
Patient Perspectives of Barriers and Facilitators for the Uptake of Pharmacogenomic Testing in Veterans Affairs’ Pharmacogenomic Testing for the Veterans (PHASER) Program

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
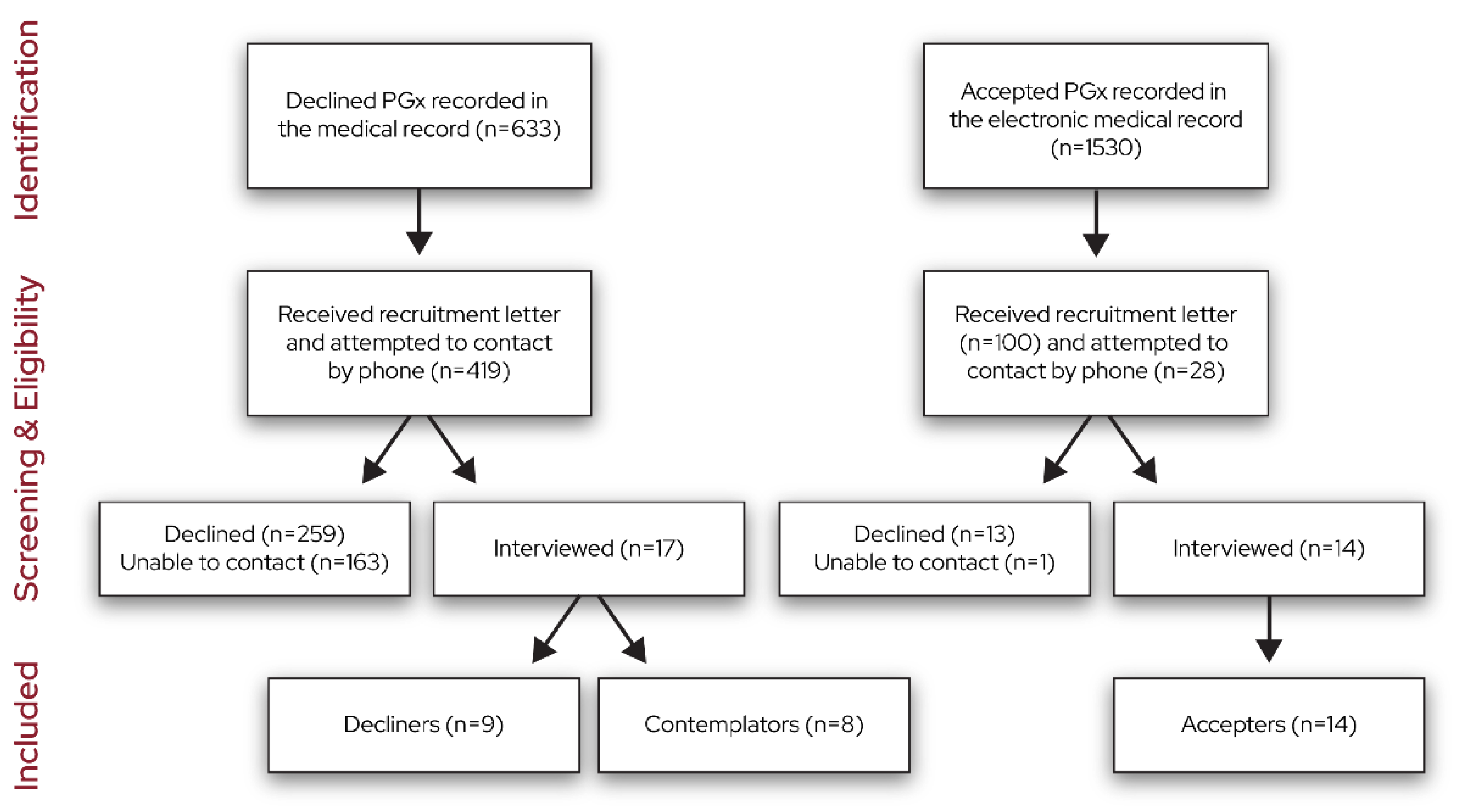
2.1. Design, Setting, and Participants
2.2. Procedures
2.3. Analysis
3. Results
3.1. Knowledge
3.2. Memory, Attention, and Decision Processes
3.3. Social Influence
3.4. Optimism
3.5. Environmental Context and Resources
3.6. Beliefs about Consequences
3.7. Emotion
3.8. Outcomes of Testing
3.9. Intentions
3.10. Suggestions for PHASER Program Improvement
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cacabelos, R.; Naidoo, V.; Corzo, L.; Cacabelos, N.; Carril, J.C. Genophenotypic factors and pharmacogenomics in adverse drug reactions. Int. J. Mol. Sci. 2021, 22, 13302. [Google Scholar] [CrossRef]
- Lee, Y.M.; McKillip, R.P.; Borden, B.A.; Klammer, C.E.; Ratain, M.J.; O’donnell, P.H. Assessment of patient perceptions of genomic testing to inform pharmacogenomic implementation. Pharm. Genom. 2017, 27, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Lemke, A.A.; Amendola, L.M.; Thompson, J.; Dunnenberger, H.M.; Kuchta, K.; Wang, C.; Dilzell-Yu, K.; Hulick, P.J. Patient-reported outcomes and experiences with population genetic testing offered through a primary care network. Genet. Test. Mol. Biomark. 2021, 25, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.; Varughese, L.A.; Conway, L.; Stojinski, C.; Ashokkumar, S.; Monono, K.; Matthai, W.; Kolansky, D.M.; Giri, J.; Tuteja, S. Attitudes toward pharmacogenetics in patients undergoing CYP2C19 testing following percutaneous coronary intervention. Pers. Med. 2022, 19, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Youssef, E.; Bhattacharya, D.; Sharma, R.; Wright, D.J. A theory-informed systematic review of barriers and enablers to implementing multi-drug pharmacogenomic testing. J. Pers. Med. 2022, 12, 1821. [Google Scholar] [PubMed]
- Dong, O.M.; Bates, J.; Chanfreau-Coffinier, C.; Naglich, M.; Kelley, M.J.; Meyer, L.J.; Icardi, M.; Vassy, J.L.; Sriram, P.; Heise, C.W.; et al. Veterans Affairs Pharmacogenomic Testing for Veterans (PHASER) clinical program. Pharmacogenomics 2021, 22, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Chanfreau-Coffinier, C.; Hull, L.E.; Lynch, J.A.; DuVall, S.L.; Damrauer, S.M.; Cunningham, F.E.; Voight, B.F.; Matheny, M.E.; Oslin, D.W.; Icardi, M.S.; et al. Projected prevalence of actionable pharmacogenetic variants and level A drugs prescribed among US Veterans Health Administration pharmacy users. JAMA Netw. Open 2019, 2, e195345. [Google Scholar] [CrossRef] [PubMed]
- Cane, J.; O’connor, D.; Michie, S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement. Sci. 2012, 7, 37. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, H.-F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J. Qualitative Inquiry and Research Design: Choose Among Five Approaches, 2nd ed.; Sage: Thousand Oaks, CA, USA, 2007. [Google Scholar]
- Wood, M.; Christy, R. Sampling for possibilities. Qual. Quant. 1999, 33, 185–202. [Google Scholar] [CrossRef]
- Strauss, A.; Corbin, J. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory; Sage: Thousand Oaks, CA, USA, 1990. [Google Scholar]
- Guest, G.; Bunce, A.; Johnson, L. How many interviews are enough?: An experiment with data saturation and variability. Field Methods 2006, 18, 59–82. [Google Scholar] [CrossRef]

{kind=link}
| Domain | Subdomain | Definition | Interview Question | Participant Group |
|---|---|---|---|---|
