

Perceived Health Benefits in Vestibular Schwannoma Patients with Long-Term Postoperative Headache: Insights from Personality Traits and Pain Coping—A Cross-Sectional Study

 ,
, 
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Demographic Characteristics
3.2. Associations between POH and PHB
3.3. Associations between Age, Hearing Loss, Facial Paresis, and Pain
3.4. Associations between Pain-Related Mental Interference, Pain Coping, and Personality Traits
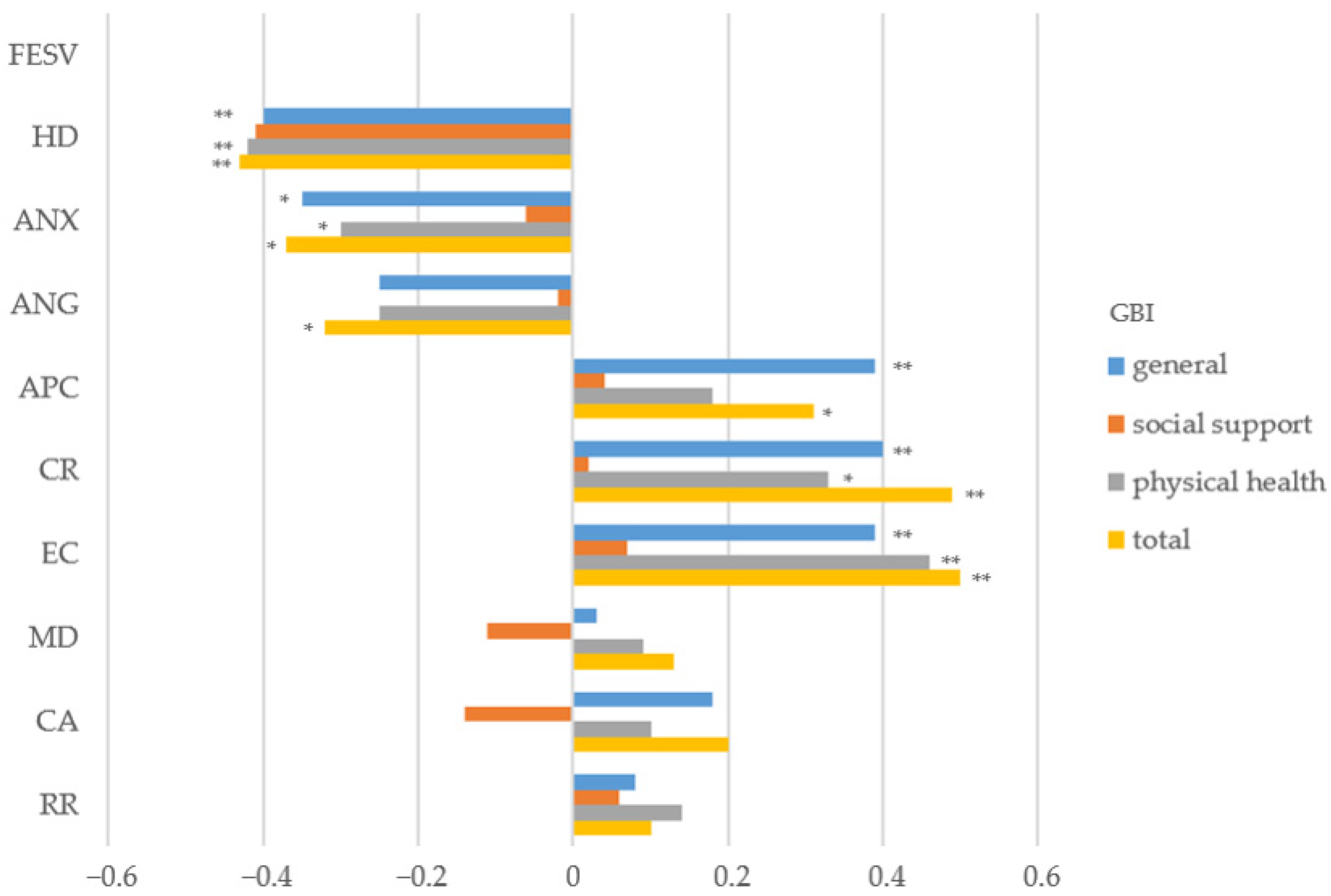
3.5. Associations between Pain-Related Mental Interference, Coping Mechanisms, and PHBs
3.6. Associations between Personality and PHBs
3.7. Predictors for PHBs
4. Discussion
4.1. Summary of Findings
4.2. Associations among Age, Hearing Loss, and Pain-Related Mental Interference
4.3. Personality Traits and Pain-Related Mental Interference and Coping
4.4. Biopsychosocial Model and Diathesis-Stress Component
4.5. PHBs and Coping Mechanisms
4.6. Psychological Interventions for POHs in VS Patients
4.7. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gauden, A.; Weir, P.; Hawthorne, G.; Kaye, A. Systematic review of quality of life in the management of vestibular schwannoma. J. Clin. Neurosci. 2011, 18, 1573–1584. [Google Scholar] [CrossRef] [PubMed]
- Presutti, L.; Magnaguagno, F.; Pavesi, G.; Cunsolo, E.; Pinna, G.; Alicandri-Ciufelli, M.; Marchioni, D.; Prontera, A.; Gioacchini, F. Combined endoscopic-microscopic approach for vestibular schwannoma removal: Outcomes in a cohort of 81 patients. Acta Otorhinolaryngol. Ital. 2014, 34, 427. [Google Scholar]
- Bender, M.; Tatagiba, M.; Gharabaghi, A. Quality of Life After Vestibular Schwannoma Surgery: A Question of Perspective. Front. Oncol. 2022, 11, 5950. [Google Scholar] [CrossRef] [PubMed]
- Turel, M.K.; Thakar, S.; Rajshekhar, V. Quality of life following surgery for large and giant vestibular schwannomas: A prospective study. J. Neurosurg. 2015, 122, 303–311. [Google Scholar] [CrossRef]
- Lucidi, D.; Fabbris, C.; Cerullo, R.; Di Gioia, S.; Calvaruso, F.; Monzani, D.; Alicandri-Ciufelli, M.; Marchioni, D.; Presutti, L. Quality of life in vestibular schwannoma: A comparison of three surgical techniques. Eur. Arch. Otorhinolaryngol. 2022, 279, 1795–1803. [Google Scholar] [CrossRef]
- Santa Maria, C.; Santa Maria, P.L.; Bulsara, V.; Jayawardena, J.; Caldow, J.D.; Png, L.H.; Atlas, M.D. Long-term quality of life in patients with vestibular schwannoma managed with microsurgery. J. Laryngol. Otol. 2019, 133, 953–959. [Google Scholar] [CrossRef]
- Breivik, C.N.; Varughese, J.K.; Wentzel-Larsen, T.; Vassbotn, F.; Lund-Johansen, M. Conservative management of vestibular schwannoma—A prospective cohort study: Treatment, symptoms, and quality of life. Neurosurgery 2012, 70, 1072–1080. [Google Scholar] [CrossRef]
