

The Anesthesiologic Impact of Single-Port Robot-Assisted Partial Nephrectomy: A Tertiary Referral Comparative Analysis Between Full-Flank Transperitoneal, Retroperitoneal, and Supine Lower Anterior Access (LAA)

 , ,
, ,  ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Overview
2.2. Intraoperative Anesthesia Protocol
2.3. Surgical Technique
2.4. Perioperative Clinical Pathway
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Klatte, T.; Ficarra, V.; Gratzke, C.; Kaouk, J.; Kutikov, A.; Macchi, V.; Mottrie, A.; Porpiglia, F.; Porter, J.; Rogers, C.G.; et al. A Literature Review of Renal Surgical Anatomy and Surgical Strategies for Partial Nephrectomy. Eur. Urol. 2015, 68, 980–992. [Google Scholar] [CrossRef]
- Bertolo, R.; Ditonno, F.; Veccia, A.; De Marco, V.; Migliorini, F.; Porcaro, A.B.; Rizzetto, R.; Cerruto, M.A.; Autorino, R.; Antonelli, A.; et al. Postoperative outcomes of transperitoneal versus retroperitoneal robotic partial nephrectomy: A propensity-score matched comparison focused on patient mobilization, return to bowel function, and pain. J. Robot. Surg. 2024, 18, 96. [Google Scholar] [CrossRef]
- Porpiglia, F.; Mari, A.; Amparore, D.; Fiori, C.; Antonelli, A.; Artibani, W.; Bove, P.; Brunocilla, E.; Capitanio, U.; Da Pozzo, L.; et al. Transperitoneal vs retroperitoneal minimally invasive partial nephrectomy: Comparison of perioperative outcomes and functional follow-up in a large multi-institutional cohort (The RECORD 2 Project). Surg. Endosc. 2021, 35, 4295–4304. [Google Scholar] [CrossRef]
- Fu, J.; Ye, S.; Ye, H. Retroperitoneal Versus Transperitoneal Laparoscopic Partial Nephrectomy: A Systematic Review Meta-analysis. Chin. Med. Sci. J. 2015, 30, 239–244. [Google Scholar] [CrossRef]
- Arora, S.; Heulitt, G.; Menon, M.; Jeong, W.; Ahlawat, R.K.; Capitanio, U.; Moon, D.A.; Maes, K.K.; Rawal, S.; Mottrie, A.; et al. Retroperitoneal vs Transperitoneal Robot-assisted Partial Nephrectomy: Comparison in a Multi-institutional Setting. Urology 2018, 120, 131–137. [Google Scholar] [CrossRef]
