
Pleural Empyema in Spain (2016–2022): A Nationwide Study on Trends in Hospitalizations, Mortality, and Impact of Comorbidities

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Statistical Analysis
2.2. Ethics
3. Results
3.1. Empyema as Primary or Secondary Diagnosis
3.2. Analysis of In-Hospital Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Foley, S.P.F.; Parrish, J.S. Pleural Space Infections. Life 2023, 13, 376. [Google Scholar] [CrossRef]
- McCauley, L.; Dean, N. Pneumonia and empyema: Causal, casual or unknown. Thorac Dis. 2015, 7, 992. [Google Scholar]
- Asai, N.; Ohashi, W.; Shibata, Y.; Sakanashi, D.; Kato, H.; Hagihara, M.; Suematsu, H.; Mikamo, H. A 15-Year Observational Cohort of Acute Empyema at a Single-Center in Japan. Antibiotics 2024, 13, 1205. [Google Scholar] [CrossRef] [PubMed]
- Ferreiro, L.; San José, M.E.; Valdés, L. Management of Parapneumonic Pleural Effusion in Adults. Arch. Bronconeumol. 2015, 51, 637–646. [Google Scholar] [CrossRef] [PubMed]
- Bobbio, A.; Bouam, S.; Frenkiel, J.; Zarca, K.; Fournel, L.; Canny, E.; Icard, P.; Porcher, R.; Alifano, M. Epidemiology and prognostic factors of pleural empyema. Thorax 2021, 76, 1117–1123. [Google Scholar] [CrossRef]
- Burgos, J.; Falcó, V.; Pahissa, A. The increasing incidence of empyema. Curr. Opin. Pulm. Med. 2013, 19, 350–356. [Google Scholar] [CrossRef]
- Merchant, N.; Liu, C. Thoracic empyema: Aetiology, diagnosis, treatment, and prevention. Curr. Opin. Pulm. Med. 2024, 30, 204–209. [Google Scholar] [CrossRef]
- Zhong, M.; Ni, R.; Zhang, H.; Sun, Y. Analysis of clinical characteristics and risk factors of community-Acquired pneumonia complicated by parapneumonic pleural effusion in elderly patients. BMC Pulm. Med. 2023, 23, 355. [Google Scholar] [CrossRef]
- Marks, D.J.B.; Fisk, M.D.; Koo, C.Y.; Pavlou, M.; Peck, L.; Lee, S.F.; Lawrence, D.; Macrae, M.B.; Wilson, A.P.R.; Brown, J.S.; et al. Thoracic empyema: A 12-year study from a UK tertiary cardiothoracic referral centre. PLoS ONE 2012, 7, e30074. [Google Scholar] [CrossRef]
- Bartlett, J.G. Anaerobic bacterial infections of the lung and pleural space. Clin. Infect. Dis. 1993, 16, 248–255. [Google Scholar] [CrossRef]
- Boyanova, L.; Djambazov, V.; Gergova, G.; Iotov, D.; Petrov, D.; Osmanliev, D.; Minchev, Z.; Mitov, I. Anaerobic microbiology in 198 cases of pleural empyema: A Bulgarian study. Anaerobe 2004, 10, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Alfageme, I.; Muñoz, F.; Peña, N.; Umbría, S. Empyema of the thorax in adults: Etiology, microbiologic findings, and management. Chest 1993, 103, 839–843. [Google Scholar] [CrossRef] [PubMed]
- Shen, K.R.; Bribriesco, A.; Crabtree, T.; Denlinger, C.; Eby, J.; Eiken, P.; Jones, D.R.; Keshavjee, S.; Maldonado, F.; Paul, S. The American Association for Thoracic Surgery consensus guidelines for the management of empyema. Thorac. Cardiovasc. Surg. 2017, 153, e129–e146. [Google Scholar] [CrossRef] [PubMed]
- Iguina, M.M.; Sharma, S. Thoracic Empyema. In StatPearls; Danckers, M., Ed.; StatPearls Publishing: Treasure Island, FL, USA, 2025. Available online: http://www.ncbi.nlm.nih.gov/books/NBK544279/ (accessed on 4 May 2025).