- Carlson, M.L.; Tveiten, Ø.V.; Driscoll, C.L.; Goplen, F.K.; Neff, B.A.; Pollock, B.E.; Tombers, N.M.; Lund-Johansen, M.; Link, M.J. What drives quality of life in patients with sporadic vestibular schwannoma? Laryngoscope 2015, 125, 1697–1702. [Google Scholar] [CrossRef]
- Pruijn, I.M.; Kievit, W.; Hentschel, M.A.; Mulder, J.J.; Kunst, H.P. What determines quality of life in patients with vestibular schwannoma? Clin. Otolaryngol. 2021, 46, 412–420. [Google Scholar] [CrossRef]
- Miller, L.E.; Brant, J.A.; Naples, J.G.; Bigelow, D.C.; Lee, J.Y.; Ruckenstein, M.J. Quality of life in vestibular schwannoma patients: A longitudinal study. Otol. Neurotol. 2020, 41, e256–e261. [Google Scholar] [CrossRef]
- Stephanie Aarts, H.; Wever, C.C.; Kunst, M.; Semin, G.R. Quality of life, social function, emotion, and facial paresis in Dutch vestibular schwannoma patients. Laryngoscope Investig. Otolaryngol. 2020, 5, 477–484. [Google Scholar]
- Sabab, A.; Sandhu, J.; Bacchi, S.; Jukes, A.; Zacest, A. Postoperative headache following treatment of vestibular schwannoma: A literature review. J. Clin. Neurosci. 2018, 52, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Ansari, S.F.; Terry, C.; Cohen-Gadol, A.A. Surgery for vestibular schwannomas: A systematic review of complications by approach. Neurosurg. Focus. 2012, 33, E14. [Google Scholar] [CrossRef] [PubMed]
- Ocak, P.E.; Doğan, I.; Sayyahmelli, S.; Başkaya, M.K. Retrosigmoid Approach for Vestibular Schwannoma Surgery; Springer: Berlin/Heidelberg, Germany, 2019; pp. 105–133. [Google Scholar]
- Thomas, M.; Rampp, S.; Scheer, M.; Strauss, C.; Prell, J.; Schönfeld, R.; Leplow, B. Premorbid Psychological Factors Associated with Long-Term Postoperative Headache after Microsurgery in Vestibular Schwannoma—A Retrospective Pilot Study. Brain Sci. 2023, 13, 1171. [Google Scholar] [CrossRef]
- Ribeyre, L.; Parietti-Winkler, C.; Lassalle, B.; Hoffmann, C.; Spitz, E. Vestibular schwannoma surgery: Personality facets, illness perceptions and coping strategies influencing long term postural recovery. Eur. Health Psychol. 2017, 19, 622. [Google Scholar]
- Garramone, F.; Baiano, C.; Russo, A.; D’Iorio, A.; Tedeschi, G.; Trojano, L.; Santangelo, G. Personality profile and depression in migraine: A meta-analysis. Neurol. Sci. 2020, 41, 543–554. [Google Scholar] [CrossRef]
- Özdemir, O.; Aykan, F.; Özdemir, P. Coping Strategies and personality traits in women patients with migraine and tension type headache. J. Mood Disord. 2014, 4, 59. [Google Scholar] [CrossRef]
- Aaseth, K.; Grande, R.B.; Leiknes, K.A.; Benth, J.; Lundqvist, C.; Russell, M.B. Personality traits and psychological distress in persons with chronic tension-type headache. The Akershus study of chronic headache. Acta Neurol. Scand. 2011, 124, 375–382. [Google Scholar] [CrossRef]
