
Opioids in Treatment of Refractory Dyspnea in Chronic Obstructive Pulmonary Disease: Yes, No or Maybe

 , , , and
, , , and
Abstract
1. Background
2. Materials and Methods
3. Rationale for the Use of Opioids in COPD
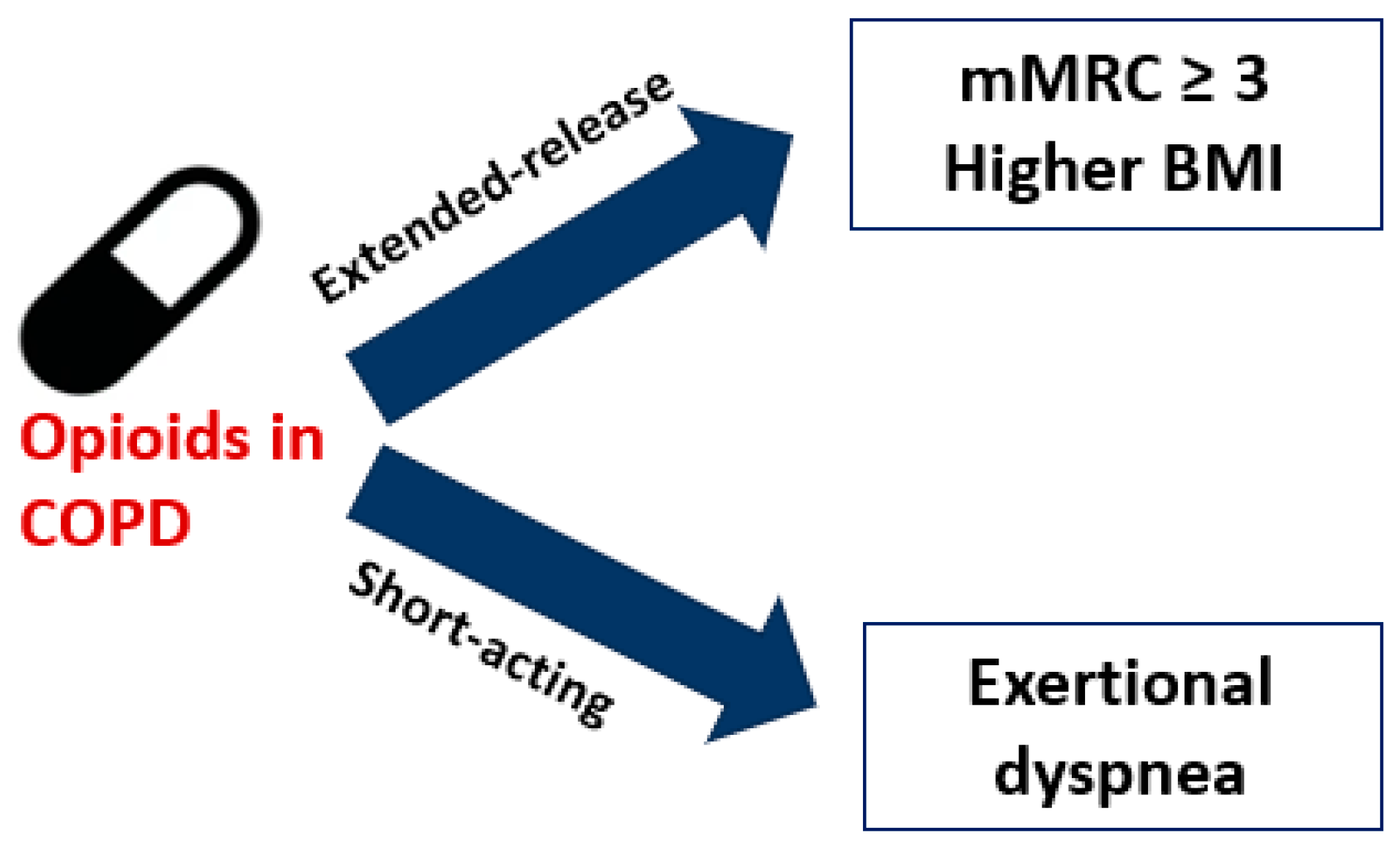
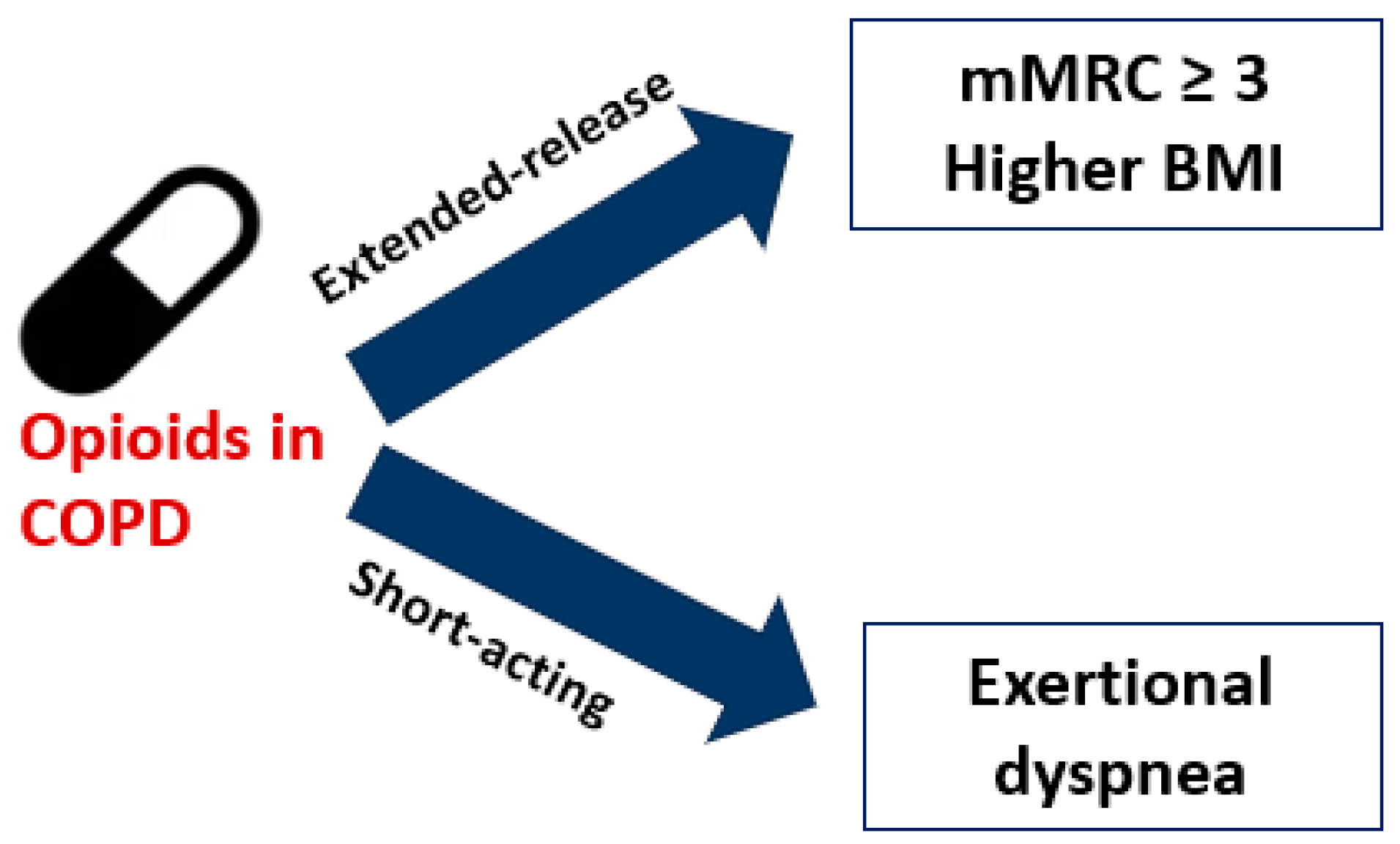
4. Type of Opioids: Extended-Release Formulations and Immediate Delivery Agents
5. Evidence Supporting the Use of Opioids in COPD
6. Latest Supporting Updates—Subgroup Analysis
7. Evidence against the Use of Opioids in COPD
8. Current Guidelines and Future Endeavors
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Initiative for Chronic Obstructive Lung Disease (GOLD), Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease (2024 Report). Available online: https://goldcopd.org/2024-gold-report/ (accessed on 5 January 2024).