- Reichert, M.; Hecker, M.; Witte, B.; Bodner, J.; Padberg, W.; Weigand, M.A.; Hecker, A. Stage-Directed therapy of pleural empyema. Langenbeck’s Arch. Surg. 2017, 402, 15–26. [Google Scholar] [CrossRef]
- Báez-Saldaña, R.; Molina-Corona, H.; Martínez-Rendón, M.E.; Iñiguez-García, M.; Escobar-Rojas, A.; Fortoul-Vandergoes, T. Parapneumonic effusion and thoracic empyema in adults. Clinical aspects, microbiology and frequency of surgical outcome. Cirugía Y Cir. 2021, 89, 63–70. [Google Scholar] [CrossRef]
- Chan, K.P.F.; Ma, T.F.; Sridhar, S.; Lam, D.C.L.; Ip, M.S.M.; Ho, P.L. Changes in Etiology and Clinical Outcomes of Pleural empyema during the COVID-19 Pandemic. Microorganisms 2023, 11, 303. [Google Scholar] [CrossRef]
- Haggie, S.; Gunasekera, H.; Pandit, C.; Selvadurai, H.; Robinson, P.; Fitzgerald, D.A. Paediatric empyema: Worsening disease severity and challenges identifying patients at increased risk of repeat intervention. Arch. Dis. Child. 2020, 105, 886–890. [Google Scholar] [CrossRef]
- Arnold, D.T.; Hamilton, F.W.; Morris, T.T.; Suri, T.; Morley, A.; Frost, V.; Vipond, I.B.; Medford, A.R.; Payne, R.A.; Muir, P. Epidemiology of pleural empyema in English hospitals and the impact of influenza. Eur. Respir. 2021, 57, 2003546. [Google Scholar] [CrossRef]
- Ho, C.H.; Chen, Y.C.; Chu, C.C.; Wang, J.J.; Liao, K.M. Age-adjusted Charlson comorbidity score is associated with the risk of empyema in patients with COPD. Medicine 2017, 96, e8040. [Google Scholar] [CrossRef]
- Eryigit, H.; Orki, A.; Unaldi, M.; Ozdemir, A.; Orki, T.; Kosar, A.; Demirhan, R.; Arman, B. Accelerated treatment of concomitant empyema and lung cancer by video-assisted thoracoscopic surgery. Cir. Esp. 2016, 94, 100–104. [Google Scholar] [CrossRef]
- Redden, M.D.; Chin, T.Y.; Driel, M.L.V. Surgical versus non-surgical management for pleural empyema. Cochrane Database Syst. Rev. 2017, 2, 303. [Google Scholar] [CrossRef] [PubMed]
- Mummadi, S.R.; Stoller, J.K.; Lopez, R.; Kailasam, K.; Gillespie, C.T.; Hahn, P.Y. Epidemiology of Adult Pleural Disease in the United States. Chest 2021, 160, 1534–1551. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.H.; Lee, S.H.; Kim, K.T.; Jung, J.S.; Son, H.S.; Sun, K. Optimal Timing of Thoracoscopic Drainage and Decortication for Empyema. Ann. Thorac. Surg. 2014, 97, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Semmelmann, A.; Baar, W.; Haude, H.; Moneke, I.; Loop, T. Risk Factors for Postoperative Pulmonary Complications Leading to Increased Morbidity and Mortality in Patients Undergoing Thoracic Surgery for Pleural Empyema. Cardiothorac Vasc Anesth. 2023, 37, 1659–1667. [Google Scholar] [CrossRef]
