Abstract
(1) Background: Non-squamous cell laryngeal carcinoma includes endothelial tumors, such as minor salivary gland tumors, lymphoepithelial tumors, neuroendocrine tumors, soft and hard tissue sarcomas, and malignant melanomas. (2) Methods: A state-of-the-art review using the MEDLINE/PUBMED, Google Scholar, Ovid Medline, Embase, and Scopus electronic databases was performed. (3) Conclusions: In order to optimize overall treatment outcomes, a multidisciplinary, patient-centered approach to the management of non-SCC of the larynx must be adopted universally; a national or international registry on non-SCC laryngeal cancer can be useful to improve understanding about the behavior of this kind of tumor.
1. Introduction
Laryngeal carcinomas represent one third of all head and neck cancers [1], with an incidence rate of 5% [2] and an estimated account of 13,000 newly diagnosed cases each year in the USA [3]. Of these, it is estimated that 95% of all laryngeal cancers (LC) are squamous cell carcinomas (SCC) [4], while the remaining cases fall under a group defined as “non-squamous cell carcinoma” (non-SCC). Non-SCC LC includes endothelial tumors, such as minor salivary gland tumors, lymphoepithelial tumors, neuroendocrine tumors, soft and hard tissue sarcomas, and malignant melanomas [5].
Despite the increasing knowledge about the treatment of LC in the last decades, the lack of information about non-SCC LC makes it difficult to establish a proper patient profile, define outcomes, or improve patient counseling. Additionally, the literature is scarce regarding these types of tumors [4,5,6,7,8,9]. The current guidelines from the National Comprehensive Cancer Network make no direct recommendation for the treatment of non-SCC LC [10] but, depending on the disease’s extent and histology, a multidisciplinary approach (surgery, radiotherapy, or systemic therapy) can be recommended.
The objective of this review was to systematically evaluate the available literature and current knowledge about primary non-SCC LC, identify future research lines on this topic, and explore potential personalized approaches.
2. Materials and Methods
This state-of-the-art review involved the MEDLINE/PUBMED, Google Scholar, Ovid Medline, Embase, and Scopus electronic databases, with search terms: “non-squamous laryngeal cancer”, “non-squamous glottic cancer”, “non-squamous head and neck cancer”, “non-squamous laryngeal cancer treatment”, “laryngeal sarcoma”, “neuroendocrine laryngeal carcinoma”, “laryngeal salivary gland carcinoma”, “laryngeal lymphoma”, “laryngeal melanoma”, and “laryngeal spindle-cell carcinoma”. Clinical prospective and retrospective studies, experimental research, meta-analyses, and systematic reviews published on non-SCC LC until October 2022 were included in the study, while case reports, publications focusing on non-SCC in children, and grey literature were excluded. Articles were required to be written in English, Italian, French, or Spanish. Despite not being a systematic review, article selection was based on the recommendations of the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) criteria [11]. Titles and abstracts were screened by two investigators (C.M.C.E. and M.R.B.) to discard irrelevant or duplicate publications. Once the duplicates were refined and the articles selected, the authors reviewed the complete texts of all the manuscripts and the bibliographic references with the aim of including possible studies not found through the search strategy.
A critical analysis of the literature was then performed focusing on histology, incidence and prevalence, clinical presentation, diagnosis, and treatment. Ethics committee approval was not required for this review.
3. Discussion
Non-SCC of the larynx represents a unique diagnostic and therapeutic challenge for clinicians because these lesions are encountered infrequently. According to the available evidence, almost all benign and malignant laryngeal neoplasms are epithelial in origin, and all of them arise from the squamous epithelium which covers the larynx. Other non-SCC LC that are usually considered separately, despite their epithelial origin, correspond to spindle-cell carcinoma or salivary gland tumors (Table 1).

Table 1.
Histological non-squamous cell carcinomas of the larynx.
These neoplasms usually originate from the submucosal region and the fibrocartilaginous skeleton (cartilage, nerve trunks, minor salivary glands, blood, and lymphatic vessels) and they appear, objectively, as laryngeal swellings covered by normal mucosa. According to the existing literature, the majority of patients affected by non-SCC carcinomas were aged between 55 and 75 years; male subjects are considered at higher risk for non-SCCs compared to females (1.7:1 ratio) [12,13,14], except for lymphoepithelial carcinoma, which is more common in women [12]. In terms of incidence, the most prevalent laryngeal non-SCCs are neuroendocrine tumors (37%) [13,14,15].
3.1. Diagnostic Workup
As these tumors are rare, there are limited data regarding optimal treatment modality based on histologic type. Because survival and staging data are limited, there is currently no consensus on management principles for most of these neoplasms.
Clinical symptoms are similar in patients affected by SCCs and in those affected by non-SCC, and they are mainly represented by hoarseness followed by dyspnea/stridor and dysphagia. Tobacco smoking and alcohol abuse, contrary to SCC, do not seem to be considered predominant risk factors for non-SCCs [16,17].
The routine clinical approach includes visualization of the larynx with flexible laryngoscopy and subsequent biopsy (in-office procedure or through direct laryngoscopy) at directed sites of suspicion. SCC may be recognized during flexible laryngoscopy as evident mucosal abnormalities, whereas non-SCC laryngeal tumors usually show up as submucosal masses, limiting the possibilities of this diagnostic approach alone. So, especially in case of persistence/worsening of symptoms, a radiographic evaluation is mandatory to confirm the diagnosis [18].
The first choice usually corresponds to computed tomography (CT), because this provides a high anatomical resolution, allowing us to determine the exact location, vascularization, and extension of the lesion, as well as the involvement of the laryngeal skeleton [19]. The second choice usually correspond to magnetic resonance imaging (MRI), which may provide a more accurate and detailed description of laryngeal subsites, anterior commissure, submucosal infiltration into pre- and paraglottic spaces, cartilage, and base of tongue invasion, as well as metastasis to regional lymph nodes in the neck [20]. Histological examination usually needs to be supported by a comprehensive immunohistochemical examination.
3.2. Neuroendocrine Tumors
Neuroendocrine laryngeal malignancies (NLM) are uncommon and heterogeneous tumors, which share some specific morphological, histochemical, immunohistochemical, and ultrastructural characteristics but may present different prognosis on the basis of the tumor type [21]. According to a recent population-based analysis published by Torabi et al., NLM represent 37% of non-SCC of the larynx [12]. Moreover, patients affected by neuroendocrine tumors have been recognized as those with the highest rate of metastases, and with the lowest survival among all histological subtypes [21].