- Zillioux, J.M.; Krupski, T.L. Patient positioning during minimally invasive surgery: What is current best practice? Robot. Surg. 2017, 4, 69–76. [Google Scholar] [CrossRef]
- Mertens zur Borg, I.R.A.M.; Lim, A.; Verbrugge, S.J.C.; IJzermans, J.N.M.; Klein, J. Effect of intraabdominal pressure elevation and positioning on hemodynamic responses during carbon dioxide pneumoperitoneum for laparoscopic donor nephrectomy: A prospective controlled clinical study. Surg. Endosc. 2004, 18, 919–923. [Google Scholar] [CrossRef]
- Mills, J.T.; Burris, M.B.; Warburton, D.J.; Conaway, M.R.; Schenkman, N.S.; Krupski, T.L. Positioning injuries associated with robotic assisted urological surgery. J. Urol. 2013, 190, 580–584. [Google Scholar] [CrossRef]
- Okhawere, K.E.; Beksac, A.T.; Wilson, M.P.; Korn, T.G.; Meilika, K.N.; Harrison, R.; Morgantini, L.S.; Ahmed, M.; Mehrazin, R.; Abaza, R.; et al. A Propensity-Matched Comparison of the Perioperative Outcomes Between Single-Port and Multi-Port Robotic Assisted Partial Nephrectomy: A Report from the Single Port Advanced Research Consortium (SPARC). J. Endourol. 2022, 36, 1526–1531. [Google Scholar] [CrossRef]
- Fan, G.; Wang, J.; Wang, Y.; Chen, Y.; Wu, Y.; Cai, S.; Li, Y.; Tang, T. Comparative short-term efficacy and safety analysis of a single-port robot in nephrectomy. J. Robot. Surg. 2025, 19, 175. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, A.A.; Chen, G.; Morgantini, L.; Calvo, R.S.; Crivellaro, S. Simplifying Retroperitoneal Robotic Single-port Surgery: Novel Supine Anterior Retroperitoneal Access. Eur. Urol. 2023, 84, 223–228. [Google Scholar] [CrossRef]
- Rohi, A.; Olofsson, M.E.T.; Jakobsson, J.G. Ambulatory anesthesia and discharge: An update around guidelines and trends. Curr. Opin. Anaesthesiol. 2022, 35, 691–697. [Google Scholar] [CrossRef]
- Campbell, S.C.; Uzzo, R.G.; Karam, J.A.; Chang, S.S.; Clark, P.E.; Souter, L. Renal Mass and Localized Renal Cancer: Evaluation, Management, and Follow-up: AUA Guideline: Part II. J. Urol. 2021, 206, 209–218. [Google Scholar] [CrossRef]
