

Bony Regrowth and New Spur Formation as Possible Causes of Failed Distal Clavicle Excision—Mid-Term Outcomes after Revision Surgery in a Matched-Pair Analysis


 ,
,
Abstract
1. Introduction:
2. Methods
2.1. Study Population
2.2. Surgical Techniques
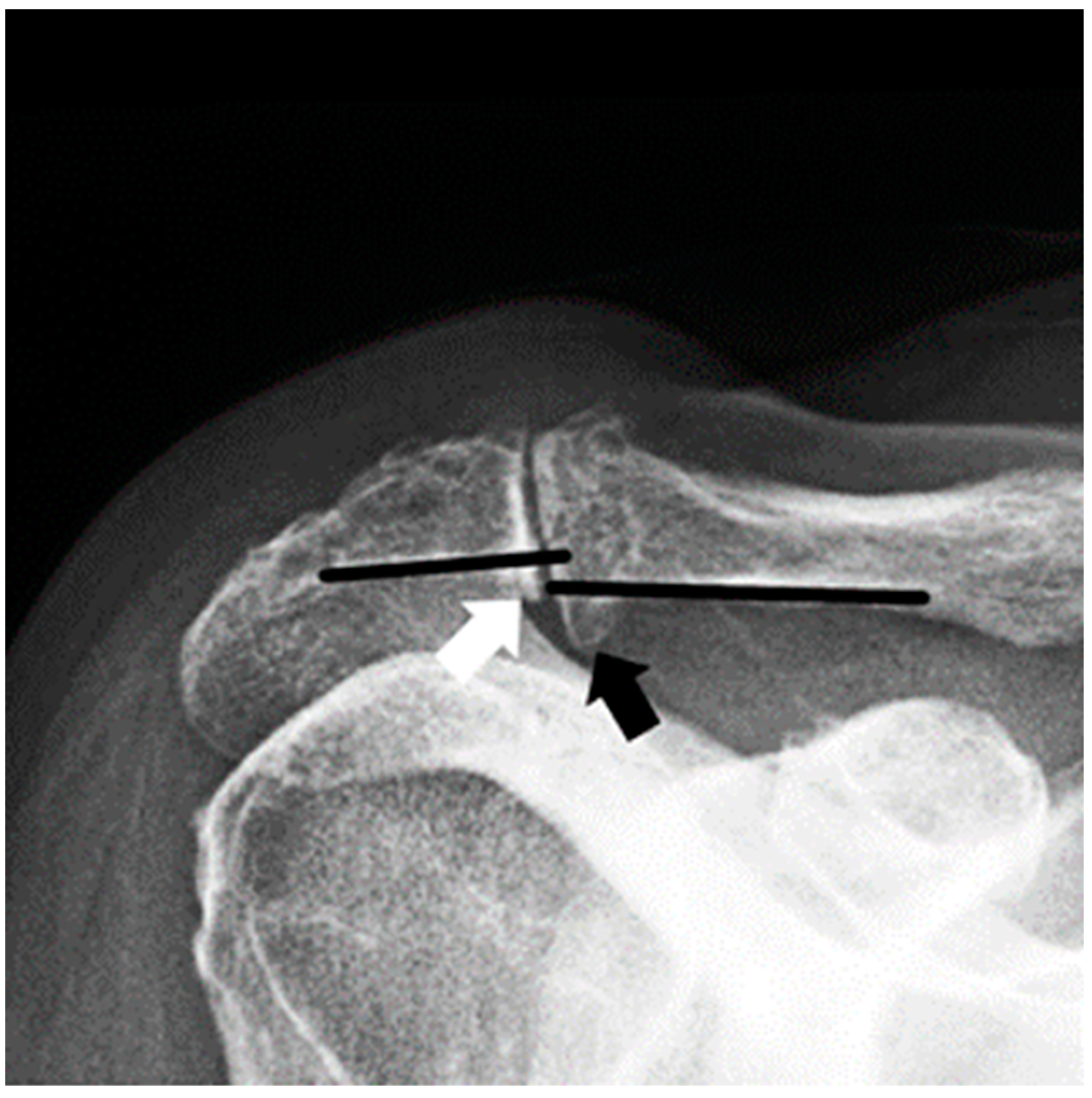
2.3. Clinical and Radiographic Assessment
2.4. Statistical Analysis
3. Results
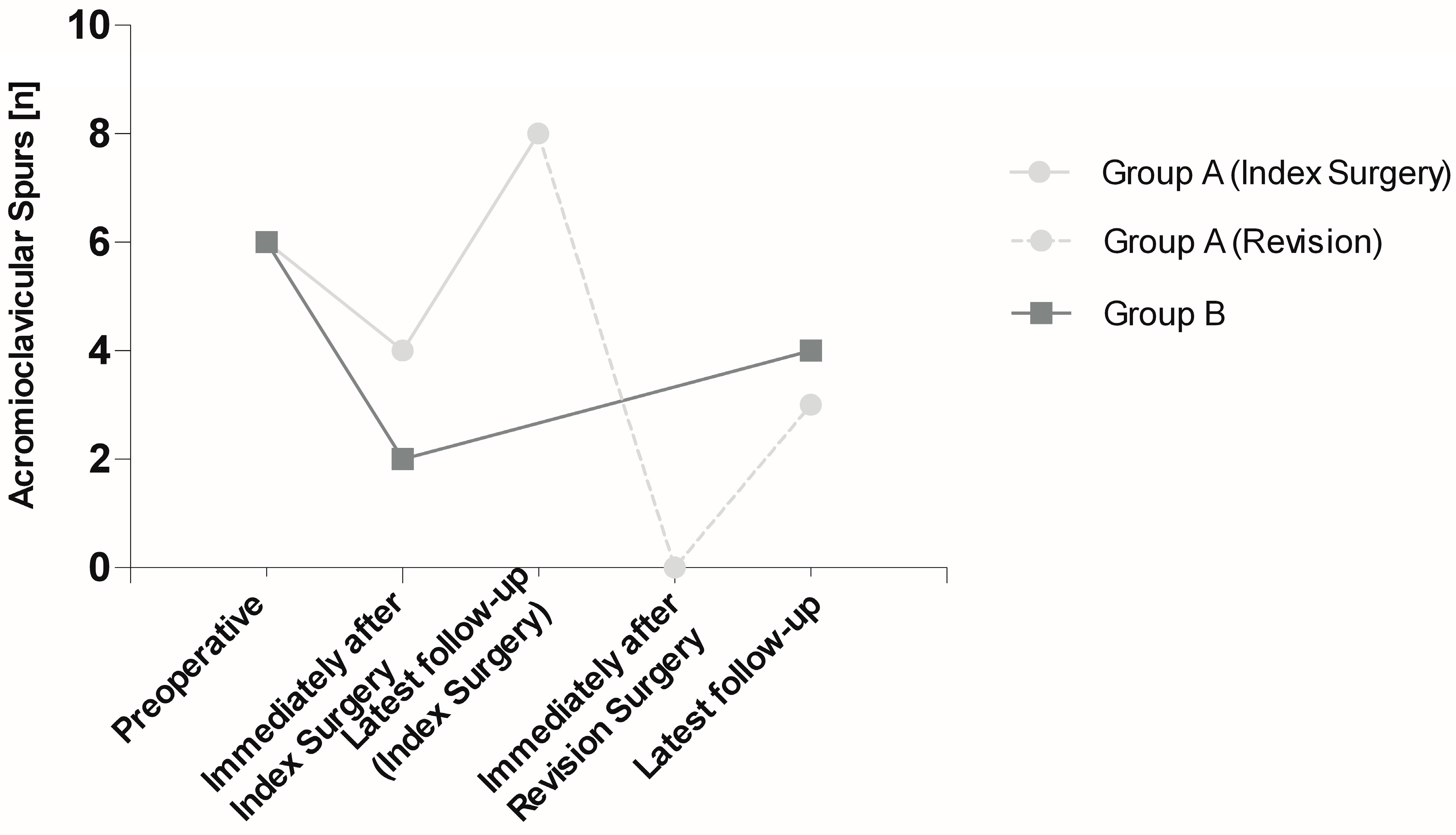
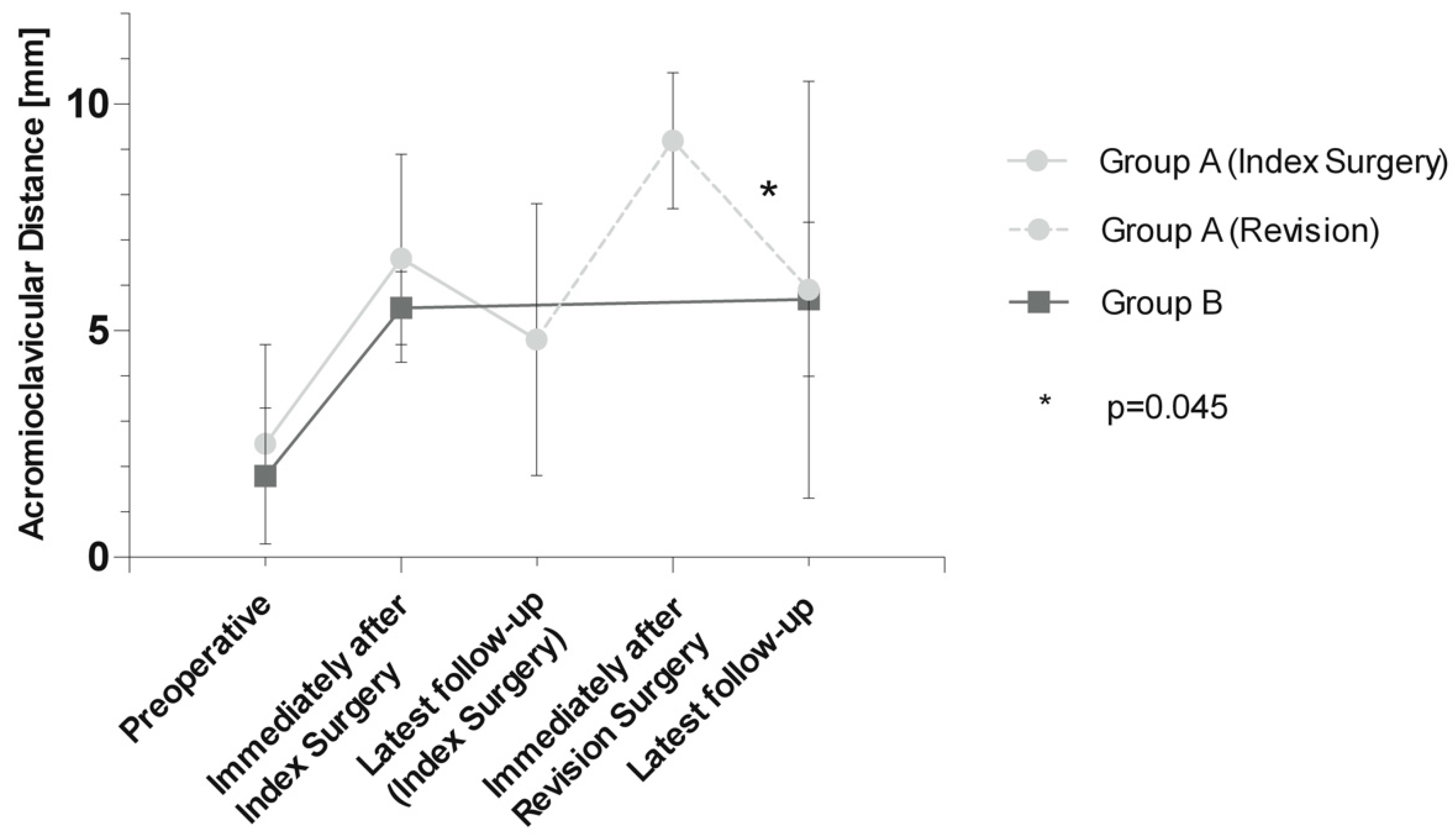
3.1. Radiographic Assessment
3.2. Functional and Subjective Assessment
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
List of Abbreviations
| ACD | Acromioclavicular joint distance | DCE | Distal clavicle excision |
| ACJ | Acromioclavicular joint | qDASH | QuickDASH score |
| ASES | American Shoulder and Elbow Surgeons score | SST | Simple shoulder test |
| CS | Constant Score | SSV | Subjective Shoulder Value |
| CT | Computed tomography | VAS | Visual analog scale |
References
- Rabalais, R.D.; McCarty, E. Surgical treatment of symptomatic acromioclavicular joint problems: A systematic review. Clin. Orthop. Relat. Res. 2007, 455, 30–37. [Google Scholar] [CrossRef]
- Robertson, W.J.; Griffith, M.H.; Carroll, K.; O’Donnell, T.; Gill, T.J. Arthroscopic versus open distal clavicle excision: A comparative assessment at intermediate-term follow-up. Am. J. Sports Med. 2011, 39, 2415–2420. [Google Scholar] [CrossRef] [PubMed]
- Mall, N.A.; Foley, E.; Chalmers, P.N.; Cole, B.J.; Romeo, A.A.; Bach, B.R., Jr. Degenerative joint disease of the acromioclavicular joint: A review. Am. J. Sports Med. 2013, 41, 2684–2692. [Google Scholar] [CrossRef] [PubMed]
- Chronopoulos, E.; Gill, H.S.; Freehill, M.T.; Petersen, S.A.; McFarland, E.G. Complications after open distal clavicle excision. Clin. Orthop. Relat. Res. 2008, 466, 646–651. [Google Scholar] [CrossRef] [PubMed]