| Knowledge | Knowledge | Level of understanding of genetic testing and how it works. Discussion of how patient learned about genetic testing. | What do you know about using genetic information to pick a medicine? | Accepter, decliner, contemplator |
| What are your thoughts about using genetic testing to pick your medicines? What concerns do you have? | Contemplator | |||
| What would you like to know about genetic testing for medicines? | Contemplator | |||
| Procedural knowledge | Knowing how to get testing done and how to get results. | How did you learn about the opportunity at the VA to use genetic testing to choose your medicine? Tell me more about your discussion with your healthcare team. | Accepter, decliner | |
| How would you like to learn about genetic testing for medicines to make an informed decision? Do you have a preference for what method, for example, letter, in person, phone call? | Contemplator | |||
| Knowledge of task environment | Understanding of who will have access to their testing results (how it will be stored, how it will be accessed, for how long). | What is your understanding of who will have access to your information? What about how they will access it? Tell me about any reservations you have about safekeeping of your information. Probes: What concerns do you have about the privacy of your results? What concerns do you have about the effect on your benefits or insurance coverage? | Accepter, decliner, contemplator | |
| What is your understanding of who would have access to your results if you were to get PGx testing? Do you have any concerns about how PGx results will be kept? | Contemplator | |||
| Goals | Goals (distal/proximal) | Mental representations of outcomes or end states that an individual wants to achieve | How does testing fit your personal health goals, if at all? | Accepter |
| How does your decision relate to your personal health goals, if at all? | Decliner | |||
| (After brief description of PGx testing) What do you see as the benefits to your health? | Contemplator | |||
| Memory, attention, and decision processes | Decision-making | Process for choosing between two or more alternatives. How did patients make the decision to get tested or not? Or how would they make the decision? | How did you decide to get the test? | Accepter |
| How did you decide not to get the test? (Probe about logistics such as travel time, transportation, time off work, informational resources) | Decliner | |||
| What would make you consider getting PGx testing? Are there other factors that would influence your decision to get testing or not? | Contemplator | |||
| Social influences | Social norms | Who or what influenced the decision to get tested | Who or what influenced your decision to get testing/not get testing? (Probes: conversations with the healthcare provider, friends and family, people in your community, media or printed information) | Accepter |
| Optimism | Optimism | The confidence that things will happen for the best and that the VHA and providers act in veterans’ best interest. | How likely do you think it is that genetic testing will lead to better decisions about finding the right medicine for you? How likely do you think it is that genetic testing will lead to better decisions about improving your overall health? | Accepter, decliner |
| Pessimism | Attitude that things will go wrong and that VHA and providers do not act in veterans’ best interest. | Emerged unprompted | Emerged unprompted | |
| Environmental context | Person x environment interactions Salient events/critical incidents Environmental Stressors | Any circumstances of a person’s situation or environment that discourages or encourages the development of skills and abilities, independence, social competence, and adaptive behavior. Environment Can include access to VA clinics, family, justice system, testing on veterans/racial–ethnic minority groups. | Tell me about anything that made it easy for you to get the test? | Accepter |
