
Spinal Arachnoid Cysts: A Single-Center Preliminary Surgical Experience with a Rare and Challenging Disease

 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
Data Collection
3. Results
3.1. Patients Overview
3.2. Radiological Data
3.3. Surgical Details and Post-Operative Outcomes
3.4. Illustrative Cases
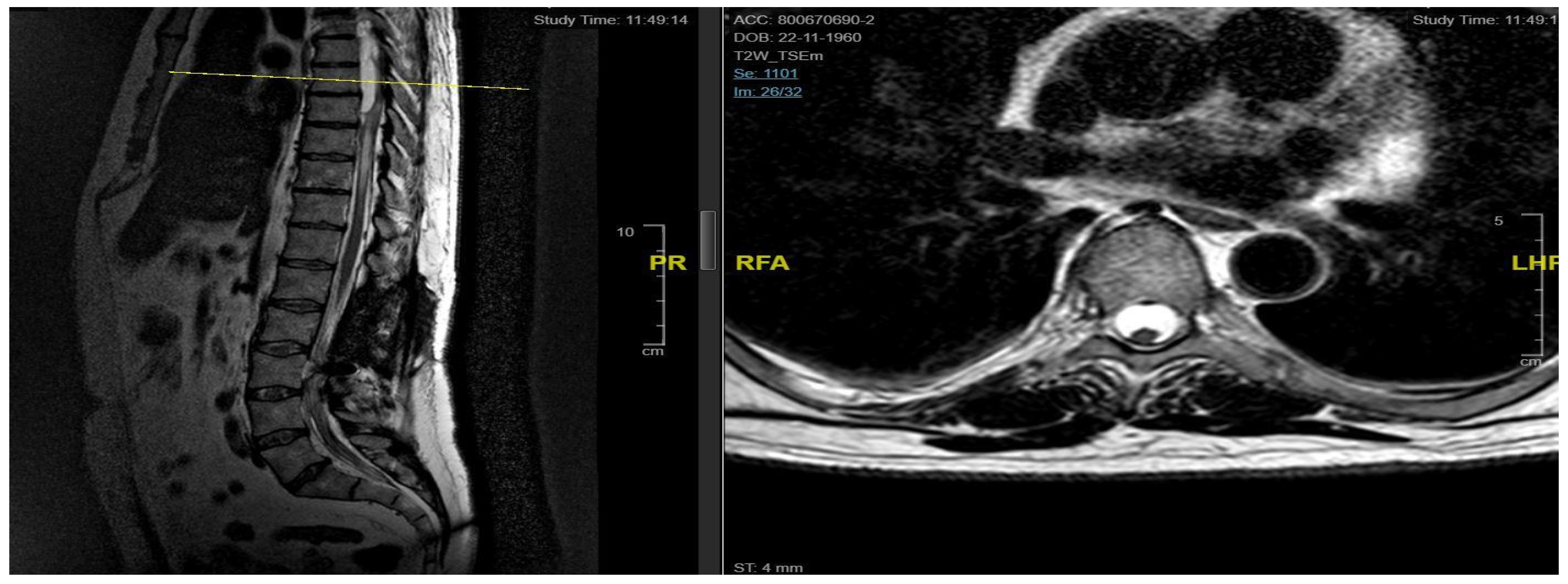
3.4.1. Case 1
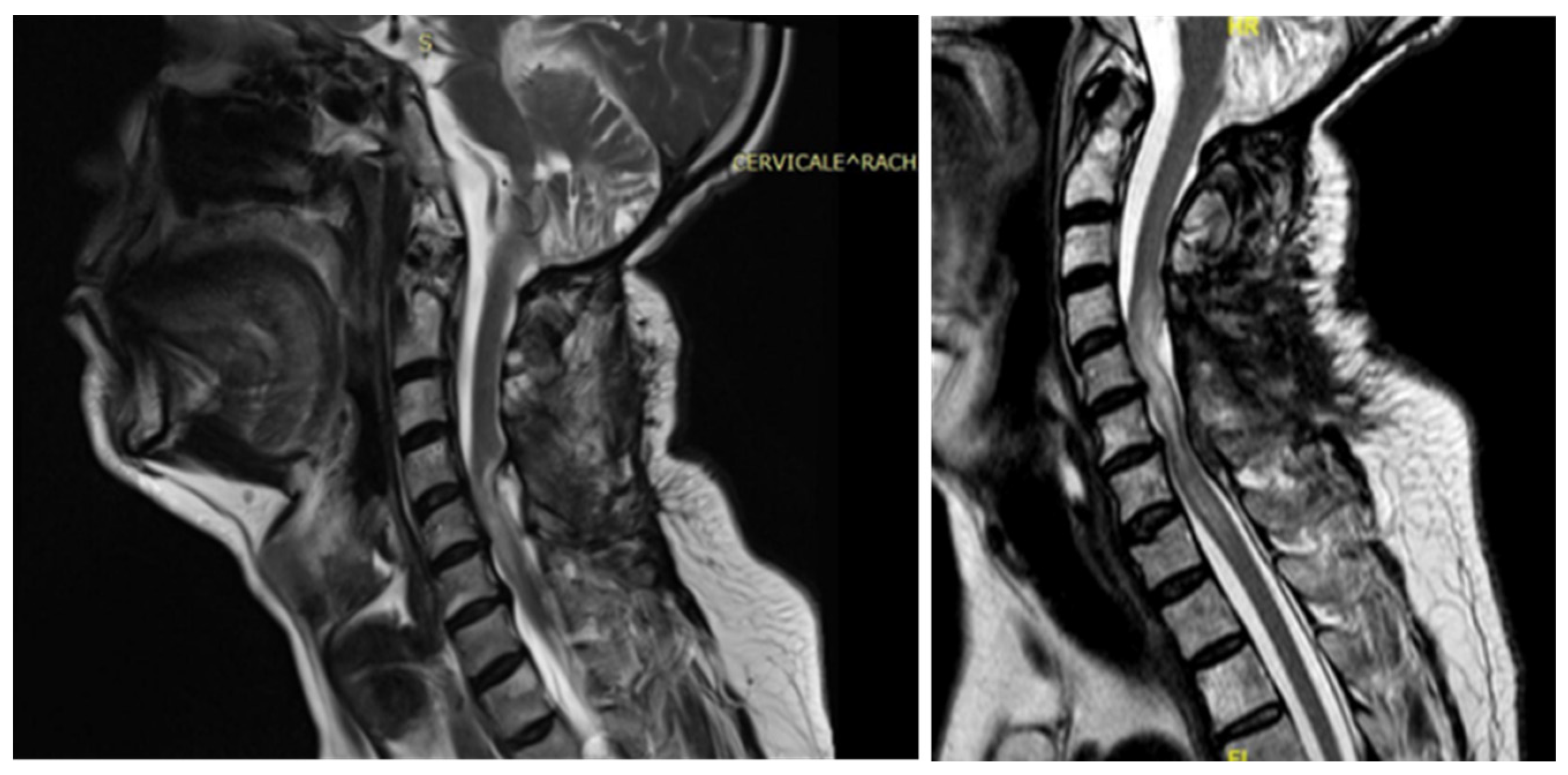
3.4.2. Case 2
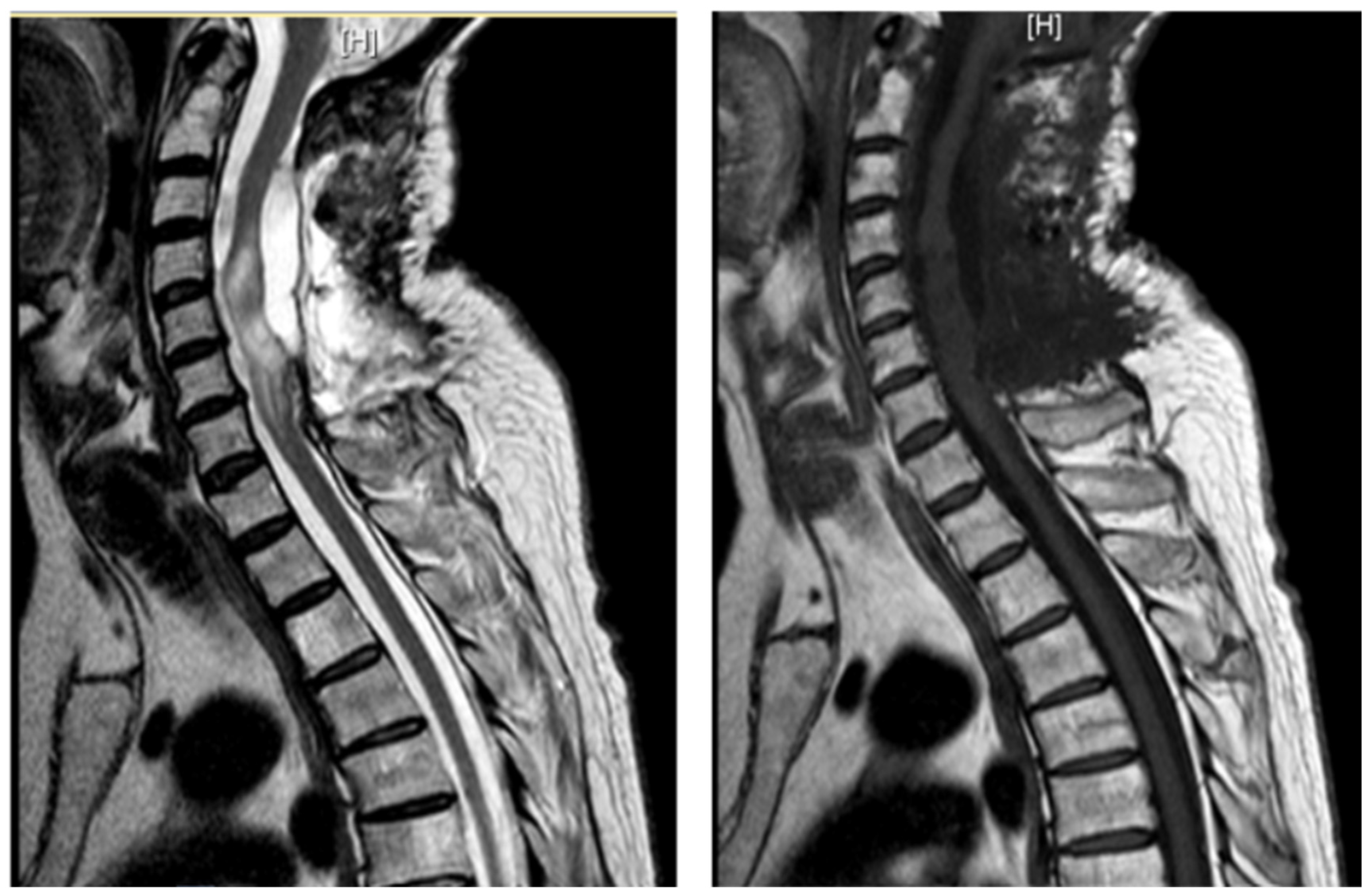
3.4.3. Case 3
3.4.4. Case 4
3.4.5. Case 5
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MRI | magnetic resonance imaging |
| CT | computed tomography |
| NRS | numeric rating scale for pain |
References
- Eroglu, U.; Bozkurt, M.; Kahilogullari, G.; Dogan, I.; Ozgural, O.; Shah, K.J.; Zaimoglu, M.; Al-Beyati, E.S.; Ugur, H.C.; Cohen-Gadol, A.A. Surgical Management of Spinal Arachnoid Cysts in Adults. World Neurosurg. 2019, 122, e1146–e1152. [Google Scholar] [CrossRef] [PubMed]
- Epstein, N.E. Review/Perspective on the Diagnosis and Surgical Management of Spinal Arachnoid Cysts. Surg. Neurol. Int. 2022, 13, 98. [Google Scholar] [CrossRef] [PubMed]
- Naito, K.; Yamagata, T.; Ohata, K.; Takami, T. Safety and Efficacy of Syringoperitoneal Shunting with a Programmable Shunt Valve for Syringomyelia Associated with Extensive Spinal Adhesive Arachnoiditis: Technical Note. World Neurosurg. 2019, 132, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.; Behr, S.; Shaw, T.; Cappello, R.; Jeffery, N.; Liebel, F.X.; Harcourt-Brown, T. Surgical techniques used in the management of intra-arachnoid diverticula in dogs across four referral centres and their immediate outcome. J. Small Anim. Pract. 2022, 63, 520–525. [Google Scholar] [CrossRef] [PubMed]