- Freedman, B.A.; Javernick, M.A.; O’Brien, F.P.; Ross, A.E.; Doukas, W.C. Arthroscopic versus open distal clavicle excision: Comparative results at six months and one year from a randomized, prospective clinical trial. J. Shoulder Elb. Surg. 2007, 16, 413–418. [Google Scholar] [CrossRef]
- Mumford, E.B. Acromioclavicular dislocation (A new operative treatment). J. Bone Jt. Surg. 1941, 23, 799–802. [Google Scholar]
- Gurd, F.B. The Treatment of Complete Dislocation of the Outer End of the Clavicle: An Hitherto Undescribed Operation. Ann. Surg. 1941, 113, 1094–1098. [Google Scholar] [CrossRef]
- Jerosch, J.; Steinbeck, J.; Schroder, M.; Castro, W.H. Arthroscopic resection of the acromioclavicular joint (ARAC). Knee Surg. Sports Traumatol. Arthrosc. 1993, 1, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Elhassan, B.; Ozbaydar, M.; Diller, D.; Massimini, D.; Higgins, L.D.; Warner, J.J. Open versus arthroscopic acromioclavicular joint resection: A retrospective comparison study. Arthroscopy 2009, 25, 1224–1232. [Google Scholar] [CrossRef]
- Pensak, M.; Grumet, R.C.; Slabaugh, M.A.; Bach, B.R., Jr. Open versus arthroscopic distal clavicle resection. Arthroscopy 2010, 26, 697–704. [Google Scholar] [CrossRef]
- Levine, W.N.; Soong, M.; Ahmad, C.S.; Blaine, T.A.; Bigliani, L.U. Arthroscopic distal clavicle resection: A comparison of bursal and direct approaches. Arthroscopy 2006, 22, 516–520. [Google Scholar] [CrossRef] [PubMed]
- Corteen, D.P.; Teitge, R.A. Stabilization of the clavicle after distal resection: A biomechanical study. Am. J. Sports Med. 2005, 33, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Kharrazi, F.D.; Busfield, B.T.; Khorshad, D.S. Acromioclavicular joint reoperation after arthroscopic subacromial decompression with and without concomitant acromioclavicular surgery. Arthroscopy 2007, 23, 804–808. [Google Scholar] [CrossRef]