| Tell me about anything that made it difficult to get the test. | Accepter | |||
| Beliefs about Consequences | Outcome expectancies | Discussion of what the consequences (drawbacks or benefits) would be if they got PGx testing. | What do you see as the benefits to you, if any, of using genetic information to make decisions about your medicines? What do you see as drawbacks? | Accepter, decliner |
| Intentions | A conscious decision to perform a behavior or a resolve to act in a certain way. Intent to be tested again or for the first time in the future. | Knowing what you do now, would you consider genetic testing for other medicines in the future? | Accepter | |
| Knowing what you do now, would you ever consider genetic testing in the future? If no: What would make you change your mind? If yes: Under what conditions would you consider it? | Decliner, contemplator | |||
| Emotions | Positive/ negative affect, anxiety, fear | Fear, anxiety, positive/negative affect as it relates to patient experience with PGx | Now that you have had the testing done, how do you feel about your decision? How does that compare to how you felt before you had the test? | Accepter |
| How do you feel about your decision now? How does that compare to how you felt before you declined testing? | Decliner | |||
| Outcomes of testing | N/A | Patient perceptions of how testing affected their health care, including prescriptions for medicines | What has happened to your care or medicines, if anything, as a result of having the genetic test? | Accepter |
| Process improvement | N/A | Suggestions for the VA for how to improve the PGx testing process. | How do you think the VA can improve the genetic testing process or experience for patients? | Accepter |
| What can the VA do better to inform other veterans about genetic testing for medicines? | Decliner, contemplator |
| Demographic Characteristic | Accepters (n = 14) | Decliners (n = 9) | Contemplators (n = 8) |
|---|---|---|---|
| Gender Male Female | |||
| 71% | 89% | 88% | |
| 29% | 11% | 12% | |
| Race White African American Native American/Alaskan Native Asian Native Hawaiian or Pacific Islander | 85.7% 7% 7% 7% | 55.6% 22% 11.1% 11.1% | 75% 25% 0% 0% |
| 7% | 0% | 0% | |
| Ethnicity Hispanic or Latino Not-Hispanic or Latino | |||
| 21.4% | 0% | 12.5% | |
| 78.6% | 100% | 87.5% | |
| Age (SD) | 60.3 (14.3) | 64.0 (16.8) | 62.4 (20.9) |
| Education High school graduate or equivalent Some college credit, but no degree Associate’s degree (AA or AS) Bachelor’s degree (BA or BS) Post-graduate work or degree | 7% 35.7% 28.6% 14.2% 14.3% | 11.1% 44.4% 25% 11.1% 11.1% | 12.5% 25% 25% 37.5% 0% |
| Marital Status Single, never married Married Divorced/separated Widowed | 7% 50% 26.7% 14.3% | 11.1% 33.3% 33.3% 11.1% | 0% 87.5% 12.5% 0% |
| Household Income $10,000–$19,999 $20,000–$29,999 $30,000–$39,999 $40,000–$49,999 $50,000–$59,999 $60,000–$79,999 $80,000 or more | 7.1% 7.1% 21.4% 7.1% 28.6% 7.1% 7.1% | 11.1% 11.1% 22.2% 0% 11.1% 11.1% 22.2% | 0% 12.5% 25% 12.5% 0% 25% 25% |
| Domain | Subdomain | Accepter Quotes | Contemplator Quotes | Decliner Quotes |
|---|---|---|---|---|
