

Influence of Augmented Reality Appliances on Tooth Preparation Designs—An In Vitro Study
 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Experimental Procedure
2.3. Alignment Procedure
2.4. Measurement Procedure
2.5. Statistical Tests
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yildirim, S.; Fu, S.Y.; Kim, K.; Zhou, H.; Lee, C.H.; Li, A.; Kim, S.G.; Wang, S.; Mao, J.J. Tooth regeneration: A revolution in stomatology and evolution in regenerative medicine. Int. J. Oral Sci. 2011, 3, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Cherukara, G.P.; Davis, G.R.; Seymour, K.G.; Zou, L.; Samarawickrama, D.Y. Dentin exposure in tooth preparations for porcelain veneers: A pilot study. J. Prosthet. Dent. 2005, 94, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S. Hinged Single Piece Putty Index for Preclinical Demonstration of Tooth Preparation for Fixed Partial Dentures and Crowns. J. Clin. Diagn. Res. 2015, 9, ZC09–ZC12. [Google Scholar] [CrossRef]
- Ram, H.K.; Shah, R.J.; Agrawal, H.S. Evaluation of three different tooth preparation techniques for metal ceramic crowns by comparing preparation depths: An in vitro study. J. Indian Prosthodont. Soc. 2015, 15, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.-T. Using silicone occlusal registration material as a guide for tooth preparation. J. Prosthet. Dent. 2004, 92, 302. [Google Scholar] [CrossRef] [PubMed]
- Yu, A.; Lee, H. A wax guide to measure the amount of occlusal reduction during tooth preparation in fixed prosthodontics. J. Prosthet. Dent. 2010, 103, 256–257. [Google Scholar] [CrossRef] [PubMed]