- Assel, M.; Sjoberg, D.; Elders, A.; Wang, X.; Huo, D.; Botchway, A.; Delfino, K.; Fan, Y.; Zhao, Z.; Koyama, T.; et al. Guidelines for Reporting of Statistics for Clinical Research in Urology. Eur. Urol. 2019, 75, 358–367. [Google Scholar] [CrossRef]
- Pandolfo, S.D.; Cerrato, C.; Wu, Z.; Franco, A.; Del Giudice, F.; Sciarra, A.; Verze, P.; Lucarelli, G.; Imbimbo, C.; Perdonà, S.; et al. A systematic review of robot-assisted partial nephrectomy outcomes for advanced indications: Large tumors (cT2-T3), solitary kidney, completely endophytic, hilar, recurrent, and multiple renal tumors. Asian J. Urol. 2023, 10, 390–406. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ng, A.M.; Shah, P.H.; Kavoussi, L.R. Laparoscopic Partial Nephrectomy: A Narrative Review and Comparison with Open and Robotic Partial Nephrectomy. J. Endourol. 2017, 31, 976–984. [Google Scholar] [CrossRef]
- Calpin, G.G.; Ryan, F.R.; McHugh, F.T.; McGuire, B.B. Comparing the outcomes of open, laparoscopic and robot-assisted partial nephrectomy: A network meta-analysis. BJU Int. 2023, 132, 353–364. [Google Scholar] [CrossRef]
- Tameze, Y.; Low, Y.H. Outpatient Robotic surgery: Considerations for the Anesthesiologist. Adv. Anesth. 2022, 40, 15–32. [Google Scholar] [CrossRef]
- Nadu, A.; Ekstein, P.; Szold, A.; Friedman, A.; Nakache, R.; Cohen, Y.; Matzkin, H.; Weinbroum, A.A. Ventilatory and hemodynamic changes during retroperitoneal and transperitoneal laparoscopic nephrectomy: A prospective real-time comparison. J. Urol. 2005, 174, 1013–1017. [Google Scholar] [CrossRef]
- Peng, C.; Shen, H.; Cao, S.; Wu, S.; Huang, Q.; Li, S.; Li, H.Z.; Zhang, X.; Wang, B.; Cao, J.; et al. Effects of Retroperitoneal or Transperitoneal Pneumoperitoneum on Inferior Vena Cava Hemodynamics and Cardiopulmonary Function: A Prospective Real-Time Comparison. J. Endourol. 2023, 37, 28–34. [Google Scholar] [CrossRef]