NLM are divided into two broad categories based on their tissue of origin: epithelial and neural. the most common subtypes usually correspond to typical carcinoid, atypical carcinoid, and small-cell undifferentiated carcinoma. In 2017, a new classification developed by the WHO modified the terminology and classification of laryngeal neuroendocrine carcinomas into well-, moderately, and poorly differentiated neuroendocrine carcinoma. Moreover, this classification emphasizes the relevance of poorly differentiated neuroendocrine carcinomas including the poorly differentiated neuroendocrine carcinomas of a small cell type (SCNEC) and a large cell type (LCNEC) [22].
The diagnosis of neuroendocrine neoplasm requires the presence of both neuroendocrine morphologies via light microscopy and the demonstration of neuroendocrine differentiation by means of immunohistochemistry or electron microscopy. NLM can appear as an infiltrative laryngeal mass on imaging, but the findings are nonspecific and can resemble those of SCC. Furthermore, there may be accompanying bulky metastatic cervical lymphadenopathy, typically without necrosis or cystic changes [23]. Primary SCNEC of the larynx may be associated with paraneoplastic syndromes, akin to small-cell cancer of the lung [24].
Regarding treatment options, due to the recent change in terminology, the literature available is scarce. However, based on previous data, carcinoid tumors (typical and atypical) are usually treated by surgery (partial or total laryngectomy) [25,26,27], while neck management can be different. In particular, in patients affected by typical carcinoid, neck dissection is not mandatory due to the low incidence of neck metastasis [14]; on the other hand, in the atypical carcinoid, elective or therapeutic neck dissection is necessary including at least levels IIa and III [14,28]. By contrast, the best option to achieve local control of SCNEC laryngeal tumors continues to be concurrent chemoradiation therapy [29].
As proposed in 1986 by Baugh et al., radiation alone does not improve survival, but it may increase local control. Adjuvant chemotherapy increases the median survival from 11 to 19 months [30], and the concomitant CRT treatment resulted in a median survival of 55 months. However, chemotherapy resistance has been described as an important indicator of poor prognosis [15].
Regarding SCNEC, we need to consider some key concepts. Firstly, the most common location affected in the H&N region is the larynx, representing at least 35% of patients [31]. Secondly, local control is often insufficient to prevent distant metastasis, and nearly 90% of these patients may develop distant recurrence that leads to death [15,29].
Another relevant factor that is important to keep in mind corresponds to the differential diagnosis among primary laryngeal neuroendocrine malignancies and laryngeal metastasis from a primary small-cell neuroendocrine carcinoma of the lung, where imaging studies of the lung want to be mandatory in order to obtain a more precise differential diagnosis [32]. Despite laryngeal neuroendocrine metastasis being extremely rare, two case reports have been described related to a prostate [33] and aggressive rectal carcinoid metastasizing to the larynx [34].
3.3. Spindle-Cell Carcinoma
Spindle-cell carcinoma (SPCC) is composed of spindle-cell elements. Histologically, the spindle-cell elements are derived from squamous epithelium but they follow a divergent mesenchymal differentiation, and usually can be misdiagnosed due to their histological appearance [35]. These tumors usually arise in the glottis, looking like a polypoid or a pedicled polyp mass [36,37]. Surgery is considered the first-line treatment, a 5-year OS rate range between 54 and 59% is reported [36,37]. The largest series to date [38] challenges the established view of SPCC as an aggressive variant of SCC. Although typically a higher grade at diagnosis, SPCC has less frequent nodal involvement than SCC; SPCC and SCC have similar incidence of distant metastasis; and SPCC is not associated with a higher hazard ratio of death, suggesting that SPCC histology is not an independent adverse prognostic factor, which should be considered when counseling patients with SPCC [38].
3.4. Minor Salivary Gland Tumors
Malignant salivary gland carcinoma (MSGC) of the larynx includes different etiologies like: adenosquamous carcinoma (ASC), mucoepidermoid carcinoma (MEC), adenoid cystic carcinoma (ACC), and adenocarcinoma. The etiology of these tumors remains unknown, and tumor distribution wants to be correlated with the anatomical distribution of submucosal minor salivary glands in the larynx, which are mainly located in the region of the false vocal cords, ventricles, and the anterior subglottic commissure [39].
These tumors tend to be indolent and spread submucosally as a mass with an intact overlying mucosal surface, which may result in delayed diagnosis. Moreover, there are some characteristics that are specific for each histological subtype.
ACC is the most common type of laryngeal MSGC, representing <1% of all tumors affecting the larynx [40]. Despite there not being a clear predominance by sex, these tumors are more common in the fifth decade of life and are not correlated with tobacco consumption. ACC patients are rarely affected by cervical lymph node metastasis and are characterized by multiple recurrences as late distant metastasis [41]. By contrast, ASC is more common in men aged 60–70 years, and has a high propensity for metastasis [41,42] (Figure 1).
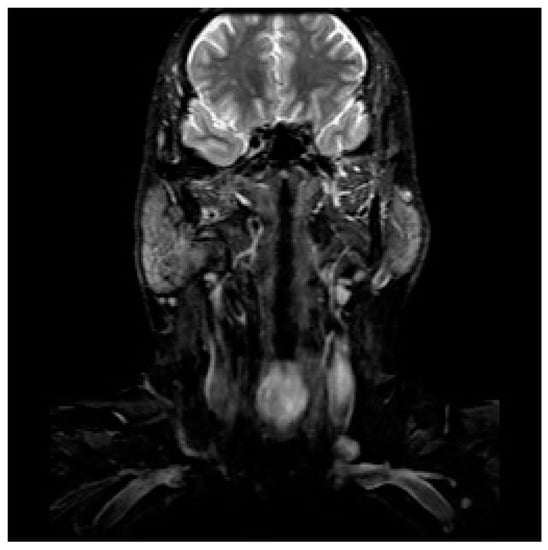
Figure 1.
MRI scan of a patients with a laryngeal adenoid cystic carcinoma.
