
Damage Control Interventional Radiology in Liver Trauma: A Comprehensive Review

 ,
,  ,
,  , ,
, ,
Abstract
1. Introduction
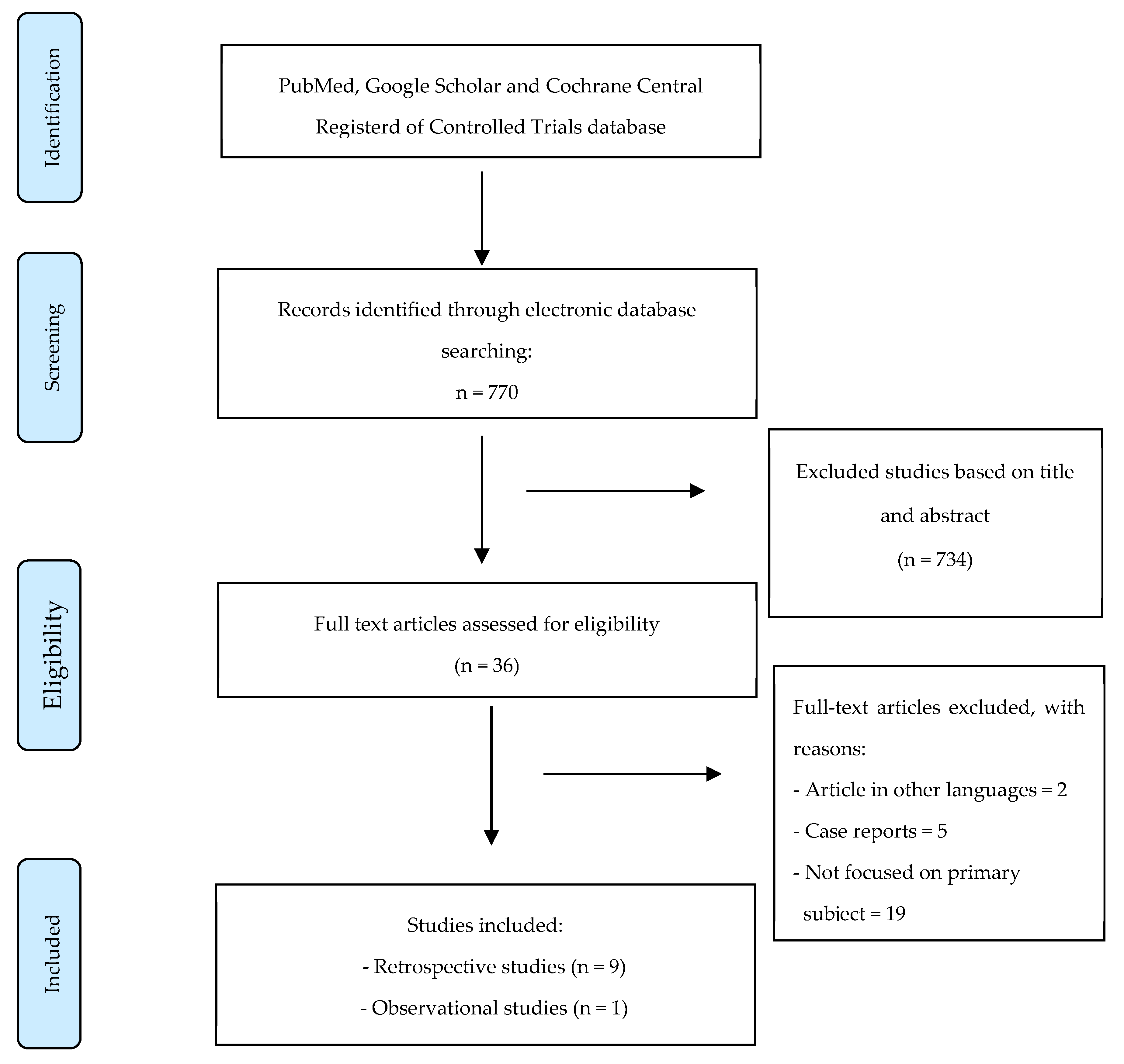
2. Materials and Methods
- -
- Hepatic bleeding from a traumatic cause, either blunt or penetrating;
- -
- Endovascular treatment used alone or in combination with surgical procedures to treat only hepatic injuries;
- -
- Description of the HD status of the patient, with a focus on articles where unstable patients were treated;
- -
- Evaluation of the outcomes after embolization.