- Garg, M.; Singh, V.; Sinha, R.J.; Sharma, P. Prospective randomized comparison of transperitoneal vs retroperitoneal laparoscopic simple nephrectomy. Urology 2014, 84, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Lambertini, L.; Pacini, M.; Morgantini, L.; Smith, J.; Torres-Anguiano, J.R.; Crivellaro, S. The atlas of supine single port extraperitoneal access. Int. Braz. J. Urol. 2024, 50, 783–784. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, C.J.; Steyn, W.H.; Boon, J.M. Segmental nerve damage during a McBurney’s incision: A cadaveric study. Surg. Radiol. Anat. 2004, 26, 66–69. [Google Scholar] [CrossRef] [PubMed]
- Lambertini, L.; Pacini, M.; Calvo, R.S.; Anguiano, J.R.T.; Cannoletta, D.; Pettenuzzo, G.; DI Maida, F.; Valastro, F.; Mari, A.; Bignante, G.; et al. Retroperitoneal single port vs. transperitoneal multiport robot assisted partial nephrectomy in patients with highly hostile abdomen: Comparative analysis from a tertiary care center. Minerva Urol. Nephrol. 2025, 77, 209–216. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristic | Overall, N = 105 1 | Surgical Approach | p-Value 2 | |||
|---|---|---|---|---|---|---|
| Transperitoneal Access N = 25 1 | Retroperitoneal Flank Access N = 42 1 | Lower Anterior Access N = 38 1 | ||||
| Age (years), median (IQR) | 59 (1–69) | 60 (47–66) | 61.50 (52.5–69.8) | 58.00 (52–64.8) | 0.6 | |
| BMI (kg/m2), median (IQR) | 30.14 (26.3–36.5) | 31.30 (25.1–38.3) | 30.12 (26.1–36.6) | 29.86 (25.2–37.8) | 0.9 | |
| Male gender, n (%) | 59 (56%) | 16 (64%) | 25 (60%) | 18 (47%) | 0.4 | |
| CCI, median (IQR) | 3 (2–4) | 3 (2–4) | 3 (2–4) | 3 (2–4) | 0.7 | |
| Substance abuse, n (%) | 17 (16%) | 5 (20%) | 6 (14%) | 6 (16%) | 0.8 | |
| Hypertension, n (%) | 73 (70%) | 17 (68%) | 30 (71%) | 26 (68%) | 0.9 | |
| Hypercholesterolemia, n (%) | 37 (35%) | 5 (20%) | 16 (38%) | 16 (42%) | 0.2 | |
| COPD, n (%) | 32 (30%) | 6 (24%) | 14 (33%) | 12 (32%) | 0.7 | |
| Diabetes, n (%) | 33 (31%) | 9 (36%) | 15 (36%) | 9 (24%) | 0.4 | |