| Knowledge | Knowledge | Well, what I understood from this test was it basically measures the metabolism of your liver enzymes and how they work with certain medications. But the test also isn’t specific enough to say, I guess, which ones work and don’t. Just maybe how you would process it if it did work, if that makes sense. (nH White female) | I don’t really know much about the genetic testing. I never done it. I know that they prescribe different medications for me, and they try to find the best ones for me, the most effective medicine for me. But as far as the genetic testing, I don’t know much about it. (African American male) | I think this is the program to see what drugs that I would be amicable with based on a genetic, you know, on my genotype as far as how I am receptive to certain drugs to help me for whatever malady that I may have. It is a valid thing, except there are so many things wrong with me that I don’t see what the purpose is for me. (Asian male) |
| Procedural knowledge | I have to go in for regular lab work anyway, so they just lumped it in with the rest of my lab work… I mean, it was just another day of going to the VA. (nH White female) | I wasn’t exactly sure what I would have to do. (African American male) | She [primary care provider] gave me a pamphlet with information about the [clinic], and then there was also a page about the PHASER testing. It tells me benefits and improves access to treatment, reduces trial and error. I mean, it’s, you know, I go down and get a blood draw, no big deal. (nH White male) | |
| Knowledge of task environment | I’m sure that it’s in my records. So, anyone that I’m seeing, you know, for care and treatment, I’m thinking they’re the ones that would be able to get my genetic testing. (Hispanic white male) | I have no problem with it. I’ve had tests done before, and it was confidential, and they kept the information between me and the VA physicians and stayed in my medical records. So no, I’m not worried about it. (African American male) | Well, I mean, with technology, the way it is, you know, your genetic DNA could get misused on other things that it’s not meant for, which I don’t know what it could be used for. But, you know, that could be something negative. It could be put in the wrong hands and be used for something negative. (African American male) | |
| Goals | Personal Goals (distal/proximal) | I am hoping that … by getting off all these medications that I don’t really need, you know, that I can have a more clear mind, be able to, you know, function better, have a, have the ability to live a better quality of life. (AI/AN White female) | Hopefully if my medication does become less effective or develop another condition that requires medication, that I wouldn’t have to take the medication that gave me real bad side effects and could just go to the ones that work. (Hispanic White male) | Right now, I’m on three hypertensive medications, and I want to drop one. When I have my annual--it should be either this month or the end of next month--I want to talk about that again with my provider. (African American female) |
| Memory, attention, and decision processes | Decision-making | So, the healthcare provider suggesting it, for one, that was step one. But I guess before step one was my negative experience with side effects from medication. (nH White male) | I wasn’t exactly sure what was entailed. And, at that time, I wasn’t, didn’t feel that interested, and I didn’t do any research or background check, and so I just decided not to participate. (African American male) | I was in a negative frame of mind, and I still am regarding medicine. The prescriptions they have given me have done nothing. They have not influenced what’s going on with my [condition redacted to protect privacy] whatsoever. And so, I don’t know that genetic testing is going to help that at all. I doubt it. (nH White male) |
