
YAP Activation Is Associated with a Worse Prognosis of Poorly Cohesive Gastric Cancer


 ,
,  , ,
, ,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analyses
3. Results
3.1. Series Description
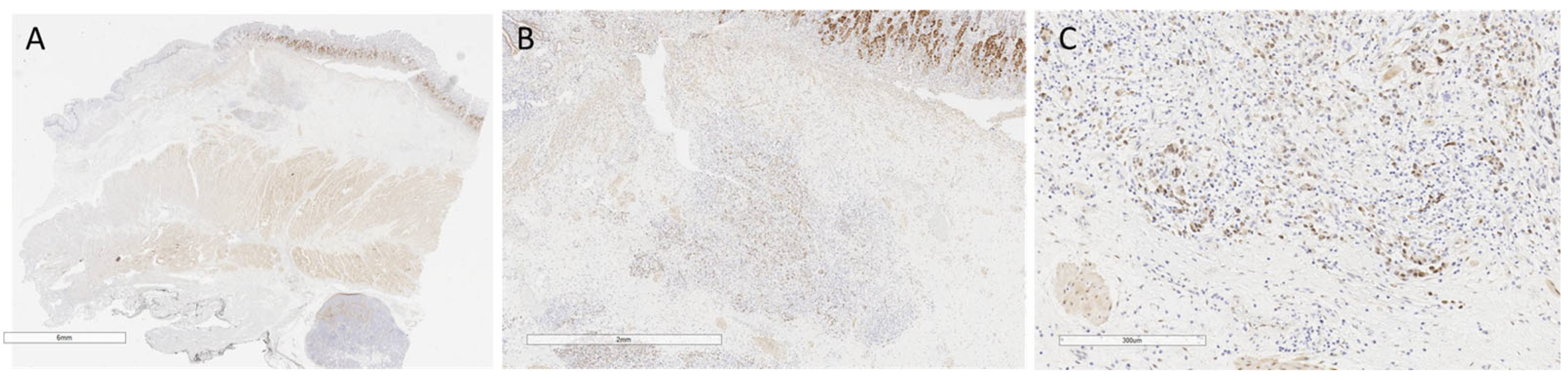
3.2. Immunohistochemistry Characterization
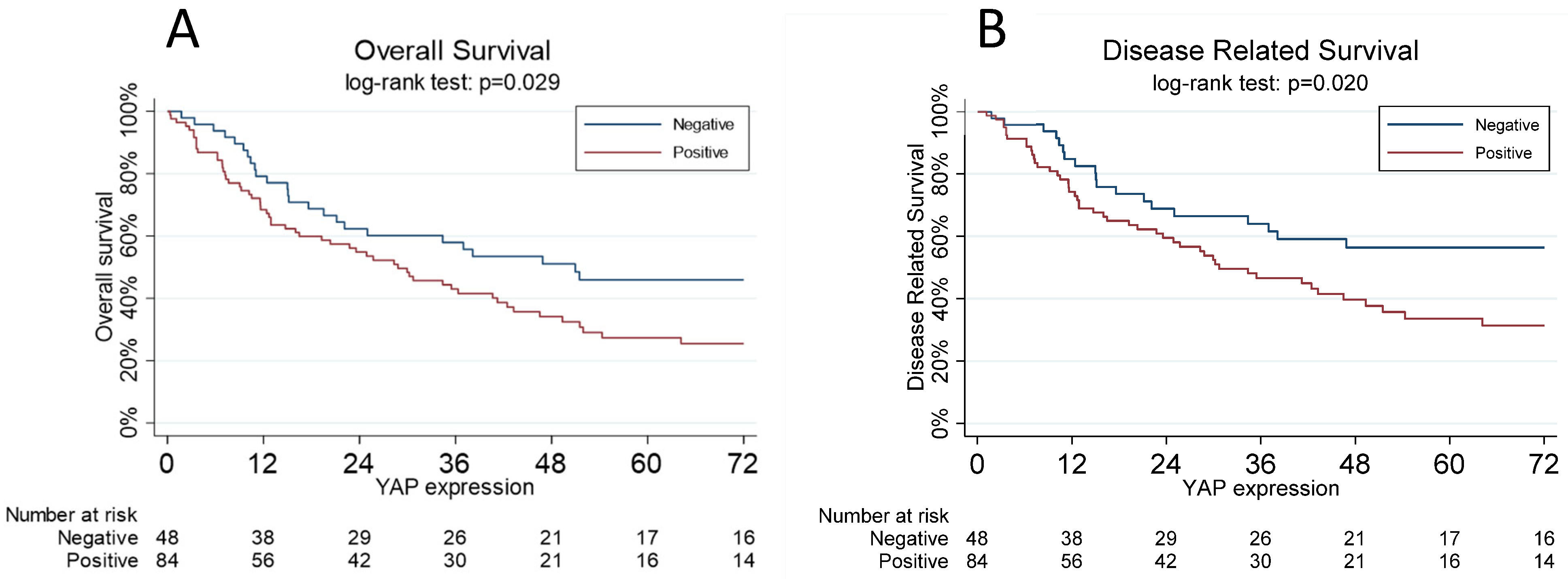
3.3. Association of YAP with Cancer Stage and Prognosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Sagaert, X.; Topal, B.; Haustermans, K.; Prenen, H. Gastric cancer. Lancet 2016, 388, 2654–2664. [Google Scholar]
- Correa, P. Human gastric carcinogenesis: A multistep and multifactorial process—First American Cancer Society Award Lecture on Cancer Epidemiology and Prevention. Cancer Res. 1992, 52, 6735–6740. [Google Scholar] [PubMed]
- Bass, A.J.; Thorsson, V.; Shmulevich, I.; Reynolds, S.M.; Miller, M.; Bernard, B.; Hinoue, T.; Laird, P.W.; Curtis, C.; Shen, H.; et al. Comprehensive molecular characterization of gastric adenocarcinoma. Nature 2014, 513, 202–209. [Google Scholar]
- Lauren, P. The Two Histological Main Types of Gastric Carcinoma: Diffuse and So-Called Intestinal-Type Carcinoma. An Attempt at a Histo-Clinical Classification. Acta Pathol. Microbiol. Scand. 1965, 64, 31–49. [Google Scholar] [CrossRef]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A.; The WHO Classification of Tumours Editorial Board. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef]
- National Cancer Institute. Available online: https://seer.cancer.gov/statistics/ (accessed on 1 July 2023).
- Bamboat, Z.M.; Tang, L.H.; Vinuela, E.; Kuk, D.; Gonen, M.; Shah, M.A.; Brennan, M.F.; Coit, D.G.; Strong, V.E. Stage-stratified prognosis of signet ring cell histology in patients undergoing curative resection for gastric adenocarcinoma. Ann. Surg. Oncol. 2014, 21, 1678–1685. [Google Scholar] [CrossRef]
- Messager, M.; Lefevre, J.H.; Pichot-Delahaye, V.; Souadka, A.; Piessen, G.; Mariette, C. The impact of perioperative chemotherapy on survival in patients with gastric signet ring cell adenocarcinoma: A multicenter comparative study. Ann Surg. 2011, 254, 684–693; discussion 693. [Google Scholar] [CrossRef]
- Kwon, C.H.; Kim, Y.K.; Lee, S.; Kim, A.; Park, H.J.; Choi, Y.; Won, Y.J.; Park, D.Y.; Lauwers, G.Y. Gastric poorly cohesive carcinoma: A correlative study of mutational signatures and prognostic significance based on histopathological subtypes. Histopathology 2018, 72, 556–568. [Google Scholar] [CrossRef]