Mucoepidermoid carcinoma (MEC) represents unusual histology in the larynx, predominantly affecting men aged 50–60 years [43]. It is thought that this tumor arises from the excretory ducts of seromucous glands and has a wide spectrum of clinical behavior from locally invasive to highly malignant [44], often corresponding to tumor grade and can be divided into high differentiation type and low differentiation type, according to the proportion of different cells in the tumor and the degree of differentiation [45]. Regarding tumor localization, 60% of tumors affect the supraglottic space, 30% the glottis, and 10% the subglottic or want to be a trans-glottic lesion [46,47]. Historically, patients affected by MEC were treated by means of total laryngectomy, while partial laryngectomy is considered suboptimal due to the submucosal spread of these lesions [47,48,49], with the exception of small, localized, and low-grade tumors [48]. Neck dissection is indicated in high-grade tumors and in patients with positive lymph nodes [50,51], and postoperative RT needs to be considered in patients affected by medium- and high-grade MEC, positive margins, and extracapsular spread. RT alone has been described in early-stage/low-grade cases [52]. However, MEC are considered moderately radiosensitive tumors, and for this reason, RT exclusively is not taken into consideration as a first option [53]. Five-year overall survival rates reported in the literature range from 0 to 45% in high-grade MEC, from 60 to 90% in intermediate-grade MEC, and from 90 to 100% in low-grade MEC [54].
Despite data concerning treatment options and outcomes are scarce, surgery is still considered the treatment of choice. The potential role of adjuvant RT has not been well defined yet, although there is an agreement that it should be considered complementary in advanced-stage or high-grade disease [40].
3.5. Soft Tissue Sarcomas
They represent less than 1% of all laryngeal tumors. A variety of uncommon sarcoma subtypes arising from the submucosal connective tissue have been described in the larynx, mainly as case reports or small series including synovial sarcoma [54,55,56], well-differentiated and dedifferentiated liposarcoma [57,58,59], alveolar soft part sarcoma [60], low-grade fibro-myxoid sarcoma [61], embryonal rhabdomyosarcoma [62,63,64,65,66], Kaposi sarcoma [67], and undifferentiated sarcoma [68,69,70] (Figure 2 and Figure 3).
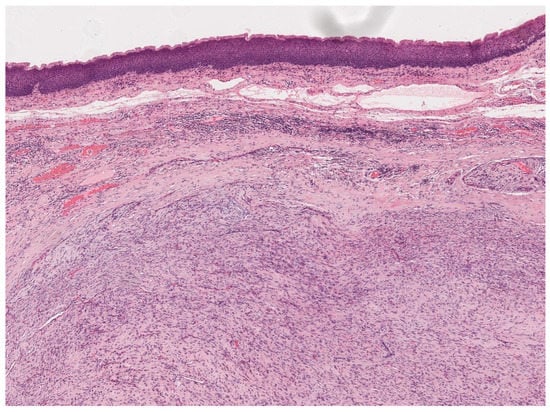
Figure 2.
Histological images (hematoxylin–eosin) of a patient with a laryngeal well-differentiated liposarcoma.

Figure 3.
CT scan of a patient with a laryngeal well-differentiated liposarcoma.
Synovial sarcoma represents an aggressive soft tissue tumor classically arising from mesenchymal tissue. Primary synovial sarcoma of the H&N is rare (<5% of all synovial sarcomas), and those originating from the larynx are even rarer [71]. The first case of laryngeal synovial sarcoma was described by Gatti and Miller in 1975 [72,73,74]. The diagnostic of this tumor represents a challenge, and the final diagnosis is made on the basis of tumor morphology (monophasic or biphasic according to the proportion of spindle and epithelial cells), immunohistochemistry, and molecular studies. Wide local resection is recommended as a treatment option with adjuvant RT, with or without CT, depending on final histological results [71].
Kaposi´s sarcoma is an extremely rare HIV-associated neoplasm. The largest series across the literature corresponds to Mochloulis et al., including 17 patients with laryngeal Kaposi’s sarcoma. In this series, the supraglottic location was the most common, and the main treatment strategy was conservative; more specifically, five patients were treated with low-dose radiotherapy and ten were treated with systemic chemotherapy for disseminated Kaposi’s sarcoma. According to the authors, laryngeal Kaposi’s sarcoma did not contribute to patient mortality [74]. More recently, treatment strategies using intralesional bevacizumab have also been reported as a possible treatment for localized mucosal lesions [75].
3.6. Bone/Cartilage Sarcomas
Demographically, these tumors usually affect patients between the sixth and seventh decades of life with a male predominance of 3–4:1 [76,77]. Chondrosarcoma is the most common sarcoma subtype [78], and the cricoid cartilage (70–75%), followed by the thyroid cartilage (20%), are the most commonly affected laryngeal subsites [54]. The majority of them are low-grade tumors with uncommon local or distant spread. Nowadays, surgery is considered the treatment of choice and, according to the disease extension, cricoarytenoid joints mobility, and histological grade, the surgical approach can range from an endoscopic approach to an open partial or total laryngectomy [54]. In one of the largest case series published by Thompson et al. including 111 laryngeal chondrosarcomas, 73 patients were treated with a partial laryngectomy while the remaining patients underwent TL; recurrence was reported in 20 patients (18% of the sample), 10 of whom underwent salvage TL [76].
Osteosarcoma of the larynx represents an extremely rare and highly malignant neoplasm [78,79], with a tendency to hematogenous dissemination and early metastasizes. Histologically, it also represents a challenge for the most experienced pathologist due to its similarities to other sarcomas. The definitive diagnosis of osteosarcoma depends on the identification of osteoid production by malignant cells in the biopsy sample. Wide local resection (TL) with clear margins remains the treatment of choice for laryngeal osteosarcoma due to the need to achieve local control and improve long-term survival [80].
Radiological evaluation can provide more information; in the case of SCC or sarcomatoid carcinoma, there is an association with the mucosal surface, whereas true sarcomas are usually centered within the soft tissue or cartilaginous structures [76]. Other radiological considerations can be the presence of calcification associated with osteoid or cartilage matrix or the presence of fat [76].
During the histological evaluation, immunostaining is crucial, and looking for cytokeratin, p63 and/or p40 could be helpful [81], as sarcomatoid carcinoma, the most common differential diagnosis, may lose expression of these markers [81].
3.7. Lymphoepithelial Carcinoma
Lymphoepithelial carcinoma (LC) usually arises in the lymphoid tissue of the pharynx within the Waldeyer´s ring. The presence of LC in the larynx is extremely rare. It has been hypothesized that the benign lymphoid component is geographical to the site rather than a reactive lymphocytic influx responding to a carcinoma [79]. This would explain the unusual presentation of such tumors in locations like the trachea or the larynx, which lack consistent organized lymphoid tissue.