- Curtis, J.R.; Patrick, D.L. The assessment of health status among patients with COPD. Eur. Respir. J. Suppl. 2003, 41, 36s–45s. [Google Scholar] [CrossRef] [PubMed]
- Vozoris, N.T. Opioids for Dyspnea in Chronic Obstructive Pulmonary Disease: Short on the Details. Am. J. Respir. Crit. Care Med. 2021, 203, 266–267. [Google Scholar] [CrossRef] [PubMed]
- Booth, S.; Silvester, S.; Todd, C. Breathlessness in cancer and chronic obstructive pulmonary disease: Using a qualitative approach to describe the experience of patients and carers. Palliat. Support. Care 2003, 1, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.; Partridge, M.R.; Miravitlles, M.; Cazzola, M.; Vogelmeier, C.; Leynaud, D.; Ostinelli, J. Symptom variability in patients with severe COPD: A pan-European cross-sectional study. Eur. Respir. J. 2011, 37, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Hill, K.; Hug, S.; Smith, A.; O’Sullivan, P. The Role of Illness Perceptions in Dyspnoea-Related Fear in Chronic Obstructive Pulmonary Disease. J. Clin. Med. 2023, 13, 200. [Google Scholar] [CrossRef]
- Elkington, H.; White, P.; Addington-Hall, J.; Higgs, R.; Pettinari, C. The last year of life of COPD: A qualitative study of symptoms and services. Respir. Med. 2004, 98, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Bausewein, C.; Farquhar, M.; Booth, S.; Gysels, M.; Higginson, I.J. Measurement of breathlessness in advanced disease: A systematic review. Respir. Med. 2007, 101, 399–410. [Google Scholar] [CrossRef]
- Ekström, M.; Nilsson, F.; Abernethy, A.A.; Currow, D.C. Effects of opioids on breathlessness and exercise capacity in chronic obstructive pulmonary disease. A systematic review. Ann. Am. Thorac. Soc. 2015, 12, 1079–1092. [Google Scholar] [CrossRef]
- Ekström, M.; Bajwah, S.; Bland, J.M.; Currow, D.C.; Hussain, J.; Johnson, M.J. One evidence base; three stories: Do opioids relieve chronic breathlessness? Thorax 2018, 73, 88–90. [Google Scholar] [CrossRef]
- Sykes, N.; Thorns, A. The use of opioids and sedatives at the end of life. Lancet Oncol. 2003, 4, 312–318. [Google Scholar] [CrossRef]
- Verberkt, C.A.; van den Beuken-van Everdingen, M.H.J.; Schols, J.M.G.A.; Hameleers, N.; Wouters, E.F.M.; Janssen, D.J.A. Effect of Sustained-Release Morphine for Refractory Breathlessness in Chronic Obstructive Pulmonary Disease on Health Status: A Randomized Clinical Trial. JAMA Intern. Med. 2020, 180, 1306–1314. [Google Scholar] [CrossRef]
- Ferreira, D.H.; Louw, S.; McCloud, P.; Fazekas, B.; McDonald, C.F.; Agar, M.R.; Clark, K.; McCaffrey, N.; Ekström, M.; Currow, D.C. Australian National Palliative Care Clinical Studies Collaborative (PaCCSC). Controlled-Release Oxycodone vs. Placebo in the Treatment of Chronic Breathlessness-A Multisite Randomized Placebo Controlled Trial. J. Pain Symptom Manag. 2020, 59, 581–589. [Google Scholar] [CrossRef]
- Ekström, M.; Ferreira, D.; Chang, S.; Louw, S.; Johnson, M.J.; Eckert, D.J.; Fazekas, B.; Clark, K.J.; Agar, M.R.; Currow, D.C. Australian National Palliative Care Clinical Studies Collaborative. Effect of Regular, Low-Dose, Extended-release Morphine on Chronic Breathlessness in Chronic Obstructive Pulmonary Disease: The BEAMS Randomized Clinical Trial. JAMA 2022, 328, 2022–2032, Erratum in JAMA 2023, 329, 687. [Google Scholar] [CrossRef] [PubMed]