- Wang, K.; Yuen, S.T.; Xu, J.; Lee, S.P.; Yan, H.H.N.; Shi, S.T.; Siu, H.C.; Deng, S.; Chu, K.M.; Law, S.; et al. Whole-genome sequencing and comprehensive molecular profiling identify new driver mutations in gastric cancer. Nat. Genet. 2014, 46, 573–582. [Google Scholar] [CrossRef]
- Guan, R.; Xu, X.; Chen, M.; Hu, H.; Ge, H.; Wen, S.; Zhou, S.; Pi, R. Advances in the studies of roles of Rho/Rho-kinase in diseases and the development of its inhibitors. Eur. J. Med. Chem. 2013, 70, 613–622. [Google Scholar] [CrossRef] [PubMed]
- Shang, X.; Marchioni, F.; Evelyn, C.R.; Sipes, N.; Zhou, X.; Seibel, W.; Wortman, M.; Zheng, Y. Small-molecule inhibitors targeting G-protein-coupled Rho guanine nucleotide exchange factors. Proc. Natl. Acad. Sci. USA 2013, 110, 3155–3160. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Chiwaki, F.; Kojima, S.; Kawazu, M.; Komatsu, M.; Ueno, T.; Inoue, S.; Sekine, S.; Matsusaki, K.; Matsushita, H.; et al. Multi-omic profiling of peritoneal metastases in gastric cancer identifies molecular subtypes and therapeutic vulnerabilities. Nat. Cancer 2021, 2, 962–977. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.W.T.; Sheng, T.; Xing, M.; Ooi, W.F.; Xu, C.; Sundar, R.; Huang, K.K.; Li, Z.; Kumar, V.; Ramnarayanan, K.; et al. Regulatory enhancer profiling of mesenchymal-type gastric cancer reveals subtype-specific epigenomic landscapes and targetable vulnerabilities. Gut 2023, 72, 226–241. [Google Scholar] [CrossRef]
- Moroishi, T.; Hansen, C.G.; Guan, K.-L. The emerging roles of YAP and TAZ in cancer. Nat. Rev. Cancer 2015, 15, 73–79. [Google Scholar] [CrossRef]
- Zhao, Y.; Yang, X. The Hippo pathway in chemotherapeutic drug resistance. Int. J. Cancer 2015, 137, 2767–2773. [Google Scholar] [CrossRef]
- Piccolo, S.; Dupont, S.; Cordenonsi, M. The biology of YAP/TAZ: Hippo signaling and beyond. Physiol. Rev. 2014, 94, 1287–1312. [Google Scholar] [CrossRef]
- Edwards, D.C.; Sanders, L.C.; Bokoch, G.M.; Gill, G.N. Activation of LIM-kinase by Pak1 couples Rac/Cdc42 GTPase signalling to actin cytoskeletal dynamics. Nat. Cell Biol. 1999, 1, 253–259. [Google Scholar] [CrossRef]