- -
- Case reports;
- -
- Studies in which embolization for the treatment of liver bleeding was used in stable patients;
- -
- Studies in which the population was pediatric;
- -
- Studies where the endovascular treatment was used to treat non-traumatic liver injuries.
2.1. Outcomes
2.2. Data Extraction
3. Results
3.1. Patient Demographics
3.2. Hemodynamic Status
3.3. Mortality and Morbidity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Loggers, S.A.I.; Koedam, T.W.A.; Giannakopoulos, G.F.; Vandewalle, E.; Erwteman, M.; Zuidema, W.P. Definition of hemodynamic stability in blunt trauma patients: A systematic review and assessment amongst Dutch trauma team members. Eur. J. Trauma Emerg. Surg. 2017, 43, 823–833. [Google Scholar] [CrossRef]
- Matsushima, K.; Piccinini, A.; Schellenberg, M.; Cheng, V.; Heindel, P.; Strumwasser, A.; Benjamin, E.; Inaba, K.; Demetriades, D. Effect of door-to-angioembolization time on mortality in pelvic fracture: Every hour of delay counts. J. Trauma Acute Care Surg. 2018, 84, 685–692. [Google Scholar] [CrossRef]
- American College of Surgeons Committee on Trauma. Resources for Optimal Care of the Injured Patient. 2022. Available online: https://www.facs.org/quality-programs/trauma/quality/verification-review-and-consultation-program/standards/ (accessed on 2 November 2022).
- Mathew, J.K.; Fitzgerald, M.C. Damage Control Interventional Radiology (DCIR): Evolving Value of Interventional Radiology in Trauma. Cardiovasc. Interv. Radiol. 2022, 45, 1757–1758. [Google Scholar] [CrossRef]
- Clements, W.; Koukounaras, J.; Joseph, T. Reply to “Damage Control Interventional Radiology (DCIR): Evolving Value of In-terventional Radiology in Trauma”. Cardiovasc. Interv. Radiol. 2022, 45, 1759–1761. [Google Scholar] [CrossRef] [PubMed]
- Segalini, E.; Morello, A.; Leati, G.; Di Saverio, S.; Aseni, P. Primary angioembolization in liver trauma: Major hepatic necrosis as a severe complication of a minimally invasive treatment-a narrative review. Updates Surg. 2022, 74, 1511–1519. [Google Scholar] [CrossRef]
- Roberts, R.; Sheth, R.A. Hepatic Trauma. Ann. Transl. Med. 2021, 9, 1195. [Google Scholar] [CrossRef]
- Coccolini, F.; Panel, T.W.E.; Coimbra, R.; Ordonez, C.; Kluger, Y.; Vega, F.; Moore, E.E.; Biffl, W.; Peitzman, A.; Horer, T.; et al. Liver trauma: WSES 2020 guidelines. World J. Emerg. Surg. 2020, 15, 24. [Google Scholar] [CrossRef] [PubMed]
- Tamura, S.; Maruhashi, T.; Kashimi, F.; Kurihara, Y.; Masuda, T.; Hanajima, T.; Kataoka, Y.; Asari, Y. Transcatheter arterial embolization for severe blunt liver injury in hemodynamically unstable patients: A 15-year retrospective study. Scand. J. Trauma Resusc. Emerg. Med. 2021, 29, 66. [Google Scholar] [CrossRef] [PubMed]
- Aoki, M.; Abe, T.; Hagiwara, S.; Saitoh, D.; Oshima, K. Embolization versus Surgery for Stabilized Patients with Solid Organ Injury. J. Vasc. Interv. Radiol. 2021, 32, 1150–1155.e5. [Google Scholar] [CrossRef]
- Alnumay, A.; Caminsky, N.; Eustache, J.H.; Valenti, D.; Beckett, A.N.; Deckelbaum, D.; Fata, P.; Khwaja, K.; Razek, T.; McKendy, K.M.; et al. Feasibility of intraoperative angioembolization for trauma patients using C-arm digital subtraction angiography. Eur. J. Trauma Emerg. Surg. 2022, 48, 315–319. [Google Scholar] [CrossRef]
- Inukai, K.; Uehara, S.; Furuta, Y.; Miura, M. Nonoperative management of blunt liver injury in hemodynamically stable versus unstable patients: A retrospective study. Emerg. Radiol. 2018, 25, 647–652. [Google Scholar] [CrossRef]
