delaney, J.A.; Duthie, G.M.; Dascombe, B.J. Effects of Preseason Training on the Sleep Characteristics of Professional Rugby League Players. Int. J. Sports Physiol. Perform. 2018, 13, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Aloulou, A.; Duforez, F.; Bieuzen, F.; Nedelec, M. The Effect of Night-Time Exercise on Sleep Architecture Among Well-Trained Male Endurance Runners. J. Sleep Res. 2020, 29, e12964. [Google Scholar] [CrossRef] [PubMed]
- Taboada, L.D.; Yu, J.; El-Amouri, S.; Gattoni-Celli, S.; Richieri, S.; McCarthy, T.; Streeter, J.; Kindy, M.S. Transcranial Laser Therapy Attenuates Amyloid-β Peptide Neuropathology in Amyloid-β Protein Precursor Transgenic Mice. J. Alzheimers Dis. 2011, 23, 521–535. [Google Scholar] [CrossRef] [PubMed]
- Grillo, S.L.; Duggett, N.A.; Ennaceur, A.; Chazot, P.L. Non-invasive Infra-red Therapy (1072 nm) Reduces b-Amyloid Protein Levels in the Brain of an Alzheimer’s Disease Mouse Model, TASTPM. J. Photochem. Photobiol. 2013, 123, 13–22. [Google Scholar] [CrossRef]
- Salehpour, F.; Majdi, A.; Pazhuhi, M.; Ghasemi, F.; Khademi, M.; Pashazadeh, F.; Hamblin, M.R.; Cassano, P. Transcranial Photobiomodulation Improves Cognitive Performance in Young Healthy Adults: A Systematic Review and Meta-Analysis. Photobiomodul. Photomed. Laser Surg. 2019, 37, 635–643. [Google Scholar] [CrossRef]
- Vanin, A.A.; Verhagen, E.; Barboza, S.D.; Pena Costa, L.O.; Leal-Junior, E.C.P. Photobiomodulation Therapy for the Improvement of Muscular Performance and Reduction of Muscular Fatigue Associated with Exercise in Healthy People: A Systematic Review and Meta-analysis. Lasers Med. Sci. 2018, 33, 181–214. [Google Scholar] [CrossRef]
- Soheilifar, S.; Fathi, H.; Naghdi, N. Photobiomodulation Therapy as a High Potential Treatment Modality for COVID-19. Lasers Med. Sci. 2021, 36, 935–938. [Google Scholar] [CrossRef] [PubMed]
- Rentz, L.E.; Ulman, H.K.; Galster, S.M. Deconstructing Commercial Wearable Technology: Contributions toward Accurate and Free-Living Monitoring of Sleep. Sensors 2021, 21, 5071. [Google Scholar] [CrossRef] [PubMed]
- Stone, J.D.; Rentz, L.E.; Forsey, J.; Ramadan, J.; Markwald, R.R.; Finomore, V.S.; Galster, S.M.; Rezai, A.; Hagen, J.A. Evaluations of Commercial Sleep Technologies for Objective Monitoring During Routine Sleeping Conditions. Nat. Sci. Sleep 2020, 12, 821–842. [Google Scholar] [CrossRef] [PubMed]
- Kinnunen, H.; Rantanen, A.; Kentta, T.; Koskimaki, H. Feasible Assessment of Recovery and Cardiovascular Health: Accuracy of Nocturnal HR and HRV Assessed via Ring PPG in Comparison to Medical Grade ECG. Physiol. Meas. 2020, 41, 04NT01. [Google Scholar] [CrossRef]
- Stone, J.D.; Ulman, H.K.; Tran, K.; Thompson, A.G.; Halter, M.D.; Ramadan, J.H.; Stephenson, M.; Finomore, V.S.; Galster, S.M.; Rezai, A.R.; et al. Assessing the Accuracy of Popular Commercial Technologies That Measure Resting Heart Rate and Heart Rate Variability. Front. Sports Act. Living 2021, 3, 37. [Google Scholar] [CrossRef]
- de Zambotti, M.; Rosas, L.; Colrain, I.M.; Baker, F.C. The Sleep of the Ring: Comparison of the OURA sleep tracker against polysomnography. Behav. Sleep Med. 2019, 17, 124–136. [Google Scholar] [CrossRef] [PubMed]
- Cao, R.; Azimi, I.; Sarhaddi, F.; Niela-Vilen, H.; Axelin, A.; Liljeberg, P.; Rahmani, A.M. Accuracy Assessment of Oura Ring Nocturnal Heart Rate and Heart Rate Variability in Comparison With Electrocardiography in Time and Frequency Domains: Comprehensive Analysis. J. Med. Internet. Res. 2022, 24, e27487. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Visible Red | NIR |
|---|---|---|
| Wavelength | 660 ± 25 nm | 850 ± 30 nm |
| LED Quantity | 1200 | 1200 |
| Power per LED | 0.267 W | 0.267 W |
| Irradiance (at patient skin) | 0.012 W/cm2 | 0.012 W/cm2 |
| Total Emitted Power | 321 W | 321 W |
| Treatment Time | 1200 s | 1200 s |