- Mana-Capelli, S.; Paramasivam, M.; Dutta, S.; McCollum, D. Angiomotins link F-actin architecture to Hippo pathway signaling. Mol. Biol. Cell. 2014, 25, 1676–1685. [Google Scholar] [CrossRef]
- Mariette, C.; Carneiro, F.; Grabsch, H.I.; van der Post, R.S.; Allum, W.; de Manzoni, G. Consensus on the pathological definition and classification of poorly cohesive gastric carcinoma. Gastric Cancer 2019, 22, 1–9. [Google Scholar] [CrossRef]
- Steinhardt, A.A.; Gayyed, M.F.; Klein, A.P.; Dong, J.; Maitra, A.; Pan, D.; Montgomery, E.A.; Anders, R.A. Expression of Yes-associated protein in common solid tumors. Hum. Pathol. 2008, 39, 1582–1589. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Kim, D.-H.; Shah, S.R.; Kim, H.-N.; Kshitiz; Kim, P.; Quiñones-Hinojosa, A.; Levchenko, A. Switch-like enhancement of epithelial-mesenchymal transition by YAP through feedback regulation of WT1 and Rho-family GTPases. Nat. Commun. 2019, 10, 2797. [Google Scholar] [PubMed]
- Yong, J.; Li, Y.; Lin, S.; Wang, Z.; Xu, Y. Inhibitors Targeting YAP in Gastric Cancer: Current Status and Future Perspectives. Drug Des. Devel. Ther. 2021, 15, 2445–2456. [Google Scholar] [CrossRef] [PubMed]
- Messina, B.; Sardo, F.L.; Scalera, S.; Memeo, L.; Colarossi, C.; Mare, M.; Blandino, G.; Ciliberto, G.; Maugeri-Saccà, M.; Bon, G. Hippo pathway dysregulation in gastric cancer: From Helicobacter pylori infection to tumor promotion and progression. Cell Death Dis. 2023, 14, 21. [Google Scholar]
- Zhang, H.; Schaefer, A.; Wang, Y.; Hodge, R.G.; Blake, D.R.; Diehl, J.N.; Papageorge, A.G.; Stachler, M.D.; Liao, J.; Zhou, J.; et al. Gain-of-Function RHOA Mutations Promote Focal Adhesion Kinase Activation and Dependency in Diffuse Gastric Cancer. Cancer Discov. 2020, 10, 288–305. [Google Scholar] [CrossRef]
- van Rensburg, H.J.J.; Azad, T.; Ling, M.; Hao, Y.; Snetsinger, B.; Khanal, P.; Minassian, L.M.; Graham, C.H.; Rauh, M.J.; Yang, X. The Hippo Pathway Component TAZ Promotes Immune Evasion in Human Cancer through PD-L1. Cancer Res. 2018, 78, 1457–1470. [Google Scholar] [CrossRef]
- Hsu, P.; Miao, J.; Wang, Y.; Zhang, W.; Yang, Y.; Wang, C.; Yang, C.; Huang, Z.; You, J.; Xu, Z.; et al. nhibition of yes-associated protein down-regulates PD-L1 (CD274) expression in human malignant pleural mesothelioma. J. Cell. Mol. Med. 2018, 22, 3139–3148. [Google Scholar] [CrossRef]