According to the evidence available, this tumor more commonly affects male patients between 40 and 82 years. Smoke or alcohol intake has not been related with the occurrence of this kind of tumors [82,83]. The correlation between this tumor and the Epstein Barr Virus (EBV) infection is still controversial [83,84,85,86,87]. The majority differential diagnosis of lymphoepitheliomas includes non-Hodgkin’s lymphoma, rhabdomyosarcoma, and squamous cell carcinoma [82].
3.8. Malignant Melanoma
Regarding malignant melanoma of the larynx (MML), it is necessary to differentiate a primary mucosal malignant melanoma from a metastasis of a cutaneous malignant melanoma. In the first case, primary MML of the H&N is an uncommon disease. This entity probably derives from scattered melanocytes in the upper aero-digestive tract mucosa, which may be included within the basal layer of the epithelium of the nasal cavity, oral cavity, oropharynx, and esophagus. However, melanocytes are rarely detected within the larynx, and this could explain the low incidence of primary melanoma in the larynx [88,89,90]. By contrast, at least 0.6% of patients affected by cutaneous melanoma suffer from a metastasize to the mucosa of the upper aerodigestive tract, and of those metastatic sites, 12% are laryngeal [91].
The differential diagnosis of primary laryngeal melanoma usually includes SCC, NET, non-Hodgkin’s malignant lymphoma, extramedullary plasmacytoma, paraganglioma, and sarcomas (malignant fibrous histiocytoma, fibrosarcoma, and malignant Schwannoma) [92]. Usually, the primary treatment for MML is radical surgery with or without adjuvant radiotherapy or chemotherapy. However, endoscopic resection has been described [54]. Although radical surgery represents the best option for local control, local recurrence occurs frequently [91]. Given the small proportion of cases, optimal management is not well established, and despite controversies, it could be useful to excise isolated recurrence and metastasis, particularly if they cause airway symptoms [93].
3.9. Primary Lymphoma of the Larynx
Lymphoproliferative diseases like extramedullary plasmacytoma or non-Hodgkin’s lymphoma (NHL) can affect the larynx. NHL usually arises in the supraglottic and subglottic structures where laryngeal lymphoid tissues predominate [94]. These tumors are usually macroscopically smooth or polypoid [95,96,97]. The majority of reported primary lymphomas of the larynx are NHL with a B cell phenotype [98].
MALT lymphoma needs to be considered in the differential diagnosis of a patient with this presentation [99]. In the past, the standard treatment for primary lymphoproliferative tumors of the larynx was RT [99,100]. However, in the recent years, given the increasing evidence of the efficacy of systemic therapies and immunologic targeting antibodies, the tendency is moving forward in this direction.
3.10. Perspectives in Non-Squamous Cell Carcinomas
Regarding treatment, as we detailed above, laryngeal non-SCCs represent a significant challenge to clinicians because no definitive guideline exists. However, recent studies like the published by Landelli et al. shed some light. In this study, the authors found a significant difference among the various laryngeal subsites involved by SCC and non-SCC. The supraglottic and subglottic regions are strongly associated with non-SCC compared to SCC [17]. Furthermore, the authors did not find differences regarding overall survival or disease-specific survival between SCC and non-SCC [17]. By contrast, Chen et al. found a significant difference in OS between non-SCC and SCC with longer OS in the latter, maybe due to the differences in the proportion of cases included by etiology with more neuroendocrine carcinomas [39]. The heterogeneity in the indexed literature makes it mandatory to improve data collection in order to generate enough evidence for guidelines development.
4. Conclusions
To optimize overall treatment outcomes, a multidisciplinary, patient-centered approach to the management of non-SCC of the larynx must be adopted universally. National or international registry on non-SCC laryngeal cancer can be useful to improve understanding about the behavior of these kind of tumors.
Author Contributions
Conceptualization, C.M.C.-E. and J.R.L.; methodology, M.R.B. and M.M.-Y.; formal analysis, A.M.; investigation, N.F. and G.C.; writing—original draft preparation, C.M.C.-E.; writing—review and editing, M.R.B. and T.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
New data were not generated in this review.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Koroulakis, A.; Agarwal, M. Laryngeal Cancer. In StatPearls [Internet]; [Updated 10 August 2020]; StatPearls Publishing: Treasure Island, FL, USA, 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK526076/ (accessed on 12 December 2022).
- American Cancer Society. Cancer Facts & Figures 2017; American Cancer Society: Atlanta, GA, USA, 2017; Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-andfigures/2017/cancer-facts-and-figures-2017.pdf (accessed on 13 December 2020).
- American Cancer Society. Cancer Facts & Figures 2018; American Cancer Society: Atlanta, GA, USA, 2018; Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statis-tics/annual-cancer-factsandfigures/2018/cancer-facts-and-figures-2018.pdf (accessed on 13 December 2020).
- Shah, J.P.; Karnell, L.H.; Hoffman, H.T.; Ariyan, S.; Brown, G.S.; Fee, W.E.; Glass, A.G.; Goepfert, H.; Ossoff, R.H.; Fremgen, A. Patterns of care for cancer of the larynx in the United States. Arch. Otolaryngol. Head Neck Surg. 1997, 123, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Tan, E.; Mody, M.D.; Saba, N.F. Systemic therapy in non-conventional cancers of the larynx. Oral Oncol. 2018, 82, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Marioni, G.; Marchese-Ragona, R.; Cartei, G.; Marchese, F.; Staffieri, A. Current opinion in diagnosis and treatment of laryngeal carcinoma. Cancer Treat. Rev. 2006, 32, 504–515. [Google Scholar] [CrossRef]
- Hoffman, H.T.; Porter, K.; Karnell, L.H.; Cooper, J.S.; Weber, R.S.; Langer, C.J.; Ang, K.-K.; Gay, G.; Stewart, A.; Robinson, R.A.; et al. Laryngeal Cancer in the United States: Changes in Demographics, Patterns of Care, and Survival. Laryngoscope 2006, 116, 1–13. [Google Scholar] [CrossRef]
- Karatzanis, A.D.; Psychogios, G.; Waldfahrer, F.; Kapsreiter, M.; Zenk, J.; Velegrakis, G.A.; Iro, H. Management of locally advanced laryngeal cancer. J. Otolaryngol.-Head Neck Surg. 2014, 43, 4. [Google Scholar] [CrossRef]
- Cheraghlou, S.; Kuo, P.; Judson, B.L. Treatment delay and facility case volume are associated with survival in early-stage glottic cancer. Laryngoscope 2017, 127, 616–622. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Head and Neck Cancers (Version 2.2018). Available online: http://oncolife.com.ua/doc/nccn/Head_and_Neck_Cancers.pdf (accessed on 10 December 2020).