- Abou Fakhr, F.S.; Kanaan, S.V.; Youness, F.M.; Hourani, M.H.; Haddad, M.C. Thoracic spinal intradural arachnoid cyst: Report of two cases and review of literature. Eur. Radiol. 2002, 12, 877–882. [Google Scholar] [CrossRef]
- Andrews, B.T.; Weinstein, P.R.; Rosenblum, M.L.; Barbaro, N.M. Intradural arachnoid cysts of the spinal canal associated with intramedullary cysts. J. Neurosurg. 1988, 68, 544–549. [Google Scholar] [CrossRef]
- Nabors, M.W.; Pait, T.G.; Byrd, E.B.; Karim, N.O.; Davis, D.O.; Kobrine, A.I.; Rizzoli, H.V. Updated assessment and current classification of spinal meningeal cysts. J. Neurosurg. 1988, 68, 366–377. [Google Scholar] [CrossRef]
- Viswanathan, V.K.; Manoharan, S.R.; Do, H.; Minnema, A.; Shaddy, S.M.; Elder, J.B.; Farhadi, H.F. Clinical and Radiologic Outcomes After Fenestration and Partial Wall Excision of Idiopathic Intradural Spinal Arachnoid Cysts Presenting with Myelopathy. World Neurosurg. 2017, 105, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Bassiouni, H.; Hunold, A.; Asgari, S.; Hübschen, U.; König, H.J.; Stolke, D. Spinal Intradural Juxtamedullary Cysts in the Adult: Surgical Management and Outcome. Neurosurgery 2004, 55, 1352–1359. [Google Scholar] [CrossRef] [PubMed]
- Klekamp, J. A New Classification for Pathologies of Spinal Meninges—Part 2: Primary and Secondary Intradural Arachnoid Cysts. Neurosurgery 2017, 81, 217–229. [Google Scholar] [CrossRef]
- Mitsuyama, T.; Asamoto, S.; Kawamata, T. Novel surgical management of spinal adhesive arachnoiditis by arachnoid microdissection and ventriculo–subarachnoid shunting. J. Clin. Neurosci. 2011, 18, 1702–1704. [Google Scholar] [CrossRef] [PubMed]
- Fukumoto, H.; Samura, K.; Katsuta, T.; Miki, K.; Fukuda, K.; Inoue, T. Extensive Multilocular Spinal Extradural Meningeal Cyst That Developed 16 Years After Traumatic Brachial Plexus Injury: A Case Report. World Neurosurg. 2016, 86, 510.e5–510.e10. [Google Scholar] [CrossRef]