- Tamiya, H.; Jo, T.; Yokoyama, A.; Sakamoto, Y.; Mitani, A.; Tanaka, G.; Matsui, H.; Ishimaru, M.; Yasunaga, H.; Nagase, T. Reduction in the need for surgery and mortality after early administration of fibrinolytics following empyema drainage. Eur. Cardio-Thorac. Surg. 2024, 66, ezae263. [Google Scholar] [CrossRef]
- Arnold, D.T.; Tucker, E.; Morley, A.; Milne, A.; Stadon, L.; Patole, S.; Nava, G.W.; Walker, S.P.; Maskell, N.A. A feasibility randomised trial comparing therapeutic thoracentesis to chest tube insertion for the management of pleural infection: Results from the ACTion trial. BMC Pulm. Med. 2022, 22, 330. [Google Scholar] [CrossRef]
- Sundaralingam, A.; Grabczak, E.M.; Burra, P.; Costa, M.I.; George, V.; Harriss, E.; Jankowska, E.A.; Janssen, J.P.; Karpathiou, G.; Laursen, C.B. ERS statement on benign pleural effusions in adults. Eur. Respir. 2024, 64, 2302307. [Google Scholar] [CrossRef]

{kind=link}
| 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | Total | p-Value | ||
|---|---|---|---|---|---|---|---|---|---|---|
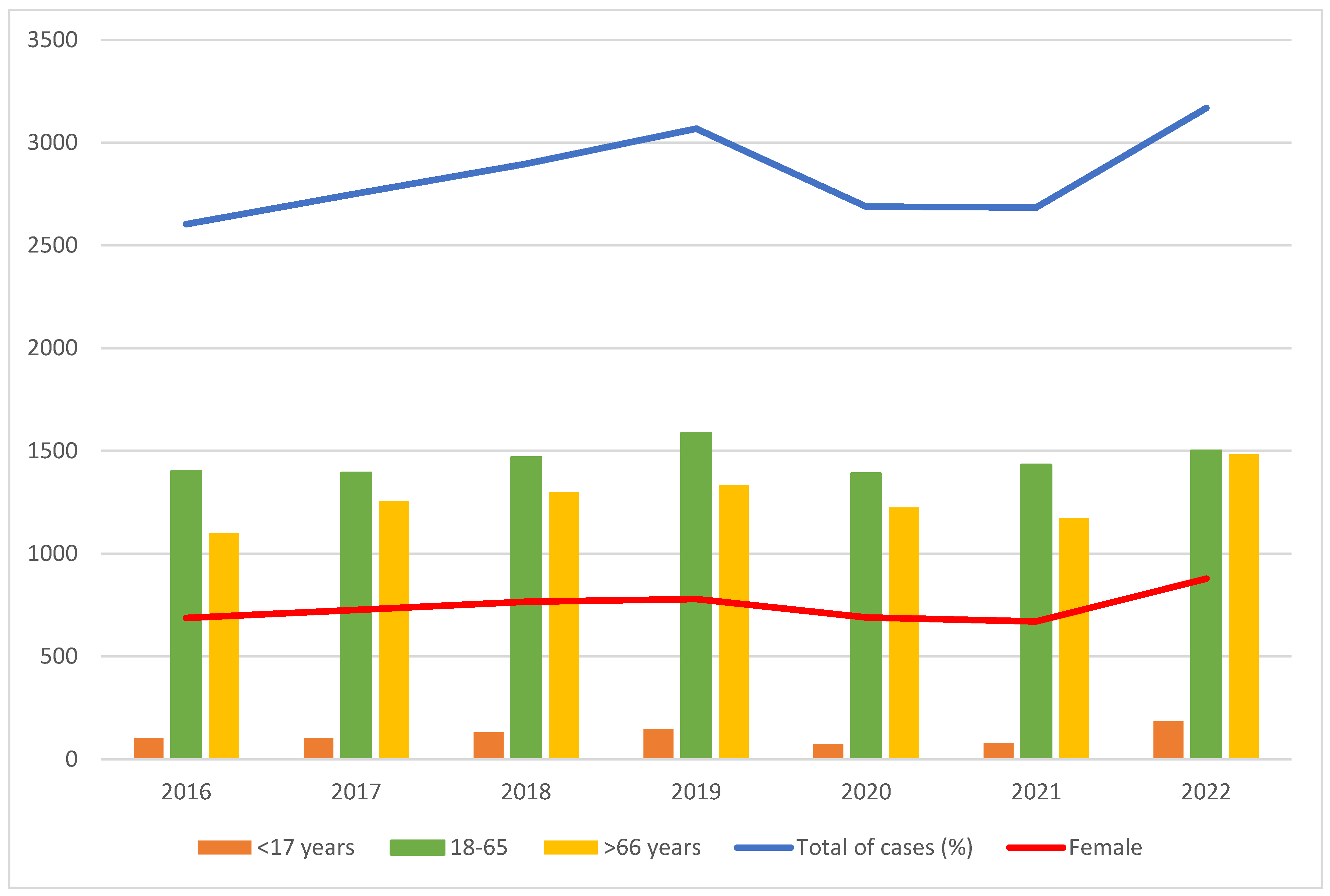
| Total PE cases | 2604 | 2752 | 2897 | 3068 | 2689 | 2685 | 3169 | 19,864 | ||
| Total admission | 4,394,207 | 4,562,182 | 4,529,107 | 4,560,089 | 4,032,912 | 4,316,158 | 4,485,352 | 30,880,007 | ||
| PE per 1000 admissions | 0.59 | 0.60 | 0.64 | 0.67 | 0.67 | 0.62 | 0.71 | 0.64 | <0.001 | |
| Female sex (%) | 687 (26.4) | 726 (26.4) | 766 (26.4) | 779 (25.4) | 689 (25.6) | 670 (25) | 878 (27.7) | 5195 (26.15) | 0.274 | |
| Mean age (SD) | 60 (19) | 61 (19) | 60 (20) | 60 (20) | 61 (18) | 61 (18) | 61 (21) | 61 (19) | 0.033 | |
| Age group (%) | ≤17 | 104 (4) | 104 (3.8) | 131 (4.5) | 148 (4.8) | 75 (2.8) | 80 (3) | 185 (6) | 827 (4.2) | <0.001 |
| 18–65 | 1401 (53.8) | 1393 (50.6) | 1468 (50.7) | 1586 (51.7) | 1389 (51.7) | 1432 (53.3) | 1501 (47.4) | 10170 (51.2) | ||
| ≥66 | 1099 (42.2) | 1255 (45.6) | 1298 (44.8) | 1334 (43.5) | 1225 (45.6) | 1173 (43.7) | 1483 (46.8) | 8867 (44.6) | ||
| PE as primary diagnosis (%) | 1039 (40) | 1056 (38) | 1064 (37) | 1106 (36) | 986 (37) | 969 (36) | 1140 (36) | 7360 (37) | 0.017 | |
| CCI categories (%) | ≤1 | 1754 (67) | 1824 (66) | 1972 (68) | 2010 (66) | 1761 (66) | 1688 (63) | 2059 (65) | 13068 (66) | 0.006 |