- Constant, C.R.; Murley, A.H. A clinical method of functional assessment of the shoulder. Clin. Orthop. Relat. Res. 1987, 214, 160–164. [Google Scholar] [CrossRef]
- Huskisson, E.C. Measurement of pain. Lancet 1974, 2, 1127–1131. [Google Scholar] [CrossRef]
- Gilbart, M.K.; Gerber, C. Comparison of the subjective shoulder value and the Constant score. J. Shoulder Elb. Surg. 2007, 16, 717–721. [Google Scholar] [CrossRef] [PubMed]
- Angst, F.; Schwyzer, H.K.; Aeschlimann, A.; Simmen, B.R.; Goldhahn, J. Measures of adult shoulder function: Disabilities of the Arm, Shoulder, and Hand Questionnaire (DASH) and its short version (QuickDASH), Shoulder Pain and Disability Index (SPADI), American Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form, Constant (Murley) Score (CS), Simple Shoulder Test (SST), Oxford Shoulder Score (OSS), Shoulder Disability Questionnaire (SDQ), and Western Ontario Shoulder Instability Index (WOSI). Arthritis Care Res. 2011, 63 (Suppl. 11), S174–S188. [Google Scholar]
- Michener, L.A.; McClure, P.W.; Sennett, B.J. American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form, patient self-report section: Reliability, validity, and responsiveness. J. Shoulder Elb. Surg. 2002, 11, 587–594. [Google Scholar] [CrossRef]
- Hudak, P.L.; Amadio, P.C.; Bombardier, C. Development of an upper extremity outcome measure: The DASH (disabilities of the arm, shoulder and hand) [corrected]. The Upper Extremity Collaborative Group (UECG). Am. J. Ind. Med. 1996, 29, 602–608. [Google Scholar] [CrossRef]