- Bottiroli, S.; Renzi, A.; Ballante, E.; Roberto De Icco Sances, G.; Tanzilli, A.; Vecchi, T.; Tassorelli, C.; Galli, F. Personality in Chronic Headache: A Systematic Review with Meta-Analysis. Pain Res. Manag. 2023, 2023, 6685372. [Google Scholar] [CrossRef]
- Rausa, M.; Cevoli, S.; Sancisi, E.; Grimaldi, D.; Pollutri, G.; Casoria, M.; Grieco, D.; Bisi, A.; Cortelli, P.; Pozzi, E.; et al. Personality traits in chronic daily headache patients with and without psychiatric comorbidity: An observational study in a tertiary care headache center. J. Headache Pain 2013, 14, 22. [Google Scholar] [CrossRef]
- Yang, F.; Dos Santos, I.A.M.; Gomez, R.S.; Kummer, A.; Barbosa, I.G.; Teixeira, A.L. Personality disorders are associated with more severe forms of migraine. Acta Neurol. Belg. 2019, 119, 201–205. [Google Scholar] [CrossRef]
- Erickson, N.J.; Schmalz, P.G.R.; Agee, B.S.; Fort, M.; Walters, B.C.; McGrew, B.M.; Fisher, W.S. Koos Classification of Vestibular Schwannomas: A Reliability Study. Neurosurgery 2018, 85, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Müller, B.; Baum, A.; Holzhausen, M.; Grittner, U.; Hilgendorf, I.; Martus, P.; Altiner, A.; Evers, S.; Rolfs, A.; Zettl, U.K.; et al. Der Rostocker Kopfschmerzfragen-Komplex (“Rokoko”)—Validierung einer schnellen diagnostischen Hilfe bei der Einordnung primärer Kopfschmerzen. Fortschritte Neurol. Psychiatr. 2014, 82, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Lui, J.T.; Lee, J.J.W.; Ma, Y.; Dixon, P.R.; Crowson, M.G.; Dahm, V.; Shipp, D.B.; Chen, J.M.; Lin, V.Y. Glasgow Benefit Inventory in Cochlear Implantation. Otol. Neurotol. 2021, 42, e1464–e1469. [Google Scholar] [CrossRef]
- Geissner, E. Fragebogen zur Erfassung der Schmerzverarbeitung; Hogrefe: Göttingen, Germany, 2001. [Google Scholar]
- McCrae, R.R.; Costa, P.T. Validation of the five-factor model of personality across instruments and observers. J. Pers. Soc. Psychol. 1987, 52, 81. [Google Scholar] [CrossRef]
- Muck, P.M.; Hell, B.; Gosling, S.D. Construct validation of a short five-factor model instrument: A self-peer study on the German adaptation of the Ten-Item Personality Inventory (TIPI-G). Eur. J. Psychol. Assess. 2007, 23, 166. [Google Scholar] [CrossRef]
- Costa, P.T., Jr.; McCrae, R.R. The Revised Neo Personality Inventory (neo-pi-r); Sage Publications, Inc.: Thousand Oaks, CA, USA, 2008. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Mac; IBM Corp: Armonk, NY, USA, 2021. [Google Scholar]
- Benjamini, Y.; Yekutieli, D. False discovery rate–adjusted multiple confidence intervals for selected parameters. J. Am. Stat. Assoc. 2005, 100, 71–81. [Google Scholar] [CrossRef]
- Hemmerich, W. StatistikGuru: Rechner zur Adjustierung des α-Niveaus. 2016. Available online: https://statistikguru.de/rechner/adjustierung-des-alphaniveaus.html (accessed on 17 November 2023).