- Rocker, G.; Young, J.; Donahue, M.; Farquhar, M.; Simpson, C. Perspectives of patients, family caregivers and physicians about the use of opioids for refractory dyspnea in advanced chronic obstructive pulmonary disease. CMAJ 2012, 184, E497–E504. [Google Scholar] [CrossRef] [PubMed]
- Boom, M.; Niesters, M.; Sarton, E.; Aarts, L.; Smith, T.W.; Dahan, A. Non-analgesic Effects of Opioids: Opioid-Induced Respiratory Depression. Curr. Pharm. Des. 2012, 18, 5994–6004. [Google Scholar] [CrossRef]
- Montandon, G.; Qin, W.; Liu, H.; Ren, J.; Greer, J.J.; Horner, R.L. PreBotzinger complex neurokinin-1 receptor-expressing neurons mediate opioid-induced respiratory depression. J. Neurosci. 2011, 31, 1292–1301. [Google Scholar] [CrossRef]
- Pattinson, K.T. Opioids, and the control of respiration. Br. J. Anaesth. 2008, 100, 747–758. [Google Scholar] [CrossRef] [PubMed]
- May, W.J.; Gruber, R.B.; Discala, J.F.; Puskovic, V.; Henderson, F.; Palmer, L.A.; Lewis, S.J. Morphine has latent deleterious effects on the ventilatory responses to a hypoxic challenge. Open J. Mol. Integr. Physiol. 2013, 3, 166–180. [Google Scholar] [CrossRef]
- Pattinson, K.T.; Governo, R.J.; MacIntosh, B.J.; Russell, E.C.; Corfield, D.R.; Tracey, I.; Wise, R.G. Opioids depress cortical centers responsible for the volitional control of respiration. J. Neurosci. 2009, 29, 8177–8186. [Google Scholar] [CrossRef]
- Wilson, M.A.; Junor, L. The role of amygdalar mu-opioid receptors in anxiety-related responses in two rat models. Neuropsychopharmacology 2008, 33, 2957–2968. [Google Scholar] [CrossRef]
- Johnson, M.J.; Currow, D.C. Opioids for breathlessness: A narrative review. BMJ Support. Palliat. Care 2020, 10, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Herigstad, M.; Hayen, A.; Evans, E.; Hardinge, F.M.; Davies, R.J.; Wiech, K.; Pattinson, K.T.S. Dyspnea-related cues engage the prefrontal cortex: Evidence from functional brain imaging in COPD. Chest 2015, 148, 953–961. [Google Scholar] [CrossRef] [PubMed]
- Currow, D.C.; Quinn, S.; Ekstrom, M.; Kaasa, S.; Johnson, M.J.; Somogyi, A.A.; Klepstad, P. Can variability in the effect of opioids on refractory breathlessness be explained by genetic factors? BMJ Open 2015, 5, e006818. [Google Scholar] [CrossRef]
- Hui, D.; Bruera, E. Use of short-acting opioids in the management of breathlessness: An evidence-based review. Curr. Opin. Support. Palliat. Care 2020, 14, 167–176. [Google Scholar] [CrossRef]
- Currow, D.C.; McDonald, C.; Oaten, S.; Kenny, B.; Allcroft, P.; Frith, P.; Briffa, M.; Johnson, M.J.; Abernethy, A.P. Once-daily opioids for chronic dyspnea: A dose increment and pharmacovigilance study. J. Pain Symptom Manag. 2011, 42, 388–399. [Google Scholar] [CrossRef]
- Abdallah, S.J.; Wilkinson-Maitland, C.; Saad, N.; Li, P.Z.; Smith, B.M.; Bourbeau, J.; Jensen, D. Effect of morphine on breathlessness and exercise endurance in advanced COPD: A randomized crossover trial. Eur. Respir. J. 2017, 50, 1701235. [Google Scholar] [CrossRef]
- Light, R.W.; Stansbury, D.W.; Webster, J.S. Effect of 30 mg of morphine alone or with promethazine or prochlorperazine on the exercise capacity of patients with COPD. Chest 1996, 109, 975–981. [Google Scholar] [CrossRef] [PubMed]
- Barnes, H.; McDonald, J.; Smallwood, N.; Manser, R. Opioids for the palliation of refractory breathlessness in adults with advanced disease and terminal illness. Cochrane Database Syst. Rev. 2016, 3, CD011008. [Google Scholar] [CrossRef]
- Krajnik, M.; Jassem, E.; Sobanski, P. Opioid receptor bronchial tree: Current science. Curr. Opin. Support. Palliat. Care 2014, 8, 191–199. [Google Scholar] [CrossRef]