- Moher, D.; Liberati, M.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Torabi, S.J.; Cheraghlou, S.; Kasle, D.A.; Savoca, E.L.; Judson, B.L. Nonsquamous cell laryngeal cancers: Incidence, demographics, care patterns, and effect of surgery. Laryngoscope 2019, 129, 2496–2505. [Google Scholar] [CrossRef]
- Lin, H.W.; Bhattacharyya, N. Staging and Survival Analysis for Nonsquamous Cell Carcinomas of the Larynx. Laryngoscope 2008, 118, 1003–1013. [Google Scholar] [CrossRef]
- Ferlito, A.; Barnes, L.; Rinaldo, A.; Gnepp, D.R.; Milroy, C.M. A review of neuroendocrine neoplasms of the larynx: Update on diagnosis and treatment. J. Laryngol. Otol. 1998, 112, 827–834. [Google Scholar] [CrossRef]
- Ferlito, A.; Silver, C.E.; Bradford, C.R.; Rinaldo, A. Neuroendocrine neoplasms of the larynx: An overview. Head Neck 2009, 31, 1634–1646. [Google Scholar] [CrossRef] [PubMed]
- Fan, L.; Zhao, R.; Chen, X.; Liu, Y.; Tian, L.; Liu, M. Establishment of a non-squamous cell carcinoma of the larynx nomogram prognostic model and prognosis analysis. Auris Nasus Larynx 2022, 49, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Iandelli, A.; Missale, F.; Laborai, A.; Filauro, M.; Marchi, F.; Del Bon, F.; Perotti, P.; Parrinello, G.; Piazza, C.; Peretti, G. Surgical management and oncological outcome of non squamous cell carcinoma of the larynx: A bicentric study. Eur. Arch. Oto-Rhino-Laryngol. 2022, 279, 299–310. [Google Scholar] [CrossRef]
- Rotsides, J.M.; Patel, E.; Oliver, J.R.; Moses, L.E.; Jacobson, A.S.; Hu, K.S.; Vaezi, A.; Tam, M.; Givi, B. Non-Squamous Cell Malignancies of the Larynx. Laryngoscope 2022, 132, 1771–1777. [Google Scholar] [CrossRef] [PubMed]
- Doğan, S.; Vural, A.; Kahriman, G.; İmamoğlu, H.; Abdülrezzak, U.; Öztürk, M. Non-squamous cell carcinoma diseases of the larynx: Clinical and imaging findings. Braz. J. Otorhinolaryngol. 2020, 86, 468–482. [Google Scholar] [CrossRef]
- Banko, B.; Đukić, V.; Milovanovic, J.; Kovač, J.; Artiko, V.; Maksimović, R. Diagnostic significance of magnetic resonance imaging in preoperative evaluation of patients with laryngeal tumors. Eur. Arch. Oto-Rhino-Laryngol. 2011, 268, 1617–1623. [Google Scholar] [CrossRef]
- Torabi, S.; Benchetrit, L.; Spock, T.; Judson, B. Clinically node-negative head and neck mucosal melanoma: An analysis of current treatment guidelines & outcomes. Oral Oncol. 2019, 92, 67–76. [Google Scholar] [CrossRef]
- Strojan, P.; Hernandez-Prera, J.C.; Beitler, J.J.; Eisbruch, A.; Saba, N.F.; Mendenhall, W.M.; Nieto, C.S.; Smee, R.; Rinaldo, A.; Ferlito, A. Small cell and large cell neuroendocrine carcinoma of the larynx: A comparative analysis. Cancer Treat. Rev. 2019, 78, 42–51. [Google Scholar] [CrossRef]
- Oren, N.; Vaysberg, A.; Ginat, D.T. Updated WHO nomenclature of head and neck lesions and associated imaging findings. Insights Imaging 2019, 10, 72. [Google Scholar] [CrossRef]
- Ferlito, A.; Rinaldo, A. Primary and secondary small cell neuroendocrine carcinoma of the larynx: A review. Head Neck 2008, 30, 518–524. [Google Scholar] [CrossRef]
- Moisa, I.; Silver, C. Treatment of Neuroendocrine Neoplasms of the Larynx. ORL 1991, 53, 259–264. [Google Scholar] [CrossRef]
- Bapat, U.; MacKinnon, N.A.; Spencer, M.G. Carcinoid tumours of the larynx. Eur. Arch. Oto-Rhino-Laryngol. 2005, 262, 194–197. [Google Scholar] [CrossRef]
- Ferlito, A.; Devaney, K.O.; Rinaldo, A. Neuroendocrine neoplasms of the larynx: Advances in identification, understanding, and management. Oral Oncol. 2006, 42, 770–788. [Google Scholar] [CrossRef]
- Goldman, N.C.; Katibah, G.M.; Medina, J. Carcinoid tumors of the larynx. ORL 1985, 64, 130–134. [Google Scholar]
- Gnepp, D. Small Cell Neuroendocrine Carcinoma of the Larynx. A critical review of the literature. ORL 1991, 53, 210–219. [Google Scholar] [CrossRef]
- Baugh, R.F.; Wolf, G.T.; Krause, C.J.; Beals, T.F.; Forastiere, A. Small Cell Carcinoma of the Larynx: Results of Therapy. Laryngoscope 1986, 96, 1283–1290. [Google Scholar] [CrossRef]
- Pointer, K.B.; Ko, H.C.; Brower, J.V.; Witek, M.E.; Kimple, R.J.; Lloyd, R.V.; Harari, P.M.; Baschnagel, A.M. Small cell carcinoma of the head and neck: An analysis of the National Cancer Database. Oral Oncol. 2017, 69, 92–98. [Google Scholar] [CrossRef]
- Barnes, L. Neuroendocrine tumours. In Pathology and Genetics Head and Neck Tumours. World Health Organization Classification of Tumours; Barnes, L., Eveson, J.W., Reichart, P., Sidransky, D., Eds.; IARC Press: Lyon, France, 2005; pp. 135–139. [Google Scholar]
- Grignon, D.J.; Ro, J.Y.; Ayala, A.G.; Chong, C. Carcinoma of prostate metastasizingto vocal cord. Urology 1990, 36, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Danikas, D.; Theodorou, S.J.; Matthews, W.E.; Rienzo, A.A. Unusually Aggressive Rectal Carcinoid Metastasizing to Larynx, Pancreas, Adrenal Glands, and Brain. Am. Surg. 2000, 66, 1179–1180. [Google Scholar] [CrossRef]