- Zanca, P. Shoulder pain: Involvement of the acromioclavicular joint. (Analysis of 1000 cases). Am. J. Roentgenol. Radium Ther. Nucl. Med. 1971, 112, 493–506. [Google Scholar] [CrossRef]
- Boehm, T.D.; Kirschner, S.; Fischer, A.; Gohlke, F. The relation of the coracoclavicular ligament insertion to the acromioclavicular joint: A cadaver study of relevance to lateral clavicle resection. Acta Orthop. Scand. 2003, 74, 718–721. [Google Scholar] [CrossRef]
- Eskola, A.; Santavirta, S.; Viljakka, H.T.; Wirta, J.; Partio, T.E.; Hoikka, V. The results of operative resection of the lateral end of the clavicle. J. Bone Jt. Surg. Am. 1996, 78, 584–587. [Google Scholar] [CrossRef] [PubMed]
- Beitzel, K.; Sablan, N.; Chowaniec, D.M.; Obopilwe, E.; Cote, M.P.; Arciero, R.A.; Mazzocca, A.D. Sequential resection of the distal clavicle and its effects on horizontal acromioclavicular joint translation. Am. J. Sports Med. 2012, 40, 681–685. [Google Scholar] [CrossRef]
- Branch, T.P.; Burdette, H.L.; Shahriari, A.S.; Carter, F.M., 2nd; Hutton, W.C. The role of the acromioclavicular ligaments and the effect of distal clavicle resection. Am. J. Sports Med. 1996, 24, 293–297. [Google Scholar] [CrossRef]
- Wang, J.; Ma, J.X.; Zhu, S.W.; Jia, H.B.; Ma, X.L. Does Distal Clavicle Resection Decrease Pain or Improve Shoulder Function in Patients With Acromioclavicular Joint Arthritis and Rotator Cuff Tears? A Meta-analysis. Clin. Orthop. Relat. Res. 2018, 476, 2402–2414. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.B.; Koh, K.H.; Shon, M.S.; Park, Y.E.; Yoo, J.C. Arthroscopic distal clavicle resection in symptomatic acromioclavicular joint arthritis combined with rotator cuff tear: A prospective randomized trial. Am. J. Sports Med. 2015, 43, 985–990. [Google Scholar] [CrossRef]