| Social influences | Social norms | She [veteran’s friend] told me about it [PGx testing] when her mental health team first suggested it. And so, we were kind of like, eh, she’s going to try this, and we’re going to kind of sit back and watch and see what happens. And her test results came back, and she sat down with her doctor and went over the test results. And they immediately switched her meds around. It was such immediate improvement, such a quick improvement after going over the results with her. (nH White Female) | N/A | N/A |
| Optimism | Optimism | Well, my goal is to try to stay as healthy as I can because I’m getting up there in the age where I need to stay healthy so I can stay alive. That’s my main goal: to stay healthy. I wanted to know that I was taking the right medicine so I could stay healthy. (nH White male) | There are some [benefits]. When I first started seeing a psychiatrist, I had some really bad side effects. Hopefully if my medication does become less effective or I develop another condition that requires medication, I wouldn’t have to take the medication that gave me real bad side effects and could just go to the ones that work. (Hispanic White male) | I think it’s a good opportunity, so they don’t have to try so many [medications] to get it right. (AI/AN male) |
| Pessimism | N/A | N/A | In a way, I just thought it was a waste of time. I mean, it is testing me, taking blood from me. How is that going to help the next veteran? It’s just for that, the individual person, right? (nH White male) | |
| Environmental context | Person x environment interactions Salient events/critical incidents Environmental Stressors | Well, me and my healthcare person have already been over them, and we think we’re doing real good. Nothing’s conflicting with anything, and the results came back good. So, we think we’re on the right, we’re doing the right thing. (nH White male) | It’s just, my PCP is like 25 min away, so, yeah, I mean, timing does have a little bit to do with it. And the VA hospital is about a 30-min drive away. So, if I had, you know, something 15 min away or 10 min away, it would be much easier to go over on a lunch break or something like that and get things like that taken care of. (nH White male) | I know that they can’t harm me if I don’t do it, and if I do, there could be possibilities of something coming up negatively in the future of my DNA used for this, my DNA used for that. I don’t know…The government has tested people without their knowledge and done things to the people without their knowledge. And find out later there was something negative that the government have done to people. (African American male) |
| Beliefs about consequences | Outcome expectancies | So, some people might view it as a waste of time or an unnecessary test, but for me it was very necessary. Because if I would have been waiting on that and took a pause and a break and waiting on those test results, I may have potentially agreed to allowing them to try some other medications and would have wound up with the same problem or worse. (Hispanic White male) | N/A | I’m just a single female. I don’t see how genetic testing is going to benefit because I’m 77 years old. I think I’ll be 78 this month. And genetic testing, I don’t understand how that’s going to work in my behalf because I am single with no children. (nH White female) |