| 2 | 362 (14) | 371 (14) | 360 (12) | 399 (13) | 353 (13) | 388 (14) | 417 (13) | 2650 (13) | ||
| ≥3 | 488 (19) | 557 (20) | 565 (20) | 659 (21) | 575 (21) | 609 (23) | 693 (22) | 4146 (21) | ||
| Mean CCI (SD) | 1.6 (2.5) | 1.6 (2.5) | 1.6 (2.4) | 1.7 (2.6) | 1.7 (2.5) | 1.8 (2.6) | 1.7 (2.5) | 1.7 (2.5) | <0.001 | |
| Pneumonia | 412 (15.8) | 445 (16.2) | 479 (16.5) | 471 (15.4) | 369 (13.7) | 337 (12.6) | 496 (15.7) | 3009 (15.2) | <0.001 | |
| Sepsis | 76 (3) | 113 (4) | 105 (3.6) | 135 (4.4) | 97 (3.6) | 100 (3.7) | 123 (4) | 749 (3.8) | 0.129 | |
| Pneumococcal sepsis | 25 (1) | 19 (0.7) | 42 (1.5) | 50 (1.6) | 22 (0.8) | 16 (0.6) | 35 (1.1) | 209 (1) | <0.001 | |
| COVID-19 | - | - | - | - | 40 (1.5) | 88 (3.2) | 87 (2.7) | 215 (1) | <0.001 | |
| Pleural drainage (%) | 1262 (88) | 1315 (88) | 1374 (91) | 1427 (91) | 1236 (92) | 1167 (93) | 1333 (93) | 9114 (91) | <0.001 | |
| Lung cancer | 21 (0.8) | 24 (0.9) | 12 (0.4) | 19 (0.6) | 10 (0.4) | 15 (0.6) | 18 (0.6) | 119 (0.6) | 0.149 | |
| Hospital ward (%) | Medical | 1869 (72) | 2026 (74) | 2190 (76) | 2296 (75) | 2021 (75) | 1991 (74) | 2366 (75) | 14759 (74) | 0.009 |
| Surgical | 637 (24) | 618 (22) | 592 (20) | 677 (22) | 573 (21) | 570 (21) | 690 (22) | 4357 (22) | ||
| ICU | 96 (4) | 100 (4) | 112 (4) | 90 (3) | 90 (3) | 112 (4) | 103 (3) | 703 (4) | ||
| Others | 2 (0.1) | 8 (0.3) | 3 (0.1) | 5 (0.2) | 11 (0.4) | 11 (0.4) | 7 (0.2) | 40 (0.2) | ||
| Severity | Low | 3 (0.1) | 4 (0.2) | 3 (0.1) | 6 (0.2) | 2 (0.1) | 4 (0.1) | 5 (0.2) | 27 (0.1) | <0.001 |
| Moderate | 130 (5) | 127 (4.6) | 100 (3.5) | 120 (3.9) | 108 (4) | 95 (3.5) | 142 (4.5) | 822 (4) | ||
| High | 1673 (64) | 1655 (60) | 1797 (62) | 1893 (62) | 1569 (58) | 1470 (55) | 1907 (60) | 11964 (60) | ||
| Extreme | 778 (30) | 954 (34.7) | 989 (34) | 1040 (34) | 1007 (37) | 1112 (41) | 1113 (35) | 6993 (35) | ||
| Mean LOS (SD) days | 19.7 (20) | 20.2 (23) | 19.6 (20) | 20.2 (24) | 20.6 (21) | 20.8 (25) | 20 (23) | 20 (22) | 0.074 | |
| In-hospital mortality (%) | 287 (11) | 289 (10.5) | 283 (9.8) | 304 (9.9) | 286 (10.6) | 333 (12.4) | 350 (11) | 2132 (11) | 0.035 | |
| Mean cost (EUR) | 886.53 | 876.92 | 920.78 | 909.94 | 1083.88 | 995.10 | 938.18 | 943.44 | <0.001 | |
| Primary Diagnosis N (%) | Secondary Diagnosis N (%) | p-Value | ||
|---|---|---|---|---|
| Total | 7360 | 12504 | ||
| Year | 2016 | 68 (15) | 219 (13) | 0.809 |