- Janowiak, P.; Krajnik, M.; Podolec, Z.; Bandurski, T.; Damps-Konstańska, I.; Sobański, P.; Currow, D.C.; Jassem, E. Dosimetrically administered nebulized morphine for breathlessness in very severe chronic obstructive pulmonary disease: A randomized, controlled trial. BMC Pulm. Med. 2017, 17, 186. [Google Scholar] [CrossRef]
- Nieminen, M.M.; Holli, H.; Lahdensuo, A.; Muittari, A.; Karvonen, J. Aerosol deposition in automatic dosimeter nebulization. Eur. J. Respir. Dis. 1987, 71, 145–152. [Google Scholar] [PubMed]
- Jensen, D.; Alsuhail, A.; Viola, R.; Dudgeon, D.J.; Webb, K.A.; O’Donnell, D.E. Inhaled fentanyl citrate improves exercise endurance during high-intensity constant work rate cycle exercise in chronic obstructive pulmonary disease. J. Pain Symptom Manag. 2012, 43, 706–719. [Google Scholar] [CrossRef]
- Janssen, D.J.A.; van den Beuken-van Everdingen, M.H.J.; Verberkt, C.A.; Creemers, J.P.H.M.; Wouters, E.F.M. Fentanyl nasal spray in a patient with end-stage COPD and severe chronic breathlessness. Breathe 2019, 15, e122–e125. [Google Scholar] [CrossRef]
- Iupati, S.; Bridge, R.; Allan, S.; Hewitt, D. Intranasal Fentanyl Versus Placebo for Treatment of Episodic Breathlessness in Hospice Patients with Advanced Nonmalignant Diseases. J. Pain Symptom Manag. 2021, 61, 1035–1041. [Google Scholar] [CrossRef] [PubMed]
- Dale, O.; Hjortkjaer, R.; Kharasch, E.D. Nasal administration of opioids for pain management in adults. Acta Anaesthesiol. Scand. 2002, 46, 759–770. [Google Scholar] [CrossRef] [PubMed]
- Simon, S.T.; Bausewein, C.; Schildmann, E.; Higginson, I.J.; Magnussen, H.; Scheve, C.; Ramsenthaler, C. Episodic breathlessness in patients with advanced disease: A systematic review. J. Pain Symptom Manag. 2013, 45, 561–578. [Google Scholar] [CrossRef]
- Rocker, G.M.; Simpson, A.C.; Young, J.; Horton, R.; Sinuff, T.; Demmons, J.; Donahue, M.; Hernandez, P.; Marciniuk, D. Opioid therapy for refractory dyspnea in patients with advanced chronic obstructive pulmonary disease: Patients’ experiences and outcomes. CMAJ Open 2013, 1, E27–E36. [Google Scholar] [CrossRef]
- Marciniuk, D.D.; Goodridge, D.; Hernandez, P.; Rocker, G.; Balter, M.; Bailey, P.; Ford, G.; Bourbeau, J.; O’Donnell, D.E.; Maltais, F.; et al. Managing dyspnea in patients with advanced chronic obstructive pulmonary disease: A Canadian Thoracic Society clinical practice guideline. Can. Respir. J. 2011, 18, 69–78. [Google Scholar] [CrossRef]
- Currow, D.C.; Ekström, M.; Johnson, M.J. Overdosing on immediate-release morphine solution has predictable adverse effects. Eur. Respir. J. 2017, 50, 1701091. [Google Scholar] [CrossRef]
- Vozoris, N.T. Opioid utility for dyspnea in chronic obstructive pulmonary disease: A complicated and controversial story. Ann. Palliat. Med. 2020, 9, 571–578. [Google Scholar] [CrossRef]
- Currow, D.; Louw, S.; McCloud, P.; Fazekas, B.; Plummer, J.; McDonald, C.F.; Agar, M.; Clark, K.; McCaffrey, N.; Ekström, M.P. Australian National Palliative Care Clinical Studies Collaborative (PaCCSC). Regular, sustained-release morphine for chronic breathlessness: A multicentre, double-blind, randomised, placebo-controlled trial. Thorax 2020, 75, 50–56, Erratum in Thorax 2020, 75, e5. [Google Scholar] [CrossRef]
- Jennings, A.L.; Davies, A.N.; Higgins, J.P.; Gibbs, J.S.; Broadley, K.E. A systematic review of the use of opioids in the management of dyspnoea. Thorax 2002, 57, 939–944. [Google Scholar] [CrossRef]