- López, F.; Williams, M.D.; Cardesa, A.; Hunt, J.L.; Strojan, P.; Rinaldo, A.; Nixon, I.J.; Rodrigo, J.P.; Saba, N.F.; Mendenhall, W.M.; et al. How phenotype guides management of non-conventional squamous cell carcinomas of the larynx? Eur. Arch. Oto-Rhino-Laryngol. 2017, 274, 2709–2726. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.; Purgina, B.; Seethala, R.R. Spindle Cell Carcinoma of the Larynx with Rhabdomyoblastic Heterologous Element: A Rare Form of Divergent Differentiation. Head Neck Pathol. 2013, 7, 263–267. [Google Scholar] [CrossRef]
- Thompson, L.D.; Wieneke, J.A.; Miettinen, M.; Heffner, D.K. Spindle cell (sarcomatoid) carcinomas of the larynx: A clinicopathologic study of 187 cases. Am. J. Surg. Pathol. 2002, 26, 153–170. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.M.; Choudhry, H.S.; Desai, A.D.; Shah, V.P.; Patel, P.; Eloy, J.A.; Roden, D.F.; Fang, C.H. Prognostic significance of head and neck spindle cell carcinoma. Head Neck 2022. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Deng, W.; Li, C.; Lau, H.; Tao, L.; Wang, S.; Zhou, L.; Zhang, M. Clinical outcome and comparison between squamous and non-squamous cell carcinoma of the larynx. Acta Otolaryngol. 2020, 140, 195–201. [Google Scholar] [CrossRef]
- López, F.; Williams, M.D.; Skálová, A.; Hellquist, H.; Suárez, C.; Nixon, I.J.; Rodrigo, J.P.; Cardesa, A.; Strojan, P.; Quer, M.; et al. How Phenotype Guides Management of the Most Common Malignant Salivary Neoplasms of the Larynx? Adv. Ther. 2017, 34, 813–825. [Google Scholar] [CrossRef]
- Ereno, C.; I Lopez, J.; Bilbao, F.J. The biphasic pattern of laryngeal and hypopharyngeal adenosquamous carcinoma is retained in lymph node metastases. Histopathology 2005, 46, 715–716. [Google Scholar] [CrossRef] [PubMed]
- Keelawat, S.; Liu, C.Z.; Roehm, P.C.; Barnes, L. Adenosquamous carcinoma of the upper aerodigestive tract: A clinicopathologic study of 12 cases and review of the literature. Am. J. Otolaryngol. 2002, 23, 160–168. [Google Scholar] [CrossRef]
- Cumberworth, V.L.; Narula, A.; MacLennan, K.A.; Bradley, P.J. Mucoepidermoid carcinoma of the larynx. J. Laryngol. Otol. 1989, 103, 420–423. [Google Scholar] [CrossRef]
- Nance, M.A.; Seethala, R.R.; Wang, Y.; Chiosea, S.I.; Myers, E.N.; Johnson, J.T.; Lai, S.Y. Treatment and survival outcomes based on histologic grading in patients with head and neck mucoepidermoid. Cancer 2008, 113, 2082–2089. [Google Scholar] [CrossRef]
- Trosman, S.; Chute, D.; Wood, B.; Lamarre, E. Unknown primary mucoepidermoid carcinoma: Diagnosis and treatment. Head Neck 2015, 37, E22–E25. [Google Scholar] [CrossRef]
- Gomes, V.; Costarelli, L.; Cimino, G.; Magaldi, L.; Bisceglia, M. Mucoepidermoid carcinoma of the larynx. Eur. Arch. Otorhinolaryngol. 1990, 248, 31–34. [Google Scholar] [CrossRef]
- Ferlito, A.; Recher, G.; Bottin, R. Mucoepidermoid Carcinoma of the Larynx. A clinicopathological study of 11 cases with review of the literature. ORL 1981, 43, 280–299. [Google Scholar] [CrossRef]
- Alavi, S.; Calcaterra, T.C.; Namazie, A.; Blackwell, K.E. Glandular Carcinoma of the Larynx: The Ucla Experience. Ann. Otol. Rhinol. Laryngol. 1999, 108, 485–489. [Google Scholar] [CrossRef] [PubMed]
- Luna-Ortiz, K.; Cano-Valdez, A.M.; Chacón, A.P.; Gómez, A.H. Horizontal partial laryngectomy in mucoepidermoid carcinoma of the larynx after failure of laser surgery followed by radiotherapy: A case report. Cases J. 2009, 2, 8421. [Google Scholar] [CrossRef]
- Ferlito, A.; Rinaldo, A.; Devaney, K.O.; Carbone, A. Management of the clinically negative cervical lymph nodes in patients with non-conventional squamous carcinoma of the larynx. J. Laryngol. Arch Otorhinolaryngol. 1999, 113, 619–623. [Google Scholar] [CrossRef]
- Walvekar, R.R.; Filho, P.A.A.; Seethala, R.R.; Gooding, W.E.; Heron, D.E.; Johnson, J.T.; Ferris, R.L. Clinicopathologic features as stronger prognostic factors than histology or grade in risk stratification of primary parotid malignancies. Head Neck 2011, 33, 225–231. [Google Scholar] [CrossRef]
- Rapidis, A.D.; Givalos, N.; Gakiopoulou, H.; Stavrianos, S.D.; Faratzis, G.; Lagogiannis, G.A.; Katsilieris, I.; Patsouris, E. Mucoepidermoid carcinoma of the salivary glands.: Review of the literature and clinicopathological analysis of 18 patients. Oral Oncol. 2007, 43, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Pires, F.R.; de Almeida, O.P.; de Araújo, V.C.; Kowalski, L.P. Prognostic Factors in Head and Neck Mucoepidermoid Carcinoma. Arch. Otolaryngol. Head Neck Surg. 2004, 130, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Karatayli-Ozgursoy, S.; Bishop, J.; Hillel, A.; Akst, L.; Best, S. Non-epithelial tumors of the larynx: A single institution review. Am. J. Otolaryngol. 2016, 37, 279–285. [Google Scholar] [CrossRef]