- Aminian, A.; Brunton, P.A. A comparison of the depths produced using three different tooth preparation techniques. J. Prosthet. Dent. 2003, 89, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Yee, S.; Richert, R.; Viguie, G.; Couraud, S.; Dehurtevent, M.; Fages, M.; Corne, P.; Ducret, M. Evaluation of the use of a guided bur during preclinical teaching of tooth preparation: A pilot study. Clin. Exp. Dent. Res. 2019, 5, 588–593. [Google Scholar] [CrossRef]
- Wang, S.; Zhao, W.; Ye, H.; Liu, Y.; Zhou, Y. Preliminary application and evaluation of digital step-by-step tooth-preparation templates. J. Prosthet. Dent. 2021, 130, 102–107. [Google Scholar] [CrossRef]
- Cho, S.H.; Nagy, W.W. Labial reduction guide for laminate veneer preparation. J. Prosthet. Dent. 2015, 114, 490–492. [Google Scholar] [CrossRef]
- Yu, H.; Zhao, Y.; Li, J.; Luo, T.; Gao, J.; Liu, H.; Liu, W.; Liu, F.; Zhao, K.; Liu, F.; et al. Minimal invasive microscopic tooth preparation in esthetic restoration: A specialist consensus. Int. J. Oral Sci. 2019, 11, 31. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.Y.; Bai, H.F.; Zhao, Y.J.; Wang, Y.; Ye, H.Q.; Sun, Y.C. 3D Evaluation of Accuracy of Tooth Preparation for Laminate Veneers Assisted by Rigid Constraint Guides Printed by Selective Laser Melting. Chin. J. Dent. Res. 2020, 23, 183–189. [Google Scholar] [CrossRef]
- Gao, J.; Li, J.; Liu, C.; Fan, L.; Yu, J.; Yu, H. A stereolithographic template for computer-assisted teeth preparation in dental esthetic ceramic veneer treatment. J. Esthet. Restor. Dent. 2020, 32, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Podhorsky, A.; Rehmann, P.; Wöstmann, B. Tooth preparation for full-coverage restorations—A literature review. Clin. Oral Investig. 2015, 19, 959–968. [Google Scholar] [CrossRef] [PubMed]
- da Silva, B.P.; Stanley, K.; Gardee, J. Laminate veneers: Preplanning and treatment using digital guided tooth preparation. J. Esthet. Restor. Dent. 2020, 32, 150–160. [Google Scholar] [CrossRef] [PubMed]