- Fam, M.D.; Woodroffe, R.W.; Helland, L.; Noeller, J.; Dahdaleh, N.S.; Menezes, A.H.; Hitchon, P.W. Spinal arachnoid cysts in adults: Diagnosis and management. A single-center experience. J. Neurosurg. Spine 2018, 29, 711–719. [Google Scholar] [CrossRef]
- Sadek, A.R.; Nader-Sepahi, A. Spinal Arachnoid Cysts: Presentation, management and pathophysiology. Clin. Neurol. Neurosurg. 2019, 180, 87–96. [Google Scholar] [CrossRef]
- Wang, M.Y.; Levi, A.D.O.; Green, B.A. Intradural spinal arachnoid cysts in adults. Surg. Neurol. 2003, 60, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Fortuna, A.; La Torre, E.; Ciappetta, P. Arachnoid diverticula: A unitary approach to spinal cysts communicating with the subarachnoid space. Acta Neurochir. 1977, 39, 259–268. [Google Scholar] [CrossRef]
- Kendall, B.E.; Valentine, A.R.; Keis, B. Spinal arachnoid cysts: Clinical and radiological correlation with prognosis. Neuroradiology 1982, 22, 225–234. [Google Scholar] [CrossRef]
- Leclerc, A.; Matveeff, L.; Emery, E. Syringomyelia and hydromyelia: Current understanding and neurosurgical management. Rev. Neurol. 2021, 177, 498–507. [Google Scholar] [CrossRef]
- Iacoangeli, A.; Alsagheir, M.; Aiudi, D.; Gladi, M.; Di Rienzo, A.; Esposito, D.P.; Diab, M.; Naas, H.; Eldellaa, A.; Gigante, A.; et al. Microendoscopic Tailored Spine Decompression as a Less-Invasive, Stability-Preserving Surgical Option to Instrumented Correction in Complex Spine Deformities: A Preliminary Multicenter Experience. World Neurosurg. 2024, 186, e142–e150. