

Airway Management of Orofacial Infections Originating in the Mandible

Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Screening
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Demographic Distribution
3.2. Etiology and Localization of Infection
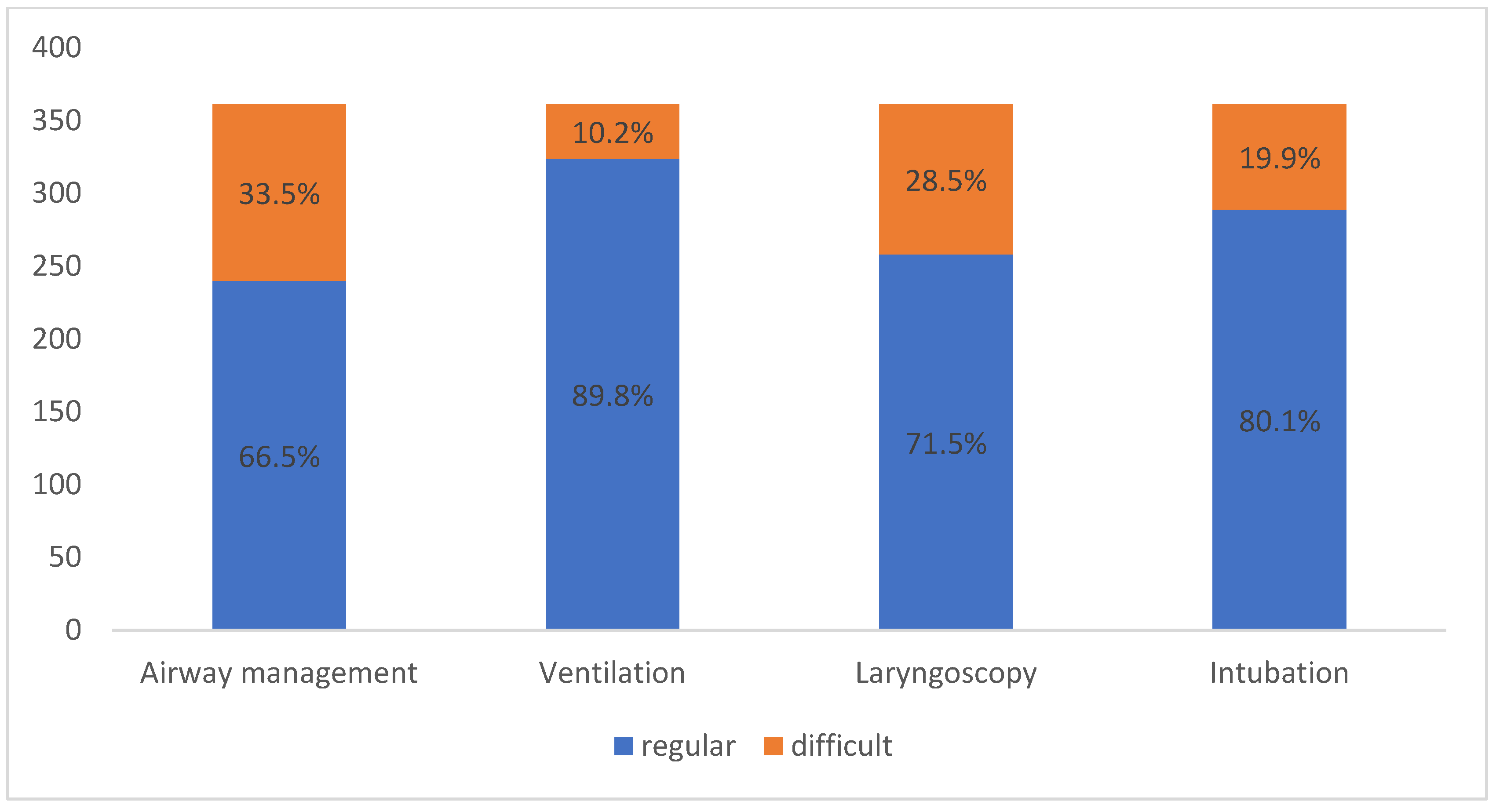
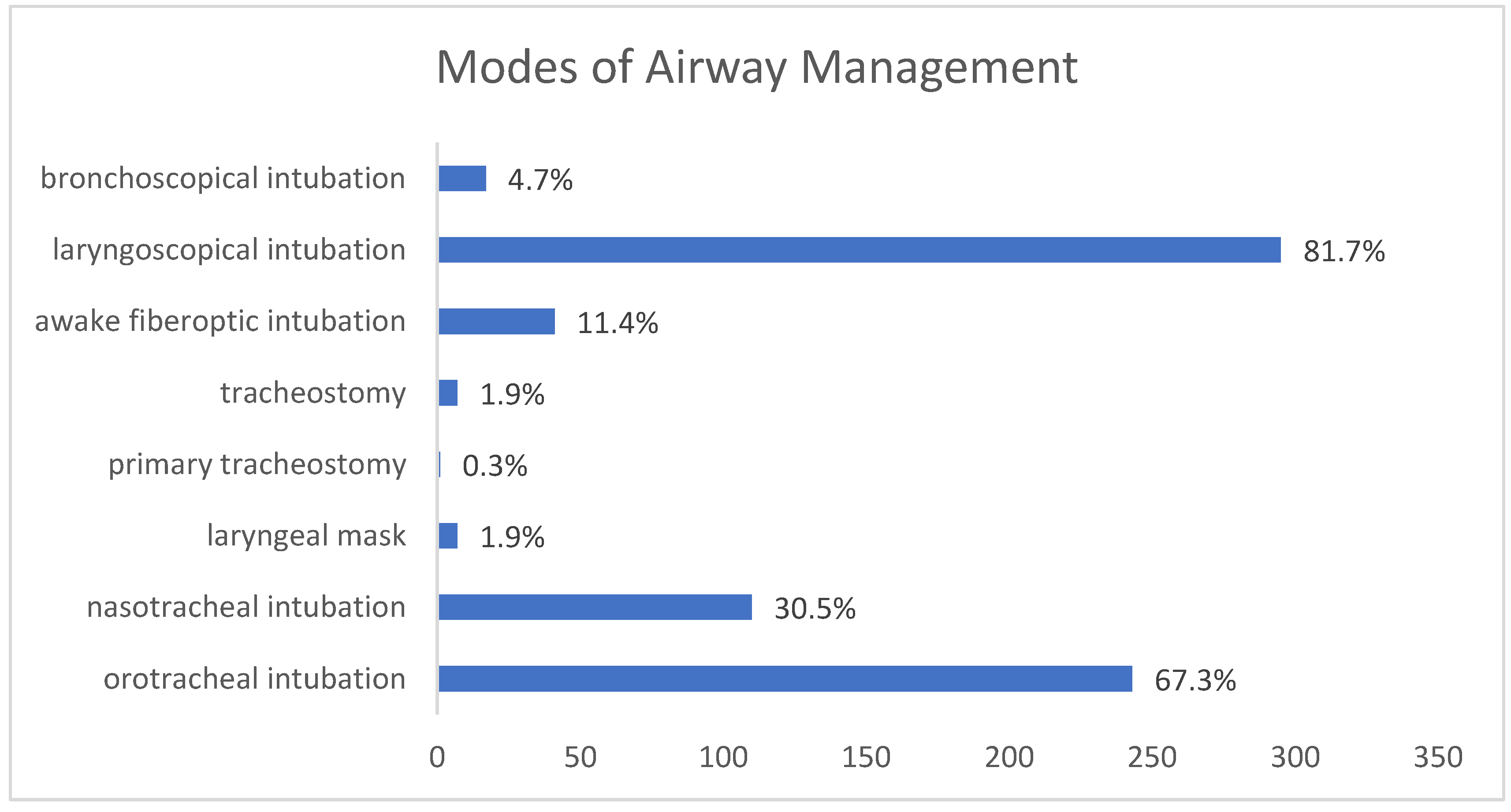
3.3. Airway Management
3.4. Multivariable Analysis
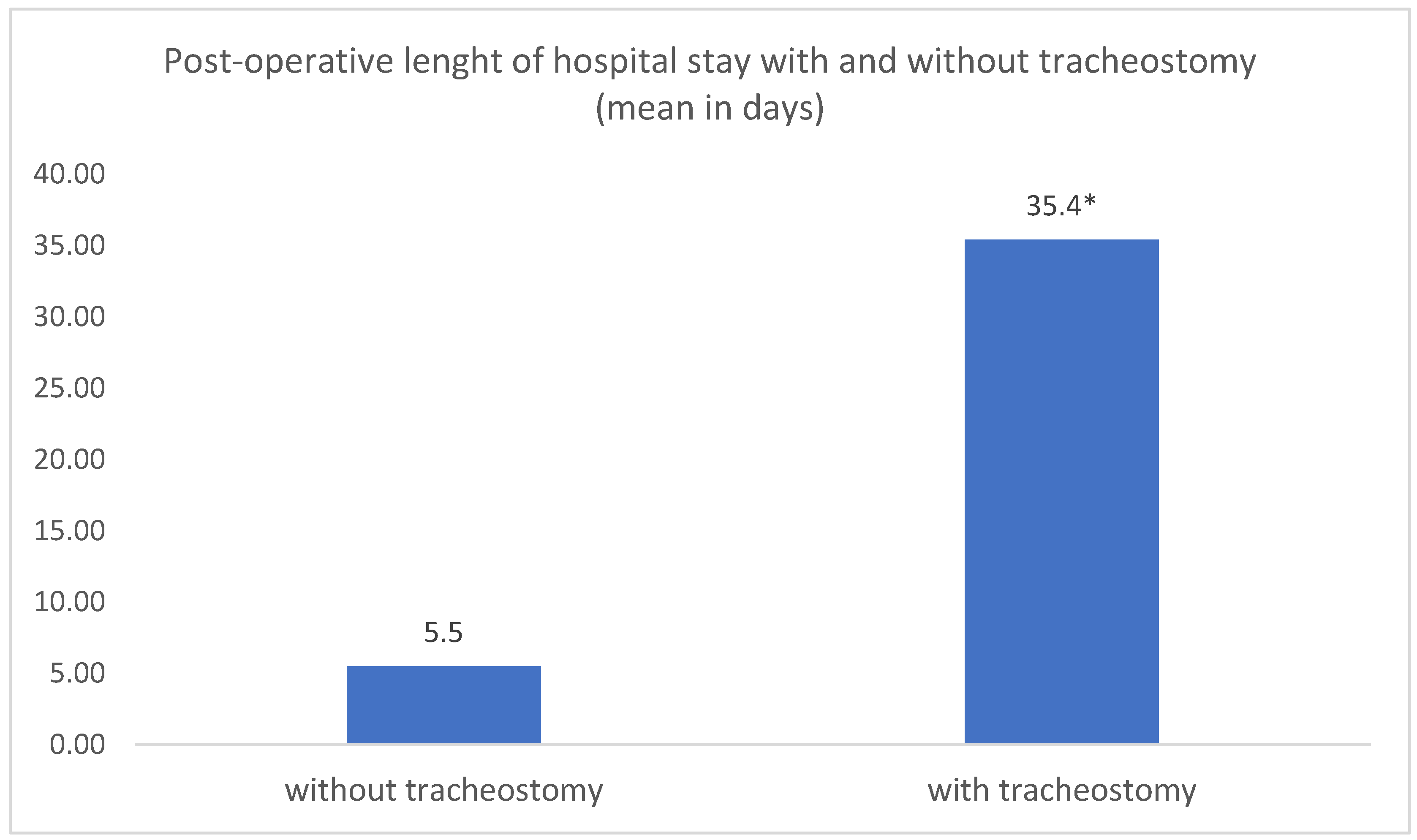
3.5. Post-operative Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bowe, C.M.; O’Neill, M.A.; O’Connell, J.E.; Kearns, G.J. The surgical management of severe dentofacial infections (DFI)-a prospective study. Ir. J. Med. Sci. 2019, 188, 327–331. [Google Scholar] [CrossRef]
- Cambria, F.; Fusconi, M.; Candelori, F.; Galli, M.; Stanganelli, F.R.F.; Venuta, F.; Valentini, V.; de Vincentiis, M. Surgical multidisciplinary approach in the management of odontogenic or non-odontogenic neck infections. Acta Otorhinolaryngol. Ital. 2021, 41, 138–144. [Google Scholar] [CrossRef]