- Blazar, P.E.; Iannotti, J.P.; Williams, G.R. Anteroposterior instability of the distal clavicle after distal clavicle resection. Clin. Orthop. Relat. Res. 1998, 348, 114–120. [Google Scholar] [CrossRef]
- Tytherleigh-Strong, G.; Gill, J.; Sforza, G.; Copeland, S.; Levy, O. Reossification and fusion across the acromioclavicular joint after arthroscopic acromioplasty and distal clavicle resection. Arthroscopy 2001, 17, E36. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Group A n = 10 | Group B n = 10 | p-Values | |
|---|---|---|---|
| Age (years) | 60.4 ± 8.9 | 60.8 ± 9.2 | 0.923 |
| Gender (female/male) | 7:3 | 7:3 | 1.000 |
| Concomitant pathologies (yes/no) | 9:1 | 9:1 | 1.000 |
| Dominant arm involved (yes/no) | 6:4 | 4:6 | 0.656 |
| Scores | Group A n = 10 | Group B n = 10 | p-Values |
|---|---|---|---|
| Overall CS [points] | 64.1 ± 19.3 | 74.9 ± 14.4 | 0.175 |
| Pain | 6.3 ± 6.0 | 13.0 ± 2.6 | 0.007 * |
| ADL | 12.9 ± 5.7 | 17.0 ± 3.3 | 0.069 |
| ROM | 32.0 ± 6.0 | 34.6 ± 5.3 | 0.318 |
| Abduction | 8.4 ± 2.3 | 8.8 ± 2.5 | 0.714 |
| Flexion | 9.0 ± 1.7 | 9.0 ± 2.2 | 0.999 |
| Internal rotation | 5.0 ± 2.2 | 7.3 ± 1.0 | 0.012 * |
| External rotation | 9.6 ± 1.3 | 9.6 ± 0.8 | 0.999 |
| Strength | 12.9 ± 6.9 | 10.3 ± 5.8 | 0.372 |
| qDASH (points) | 44.1 ± 31.3 | 24.3 ± 27.5 | 0.150 |
| ASES (points) | 56.7 ± 32.7 | 75.0 ± 24.3 | 0.172 |
| SSV (%) | 65.5 ± 22.3 | 85.9 ± 16.4 | 0.031 * |
| SST (points) | 6.1 ± 3.6 | 7.9 ± 3.6 | 0.281 |
| VAS (points) | 4 (range 0–7) | 1 (range 0–4) | 0.123 |
| Constant Score (Points) | Group A Before Revision | Group A After Revision (latest FU) | p-Value |
|---|---|---|---|
| Pain | 5 (range, 0–15) | 5 (range, 0–15) | 0.478 |
| ADL | 7.5 (range, 4–20) | 10.5 (range, 6–20) | 0.284 |
| ROM | 24 (range, 16–38) | 34 (range, 20–38) | 0.185 |