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Cho, W.H.; Han, I.H.; Choi, B.K. Large Thoracolumbar Extradural Arachnoid Cyst Excised by Minimal Skipped Hemilaminectomy: A Case Report. Korean J. Spine 2013, 10, 28–31. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mirza, A.B.; Bartram, J.; Sinha, S.; Gebreyohanes, A.; Boardman, T.; Vastani, A.; Dyson, E.; Lavrador, J.P.; Russo, V.; Choi, D.; et al. Surgical management and outcomes in spinal intradural arachnoid cysts: The experience from two tertiary neurosurgical centres. Acta Neurochir. 2022, 164, 1217–1228. [Google Scholar] [CrossRef]
- Kalsi, P.; Hejrati, N.; Charalampidis, A.; Wu, P.H.; Schneider, M.; Wilson, J.R.; Gao, A.F.; Massicotte, E.M.; Fehlings, M.G. Spinal arachnoid cysts: A case series & systematic review of the literature. Brain Spine 2022, 2, 100904. [Google Scholar] [CrossRef] [PubMed]
- Moses, Z.B.; Friedman, G.N.; Penn, D.L.; Solomon, I.H.; Chi, J.H. Intradural spinal arachnoid cyst resection: Implications of duraplasty in a large case series. J. Neurosurg. Spine 2018, 28, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.B.; Wang, D.H.; Deng, S.L. Symptomatic secondary spinal arachnoid cysts: A systematic review. Spine J. 2023, 23, 1199–1211. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, Y.; Hida, K.; Koyanagi, I.; Abe, H. Reevaluation of Syringosubarachnoid Shunt for Syringomyelia with Chiari Malformation. Neurosurgery 2000, 46, 407–412. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criteria Type | Criteria |
|---|---|
| Inclusion |
|
| |
| |
| |
| Exclusion |
|
| |
|
| Patient | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Age | 46 | 48 | 62 | 43 | 68 |
| Gender | M | M | M | F | F |
| Level | T12–L2 | C5–C6 | T7–T10 | T8–T9 | T8–T11 |
| Location | Intramedullary | Intradural | Intradural–Extradural | Intramedullary | Intradural |