- Buckley, J.; Harris, A.S.; Addams-Williams, J. Ten years of deep neck space abscesses. J. Laryngol. Otol. 2019, 133, 324–328. [Google Scholar] [CrossRef]
- Fu, B.; McGowan, K.; Sun, J.H.; Batstone, M. Increasing frequency and severity of odontogenic infection requiring hospital admission and surgical management. Br. J. Oral. Maxillofac. Surg. 2020, 58, 409–415. [Google Scholar] [CrossRef]
- Salomon, D.; Heidel, R.E.; Kolokythas, A.; Miloro, M.; Schlieve, T. Does restriction of public health care dental benefits affect the volume, severity, or cost of dental related hospital visits? J. Oral. Maxillofac. Surg. 2017, 75, 467–474. [Google Scholar] [CrossRef]
- Mücke, T.; Dujka, N.; Ermer, M.A.; Wolff, K.D.; Kesting, M.; Mitchell, D.A.; Ritschl, L.; Deppe, H. The value of early intraoral incisions in patients with perimandibular odontogenic maxillofacial abscesses. J. Craniomaxillofac. Surg. 2015, 43, e220–e223. [Google Scholar] [CrossRef]
- Heim, N.; Warwas, F.B.; Wiedemeyer, V.; Wilms, C.T.; Reich, R.H.; Martini, M. The role of immediate versus secondary removal of the odontogenic focus in treatment of deep head and neck space infections. A retrospective analysis of 248 patients. Clin. Oral. Investig. 2019, 23, 2921–2927. [Google Scholar] [CrossRef]
- Bhardwaj, R.; Makkar, S.; Gupta, A.; Khandelwal, K.; Nathan, K.; Basu, C.; Palaniyappan, G. Deep Neck Space Infections: Current Trends and Intricacies of Management? Indian J. Otolaryngol. Head Neck Surg. 2022, 74, 2344–2349. [Google Scholar] [CrossRef]
- Ogle, O.E. Odontogenic Infections. Dental Clin. N. Am. 2017, 61, 235–252. [Google Scholar] [CrossRef]