- Otani, T.; Raigrodski, A.J.; Mancl, L.; Kanuma, I.; Rosen, J. In vitro evaluation of accuracy and precision of automated robotic tooth preparation system for porcelain laminate veneers. J. Prosthet. Dent. 2015, 114, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; He, J.; Fan, L.; Lu, J.; Xie, C.; Yu, H. Accuracy of Reduction Depths of Tooth Preparation for Porcelain Laminate Veneers Assisted by Different Tooth Preparation Guides: An In Vitro Study. J. Prosthodont. 2022, 31, 593–600. [Google Scholar] [CrossRef]
- Gao, J.; Luo, T.; Zhao, Y.; Xie, C.; Yu, H. Accuracy of the preparation depth in mixed targeted restorative space type veneers assisted by different guides: An in vitro study. J. Prosthodont. Res. 2023, 67, 556–561. [Google Scholar] [CrossRef]
- Zitzmann, N.U.; Matthisson, L.; Ohla, H.; Joda, T. Digital Undergraduate Education in Dentistry: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 3269. [Google Scholar] [CrossRef]
- Joda, T.; Gallucci, G.; Wismeijer, D.; Zitzmann, N. Augmented and virtual reality in dental medicine: A systematic review. Comput. Biol. Med. 2019, 108, 93–100. [Google Scholar] [CrossRef]
- Rosella, D.; Rosella, G.; Brauner, E.; Papi, P.; Piccoli, L.; Pompa, G. A tooth preparation technique in fixed prosthodontics for students and neophyte dentists. Ann. Stomatol. 2016, 6, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Luo, T.; Zhang, J.; Fan, L.; Huang, Y.; Yu, J.; Yu, H. A digital workflow with the virtual enamel evaluation and stereolithographic template for accurate tooth preparation to conservatively manage a case of complex exogenous dental erosion. J. Esthet. Restor. Dent. 2022, 34, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.X.; Gao, J.; Zhao, Y.W.; Fan, L.; Jia, L.M.; Hu, N.; Mei, Z.Y.; Dong, B.; Zhang, Q.Q.; Yu, H.Y. Precise tooth preparation technique guided by 3D printing guide plate with quantitative hole. Hua Xi Kou Qiang Yi Xue Za Zhi 2020, 38, 350–355. (In Chinese) [Google Scholar]