- Cohen, J. A power primer. In Methodological Issues and Strategies in Clinical Research, 4th ed.; American Psychological Association: Washington, DC, USA, 2016; pp. 279–284. [Google Scholar]
- Garnefski, N.; Kraaij, V. Cognitive coping and goal adjustment are associated with symptoms of depression and anxiety in people with acquired hearing loss. Int. J. Audiol. 2012, 51, 545–550. [Google Scholar] [CrossRef]
- Völter, C.; Götze, L.; Ballasch, I.; Harbert, L.; Dazert, S.; Thomas, J.P. Third-party disability in cochlear implant users. Int. J. Audiol. 2022, 21, 1059–1066. [Google Scholar] [CrossRef]
- Magyar, M.; Gonda, X.; Pap, D.; Edes, A.; Galambos, A.; Baksa, D.; Kocsel, N.; Szabo, E.; Bagdy, G.; Elliott, R.; et al. Decreased openness to experience is associated with migraine-type headaches in subjects with lifetime depression. Front. Neurol. 2017, 8, 270. [Google Scholar] [CrossRef]
- Chan, J.K.; Consedine, N.S. Negative affectivity, emotion regulation, and coping in migraine and probable migraine: A new zealand case–control study. Int. J. Behav. Med. 2014, 21, 851–860. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Maestre, C.; Martínez, A.E.L.; Zarazaga, R.E. Personality Characteristics as Differential Variables of the Pain Experience. J. Behav. Med. 2004, 27, 147–165. [Google Scholar] [CrossRef]
- Rosignoli, C.; Ornello, R.; Onofri, A.; Caponnetto, V.; Grazzi, L.; Raggi, A.; Leonardi, M.; Sacco, S. Applying a biopsychosocial model to migraine: Rationale and clinical implications. J. Headache Pain 2022, 23, 100. [Google Scholar] [CrossRef] [PubMed]
- Meints, S.M.; Edwards, R.R. Evaluating psychosocial contributions to chronic pain outcomes. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2018, 87, 168–182. [Google Scholar] [CrossRef] [PubMed]
- Scheidegger, A.; Jäger, J.; Blättler, L.T.; Aybek, S.; Bischoff, N.; Grosse Holtforth, M. Identification and Characterization of Pain Processing Patterns among Patients with Chronic Primary Pain: A Replication. Clin. J. Pain. 2023, 39, 414–425. [Google Scholar] [CrossRef] [PubMed]
- Grolimund, J.; Studer, M.; Stewart, J.A.; Egloff, N.; Grosse Holtforth, M. Typen der Schmerzverarbeitung bei Patienten mit chronischen Schmerzen. Schmerz 2018, 32, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Scheidegger, A.; Gómez Penedo, J.M.; Blättler, L.T.; Aybek, S.; Bischoff, N.; Grosse Holtforth, M. Improvements in pain coping predict treatment success among patients with chronic primary pain. J. Psychosom. Res. 2023, 168, 111208. [Google Scholar] [CrossRef]
- Hackshaw, A. Small studies: Strengths and limitations. Eur. Respir. J. Eur. Respir. Soc. 2008, 32, 1141–1143. [Google Scholar] [CrossRef]
- Ball, H.L. Conducting online surveys. J. Hum. Lact. 2019, 35, 413–417. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable/ Questionnaire Scale | Minimum | Maximum | M (SD) |