- Bowe, C.M.; Gargan, M.L.; Kearns, G.J.; Stassen, L. Does altered access to general dental treatment affect the number and complexity of patients presenting to the acute hospital service with severe dentofacial infections? J. Ir. Dent Assoc. 2015, 61, 196–200. [Google Scholar]
- Tapiovaara, L.K.; Aro, K.L.S.; Bäck, L.J.J.; Koskinen, A.I.M. Comparison of intubation and tracheotomy in adult patients with acute epiglottitis or supraglottitis. Eur. Arch. Otorhinolaryngol. 2019, 276, 3173–3177. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.Y.; Woo, J.H.; Kim, Y.J.; Chun, E.H.; Han, J.I.; Kim, D.Y.; Baik, H.J.; Chung, R.K. Airway management in patients with deep neck infections: A retrospective analysis. Medicine 2016, 95, e4125. [Google Scholar] [CrossRef] [PubMed]
- Piepho, T.; Cavus, E.; Noppens, R.; Byhahn, C.; Dörges, V.; Zwissler, B.; Timmermann, A. S1 Leitlinie: Atemwegsmanagement Airwaymanagement. AWMF-Register Nr.: 001/028. Available online: https://register.awmf.org/de/leitlinien/detail/001-028 (accessed on 12 March 2015).