| 2017 | 60 (13) | 229 (14) | ||
| 2018 | 61 (13) | 222 (13) | ||
| 2019 | 62 (14) | 242 (14) | ||
| 2020 | 53 (12) | 233 (14) | ||
| 2021 | 76 (17) | 257 (15) | ||
| 2022 | 73 (16) | 277 (17) | ||
| Female sex | 116 (26) | 454 (27) | 0.541 | |
| Mean age (SD) | 74 (13) | 70 (14) | <0.001 | |
| Age group (%) | ≤17 | - | 9 (0.5) | 0.007 |
| 18–65 | 123 (27) | 567 (34) | ||
| ≥66 | 330 (73) | 1103 (66) | ||
| Mean CCI (SD) | 1.4 (2.3) | 1.8 (2.6) | <0.001 | |
| Charlson commorbidity index (%) | ≤1 | 5204 (71) | 7864 (63) | <0.001 |
| 2 | 908 (12) | 1742 (14) | ||
| ≥3 | 1248 (17) | 2898 (23) | ||
| Hospital ward (%) | Medical | 369 (81) | 1068 (64) | <0.001 |
| Surgical | 46 (10) | 170 (10) | ||
| ICU | 37 (8) | 435 (26) | ||
| Others | 1 (0.2) | 6 (0.4) | ||
| Pneumonia (%) | - | 3369 (27) | ||
| Sepis (%) | - | 749 (6) | ||
| Lung abscess (%) | - | 253 (2) | ||
| Lung Cancer (%) | - | 220 (2) | ||
| COVID-19 (%) | - | 215 (2) | ||
| Pneumococcal bacteremia (%) | - | 209 (1.6) | ||
| COPD (%) | - | 161 (1) | ||
| Aspiration pneumonia (%) | - | 143 (1) | ||
| Pleural drainage (%) | 242 (86) | 487 (79) | 0.011 | |
| Severity (%) | Low | - | 1(0.1) | <0.001 |
| Moderate | 4 (1) | 13(1) | ||
| High | 300 (66) | 399 (24) | ||
| Extreme | 149 (33) | 1252 (75) | ||
| Mean LOS (SD) | 10 (4–19) | 15 (6–30) | <0.001 | |
| Mortality | 453 (6.2) | 1679 (13.4) | <0.001 | |
| Mean cost (EUR) | 912.07 (363.7) | 1030.35 (436.7) | <0.001 | |
| In-Hospital Mortality | ||||
|---|---|---|---|---|
| Primary Diagnosis | Secondary Diagnosis | Any Position | ||
| aOR (95%CI) p Value | aOR (95%CI) p Value | aOR (95%CI) | ||
| Year | 1.01 (0.94–1.07) 0.751 | 0.98 (0.93–1.03) 0.592 | 0.99 (0.95–1.03) 0.831 | |
| Female sex | 1.26 (0.94–1.69) 0.111 | 1.18 (0.94–1.47) 0.137 | 1.20 (1.01–1.44) 0.034 | |
| Age | ≤17 (reference) | 1 | 1 | 1 |
| 18–65 | 0.34 (0.25–0.46) <0.001 | 12.30 (1.68–89.56) 0.013 | 13.45 (1.85–97.29) 0.010 | |
| ≥66 | - | 30.22 (4.15–219.89) 0.001 | 34.74(4.80–251.01) <0.001 | |
| CCI | ≤1 (reference) | 1 | 1 | 1 |
| 2 | 2.13 (1.49–3.05) <0.001 | 2.52 (1.91–3.32) <0.001 | 2.40 (1.93–2.98) <0.001 | |
| ≥3 | 3.64 (2.72–4.87) <0.001 | 4.39 (3.51–5.49) <0.001 | 4.22 (3.54–5.03) <0.001 | |
| Hospital ward | Medical | - | 0.71 (0.13–3.74) 0.688 | 0.77 (0.15–3.89) 0.752 |
| Surgical | 0.30 (0.18–0.50) <0.001 | 0.32 (0.05–1.77) 0.194 | 0.29 (0.05–1.52) 0.145 | |
| ICU | 6.93 (2.86–16.75) <0.001 | 9.38 (1.70–51.68) 0.010 | 9.29 (1.77–48.82) 0.008 | |