- Liu, C.; Guo, J.; Gao, J.; Yu, H. Computer-assisted tooth preparation template and predesigned restoration: A digital workflow. Int. J. Comput. Dent. 2020, 23, 351–362. [Google Scholar] [PubMed]
- Sigcho López, D.A.; García, I.; Da Silva Salomao, G.; Cruz Laganá, D. Potential Deviation Factors Affecting Stereolithographic Surgical Guides: A Systematic Review. Implant. Dent. 2019, 28, 68–73. [Google Scholar] [CrossRef]
- Yu, H.Y. Guided micro tooth preparation: From new strategies to new clinical practices. Zhonghua Kou Qiang Yi Xue Za Zhi 2020, 55, 710–715. (In Chinese) [Google Scholar]
- Yeung, A.W.K.; Tosevska, A.; Klager, E.; Eibensteiner, F.; Laxar, D.; Stoyanov, J.; Glisic, M.; Zeiner, S.; Kulnik, S.T.; Crutzen, R.; et al. Virtual and Augmented Reality Applications in Medicine: Analysis of the Scientific Literature. J. Med. Internet Res. 2021, 23, e25499. [Google Scholar] [CrossRef]
- Huang, T.K.; Yang, C.H.; Hsieh, Y.H.; Wang, J.C.; Hung, C. Augmented reality (AR) and virtual reality (VR) applied in dentistry. Kaohsiung J. Med. Sci. 2018, 34, 243–248. [Google Scholar] [CrossRef]
- Mai, H.N.; Dam, V.V.; Lee, D.H. Accuracy of Augmented Reality–Assisted Navigation in Dental Implant Surgery: Systematic Review and Meta-analysis. J. Med. Internet Res. 2023, 25, e42040. [Google Scholar] [CrossRef]
- Farronato, M.; Maspero, C.; Lanteri, V.; Fama, A.; Ferrati, F.; Pettenuzzo, A.; Farronato, D. Current state of the art in the use of augmented reality in dentistry: A systematic review of the literature. BMC Oral Health 2019, 19, 135. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