- Nagarkar, R.; Kokane, G.; Wagh, A.; Kulkarni, N.; Roy, S.; Tandale, R.; Pawar, S. Airway management techniques in head and neck cancer surgeries: A retrospective analysis. Oral. Maxillofac. Surg. 2019, 23, 311–315. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.; Kang, H.G.; Lim, T.H.; Choi, B.Y.; Shin, Y.J.; Choi, H.J. What factors affect the success rate of the first attempt at endotracheal intubation in emergency departments? Emerg. Med. J. 2013, 30, 888–892. [Google Scholar] [CrossRef]
- Bertossi, D.; Barone, A.; Iurlaro, A.; Marconcini, S.; De Santis, D.; Finotti, M.; Procacci, P. Odontogenic Orofacial Infections. J. Craniofac. Surg. 2017, 28, 197–202. [Google Scholar] [CrossRef]
- Reddy, M.S.; Shetty, S.R.; Vannala, V. Embracing Personalized Medicine in Dentistry. J. Pharm. Bioallied. Sci. 2019, 11, 92–96. [Google Scholar] [CrossRef]
- Cormack, R.S.; Lehane, J. Difficult tracheal intubation in obstetrics. Anaesthesia 1984, 39, 1105–1111. [Google Scholar] [CrossRef]
- Mallampati, S.R.; Gatt, S.P.; Gugino, L.D.; Desai, S.P.; Waraksa, B.; Freiberger, D.; Liu, P.L. A clinical sign to predict difficult tracheal intubation: A prospective study. Can. Anaesth. Soc. J. 1985, 32, 429–434. [Google Scholar] [CrossRef]
- Kinzer, S.; Pfeifer, J.; Becker, S.; Ridder, G.J. Severe deep neck space infections and mediastinitis of odontogenic origin: Clinical relevance and implications for diagnosis and treatment. Acta Otolaryngol. 2009, 129, 62–70. [Google Scholar] [CrossRef]
- Kheterpal, S.; Han, R.; Tremper, K.K.; Shanks, A.; Tait, A.R.; O’Reilly, M.; Ludwig, T.A. Incidence and predictors of difficult and impossible mask ventilation. Anesthesiology 2006, 105, 885–891. [Google Scholar] [CrossRef]
- Kheterpal, S.; Healy, D.; Aziz, M.F.; Shanks, A.M.; Freundlich, R.E.; Linton, F.; Martin, L.D.; Linton, J.; Epps, J.L.; Fernandez-Bustamante, A.; et al. Multicenter Perioperative Outcomes Group (MPOG) Perioperative Clinical Research Committee. Incidence, predictors, and outcome of difficult mask ventilation combined with difficult laryngoscopy: A report from the multicenter perioperative outcomes group. Anesthesiology 2013, 119, 1360–1369. [Google Scholar] [CrossRef] [PubMed]
- Lavery, G.G.; McCloskey, B.V. The difficult airway in adult critical care. Crit. Care Med. 2008, 36, 2163–2173. [Google Scholar] [CrossRef] [PubMed]
- Savatmongkorngul, S.; Pitakwong, P.; Sricharoen, P.; Yuksen, C.; Jenpanitpong, C.; Watcharakitpaisan, S. Difficult Laryngoscopy Prediction Score for Intubation in Emergency Departments: A Retrospective Cohort Study. Open Access Emerg. Med. 2022, 29, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Motahari, S.J.; Poormoosa, R.; Nikkhah, M.; Bahari, M.; Shirazy, S.M.; Khavarinejad, F. Treatment and prognosis of deep neck infections. Indian J. Otolaryngol. Head Neck Surg. 2015, 67, 134–137. [Google Scholar] [CrossRef] [PubMed]