| Strength | 8 (range, 4–26) | 13.5 (range, 1–22) | 0.575 |
| Overall CS | 51.4 ± 22.1 | 64.1 ± 19.3 | 0.316 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ostermann, R.C.; Eigenschink, M.; Heuberer, P.R.; Siegert, P.; Muellbacher, W.; Anderl, L.; Schrott, B.; Laky, B.; Pauzenberger, L.; Anderl, W. Bony Regrowth and New Spur Formation as Possible Causes of Failed Distal Clavicle Excision—Mid-Term Outcomes after Revision Surgery in a Matched-Pair Analysis. J. Pers. Med. 2023, 13, 1221. https://doi.org/10.3390/jpm13081221
Ostermann RC, Eigenschink M, Heuberer PR, Siegert P, Muellbacher W, Anderl L, Schrott B, Laky B, Pauzenberger L, Anderl W. Bony Regrowth and New Spur Formation as Possible Causes of Failed Distal Clavicle Excision—Mid-Term Outcomes after Revision Surgery in a Matched-Pair Analysis. Journal of Personalized Medicine. 2023; 13(8):1221. https://doi.org/10.3390/jpm13081221
Chicago/Turabian StyleOstermann, Roman C., Martin Eigenschink, Philipp R. Heuberer, Paul Siegert, Willi Muellbacher, Lisa Anderl, Beate Schrott, Brenda Laky, Leo Pauzenberger, and Werner Anderl. 2023. "Bony Regrowth and New Spur Formation as Possible Causes of Failed Distal Clavicle Excision—Mid-Term Outcomes after Revision Surgery in a Matched-Pair Analysis" Journal of Personalized Medicine 13, no. 8: 1221. https://doi.org/10.3390/jpm13081221
APA StyleOstermann, R. C., Eigenschink, M., Heuberer, P. R., Siegert, P., Muellbacher, W., Anderl, L., Schrott, B., Laky, B., Pauzenberger, L., & Anderl, W. (2023). Bony Regrowth and New Spur Formation as Possible Causes of Failed Distal Clavicle Excision—Mid-Term Outcomes after Revision Surgery in a Matched-Pair Analysis. Journal of Personalized Medicine, 13(8), 1221. https://doi.org/10.3390/jpm13081221