- Fernández-Aceñero, M.J.; Larach, F.; Ortega-Fernández, C. Non-epithelial lesions of the larynx: Review of the 10-year experience in a tertiary Spanish hospital. Acta Oto-Laryngol. 2009, 129, 108–112. [Google Scholar] [CrossRef]
- Friedman, A.D.; A Burns, J.; Lutch, M.J.; Zeitels, S.M. Submucosal neoplasms of the laryngeal introitus. J. Laryngol. Otol. 2012, 126, 706–713. [Google Scholar] [CrossRef] [PubMed]
- Wenig, B.M.; Weiss, S.W.; Gnepp, D.R. Laryngeal and Hypopharyngeal Liposarcoma a Clinicopathologic Study of 10 Cases with a Comparison to Soft-Tissue Counterparts. Am. J. Surg. Pathol. 1990, 14, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Makeieff, M.; Pelliccia, P.; Poizat, F.; Arnaud, S.; Rat, F.; Cupissol, D.; Guerrier, B.; Costes, V. Laryngeal dedifferentiated liposarcoma. Eur. Arch. Otorhinolaryngol. 2010, 267, 991–994. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Sun, J.; Wei, S.; Wang, D.; Brandwein, M. Well-Differentiated Laryngeal/Hypopharyngeal Liposarcoma in the MDM2 Era Report of Three Cases and Literature Review. Head Neck Pathol. 2017, 11, 146–151. [Google Scholar] [CrossRef]
- Tamaki, A.; Wasman, J.; Weidenbecher, M. Laryngeal alveolar soft part sarcoma: A case report of a rare malignancy in an atypical location. Am. J. Otolaryngol. 2017, 38, 260–262. [Google Scholar] [CrossRef]
- Cowan, M.L.; Thompson, L.; Leon, M.E.; Bishop, J.A. Low-Grade Fibromyxoid Sarcoma of the Head and Neck: A Clinicopathologic Series and Review of the Literature. Head Neck Pathol. 2016, 10, 161–166. [Google Scholar] [CrossRef]
- Dikbas, O.; Altundag, K.; Abali, H.; Turker, A.; Engin, H.; Sungur, A.; Baltali, E. Embryonal Rhabdomyosarcoma of the Larynx. Otolaryngol. Head Neck Surg. 2005, 133, 160–162. [Google Scholar] [CrossRef]
- Jain, A.; Singh, S.N.; Singhal, P.; Sharma, M.P. A rare case of subglottic embryonal rhabdomyosarcoma: Managed with the aim of organ preservation. J. Laryngol. Otol. 2015, 129, 106–109. [Google Scholar] [CrossRef] [PubMed]
- Kukwa, W.; Wojtowicz, P.; Jagielska, B.; Sobczyk, G.; Kukwa, A.; Czarnecka, A.M. Laryngeal embryonal rhabdomyosarcoma in an adult—A case presentation in the eyes of geneticists and clinicians. BMC Cancer 2011, 11, 166. [Google Scholar] [CrossRef]
- Russell, J.O.; Revenaugh, P.C.; Budd, G.T.; Greskovich, J.; Scharpf, J. Failed organ preservation strategy for adult laryngeal embryonal rhabdomyosarcoma. Am. J. Otolaryngol. 2015, 36, 277–279. [Google Scholar] [CrossRef]
- Sivanandan, R.; Kong, C.S.; Kaplan, M.J.; Fee, W.E.; Thu-Le, Q.; Goffinet, D.R. Laryngeal Embryonal Rhabdomyosarcoma: A case of cervical metastases 13 years after treatment and a 25-year review of existing literature. Arch. Otolaryngol. Head Neck Surg. 2004, 130, 1217–1222. [Google Scholar] [CrossRef]
- Pantanowitz, L.; Dezube, B.J. Kaposi sarcoma in unusual locations. BMC Cancer 2008, 8, 190. [Google Scholar] [CrossRef] [PubMed]
- Jeong, C.Y.; Kim, C.S. Undifferentiated pleomorphic sarcoma of the vocal fold. Ear Nose Throat J. 2016, 95, E12–E14. [Google Scholar] [PubMed]
- Kim, J.P.; Kim, J.Y.; Ko, G.H.; Woo, S.H. A rare case of malignant fibrous histiocytoma (pleomorphic undifferentiated sarcoma NOS) of the vocal fold. Ear Nose Throat J. 2015, 94, 270–272. [Google Scholar] [CrossRef] [PubMed]
- Cambruzzi, E.; Cruz, R.P.; Gava, V.G.; Pêgas, K.L. Undifferentiated high-grade pleomorphic sarcoma of the larynx treated with partial laringectomy. Braz. J. Otorhinolaryngol. 2016, 86, 14–16. [Google Scholar] [CrossRef]
- Shein, G.; Sandhu, G.; Potter, A.; Loo, C.; Jacobson, I.; Anazodo, A. Laryngeal Synovial Sarcoma: A Systematic Review of the Last 40 Years of Reported Cases. Ear Nose Throat J. 2021, 100, NP93–NP104. [Google Scholar] [CrossRef]
- Gatti, W.M.; Strom, C.G.; Orfei, E. Synovial sarcoma of laryngopharynx. Arch. Otolaryngol. Head Neck Surg. 1975, 101, 633–636. [Google Scholar] [CrossRef]
- Miller, L.H.; Santaella Latimer, L.; Miller, T. Synovial sarcoma of the larynx. Trans. Sect. Ophthalmol. Am. Acad. Ophthalmol. Otolaryngol. 1975, 80, 448–451. [Google Scholar]
- Mochloulis, G.; Irving, R.M.; Grant, H.R.; Miller, R.F. Laryngeal Kaposi’s sarcoma in patients with AIDS. J. Laryngol. Otol. 1996, 110, 1034–1037. [Google Scholar] [CrossRef]
- Ablanedo-Terrazas, Y.; La Barrera, C.A.-D.; Ormsby, C.E.; Ruiz-Cruz, M.; Reyes-Terán, G. Intralesional bevacizumab in patients with Human immunodeficiency virus-associated Kaposi’s sarcoma in the upper airway. Laryngoscope 2015, 125, E132–E137. [Google Scholar] [CrossRef]
- Thompson, L.D.R.; Gannon, F.H. Chondrosarcoma of the Larynx: A clinicopathologic study of 111 cases with a review of the literature. Am. J. Surg. Pathol. 2002, 26, 836–851. [Google Scholar] [CrossRef]