- Kim, M.H.; Kim, C.G.; Kim, S.-K.; Shin, S.J.; Choe, E.A.; Park, S.-H.; Shin, E.-C.; Kim, J. YAP-Induced PD-L1 Expression Drives Immune Evasion in BRAFi-Resistant Melanoma. Cancer Immunol. Res. 2018, 6, 255–266. [Google Scholar] [CrossRef]
- Lee, B.S.; Park, D.I.; Lee, D.H.; Lee, J.E.; Yeo, M.-K.; Park, Y.H.; Lim, D.S.; Choi, W.; Yoo, G.; Kim, H.-B.; et al. Hippo effector YAP directly regulates the expression of PD-L1 transcripts in EGFR-TKI-resistant lung adenocarcinoma. Biochem. Biophys. Res. Commun. 2017, 491, 493–499. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Total n = 133 (%) | ||
|---|---|---|
| Sex (women) | 69 (52.7) | |
| Age 1 | 64.3 (53–74.5) | |
| cT * | cT1 | 8 (7.3) |
| cT2 | 10 (9.1) | |
| cT3 | 44 (40.0) | |
| cT4 | 48 (43.6) | |
| cN * | N0 | 39 (35.5) |
| N+ | 71 (64.5) | |
| cM * | cM0 | 103 (93.6) |
| cM1 | 7 (6.4) | |
| Neoadjuvant therapy * | Chemotherapy | 13 (10.0) |
| Chemo + radiotherapy | 1 (0.8) | |
| No treatment | 116 (89.2) | |
| Adjuvant therapy * | Chemotherapy | 35 (36.5) |
| Radiotherapy | 2 (2.1) | |
| Chemo + radiotherapy | 15 (15.6) | |
| No treatment | 44 (45.8) | |
| Gastrectomy | Total | 68 (51.1) |
| Sub-total | 65 (48.9) | |
| Lymphadenectomy | D1 | 34 (25.6) |
| D2 | 72 (54.1) | |
| D3 | 27 (20.3) | |
| Total lymph nodes harvested 1 | 36 (23–45) | |
| Total positive lymph nodes 1 | 7 (0–15) | |
| Resection of adjacent organs (including cholecystectomy) | Yes | 94 (70.7) |
| No | 39 (29.3) | |
| Curativity | R0 | 106 (79.7) |
| R1 | 15 (11.3) | |
| R2 | 12 (9.0) | |
| SRC group * | <10% | 34 (26.8) |
| 10–90% | 78 (61.4) | |
| >90% | 15 (11.8) | |
| pT | pT1 | 21 (15.8) |
| pT2 | 7 (5.3) | |
| pT3 | 30 (22.5) | |
| pT4 | 75 (56.4) | |
| pN * | pN0 | 39 (29.8) |
| pN1 | 11 (8.4) | |
| pN2 | 18 (13.7) | |
| pN3 | 63 (48.1) | |
| pM | pM0 | 113 (85.0) |
| pM1 | 20 (15.0) | |
| Length of hospital stay (days) 1 | 8 (7–10) |
| Total n = 133 (%) | |
|---|---|
| Recurrence 1 | |
| Yes | 75 (59.2) |
| No | 51 (40.5) |
| Loco-regional recurrence 1 | |
| Yes | 24 (24.0) |
| No | 76 (76.0) |
| Time of recurrence (months) 2 | 11.7 (7.4–24.4) |
| Distant metastases 1 | |
| Yes | 8 (6.1) |
| No | 124 (93.9) |
| Death 1 | |
| Yes | 84 (67.7) |
| No | 40 (32.3) |
| Cause of death 1 | |
| Therapy-related | 1 (1.2) |
| Cancer-related | 68 (82.9) |