| Primary/secondary | Secondary | Secondary | Secondary | Secondary | Secondary |
| Numbness | Yes | No | Yes | Yes | Yes |
| Gait disturbances/ataxia | No | Yes | No | Yes | Yes |
| Lumbar pain | No | No | Yes | Yes | No |
| Urinary–bowel dysfunction | Yes | No | Yes | No | No |
| Limb weakness | Yes | Yes | No | No | No |
| Paraplegia | No | No | Yes | No | No |
| Sexual disfunction | Yes | No | No | No | No |
| Surgical treatment | lysis of adherences and syrinx cavity opening | resection of the cystic formation and adhesiolysis | resection of the cystic formation and adhesiolysis | resection of the cystic formation and adhesiolysis | resection of the cystic formation and adhesiolysis |
| Complications | CSF fistula | infection | None | CSF fistula | None |
| KPS pre-op (%) | 70 | 50 | 70 | 80 | 90 |
| KPS post-op (%) | 80 | 50 | 60 | 90 | 80 |
| ASIA score pre-op | C | B | B | C | D |
| ASIA score post-op | D | B | C | C | D |
| Follow-up (years) | 2 | 2 | 2 | 3 | 1 |
| Viswanathan et al. [8] | Bassiouni et al. [9] | Klekamp et al. [10] | Eroglu et al. [1] | Mitsuyama et al. [11] | |
|---|---|---|---|---|---|
| Patients | 14 | 21 | 21 | 13 | 1 |
| Level | C7-L1 | D1-D12 | C7-L5 | T1-T12 | T8-T11 |
| Location | Intradural | Intradural | Intradural | Intra and extradural | Intradural |
| Primary/secondary | primary | complete | primary/secondary | primary/secondary | primary |
| Surgical treatment | cyst fenestration and partial wall resection through a posterior approach | resection of the cystic formation and adhesiolysis | cyst fenestration and partial wall resection through a posterior approach | resection of the cystic formation and adhesiolysis | Primary micro-dissection, ventriculo-subarachnoid shunt next |
| Complications | none | infection | CSF fistula | none | none |