| Intentions | I would do anything to help myself and to help other veterans, of course. I would do another genetic testing if it was more specific… Like specific to the medication that would work. (H White, male) | There’s a possibility. I have a lot of medical issues going on right now. So now that I have a little more information on it, if the opportunity presented itself again, then there’s a possibility that I might go ahead and do it. (African American male) | Well, I can’t predict the future, and I know that that I’m always subject to changing my mind. That’s, the older I get, the more I learn every day from my own mistakes. And it may happen that I see this as a mistake. It hasn’t yet. (nH White, male) | |
| Emotions | Positive/negative affect, anxiety, fear | Oh, I felt that, I’m just really grateful I had that opportunity. I could cry. I mean, that’s, not everybody can get that done. I don’t know what something like that costs. I don’t have a clue, but I just feel honored that I could, and humbled that I could get that done, you know. (nH White, female) | N/A | Just kind of like just anxiety, just having that kind of, yeah, specific detail, just your genetic makeup being handed over to, you know, VA is not necessarily the most trustworthy entity. (nH White, male) |
| Outcomes of testing | [I feel] good, very good, because there’s not a question in the back ofmy mind if I’m going to keep trying medications, which I’m not. So that’s, for me, that’sa big thing I can check off the boxes. I’m not going to be playing around trying to figureout what concoction of chemicals works or doesn’t work. (H White, male) | N/A | N/A | |
| Process improvement | I think it needs to be more readily available to everybody right now. (nH White female) | I think maybe if I was provided a pamphlet with information, what the testing would be used for exactly, who would have that information, know what exactly they’re looking for. (nH White male) | Maybe more information just because, and it’s like when you say we’re going to use your DNA to test, to, say, test to see if we use the right medication for the right people. It’s like, when they say it like that, it’s like a more clinical thing. Like it’s not personal. You understand? …Maybe make it a little bit more personal instead of like more cut-and-dry clinical. (African American male) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melendez, K.; Gutierrez-Meza, D.; Gavin, K.L.; Alagoz, E.; Sperber, N.; Wu, R.R.; Silva, A.; Pati, B.; Voora, D.; Hung, A.; et al. Patient Perspectives of Barriers and Facilitators for the Uptake of Pharmacogenomic Testing in Veterans Affairs’ Pharmacogenomic Testing for the Veterans (PHASER) Program. J. Pers. Med. 2023, 13, 1367. https://doi.org/10.3390/jpm13091367
Melendez K, Gutierrez-Meza D, Gavin KL, Alagoz E, Sperber N, Wu RR, Silva A, Pati B, Voora D, Hung A, et al. Patient Perspectives of Barriers and Facilitators for the Uptake of Pharmacogenomic Testing in Veterans Affairs’ Pharmacogenomic Testing for the Veterans (PHASER) Program. Journal of Personalized Medicine. 2023; 13(9):1367. https://doi.org/10.3390/jpm13091367
Chicago/Turabian StyleMelendez, Karina, Diana Gutierrez-Meza, Kara L. Gavin, Esra Alagoz, Nina Sperber, Rebekah Ryanne Wu, Abigail Silva, Bhabna Pati, Deepak Voora, Allison Hung, and et al. 2023. "Patient Perspectives of Barriers and Facilitators for the Uptake of Pharmacogenomic Testing in Veterans Affairs’ Pharmacogenomic Testing for the Veterans (PHASER) Program" Journal of Personalized Medicine 13, no. 9: 1367. https://doi.org/10.3390/jpm13091367
APA StyleMelendez, K., Gutierrez-Meza, D., Gavin, K. L., Alagoz, E., Sperber, N., Wu, R. R., Silva, A., Pati, B., Voora, D., Hung, A., Roberts, M. C., & Voils, C. I. (2023). Patient Perspectives of Barriers and Facilitators for the Uptake of Pharmacogenomic Testing in Veterans Affairs’ Pharmacogenomic Testing for the Veterans (PHASER) Program. Journal of Personalized Medicine, 13(9), 1367. https://doi.org/10.3390/jpm13091367