| Other | 13 (15.8) |
| Total n = 133 | |
|---|---|
| YAP | |
| Positive | 85 (63.9) |
| Negative | 48 (36.1) |
| YAP grade | |
| High | 46 (34.6) |
| Low | 39 (29.3) |
| Negative | 48 (36.1) |
| YAP percentage 1 | 10 (0–20) |
| Total n = 133 | YAP Expression | p-Value | |
|---|---|---|---|
| Negative n = 48 (%) | Positive n = 85 (%) | ||
| Sex | 0.104 | ||
| M | 18 (37.5) | 44 (53.0) | |
| F | 30 (62.5) | 39 (47.0) | |
| Age 1 | 64 (47–77) | 64 (55–73) | 0.882 |
| cT | 0.039 | ||
| cT1 | 4 (10.3) | 4 (5.6) | |
| cT2 | 7 (18.0) | 3 (4.2) | |
| cT3 | 16 (41.0) | 28 (39.4) | |
| cT4 | 12 (30.7) | 36 (50.7) | |
| cN | 0.408 | ||
| cN0 | 16 (41.0) | 23 (32.4) | |
| cN+ | 23 (59.0) | 48 (67.6) | |
| cM | 1.00 | ||
| M0 | 37 (94.9) | 66 (92.9) | |
| M1 | 2 (5.1) | 5 (7.1) | |
| Neoadjuvant therapy | 0.164 | ||
| Chemotherapy | 2 (4.4) | 11 (13.1) | |
| Chemo + radiotherapy | 0 | 1 (1.2) | |
| No treatment | 44 (95.6) | 72 (85.7) | |
| Adjuvant therapy | 0.573 | ||
| Chemotherapy | 13 (36.1) | 22 (36.7) | |
| Radiotherapy | 0 | 2 (3.3) | |
| Chemo + radiotherapy | 4 (11.1) | 11 (18.3) | |
| No treatment | 19 (52.8) | 25 (41.7) | |
| Gastrectomy | 1.00 | ||
| Total | 25 (52.1) | 43 (50.6) | |
| Sub-total | 23 (47.9) | 42 (49.4) | |
| Other resection | 0.241 | ||
| Yes | 11 (22.9) | 28 (32.9) | |
| No | 37 (77.1) | 57(67.1) | |
| Lymphadenectomy | 0.544 | ||
| D1 | 10 (20.8) | 24 (28.4) | |
| D2 | 29 (60.4) | 43 (50.6) | |
| D3 | 9 (18.8) | 18 (21.2) | |
| Total lymph nodes harvested 1 | 33.5 (23–45) | 36 (23.0–44) | 0.818 |
| Total positive lymph nodes 1 | 6 (0–18) | 7 (0–13) | 0.856 |
| pT | 0.507 | ||
| 1–2 | 12 (25.0) | 16 (18.8) | |
| 3–4 | 36 (75.0) | 69 (81.2) | |
| pN | 0.542 | ||
| 0 | 16 (34.0) | 23 (27.4) | |
| 1–2 | 8 (17.0) | 21 (25.0) | |
| >3 | 23 (49.0) | 40 (47.6) | |
| pM | 0.801 | ||
| 0 | 40 (83.3) | 73 (85.9) | |
| 1 | 8 (16.7) | 12 (14.1) | |
| Curativity | 0.159 | ||
| R0 | 41 (85.4) | 65 (76.5) | |
| R1 | 2 (4.2) | 13 (15.3) | |
| R2 | 5 (10.4) | 7 (8.2) | |
| SRC group | 0.412 | ||
| <10% | 14 (31.1) | 20 (24.4) | |
| >10% | 31 (68.9) | 62 (75.6) | |
| Recurrence | 0.256 | ||
| Yes | 23 (52.3) | 52 (63.4) | |
| No | 21 (47.7) | 30 (36.6) | |
| Loco-regional recurrence | 0.806 | ||
| Yes | 7 (21.9) | 17 (25.0) | |
| No | 25 (78.1) | 51 (75.0) | |