- Nici, L.; Mammen, M.J.; Charbek, E.; Alexander, P.E.; Au, D.H.; Boyd, C.M.; Criner, G.J.; Donaldson, G.C.; Dreher, M.; Fan, V.S.; et al. Pharmacologic Management of Chronic Obstructive Pulmonary Disease. An Official American Thoracic Society Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2020, 201, e56–e69, Erratum in Am. J. Respir. Crit. Care Med. 2020, 202, 910. [Google Scholar] [CrossRef]
- Lopez-Campos, J.L.; Almagro, P.; Gómez, J.T.; Chiner, E.; Palacios, L.; Hernández, C.; Navarro, M.D.; Molina, J.; Rigau, D.; Soler-Cataluña, J.J.; et al. Spanish COPD Guideline (GesEPOC) Update: Comorbidities, Self-Management and Palliative Care. Arch. Bronconeumol. 2022, 58, 334–344, (In English, Spanish). [Google Scholar] [CrossRef]
- Ahmadi, Z.; Bernelid, E.; Currow, D.C.; Ekström, M. Prescription of opioids for breathlessness in end-stage COPD: A national population-based study. Int. J. Chron. Obstruct Pulmon Dis. 2016, 11, 2651–2657. [Google Scholar] [CrossRef]
- Verberkt, C.A.; van den Beuken-Everdingen, M.H.J.; Schols, J.M.G.A.; Wouters, E.F.M.; Janssen, D.J.A. Morphine for chronic breathlessness in COPD: Improvement predictors-cross-sectional study. BMJ Support. Palliat. Care 2022, 18, bmjspcare-2022-003693. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Xiao, W.; Du, L.; Yu, Y.; Chen, X.; Mao, B.; Fu, J. Effectiveness, and safety of opioids on breathlessness and exercise endurance in patients with chronic obstructive pulmonary disease: A systematic review and meta-analysis of randomised controlled trials. Palliat. Med. 2023, 37, 1365–1378. [Google Scholar] [CrossRef] [PubMed]
- van Dijk, M.; Mooren, K.J.M.; van den Berg, J.K.; van Beurden-Moeskops, W.J.C.; Heller-Baan, R.; de Hosson, S.M.; Lam-Wong, W.Y.; Peters, L.; Pool, K.; Kerstjens, H.A.M. Opioids in patients with COPD and refractory dyspnea: Literature review and design of a multicenter double-blind study of low dosed morphine and fentanyl (MoreFoRCOPD). BMC Pulm. Med. 2021, 21, 289. [Google Scholar] [CrossRef] [PubMed]
- Jamil, M.; Jahangir, A.; Abdo, T. Use of opioids to relieve chronic dyspnea in advanced COPD. Am. J. Respir. Crit. Care Med. 2023, 207, A3352. [Google Scholar]
- Simon, S.T.; Köskeroglu, P.; Gaertner, J.; Voltz, R. Fentanyl for the relief of refractory breathlessness: A systematic review. J. Pain Symptom Manag. 2013, 46, 874–886. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A.; Young, J.B. Which medications to avoid in people at risk of delirium: A systematic review. Age Ageing 2011, 40, 23–29. [Google Scholar] [CrossRef]
- Buckeridge, D.; Huang, A.; Hanley, J.; Kelome, A.; Reidel, K.; Verma, A.; Winslade, N.; Tamblyn, R. Risk of injury associated with opioid use in older adults. J. Am. Geriatr. Soc. 2010, 58, 1664–1670. [Google Scholar] [CrossRef]
- Papaleontiou, M.; Henderson, C.R., Jr.; Turner, B.J.; Moore, A.A.; Olkhovskaya, Y.; Amanfo, L.; Reid, M.C. Outcomes associated with opioid use in the treatment of chronic noncancer pain in older adults: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 2010, 58, 1353–1369. [Google Scholar] [CrossRef] [PubMed]
- Ray, W.A.; Chung, C.P.; Murray, K.T.; Hall, K.; Stein, C.M. Prescription of Long-Acting Opioids and Mortality in Patients with Chronic Noncancer Pain. JAMA 2016, 315, 2415–2423. [Google Scholar] [CrossRef] [PubMed]