| Obesity, n (%) | 55 (52%) | 14 (56%) | 22 (52%) | 19 (50%) | 0.9 | |
| Anticoagulant therapy, n (%) | 20 (19%) | 8 (32%) | 7 (17%) | 5 (13%) | 0.2 | |
| ASA, median (IQR) | 3 (2–4) | 2 (2–3) | 3(2–3) | 3 (2–4) | 0.10 | |
| Abdominal surgery, n (%) | 45 (43%) | 11 (44%) | 18 (43%) | 16 (42%) | >0.9 | |
| Preoperative Hb (g/dL), median (IQR) | 13.0 (9.2–16.8) | 13.2 (9.8–16.7) | 13.0 (10.1–15.2) | 12.9 (10.6–14.2) | 0.6 | |
| Preoperative eGFR (mL/min/1.72 m2), median (IQR) | 76.0 (57–97.2) | 78.0 (47.8–86.6) | 76.8 (45.2–81.4) | 71.0 (58.5–87.2) | 0.9 | |
| Clinical T stage, n (%) | 0.4 | |||||
| cT1a | 75 (71.4) | 17 (76.0) | 31 (76.2) | 27 (73.6) | ||
| cT1b | 20 (22.9) | 4 (16.0) | 8 (19.0) | 8 (21.1) | ||
| cT2a | 8 (5.7) | 2 (8.0) | 3 (4.8) | 3 (5.3) | ||
| Renal nephrometry score, median (IQR) | 7 (4–7) | 6 (4–7) | 7 (5–8) | 7 (6–8) | 0.07 | |
| Characteristic | Overall, N = 105 1 | Surgical Approach | p-Value 2 | |||
|---|---|---|---|---|---|---|
| Transperitoneal Access N = 25 1 | Retroperitoneal Flank Access N = 42 1 | Lower Anterior Access N = 38 1 | ||||
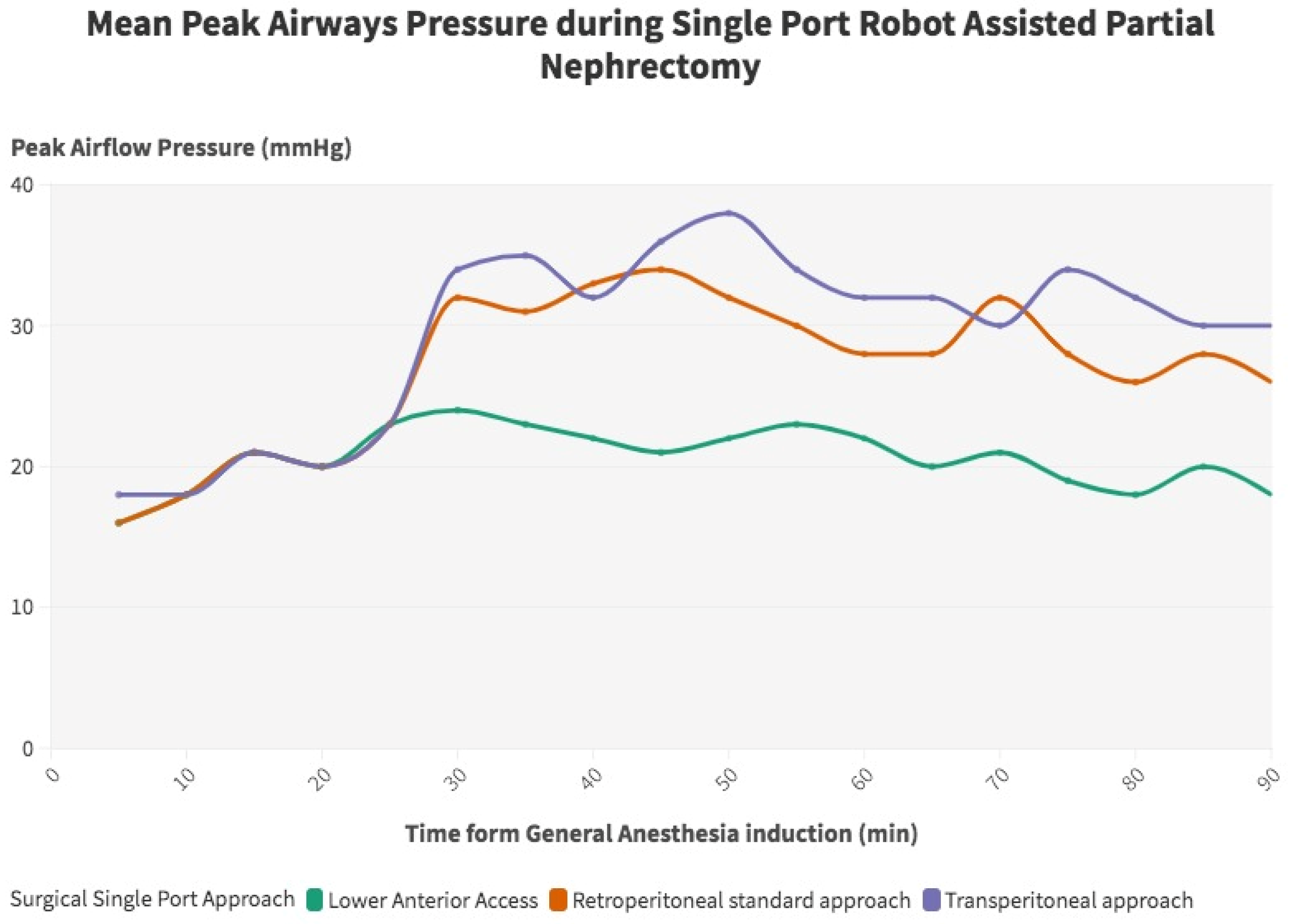
| Peak inspiratory pressure (cm H2O), median (IQR) | 26 (22–36) | 28 (24–34) | 26.0 (22–34) | 20 (16–26) | 0.03 | |
| Induction | 16 (10–20) | 16 (9–16) | 14 (9–16) | 0.2 | ||
| 30 min | 34 (24–36) | 32 (24–34) | 24 (14–24) | 0.02 | ||
| 60 min | 32 (24–34) | 28 (26–32) | 22 (14–24) | 0.03 | ||
| 90 min | 30 (24–34) | 26 (26–34) | 18 (14–24) | 0.04 | ||
| 120 min | 30 (26–38) | 28 (24–28) | 18 (14–26) | 0.03 | ||
| 150 min | 32 (24–36) | 28 (22–30) | 20 (16–24) | 0.04 | ||
| EtCO2, median (IQR) | 37 (31–42) | 37 (30–44) | 37 (32–39) | 34 (28–38) | 0.2 | |
| SpO2, median (IQR) | 99 (97–100) | 98 (96–99) | 99 (98–100) | 99 (98–100) | 0.7 | |
| Systolic blood pressure (mmHg), median (IQR) | 123 (98–136) | 136 (102–146) | 123 (96–136) | 118 (96–130) | 0.03 | |
| Diastolic blood pressure (mmHg), median (IQR) | 71 (50–90) | 82 (64–100) | 70.50 (52–88) | 67.50 (54–92) | 0.04 | |