- Tiwari, R.; Mahieu, H.; Snow, G. Long-term results of organ preservation in chondrosarcoma of the cricoid. Eur. Arch. Oto-Rhino-Laryngol. 1999, 256, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Mosalleum, E.; Afrogheh, A.; Stofberg, S.; Bezuidenhout, A.F.; Schneider, J.; Hille, J. A Review of Primary Osteosarcoma of the Larynx and Case Report. Head Neck Pathol. 2015, 9, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Madrigal, F.M.; Godoy, L.M.R.; Daboin, K.P.; Casiraghi, O.; Garcia, A.M.; Luna, M.A. Laryngeal osteosarcoma: A clinicopathologic analysis of four cases and comparison with a carcinosarcoma. Ann. Diagn. Pathol. 2002, 6, 1–9. [Google Scholar] [CrossRef]
- Mäkitie, A.A.; Devaney, K.O.; Baujat, B.; Almangush, A.; Ferlito, A. Characteristics of Laryngeal Osteosarcoma: A Critical Review. Oncol. Ther. 2020, 8, 33–44. [Google Scholar] [CrossRef]
- Miettinen, M. Keratin subsets in spindle cell sarcomas. Keratins are widespread but synovial sarcoma contains a distinctive keratin polypeptide pattern and desmoplakins. Am. J. Pathol. 1991, 138, 505–513. [Google Scholar] [PubMed]
- Dray, T.; Vargas, H.; Weidnerg, N.; Sofferman, R.A. Lymphoepitheliomas of the laryngohypopharynx. Am. J. Otolaryngol. 1998, 19, 263–266. [Google Scholar] [CrossRef]
- Macmillan, C.; Kapadia, S.B.; Finkelstein, S.D.; Nalesnik, M.A.; Barnes, L. Lymphoepithelial carcinoma of the larynx and hypopharynx: Study of eight cases with relationship to Epstein-Barr virus and p53 gene alterations, and review of the literature. Hum. Pathol. 1996, 27, 1172–1179. [Google Scholar] [CrossRef]
- Weiss, L.M.; Movahed, L.A.; Butler, A.E.; Swanson, S.A.; Frierson, H.F.; Cooper, P.H.; Colby, T.V.; Mills, S.E. Analysis of Lymphoepithelioma and Lymphoepithelioma-like Carcinomas for Epstein-Barr Viral Genomes by in situ Hybridization. Am. J. Surg. Pathol. 1989, 13, 625–631. [Google Scholar] [CrossRef]
- Frank, D.K.; Cheron, F.; DiCostanzo, D.; Cho, H.; Sclafani, A. Nonnasopharyngeal Lymphoepitheliomas (Undifferentiated Carcinomas) of the Upper Aerodigestive Tract. Ann. Otol. Rhinol. Laryngol. 1995, 104, 305–310. [Google Scholar] [CrossRef]
- Andryk, J.; Freije, J.E.; Schultz, C.J.; Campbell, B.H.; Komorowski, R.A. Lymphoepithelioma of the larynx. Am. J. Otolaryngol. 1996, 17, 61–63. [Google Scholar] [CrossRef] [PubMed]
- Vargas, M.P.; Vargas, H.I.; Kleiner, D.E.; Merino, M.J. The role of prognostic markers (MiB-1, RB, and bcl-2) in the diagnosis bf parathyroid tumors. Mod. Pathol. 1997, 10, 12–17. [Google Scholar]
- Busuttil, A. Dendritic Pigmented Cells Within Human Laryngeal Mucosa. Arch. Otolaryngol. Neck Surg. 1976, 102, 43–44. [Google Scholar] [CrossRef] [PubMed]
- Reuter, V.E.; Woodruff, J.M. Melanoma of the larynx. Laryngoscope 1986, 94, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Goldman, J.L.; Lawson, W.; Zak, F.G.; Roffman, J.D. The presence of melanocytes in the human larynx. Laryngoscope 1972, 82, 824–835. [Google Scholar] [CrossRef] [PubMed]
- Henderson, L.T.; Robbins, K.T.; Weitzner, S. Upper Aerodigestive Tract Metastases in Disseminated Malignant Melanoma. Arch. Otolaryngol. Head Neck Surg. 1986, 112, 659–663. [Google Scholar] [CrossRef]
- Wenig, B.M. Laryngeal mucosal malignant melanoma. A clinicopathologic, immunohistochemical, and ultrastructural study of four patients and review of the literature. Cancer 1995, 75, 1568–1577. [Google Scholar] [CrossRef]
- Mifsud, M.; Padhya, T.A. Metastatic melanoma to the upper aerodigestive tract: A systematic review of the literature. Laryngoscope 2014, 124, 1143–1149. [Google Scholar] [CrossRef]
- Browne, J.D. Management of nonepidermoid cancer of the larynx. Otolaryngol. Clin. N. Am. 2002, 30, 215–229. [Google Scholar] [CrossRef]
- Ferlito, A.; Rinaldo, A.; Devaney, K.O.; Devaney, S.L.; Milroy, C.M. Impact of phenotype on treatment and prognosis of laryngeal malignancies. J. Laryngol. Otol. 2002, 112, 710–714. [Google Scholar] [CrossRef]
- Cavalot, A.L.; Preti, G.; Vione, N.; Nazionale, G.; Palonta, F.; Fadda, G.L. Isolated primary non-Hodgkin’s malignant lymphoma of the larynx. J. Laryngol. Otol. 2001, 115, 324–326. [Google Scholar] [CrossRef]
- Horny, H.-P.; Ferlito, A.; Carbone, A. Laryngeal Lymphoma Derived from Mucosa-Associated Lymphoid Tissue. Ann. Otol. Rhinol. Laryngol. 1996, 105, 577–583. [Google Scholar] [CrossRef]
- Nayak, J.V.; Cook, J.R.; Molina, J.T.; Branch, M.P.; Iv, B.F.B.; Ferris, R.L.; Myers, E.N. Primary Lymphoma of the Larynx: New Diagnostic and Therapeutic Approaches. ORL 2003, 65, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Zinzani, P.L.; Magagnoli, M.; Galieni, P.; Martelli, M.; Poletti, V.; Zaja, F.; Molica, S.; Zaccaria, A.; Cantonetti, A.M.; Gentilini, P.; et al. Nongastrointestinal Low-Grade Mucosa-Associated Lymphoid Tissue Lymphoma: Analysis of 75 Patients. J. Clin. Oncol. 1999, 17, 1254. [Google Scholar] [CrossRef] [PubMed]
- De Bree, R.; Mahieu, H.F.; Ossenkoppele, G.J.; Van Der Valk, P. Malignant lymphoma of mucosa-associated lymphoid tissue in the larynx. Eur. Arch. Oto-Rhino-Laryngol. 1998, 255, 368–370. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).