- Otsuka, H.; Sato, T.; Sakurai, K.; Aoki, H.; Yamagiwa, T.; Iizuka, S.; Inokuchi, S. Use of interventional radiology as initial hemorrhage control to improve outcomes for potentially lethal multiple blunt injuries. Injury 2018, 49, 226–229. [Google Scholar] [CrossRef] [PubMed]
- Ogura, T.; Lefor, A.T.; Nakano, M.; Izawa, Y.; Morita, H. Nonoperative management of hemodynamically unstable abdominal trauma patients with angioembolization and resuscitative endovascular balloon occlusion of the aorta. J. Trauma Acute Care Surg. 2015, 78, 132–135. [Google Scholar] [CrossRef]
- Mitsusada, M.; Nakajima, Y.; Shirokawa, M.; Takeda, T.; Honda, H. Non-operative management of blunt liver injury: A new protocol for selected hemodynamically unstable patients under hypotensive resuscitation. J. Hepatobiliary Pancreat. Sci. 2014, 21, 205–211. [Google Scholar] [CrossRef]
- Di Saverio, S.; Catena, F.; Filicori, F.; Ansaloni, L.; Coccolini, F.; Keutgen, X.M.; Giugni, A.; Coniglio, C.; Biscardi, A.; Cavallo, P.; et al. Predictive factors of morbidity and mortality in grade IV and V liver trauma undergoing perihepatic packing: Single institution 14 years experience at European trauma centre. Injury 2012, 43, 1347–1354. [Google Scholar] [CrossRef]
- Misselbeck, T.S.; Teicher, E.J.; Cipolle, M.D.; Pasquale, M.D.; Shah, K.T.; Dangleben, D.A.; Badellino, M.M. Hepatic angioembolization in trauma patients: Indications and complications. J. Trauma 2009, 67, 769–773. [Google Scholar] [CrossRef]
- Monnin, V.; Sengel, C.; Thony, F.; Bricault, I.; Voirin, D.; Letoublon, C.; Broux, C.; Ferretti, G. Place of arterial embolization in severe blunt hepatic trauma: A multidisciplinary approach. Cardiovasc. Interv. Radiol. 2008, 31, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Moore, E.E.; Cogbill, T.H.; Jurkovich, G.J.; Shackford, S.R.; Malangoni, M.A.; Champion, H.R. Organ injury scaling Spleen and liver (1994 revision). J. Trauma 1995, 38, 323–324. [Google Scholar] [CrossRef]
- American College of Surgeons. Advanced Trauma Life Support for Doctors, 8th ed.; American College of Surgeons: Chicago, IL, USA, 2008. [Google Scholar]
- Kim, Y.J.; Kim, J.S.; Cho, S.H.; Bae, J.I.; Sohn, C.H.; Lee, Y.S.; Lee, J.H.; Lim, K.S.; Kim, W.Y. Characteristics of computed tomography in hemodynamically unstable blunt trauma patients: Experience at a tertiary care center. Medicine 2017, 96, e9168. [Google Scholar] [CrossRef]
- Gaski, I.A.; Skattum, J.; Brooks, A.; Koyama, T.; Eken, T.; Naess, P.A.; Gaarder, C. Decreased mortality, laparotomy, and embolization rates for liver injuries during a 13-year period in a major Scandinavian trauma center. Trauma Surg. Acute Care Open 2018, 3, e000205. [Google Scholar] [CrossRef]
- Tan, T.; Luo, Y.; Hu, J.; Li, F.; Fu, Y. Nonoperative management with angioembolization for blunt abdominal solid organ trauma in hemodynamically unstable patients: A systematic review and meta-analysis. Eur. J. Trauma Emerg. Surg. 2022, 49, 1751–1761. [Google Scholar] [CrossRef] [PubMed]
- Gaarder, C.; Naess, P.A.; Eken, T.; Skaga, N.O.; Pillgram-Larsen, J.; Klow, N.E.; Buanes, T. Liver injuries--improved results with a formal protocol including angiography. Injury 2007, 38, 1075–1083. [Google Scholar] [CrossRef] [PubMed]
- Bertens, K.A.; Vogt, K.N.; Hernandez-Alejandro, R.; Gray, D.K. Non-operative management of blunt hepatic trauma: Does angioembolization have a major impact? Eur. J. Trauma Emerg. Surg. 2014, 41, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Clarke, J.R.; Trooskin, S.Z.; Doshi, P.J.; Greenwald, L.; Mode, C.J. Time to laparotomy for intra-abdominal bleeding from trauma does affect survival for delays up to 90 min. J. Trauma 2002, 52, 420–425. [Google Scholar] [PubMed]