| Mean blood pressure (mmHg), median (IQR) | 97 (74–120) | 105 (82–123) | 95 (73–115) | 93 (72–118) | 0.04 | |
| Intraoperative opioid administration *, median (IQR) | 12 (10–18) | 14 (12–20) | 14 (12–18) | 10 (6–12) | 0.023 | |
| Postoperative pain score, median (IQR) | 4 (3–6) | 5 (3–7) | 5 (4–6) | 3 (2–4) | 0.001 | |
| Opioid use on 0 or 1 PO day, n (%) | 62 (59.0) | 18 (72.1) | 31 (73.8) | 13 (34.2) | 0.001 | |
| Total Intravenous Anesthesia (TIVA), n (%) | 5 (4.8) | 1 (4) | 2 (4.8) | 2 (5.2) | 0.2 | |
| Characteristic | Overall, N = 105 1 | Surgical Approach | p-Value 2 | ||
|---|---|---|---|---|---|
| Transperitoneal Access N = 25 1 | Retroperitoneal Flank Access N = 42 1 | Lower Anterior Access N = 38 1 | |||
| Operative time (min), median (IQR) | 184 (81) | 218 (75) | 190 (95) | 169 (45) | 0.012 |
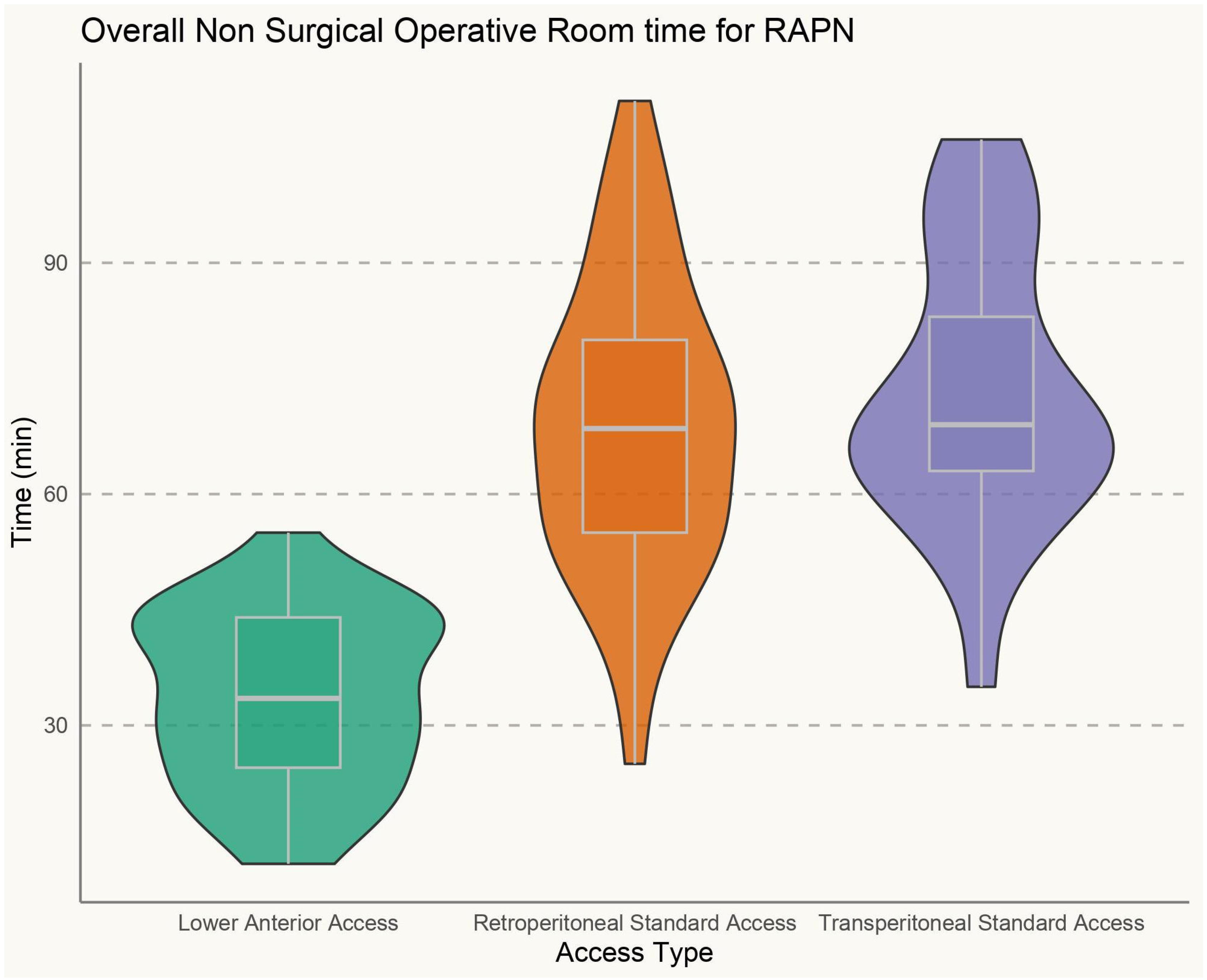
| Non-surgical OR time (min), median (IQR) | 51 (39–71) | 54 (45–76) | 54 (42–73) | 41 (35–62) | 0.003 |
| EBL (cc), median (IQR) | 50 (42.5–200) | 50 (35–200) | 70 (50–100) | 90 (50–150) | 0.2 |
| Ischemia time (min), median (IQR) | 19 (17–24) | 21 (15–28) | 22 (14–32) | 21.5 (19.2–31) | 0.07 |
| Intraoperative complications, n (%) | 4 (3.8) | 3 (12) | 1 (2.4) | 0 (0) | 0.057 |
| Drainage placement, n (%) | 21(20) | 13 (52) | 8 (19) | 0 (0) | <0.001 |
| Successful same day discharge, n (%) | 58 (55) | 4 (16) | 22 (52) | 32 (84) | <0.001 |
| Postoperative complications, n (%) | 9 (8.6) | 4 (16) | 4 (9.5) | 1 (2.6) | 0.2 |
| Length of hospital stay (days), median (IQR) | 1 (0–2) | 1 (1–2) | 0 (0–2) | 0 (0–1) | <0.001 |
| Failure to meet SSD criteria, n (%) | 27 (25.7) | 17 (68) | 16 (38) | 5 (13.2) | <0.001 |
| 90-day remediation rate, n (%) | 20 (19) | 5 (20) | 6 (14) | 9 (24) | 0.6 |
| 90-day readmission rate, n (%) | 8 (7.6) | 1 (4.0) | 3 (7.1) | 2 (5.2) | 0.7 |
| Follow-up (months), median (IQR) | 16.00 (6–24) | 18.00 (9–24) | 16.00 (6–24) | 12.00 (3–18) | 0.07 |