| Energy Emitted | 385,056 J | 385,056 J |
| Fluence | 14.4 J/cm2 | 14.4 J/cm2 |
| Variable | Pre | Post | Mean Difference | p-Value | d | |
|---|---|---|---|---|---|---|
| Physiology | Average HR (bpm) | 54.31 | 53.31 | 0.996 (0.300, 1.691) | 0.0055 * | 0.175 |
| Average HRV (ms) | 100.46 | 103.73 | −3.269 (−6.899, 0.362) | 0.0770 | 0.251 | |
| Average RR (rpm) | 16.85 | 16.80 | 0.058 (−0.094, 0.210) | 0.4504 | 0.022 | |
| Sleep | Total Sleep Time (h) | 7.93 | 7.29 | 0.635 (0.282, 0.989) | 0.0006 * | 0.156 |
| Awake Time (h) | 1.35 | 1.28 | 0.070 (−0.061, 0.200) | 0.2935 | 0.028 | |
| Sleep Efficiency (%) | 85.65 | 85.13 | 0.516 (−0.602, 1.634) | 0.3616 | 0.071 | |
| Light Duration (h) | 4.62 | 4.30 | 0.322 (0.031, 0.613) | 0.0307 * | 0.087 | |
| Deep Duration (h) | 2.24 | 2.12 | 0.114 (−0.030, 0.258) | 0.1188 | 0.044 | |
| REM Duration (h) | 1.07 | 0.87 | 0.200 (0.075, 0.324) | 0.0019 * | 0.083 | |
| % Light | 57.84 | 58.70 | −0.862 (−3.178, 1.453) | 0.4614 | 0.083 | |
| % Deep | 28.97 | 29.90 | −0.933 (−3.109, 1.243) | 0.3966 | 0.092 | |
| % REM | 13.21 | 11.41 | 1.798 (0.41, 3.185) | 0.0117 * | 0.223 |
| Outcome Measure | Fixed Effect | F | df | p-Value |
|---|---|---|---|---|
| Average HR | Night | 8.18 | 1, 90.7 | 0.0052 * |
| TST | 0.41 | 1, 102.4 | 0.5254 | |
| Night*TST | 0.59 | 1, 102.7 | 0.4451 | |
| Average HRV | Night | 6.43 | 1, 89.0 | 0.0130 * |
| TST | 6.09 | 1, 98.5 | 0.0153 * | |
| Night*TST | 3.05 | 1, 98.8 | 0.0839 | |
| Average RR | Night | 1.05 | 1, 88.9 | 0.3090 |
| TST | 0.86 | 1, 93.0 | 0.3552 | |
| Night*TST | 0.01 | 1, 93.1 | 0.9051 |
| Single-Day PL | 4D Cumulative PL | ||||||
|---|---|---|---|---|---|---|---|
| Variable | Night | PL | Night*PL | Night | PL | Night*PL | |
| Physiology | Average HR (bpm) | 0.0643 | <0.0001 * | 0.0761 | 0.0089 * | 0.0132 * | 0.6472 |
| Average HRV (ms) | 0.1598 | 0.1793 | 0.1916 | 0.0912 | 0.5113 | 0.6187 | |
| Average RR (rpm) | 0.8956 | 0.0004 * | 0.0549 | 0.6076 | 0.0140 * | 0.6390 | |
| Sleep | Total Sleep Time (h) | 0.0003 * | 0.3309 | 0.0106 * | 0.0005 * | 0.1993 | 0.8867 |
| Awake Time (h) | 0.2438 | 0.4530 | 0.9029 | 0.2798 | 0.4659 | 0.9330 | |
| Sleep Efficiency (%) | 0.4060 | 0.7732 | 0.2514 | 0.3742 | 0.8003 | 0.8906 | |
| Light Duration (h) | 0.0299 * | 0.8949 | 0.0401 * | 0.0301 * | 0.7022 | 0.7982 | |
| Deep Duration (h) | 0.0881 | 0.3869 | 0.1862 | 0.1087 | 0.3192 | 0.5547 | |
| REM Duration (h) | 0.0016 * | 0.6175 | 0.2155 | 0.0018 * | 0.3259 | 0.7460 | |
| % Light | 0.4304 | 0.7136 | 0.9402 | 0.4461 | 0.5736 | 0.4394 | |
| % Deep | 0.4016 | 0.9552 | 0.4968 | 0.3929 | 0.8361 | 0.7182 | |
| % REM | 0.0098 * | 0.6314 | 0.2001 | 0.010 5 * | 0.3244 | 0.4464 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rentz, L.E.; Bryner, R.W.; Ramadan, J.; Rezai, A.; Galster, S.M. Full-Body Photobiomodulation Therapy Is Associated with Reduced Sleep Durations and Augmented Cardiorespiratory Indicators of Recovery. Sports 2022, 10, 119. https://doi.org/10.3390/sports10080119
Rentz LE, Bryner RW, Ramadan J, Rezai A, Galster SM. Full-Body Photobiomodulation Therapy Is Associated with Reduced Sleep Durations and Augmented Cardiorespiratory Indicators of Recovery. Sports. 2022; 10(8):119. https://doi.org/10.3390/sports10080119
Chicago/Turabian StyleRentz, Lauren E., Randy W. Bryner, Jad Ramadan, Ali Rezai, and Scott M. Galster. 2022. "Full-Body Photobiomodulation Therapy Is Associated with Reduced Sleep Durations and Augmented Cardiorespiratory Indicators of Recovery" Sports 10, no. 8: 119. https://doi.org/10.3390/sports10080119
APA StyleRentz, L. E., Bryner, R. W., Ramadan, J., Rezai, A., & Galster, S. M. (2022). Full-Body Photobiomodulation Therapy Is Associated with Reduced Sleep Durations and Augmented Cardiorespiratory Indicators of Recovery. Sports, 10(8), 119. https://doi.org/10.3390/sports10080119