- Neutel, C.I.; Johansen, H.L. Association between hypnotics use and increased mortality: Causation or confounding? Eur. J. Clin. Pharmacol. 2015, 71, 637–642. [Google Scholar] [CrossRef] [PubMed]
- Lalley, P.M. Mu-opioid receptor agonist effects on medullary respiratory neurons in the cat: Evidence for involvement in certain types of ventilatory disturbances. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2003, 285, R1287–R1304, Erratum in Am. J. Physiol. Regul. Integr. Comp. Physiol. 2004, 56, R489. [Google Scholar] [CrossRef]
- Adcock, J.J.; Schneider, C.; Smith, T.W. Effects of codeine, morphine and a novel opioid pentapeptide BW443C, on cough, nociception and ventilation in the unanaesthetized guinea-pig. Br. J. Pharmacol. 1988, 93, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Vallejo, R.; de Leon-Casasola, O.; Benyamin, R. Opioid therapy and immunosuppression: A review. Am. J. Ther. 2004, 11, 354–365. [Google Scholar] [CrossRef]
- Wang, J.; Barke, R.A.; Charboneau, R.; Roy, S. Morphine impairs host innate immune response and increases susceptibility to Streptococcus pneumoniae lung infection. J. Immunol. 2005, 174, 426–434. [Google Scholar] [CrossRef]
- Woodcock, A.A.; Gross, E.R.; Gellert, A.; Shah, S.; Johnson, M.; Geddes, D.M. Effects of dihydrocodeine, alcohol, and caffeine on breathlessness and exercise tolerance in patients with chronic obstructive lung disease and normal blood gases. N. Engl. J. Med. 1981, 305, 1611–1616. [Google Scholar] [CrossRef]
- Ekström, M.P.; Bornefalk-Hermansson, A.; Abernethy, A.P.; Currow, D.C. Safety of benzodiazepines and opioids in very severe respiratory disease: National prospective study. BMJ 2014, 348, g445. [Google Scholar] [CrossRef]
- Vozoris, N.T.; Wang, X.; Fischer, H.D.; Bell, C.M.; O’Donnell, D.E.; Austin, P.C.; Stephenson, A.L.; Gill, S.S.; Rochon, P.A. Incident opioid drug use and adverse respiratory outcomes among older adults with COPD. Eur. Respir. J. 2016, 48, 683–693. [Google Scholar] [CrossRef]
- De Lara, F.V.; Rincon, F.B.; Pondaiah, S.; Freites, C.O.; Pan, D.; Mathew, J. Effect of opioid abuse and dependance on outcomes of patients hospitalized with COPD: A 5-year analysis. Obstr. Lung Dis. 2018, 154 (Suppl. S4), 771A. [Google Scholar]
- Downar, J.; Colman, R.; Horton, R.; Hernandez, P.; Rocker, G. Opioids in COPD: A cause of death or a marker of illness severity? Eur. Respir. J. 2016, 48, 1520–1521. [Google Scholar] [CrossRef] [PubMed]
- Freemantle, N.; Marston, L.; Walters, K.; Wood, J.; Reynolds, M.R.; Petersen, I. Making inferences on treatment effects from real world data: Propensity scores, confounding by indication, and other perils for the unwary in observational research. BMJ 2013, 347, f6409. [Google Scholar] [CrossRef] [PubMed]
- Weiss, A.; Porter, S.; Rozenberg, D.; O’Connor, E.; Lee, T.; Balter, M.; Wentlandt, K. Chronic Obstructive Pulmonary Disease: A Palliative Medicine Review of the Disease, Its Therapies, and Drug Interactions. J. Pain Symptom Manag. 2020, 60, 135–150. [Google Scholar] [CrossRef] [PubMed]
- Mahler, D.A.; Selecky, P.A.; Harrod, C.G.; Benditt, J.O.; Carrieri-Kohlman, V.; Curtis, J.R.; Manning, H.L.; Mularski, R.A.; Varkey, B.; Campbell, M.; et al. American College of Chest Physicians consensus statement on the management of dyspnea in patients with advanced lung or heart disease. Chest 2010, 137, 674–691. [Google Scholar] [CrossRef]

{kind=link}
| Study/Analysis | Number of Participants /mMRC | Opioid Type | Dosage | Breathlessness Scale | Outcome Measure | Findings |