| Time of recurrence (months) 1 | 15.8 (9.3–32.2) | 10.1 (5.9–20.2) | 0.173 |
| Metastases | 0.139 | ||
| Yes | 5 (10.4) | 3 (3.6) | |
| No | 43 (89.6) | 81 (96.4) | |
| Days of hospitalization 1 | 7.5 (6.5–8.5) | 8 (7.0–13.0) | 0.157 |
| Death | 0.071 | ||
| Yes | 25 (56.8) | 59 (73.7) | |
| No | 19 (43.2) | 21 (26.3) | |
| Cause of death | 1.00 | ||
| Therapy-related | 0 | 1 (1.7) | |
| Cancer-related | 19 (82.6) | 49 (83.0) | |
| Other | 4 (17.4) | 9 (15.3) | |
| Haz. Ratio | 95% CI | p-Value | |
|---|---|---|---|
| Sex | |||
| (F vs. M) | 0.70 | 0.43–1.14 | 0.156 |
| Age | 1.03 | 1.01–1.04 | 0.001 |
| pT (3–4 vs. 1–2) | 3.61 | 1.44–8.98 | 0.006 |
| pN | |||
| (1–2 vs. 0) | 4.16 | 1.88–9.16 | <0.001 |
| (>3 vs. 0) | 3.50 | 1.70–7.21 | 0.001 |
| YAP | |||
| (Positive vs. negative) | 2.03 | 1.18–3.51 | 0.011 |
| SRC | |||
| (≥10% vs. <10%) | 0.98 | 0.55–1.72 | 0.910 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bencivenga, M.; Torroni, L.; Dal Cero, M.; Quinzii, A.; Zecchetto, C.; Merz, V.; Casalino, S.; Taus, F.; Pietrobono, S.; Mangiameli, D.; et al. YAP Activation Is Associated with a Worse Prognosis of Poorly Cohesive Gastric Cancer. J. Pers. Med. 2023, 13, 1294. https://doi.org/10.3390/jpm13091294
Bencivenga M, Torroni L, Dal Cero M, Quinzii A, Zecchetto C, Merz V, Casalino S, Taus F, Pietrobono S, Mangiameli D, et al. YAP Activation Is Associated with a Worse Prognosis of Poorly Cohesive Gastric Cancer. Journal of Personalized Medicine. 2023; 13(9):1294. https://doi.org/10.3390/jpm13091294
Chicago/Turabian StyleBencivenga, Maria, Lorena Torroni, Mariagiulia Dal Cero, Alberto Quinzii, Camilla Zecchetto, Valeria Merz, Simona Casalino, Francesco Taus, Silvia Pietrobono, Domenico Mangiameli, and et al. 2023. "YAP Activation Is Associated with a Worse Prognosis of Poorly Cohesive Gastric Cancer" Journal of Personalized Medicine 13, no. 9: 1294. https://doi.org/10.3390/jpm13091294
APA StyleBencivenga, M., Torroni, L., Dal Cero, M., Quinzii, A., Zecchetto, C., Merz, V., Casalino, S., Taus, F., Pietrobono, S., Mangiameli, D., Filippini, F., Alloggio, M., Castelli, C., Iglesias, M., Pera, M., & Melisi, D. (2023). YAP Activation Is Associated with a Worse Prognosis of Poorly Cohesive Gastric Cancer. Journal of Personalized Medicine, 13(9), 1294. https://doi.org/10.3390/jpm13091294