- Kataria, G.; Saxena, A.; Bhagat, S.; Singh, B.; Kaur, M.; Kaur, G. Deep neck space infections: A study of 76 cases. Iran J. Otorhinolaryngol. 2015, 27, 293–299. [Google Scholar]
- Celakovsky, P.; Kalfert, D.; Tucek, L.; Mejzlik, J.; Kotulek, M.; Vrbacky, A.; Matousek, P.; Stanikova, L.; Hoskova, T.; Pasz, A. Deep neck infections: Risk factors for mediastinal extension. Eur. Arch. Otorhinolaryngol. 2014, 271, 1679–1683. [Google Scholar] [CrossRef]
- Karkouti, K.; Rose, D.K.; Wigglesworth, D.; Cohen, M.M. Predicting difficult intubation: A multivariable analysis. Can J. Anaesth. 2000, 47, 730–739. [Google Scholar] [CrossRef]
- Rossa, B.; Selle, E. Quantitative changes in the elastic fibers of the human oral mucosa of the hard palate and cheek at various ages. Zahn. Mund Kieferheilkd Zent. 1984, 72, 217–222. [Google Scholar]
- Uribe, A.A.; Zvara, D.A.; Puente, E.G.; Otey, A.J.; Zhang, J.; Bergese, S.D. BMI as a Predictor for Potential Difficult Tracheal Intubation in Males. Front. Med. 2015, 4, 38. [Google Scholar] [CrossRef]
- Wang, T.; Sun, S.; Huang, S. The association of body mass index with difficult tracheal intubation management by direct laryngoscopy: A meta-analysis. BMC Anesth. 2018, 30, 79. [Google Scholar] [CrossRef]
- Siddiqui, A.S.; Dogar, S.A.; Lal, S.; Akhtar, S.; Khan, F.A. Airway management and postoperative length of hospital stay in patients undergoing head and neck cancer surgery. J. Anaesthesiol. Clin. Pharm. 2016, 32, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Cameron, M.; Corner, A.; Diba, A.; Hankins, M. Development of a tracheostomy scoring system to guide airway management after major head and neck surgery. Int. J. Oral. Maxillofac. Surg. 2009, 38, 846–849. [Google Scholar] [CrossRef]
- Böttger, S.; Lautenbacher, K.; Domann, E.; Howaldt, H.P.; Attia, S.; Streckbein, P.; Wilbrand, J.F. Indication for an additional postoperative antibiotic treatment after surgical incision of serious odontogenic abscesses. J. Craniomaxillofac. Surg. 2020, 48, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Cramer, J.D.; Purkey, M.R.; Smith, S.S.; Schroeder, J.W., Jr. The impact of delayed surgical drainage of deep neck abscesses in adult and pediatric populations. Laryngoscope 2016, 126, 1753–1760. [Google Scholar] [CrossRef] [PubMed]
- Doll, C.; Carl, F.; Neumann, K.; Voss, J.O.; Hartwig, S.; Waluga, R.; Heiland, M.; Raguse, J.D. Odontogenic Abscess-Related Emergency Hospital Admissions: A Retrospective Data Analysis of 120 Children and Young People Requiring Surgical Drainage. Biomed. Res. Int. 2018, 26, 3504727. [Google Scholar] [CrossRef]