| Neurological status | Improved/stableafter surgery | Improved/stableafter surgery | Improved in primarycysts/worsened insecondary cysts | Improved/stableafter surgery | Improved aftersurgery |
| Follow-up | 6 weeks | 3.2 years | 10 years | 55 months | 22 months |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iacoangeli, A.; Ilochonwu, L.C.; Mazzanti, G.; Polonara, G.; Ercolani, L.; Marini, A.; Luzi, M.; Trignani, R.; Bruni, S.; Barboni, E.; et al. Spinal Arachnoid Cysts: A Single-Center Preliminary Surgical Experience with a Rare and Challenging Disease. J. Pers. Med. 2025, 15, 234. https://doi.org/10.3390/jpm15060234
Iacoangeli A, Ilochonwu LC, Mazzanti G, Polonara G, Ercolani L, Marini A, Luzi M, Trignani R, Bruni S, Barboni E, et al. Spinal Arachnoid Cysts: A Single-Center Preliminary Surgical Experience with a Rare and Challenging Disease. Journal of Personalized Medicine. 2025; 15(6):234. https://doi.org/10.3390/jpm15060234
Chicago/Turabian StyleIacoangeli, Alessio, Love Chibuzor Ilochonwu, Giulia Mazzanti, Gabriele Polonara, Lauredana Ercolani, Alessandra Marini, Michele Luzi, Roberto Trignani, Stefano Bruni, Edoardo Barboni, and et al. 2025. "Spinal Arachnoid Cysts: A Single-Center Preliminary Surgical Experience with a Rare and Challenging Disease" Journal of Personalized Medicine 15, no. 6: 234. https://doi.org/10.3390/jpm15060234
APA StyleIacoangeli, A., Ilochonwu, L. C., Mazzanti, G., Polonara, G., Ercolani, L., Marini, A., Luzi, M., Trignani, R., Bruni, S., Barboni, E., Gladi, M., Iacoangeli, M., & Aiudi, D. (2025). Spinal Arachnoid Cysts: A Single-Center Preliminary Surgical Experience with a Rare and Challenging Disease. Journal of Personalized Medicine, 15(6), 234. https://doi.org/10.3390/jpm15060234