- Kanani, A.; Sandve, K.O.; Søreide, K. Management of severe liver injuries: Push, pack, pringle—And plug! Scand. J. Trauma, Resusc. Emerg. Med. 2021, 29, 93. [Google Scholar] [CrossRef] [PubMed]
- Carver, D.; Kirkpatrick, A.W.; D’Amours, S.; Hameed, S.M.; Beveridge, J.; Ball, C.G. A Prospective Evaluation of the Utility of a Hybrid. Operating Suite for Severely Injured Patients: Overstated or Underutilized? Ann. Surg. 2020, 271, 958–961. [Google Scholar] [CrossRef]
- Kirkpatrick, A.W.; Vis, C.; Dubé, M.; Biesbroek, S.; Ball, C.G.; Laberge, J.; Shultz, J.; Rea, K.; Sadler, D.; Holcomb, J.B.; et al. The evolution of a purpose designed hybrid trauma operating room from the trauma service perspective: The RAPTOR (Resuscitation with Angiography Percutaneous Treatments and Operative Resuscitations). Injury 2014, 45, 1413–1421. [Google Scholar] [CrossRef]

{kind=link}
| Authors | Year | Study Type | Total Patients | M/F Ratio | Mean Age | Total Primary Embolization in Unstable Patients | % Grade Trauma (AAST) |
|---|---|---|---|---|---|---|---|
| Tamura S et al. [9] | 2021 | RT | 92 | 3.7/1 | 29.5 | 59 | Grade III (58%) Grade IV (34%) Grade V (8%) |
| Aoki M et al. [10] | 2021 | RT | 224 | 1.5/1 | 55 | 57 | Grade III (40%) Grade IV (18%) Grade V (5%) |
| Alnumay A et al. [11] | 2021 | RT | 49 | 4/1 | 44 | 5 | Not available |
| Inukai K et al. [12] | 2018 | RT | 23 | 1/1 | 32.3 | 10 | Grade IV (80%) Grade V (20%) |
| Otsuka et al. [13] | 2017 | OB | 16 | 3/1 | 46 | 5 | Grade III (40%) Grade IV (20%) Grade V (40%) |
| Ogura et al. [14] | 2014 | RT | 7 | 3/1 | 63.5 | 3 | Grade II (33%) Grade IV (34%) Grade V (33%) |
| Mitsusada M et al. [15] | 2013 | RT | 29 | 2.2/1 | 38.5 | 8 | Not available |
| Di Saverio S et al. [16] | 2012 | RT | 34 | 1.5/1 | 42 | 10 | Not available |
| Misselbeck TS et al. [17] | 2009 | RT | 21 | N/A | N/A | 11 | Not available |
| Monnin et al. [18] | 2007 | RT | 12 | N/A | 35 | 3 | Grade IV (100%) |
| Authors | Year | Definition of Stable Patient | Definition of Unstable Patient |
|---|---|---|---|
| Tamura S et al. [9] | 2021 | All trauma patients responding to initial standard infusion therapy (crystalloid, albumin and blood transfusion) | SI > 1, despite initial infusion therapy |
| Aoki M et al. [10] | 2021 | sBP ≥ 90 mmHg upon hospital arrival | sBP < 90 mmHg upon hospital arrival and received blood transfusion within the first 24 h after arrival |
| Alnumay A et al. [11] | 2021 | Not available | Not available |
| Inukai K et al. [12] | 2018 | sBP ≥ 90 mmHg after initial fluid treatment | sBP ≥ 90 mmHg for even a second and therefore required rapid fluid infusion or blood transfusion |
| Otsuka et al. [13] | 2017 | sBP ≥ 90 mmHg after initial fluid treatment | sBP < 90 mmHg without improvement following primary resuscitation |
| Ogura et al. [14] | 2014 | Not available | sBP maintained at 70 mm Hg or greater during deflation of the balloon (REBOA) |
| Mitsusada M et al. [15] | 2013 | Not available | sBP ≥ 80 mmHg after resuscitative therapy |
| Di Saverio S et al. [16] | 2012 | Not available | Not available |
| Misselbeck TS et al. [17] | 2009 | At admission, sBP was ≥ 90 mm Hg and intravenous fluid requirements did not exceed 2 L. | Not available |