| Significant renal function loss at last follow-up, n (%) | 43 (41) | 9 (36) | 19 (45) | 15 (39) | 0.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lambertini, L.; Pacini, M.; Polverino, P.; Wilkinson, N.R.; Calvo, R.S.; Cannoletta, D.; Pellegrino, A.A.; Pettenuzzo, G.; Di Maida, F.; Mari, A.; et al. The Anesthesiologic Impact of Single-Port Robot-Assisted Partial Nephrectomy: A Tertiary Referral Comparative Analysis Between Full-Flank Transperitoneal, Retroperitoneal, and Supine Lower Anterior Access (LAA). J. Pers. Med. 2025, 15, 306. https://doi.org/10.3390/jpm15070306
Lambertini L, Pacini M, Polverino P, Wilkinson NR, Calvo RS, Cannoletta D, Pellegrino AA, Pettenuzzo G, Di Maida F, Mari A, et al. The Anesthesiologic Impact of Single-Port Robot-Assisted Partial Nephrectomy: A Tertiary Referral Comparative Analysis Between Full-Flank Transperitoneal, Retroperitoneal, and Supine Lower Anterior Access (LAA). Journal of Personalized Medicine. 2025; 15(7):306. https://doi.org/10.3390/jpm15070306
Chicago/Turabian StyleLambertini, Luca, Matteo Pacini, Paolo Polverino, Nikki R. Wilkinson, Ruben Sauer Calvo, Donato Cannoletta, Antony Angelo Pellegrino, Greta Pettenuzzo, Fabrizio Di Maida, Andrea Mari, and et al. 2025. "The Anesthesiologic Impact of Single-Port Robot-Assisted Partial Nephrectomy: A Tertiary Referral Comparative Analysis Between Full-Flank Transperitoneal, Retroperitoneal, and Supine Lower Anterior Access (LAA)" Journal of Personalized Medicine 15, no. 7: 306. https://doi.org/10.3390/jpm15070306
APA StyleLambertini, L., Pacini, M., Polverino, P., Wilkinson, N. R., Calvo, R. S., Cannoletta, D., Pellegrino, A. A., Pettenuzzo, G., Di Maida, F., Mari, A., Bignante, G., Lasorsa, F., Zucchi, A., Serni, S., Minervini, A., Glick, D. B., & Crivellaro, S. (2025). The Anesthesiologic Impact of Single-Port Robot-Assisted Partial Nephrectomy: A Tertiary Referral Comparative Analysis Between Full-Flank Transperitoneal, Retroperitoneal, and Supine Lower Anterior Access (LAA). Journal of Personalized Medicine, 15(7), 306. https://doi.org/10.3390/jpm15070306