|---|---|---|---|---|---|---|
| Janoviak et al. [31] | 10 (mMRC ≥ 3) | Nebulized morphine | 3–5 mg | VAS | Chronic breathlessness now | Superiority of dosimetrically administered nebulized morphine. |
| Abdallah et al. [27] | 20 (mMRC ≥ 3) | Oral immediate-release morphine | 10 mg maximum dose | Borg | Exertional breathlessness | Morphine decreased breathlessness intensity ratings during exercise at isotime. |
| Rocker et al. [38] | 44 (mMRC ≥ 4) | Immediate-release morphine sulfate syrup | 0.5 mg twice daily (initially) | NRS and Chronic Respiratory Questionnaire–Dyspnea domain | Health-related quality of life, dyspnea, anxiety, depression | Beneficial for 61% of patients; positive effects early on and maintained over several months. |
| MORDYC study [12] | 111 (mMRC ≥ 2) | Oral sustained-release morphine | 10 mg twice daily (escalation to three times daily) | NRS | Disease-specific health status (COPD Assessment Test), PaCO2, Breathlessness | Improvement in disease-specific health status; no notable change in breathlessness; improvement in worst breathlessness for mMRC grades 3 to 4. |
| Currow et al. [42] | 164 (mMRC ≥ 2) | Oral sustained-release morphine | 20 mg daily (≤6 doses of 2.5 mg immediate-release morphine (≤15 mg/24 h) | VAS | Intensity of breathlessness now | No difference between groups. Decreased worst breathlessness in opioid subgroup (for mMRC ≥ 3) compared to placebo. |
| Verberkt et al. [47] | 45 (mMRC ≥ 3) | Oral sustained-release morphine | 20–30 mg | NRS | Chronic breathlessness | Greater baseline breathlessness and higher BMI linked to improvement. |
| BEAMS trial [14] | 160 (mMRC ≥ 3) | Oral sustained-release morphine | Week 1: 8 mg/d or 16 mg/d or placebo Week 2–3: +8 mg/d | NRS | Intensity of worst breathlessness | No difference between groups. |
| MoreFoRCOPD study [49] | Ongoing (mMRC ≥ 3) | Oral sustained-release or transdermal fentanyl | 10 mg twice a day (morphine) or 12 mcg/h transdermal fentanyl | NRS | Refractory breathlessness | Ongoing |
| Jensen et al. [33] | 12 | Nebulized fentanyl citrate | 50 mcg | Borg | Exercise tolerance and dyspnea intensity and unpleasantness | Increased exercise endurance time. Delay in the onset of intolerable dyspnea. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rajnoveanu, R.-M.; Harangus, A.; Todea, D.A.; Man, M.A.; Budin, C.E.; Rajnoveanu, A.-G. Opioids in Treatment of Refractory Dyspnea in Chronic Obstructive Pulmonary Disease: Yes, No or Maybe. J. Pers. Med. 2024, 14, 318. https://doi.org/10.3390/jpm14030318
Rajnoveanu R-M, Harangus A, Todea DA, Man MA, Budin CE, Rajnoveanu A-G. Opioids in Treatment of Refractory Dyspnea in Chronic Obstructive Pulmonary Disease: Yes, No or Maybe. Journal of Personalized Medicine. 2024; 14(3):318. https://doi.org/10.3390/jpm14030318
Chicago/Turabian StyleRajnoveanu, Ruxandra-Mioara, Antonia Harangus, Doina Adina Todea, Milena Adina Man, Corina Eugenia Budin, and Armand-Gabriel Rajnoveanu. 2024. "Opioids in Treatment of Refractory Dyspnea in Chronic Obstructive Pulmonary Disease: Yes, No or Maybe" Journal of Personalized Medicine 14, no. 3: 318. https://doi.org/10.3390/jpm14030318
APA StyleRajnoveanu, R.-M., Harangus, A., Todea, D. A., Man, M. A., Budin, C. E., & Rajnoveanu, A.-G. (2024). Opioids in Treatment of Refractory Dyspnea in Chronic Obstructive Pulmonary Disease: Yes, No or Maybe. Journal of Personalized Medicine, 14(3), 318. https://doi.org/10.3390/jpm14030318