|---|---|---|---|
| Age | 30 | 75 | 53.94 (12.68) |
| Age at onset | 28 | 69 | 45.92 (10.04) |
| Time since treatment in years | 1 | 36 | 8.02 (9.36) |
| Pain (NAS) | 2 | 10 | 6.65 (2.13) |
| TIPI-G | |||
| Extraversion | 2 | 14 | 8.04 (3.20) |
| Agreeableness | 6 | 14 | 10.50 (2.23) |
| Conscientiousness | 8 | 14 | 12.37 (1.58) |
| Emotional stability | 2 | 14 | 9.6 (3.34) |
| Openness | 5 | 14 | 10.58 (2.48) |
| FESV | |||
| HD | 5 | 30 | 15.40 (7.71) |
| ANX | 4 | 24 | 10.77 (6.12) |
| ANG | 5 | 26 | 11.15 (6.29) |
| APC | 4 | 24 | 15.55 (5.33) |
| CR | 4 | 24 | 14.70 (5.56) |
| EC | 4 | 24 | 16.08 (5.56) |
| MD | 4 | 18 | 7.94 (4.01) |
| CA | 3 | 20 | 8.34 (4.30) |
| RR | 4 | 24 | 11.49 (5.58) |
| GBI | |||
| Global | −100.00 | 75.00 | −23.19 (34.93) |
| Social support | −83.33 | 66.67 | 0.31 (27.44) |
| Physical health | −83.33 | 33.33 | −21.96 (31.86) |
| Overall | −80.56 | 63.69 | −20.09 (25.68) |
| Questionnaire Scale | With POHs (n = 50) | Without POHs (n = 42) | p | FDR-Corrected p | Cohen’s d |
|---|---|---|---|---|---|
| GBI | |||||
| General | −23.4 (34.6) | −10.9 (27.5) | 0.16 | 0.21 | - |
| Social support | −0.9 (29.5) | 1.1 (20.6) | 0.56 | 0.56 | - |
| Physical health | −23.2 (32.0) | −9.1 (21.5) | 0.049 | 0.098 | - |
| Total | −20.7 (25.3) | −8.6 (19.9) | 0.01 | 0.04 | 0.52 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thomas, M.; Führes, H.; Scheer, M.; Rampp, S.; Strauss, C.; Schönfeld, R.; Leplow, B. Perceived Health Benefits in Vestibular Schwannoma Patients with Long-Term Postoperative Headache: Insights from Personality Traits and Pain Coping—A Cross-Sectional Study. J. Pers. Med. 2024, 14, 75. https://doi.org/10.3390/jpm14010075
Thomas M, Führes H, Scheer M, Rampp S, Strauss C, Schönfeld R, Leplow B. Perceived Health Benefits in Vestibular Schwannoma Patients with Long-Term Postoperative Headache: Insights from Personality Traits and Pain Coping—A Cross-Sectional Study. Journal of Personalized Medicine. 2024; 14(1):75. https://doi.org/10.3390/jpm14010075
Chicago/Turabian StyleThomas, Mareike, Hannah Führes, Maximilian Scheer, Stefan Rampp, Christian Strauss, Robby Schönfeld, and Bernd Leplow. 2024. "Perceived Health Benefits in Vestibular Schwannoma Patients with Long-Term Postoperative Headache: Insights from Personality Traits and Pain Coping—A Cross-Sectional Study" Journal of Personalized Medicine 14, no. 1: 75. https://doi.org/10.3390/jpm14010075
APA StyleThomas, M., Führes, H., Scheer, M., Rampp, S., Strauss, C., Schönfeld, R., & Leplow, B. (2024). Perceived Health Benefits in Vestibular Schwannoma Patients with Long-Term Postoperative Headache: Insights from Personality Traits and Pain Coping—A Cross-Sectional Study. Journal of Personalized Medicine, 14(1), 75. https://doi.org/10.3390/jpm14010075