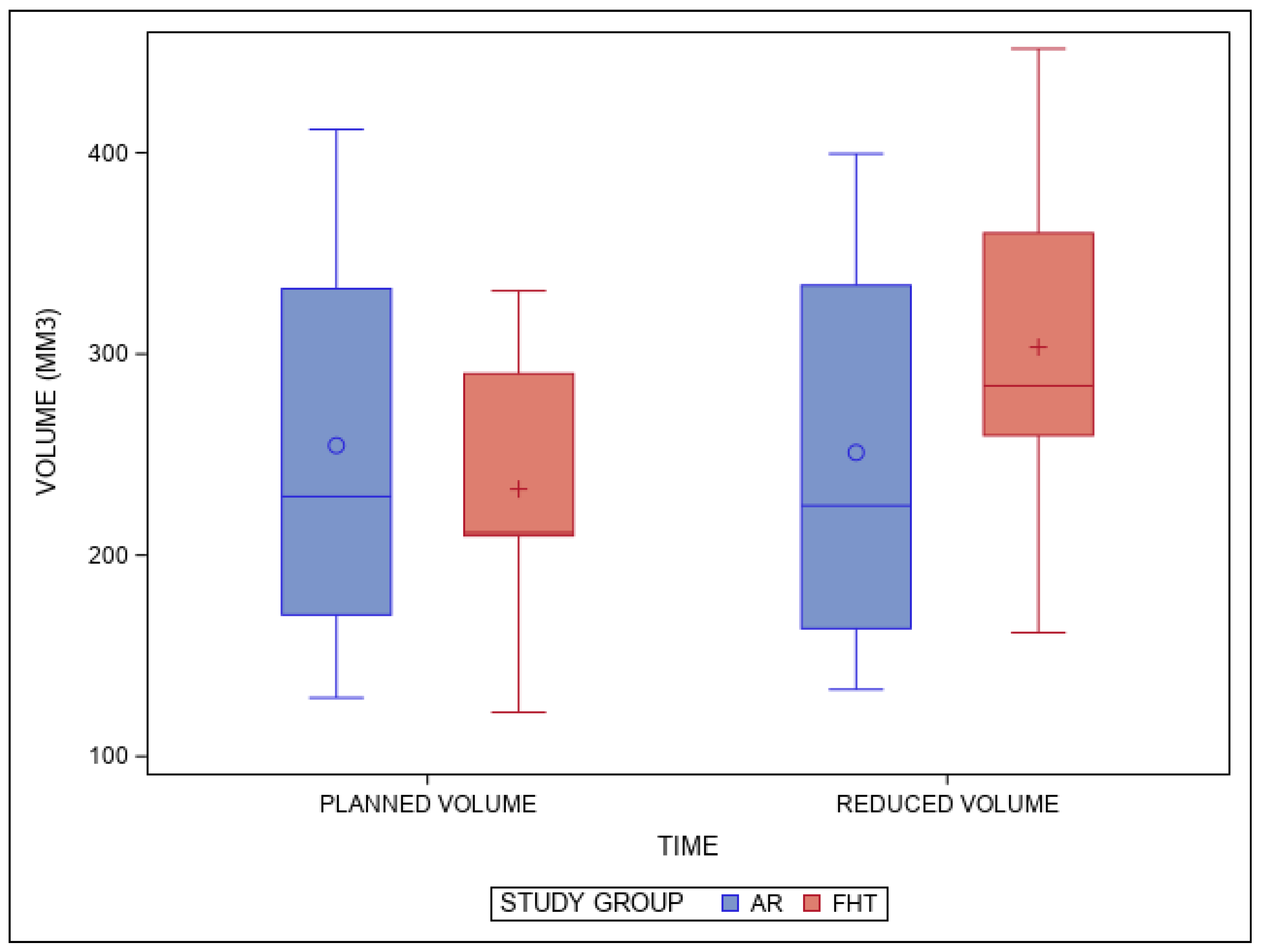
| Study Group | Variable | n | Mean | SD | Minimum | Maximum |
|---|---|---|---|---|---|---|
| AR | Planned volume | 5 | 254.54 a | 116.44 | 129.10 | 411.69 |
| Reduced volume | 5 | 251.03 a | 113.12 | 133.25 | 339.53 | |
| FHT | Planned volume | 5 | 232.87 a | 81.13 | 121.87 | 331.41 |
| Reduced volume | 5 | 303.43 b | 109.15 | 161.48 | 451.76 |
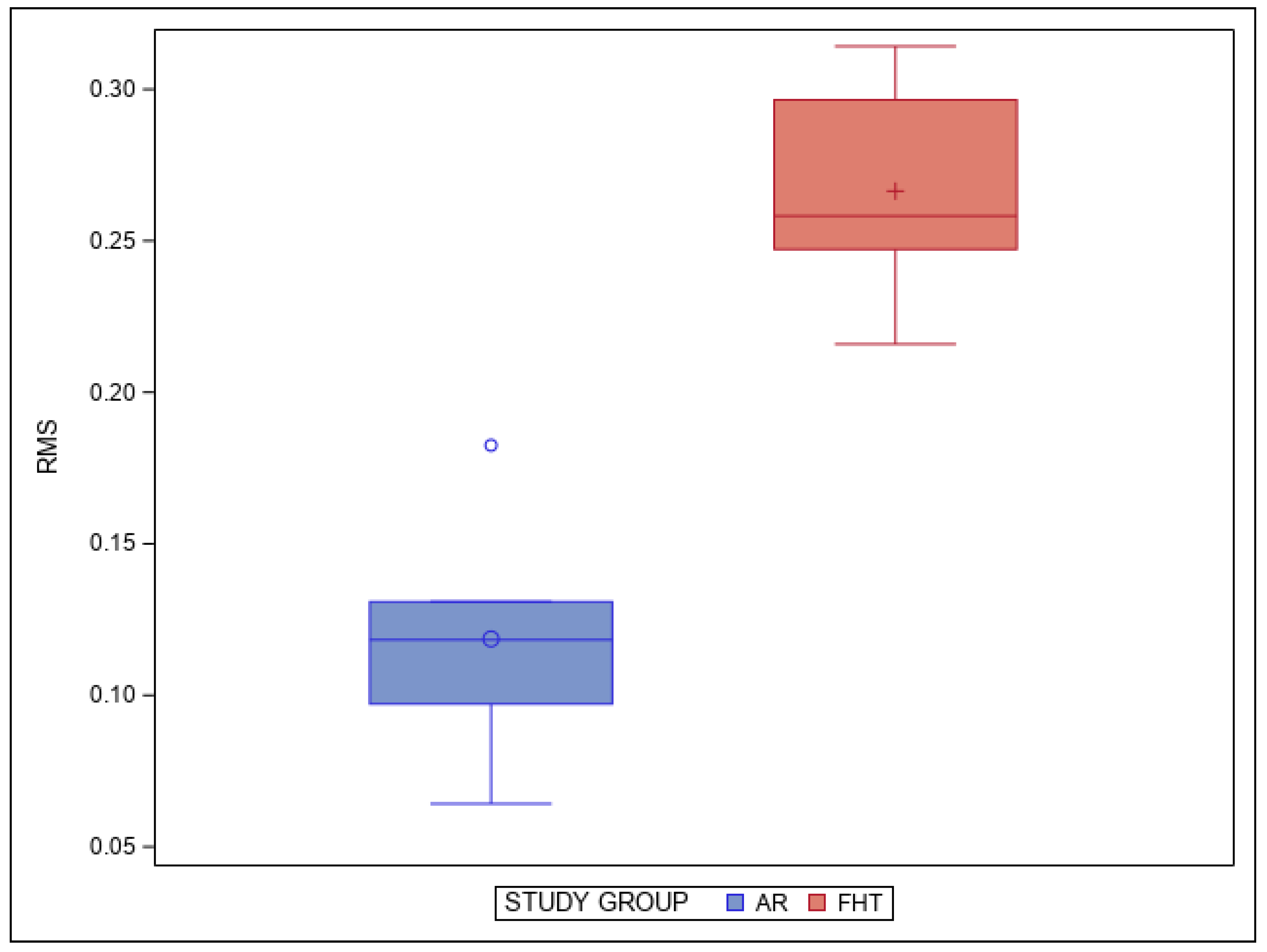
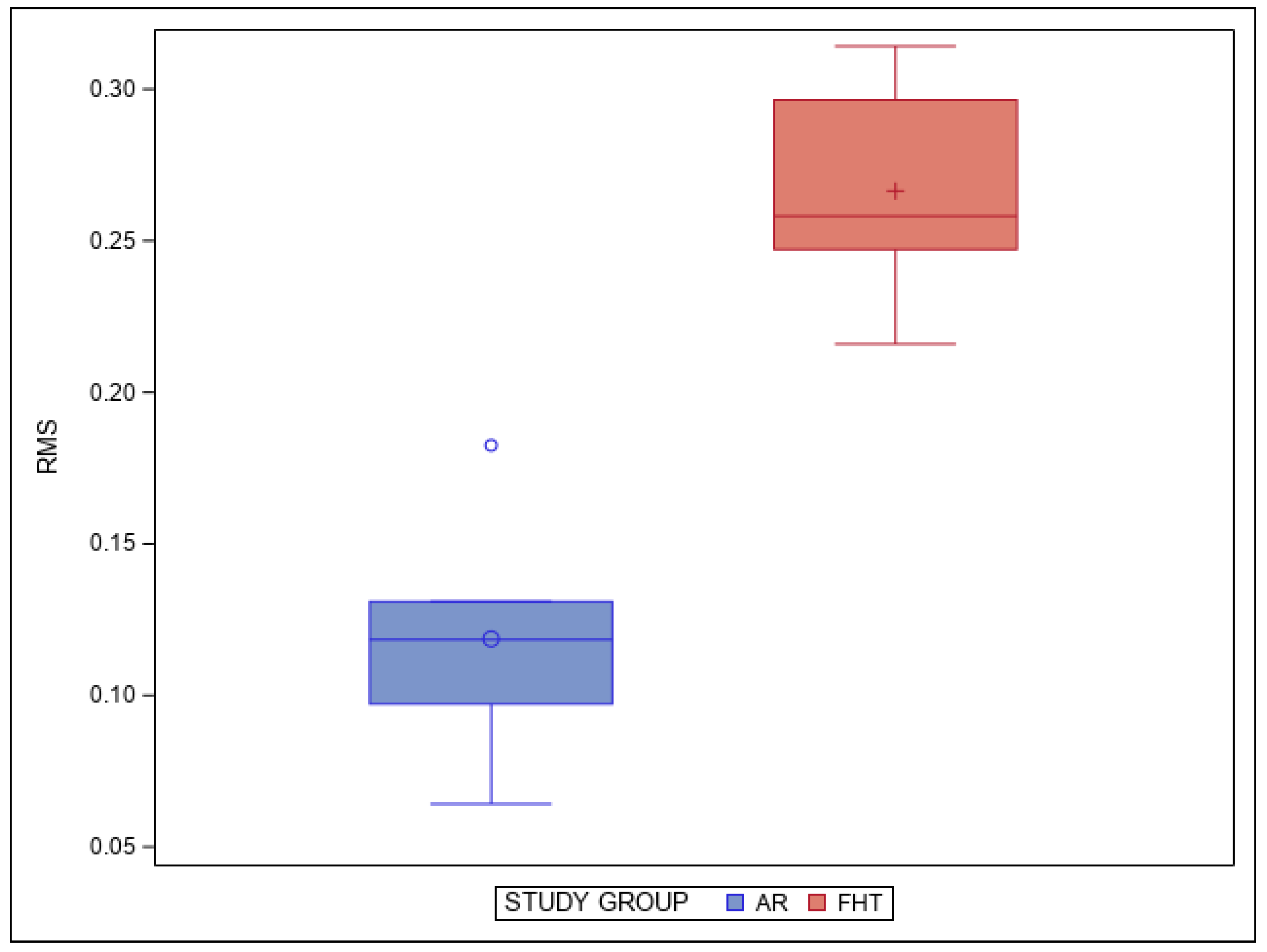
| Study Group | n | Mean | SD | Minimum | Maximum |
|---|---|---|---|---|---|
| AR | 5 | 0.12 a | 0.04 | 0.06 | 0.18 |
| FHT | 5 | 0.27 b | 0.04 | 0.22 | 0.31 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Obispo, C.; Gragera, T.; Giovannini, G.; Zubizarreta-Macho, Á.; Aragoneses Lamas, J.M. Influence of Augmented Reality Appliances on Tooth Preparation Designs—An In Vitro Study. J. Pers. Med. 2024, 14, 37. https://doi.org/10.3390/jpm14010037
Obispo C, Gragera T, Giovannini G, Zubizarreta-Macho Á, Aragoneses Lamas JM. Influence of Augmented Reality Appliances on Tooth Preparation Designs—An In Vitro Study. Journal of Personalized Medicine. 2024; 14(1):37. https://doi.org/10.3390/jpm14010037
Chicago/Turabian StyleObispo, Cristina, Teresa Gragera, Giovanni Giovannini, Álvaro Zubizarreta-Macho, and Juan Manuel Aragoneses Lamas. 2024. "Influence of Augmented Reality Appliances on Tooth Preparation Designs—An In Vitro Study" Journal of Personalized Medicine 14, no. 1: 37. https://doi.org/10.3390/jpm14010037
APA StyleObispo, C., Gragera, T., Giovannini, G., Zubizarreta-Macho, Á., & Aragoneses Lamas, J. M. (2024). Influence of Augmented Reality Appliances on Tooth Preparation Designs—An In Vitro Study. Journal of Personalized Medicine, 14(1), 37. https://doi.org/10.3390/jpm14010037