| COVID-19 | - | 1.57 (0.67–3.69) 0.296 | 1.61 (0.68–3.77) 0.270 | |
| Pneumonia | - | 0.63 (0.47–0.84) 0.002 | 0.67 (0.51–0.89) 0.006 | |
| Lung cancer | - | 2.46 (1.32–4.58) 0.005 | 2.93 (1.58–5.44) 0.001 | |
| Sepsis | - | 1.68 (1.22–2.31) 0.001 | 1.74 (1.27–2.38) <0.001 | |
| Pleural drainage | 0.52 (0.35–0.77) 0.001 | 0.46 (0.35–0.60) <0.001 | 0.45 (0.37–0.56) <0.001 | |
| Severity | Low (reference) | 1 | 1 | 1 |
| Moderate | - | 0.82 (0.17–3.84) 0.807 | 0.49 (0.11–2.25) 0.366 | |
| High | 0.24 (0.17–0.33) <0.001 | 0.55 (0.15–2.01) 0.347 | 0.43 (0.12–1.56) 0.204 | |
| Extreme | - | 1.45 (0.40–5.22) 0.568 | 1.40 (0.39–5.05) 0.602 | |
| LOS | <10 days | 2.67 (2.03–3.49) <0.001 | 2.34 (1.90–2.89) <0.001 | 2.40 (2.04–2.83) <0.001 |
| ≥10 days (reference) | 1 | 1 | 1 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perez-de-Paz, B.; Fernandez-Cotarelo, M.-J.; Rodriguez-Romero, L.; Ribeiro-Neves-Pinto, C.; Quilez-Ruiz-Rico, N.; Álvaro-Álvarez, D.; Moreno-Cuerda, V.; Henriquez-Camacho, C. Pleural Empyema in Spain (2016–2022): A Nationwide Study on Trends in Hospitalizations, Mortality, and Impact of Comorbidities. J. Pers. Med. 2025, 15, 263. https://doi.org/10.3390/jpm15070263
Perez-de-Paz B, Fernandez-Cotarelo M-J, Rodriguez-Romero L, Ribeiro-Neves-Pinto C, Quilez-Ruiz-Rico N, Álvaro-Álvarez D, Moreno-Cuerda V, Henriquez-Camacho C. Pleural Empyema in Spain (2016–2022): A Nationwide Study on Trends in Hospitalizations, Mortality, and Impact of Comorbidities. Journal of Personalized Medicine. 2025; 15(7):263. https://doi.org/10.3390/jpm15070263
Chicago/Turabian StylePerez-de-Paz, Begoña, Maria-Jose Fernandez-Cotarelo, Lydia Rodriguez-Romero, Carolina Ribeiro-Neves-Pinto, Natividad Quilez-Ruiz-Rico, Dolores Álvaro-Álvarez, Victor Moreno-Cuerda, and Cesar Henriquez-Camacho. 2025. "Pleural Empyema in Spain (2016–2022): A Nationwide Study on Trends in Hospitalizations, Mortality, and Impact of Comorbidities" Journal of Personalized Medicine 15, no. 7: 263. https://doi.org/10.3390/jpm15070263
APA StylePerez-de-Paz, B., Fernandez-Cotarelo, M.-J., Rodriguez-Romero, L., Ribeiro-Neves-Pinto, C., Quilez-Ruiz-Rico, N., Álvaro-Álvarez, D., Moreno-Cuerda, V., & Henriquez-Camacho, C. (2025). Pleural Empyema in Spain (2016–2022): A Nationwide Study on Trends in Hospitalizations, Mortality, and Impact of Comorbidities. Journal of Personalized Medicine, 15(7), 263. https://doi.org/10.3390/jpm15070263