| Monnin et al. [18] | 2007 | Patients who were hemodynamically stable or stabilized by low or moderate resuscitation. | Patients with hemorrhagic shock improved or stabilized after resuscitative treatment. |
| Authors | Year | Total Number of Embolized Patients N | Mortality N (%) | AE Failure N (%) | Post-AE Complications N (%) |
|---|---|---|---|---|---|
| Tamura S et al. [9] | 2021 | 59 | 3 (3.2) | 2 (2.1) | 29 (31.5) |
| Aoki M et al. [10] | 2021 | 57 | 7 (12) | Not available | 9 (15.7) |
| Alnumay A et al. [11] | 2021 | 5 | Not available | Not available | Not available |
| Inukai K et al. [12] | 2018 | 10 | 1 (10) | 0 | 5 (50) |
| Otsuka et al. [13] | 2017 | 5 | Not available | 1 (20) | 4 (80) |
| Ogura et al. [14] | 2014 | 3 | 1 (33) | Not available | Not available |
| Mitsusada M et al. [15] | 2013 | 8 | 0 | 0 | 3 (37.5) |
| Di Saverio S et al. [16] | 2012 | 10 | Not available | Not available | Not available |
| Misselbeck TS et al. [17] | 2009 | 11 | 4 (36) | 1 (9) | 9 (81) |
| Monnin et al. [18] | 2007 | 3 | N/A | N/A | N/A |
| TOTAL | 171 | 16 (9.35) | 4 (2.33) | 59 (34.5) |
| Authors | Year | Total Number of Embolized Patients N | Liver Abscess/Biloma N (%) | Bile Leakage N (%) | Gallbladder Necrosis/Cholecystitis N (%) | Peritonitis N (%) | Abdominal Compartment Syndrome N (%) |
|---|---|---|---|---|---|---|---|
| Tamura S et al. [9] | 2021 | 59 | 13 (14.1) | 0 | 1 (1.08) | 0 | 0 |
| Aoki M et al. [10] | 2021 | 57 | 3 (5.26) | 0 | 1 (1.7) | 3 (5.2) | Not available |
| Alnumay A et al. [11] | 2021 | 5 | Not available | Not available | Not available | Not available | Not available |
| Inukai K et al. [12] | 2018 | 10 | 2 (20) | 1 (10) | 0 | 0 | 2 (20) |
| Otsuka et al. [13] | 2017 | 5 | 0 | 0 | 1 (20) | 2 (40) | 0 |
| Ogura et al. [14] | 2014 | 3 | Not available | Not available | Not available | Not available | Not available |
| Mitsusada M et al. [15] | 2013 | 8 | 0 | 3 (37.5) | 0 | 0 | 0 |
| Di Saverio S et al. [16] | 2012 | 10 | Not available | Not available | Not available | Not available | Not available |
| Misselbeck TS et al. [17] | 2009 | 11 | 4 (36) | 1 (9) | 6 (66) | 6 (54) | 0 |
| Monnin et al. [18] | 2007 | 3 | Not available | Not available | Not available | Not available | Not available |
| TOTAL | 171 | 22 (12.8) | 5 (3) | 9 (5.3) | 11 (6.4) | 2 (1.16) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corvino, F.; Giurazza, F.; Marra, P.; Ierardi, A.M.; Corvino, A.; Basile, A.; Galia, M.; Inzerillo, A.; Niola, R. Damage Control Interventional Radiology in Liver Trauma: A Comprehensive Review. J. Pers. Med. 2024, 14, 365. https://doi.org/10.3390/jpm14040365
Corvino F, Giurazza F, Marra P, Ierardi AM, Corvino A, Basile A, Galia M, Inzerillo A, Niola R. Damage Control Interventional Radiology in Liver Trauma: A Comprehensive Review. Journal of Personalized Medicine. 2024; 14(4):365. https://doi.org/10.3390/jpm14040365
Chicago/Turabian StyleCorvino, Fabio, Francesco Giurazza, Paolo Marra, Anna Maria Ierardi, Antonio Corvino, Antonio Basile, Massimo Galia, Agostino Inzerillo, and Raffaella Niola. 2024. "Damage Control Interventional Radiology in Liver Trauma: A Comprehensive Review" Journal of Personalized Medicine 14, no. 4: 365. https://doi.org/10.3390/jpm14040365
APA StyleCorvino, F., Giurazza, F., Marra, P., Ierardi, A. M., Corvino, A., Basile, A., Galia, M., Inzerillo, A., & Niola, R. (2024). Damage Control Interventional Radiology in Liver Trauma: A Comprehensive Review. Journal of Personalized Medicine, 14(4), 365. https://doi.org/10.3390/jpm14040365