- Kara, A.; Ozsurekci, Y.; Tekcicek, M.; Karadag Oncel, E.; Cengiz, A.B.; Karahan, S.; Ceyhan, M.; Celik, M.O.; Ozkaya-Parlakay, A. Length of hospital stay and management of facial cellulitis of odontogenic origin in children. Pediatr. Dent. 2014, 36, 18–22. [Google Scholar]
- Penel, N.; Mallet, Y.; Roussel-Delvallez, M.; Lefebvre, J.L.; Yazdanpanah, Y. Factors determining length of the postoperative hospital stay after major head and neck cancer surgery. Oral. Oncol. 2008, 44, 555–562. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study Population | ||
|---|---|---|
| n | % | |
| Total | 361 | 100.0% |
| Gender | ||
| male | 196 | 54.3% |
| female | 165 | 45.7% |
| Age | ||
| <30 years | 79 | 21.9% |
| ≤30–50 years | 113 | 31.3% |
| ≥50 years | 169 | 46.8% |
| BMI | ||
| <24.9 | 160 | 44.3% |
| ≤25–29.9 | 106 | 29.4% |
| ≥30 | 95 | 26.3% |
| ASA | ||
| 1 | 87 | 24.1% |
| 2 | 218 | 60.4% |
| 3 | 55 | 15.2% |
| 4 | 1 | 0.3% |
| Infection localization | ||
| paramandibular | 3 | 0.8% |
| submandibular | 111 | 30.7% |
| perimandibular | 168 | 46.5% |
| mouth floor | 5 | 1.4% |
| Submental | 36 | 10.0% |
| Massetericomandibular | 7 | 1.9% |
| pterygomandibular | 17 | 4.7% |
| parapharyngeal | 14 | 3.9% |
| Infection etiology | ||
| chronic apical parodontitis | 270 | 74.8% |
| Antiresorptiv-related osteonecrosis of the jaw | 7 | 1.9% |
| osteomyelitis | 6 | 1.7% |
| post-osteotomy | 60 | 16.6% |
| post-implantation | 7 | 1.9% |
| post-osteosynthesis | 2 | 0.6% |
| sialadenitis from submandibular gland | 2 | 0.6% |
| Unknown | 7 | 1.9% |
| Clinical symptoms | ||
| dysphagia | 330 | 91.4% |
| dyspnea | 12 | 3.3% |
| stridor | 4 | 1.1% |
| Clinical findings | ||
| mandibular rim non-palpable | 295 | 81.7% |
| restricted mouth opening | 348 | 96.4% |
| Mallampati score | ||
| 1 | 29 | 8.0% |
| 2 | 98 | 27.1% |
| 3 | 59 | 16.3% |
| 4 | 42 | 11.6% |
| 5 | 1 | 0.3% |
| No ascertainable | 132 | 36.6% |
| Cormack–Lehane grade | ||
| 1 | 167 | 46.3% |
| 2 | 91 | 25.2% |
| 3 | 57 | 15.8% |
| 4 | 12 | 3.3% |
| No ascertainable | 34 | 9.4% |
| Admission disposition | ||
| surgical ward | 345 | 95.6% |
| ICU | 16 | 4.4% |
| surgical revision | 22 | 6.1% |
| Death | 1 | 0.3% |
| Infection Localization | Intubation | |||||
|---|---|---|---|---|---|---|
| Difficult | Regular | Total | p Value | |||
| n/% | n/% | |||||
| paramandibular | 0 | 0% | 3 | 100% | 3 | ** 1.000 |
| submandibular | 19 | 17.1% | 92 | 82.9% | 111 | * 0.3703 |
| perimandibular | 35 | 20.8% | 133 | 79.2% | 168 | * 0.6934 |
| mouth floor | 2 | 40.0% | 3 | 60% | 5 | ** 0.2610 |
| submental | 7 | 19.4% | 29 | 80.6% | 36 | * 0.9369 |
| massetericomandibular | 3 | 42.6% | 4 | 57.4% | 7 | ** 0.1451 |
| pterygomandibular | 4 | 23.5% | 13 | 76.5% | 17 | ** 0.7554 |
| parapharyngeal | 2 | 14.2% | 12 | 85.8% | 14 | ** 0.7449 |
| Total | 72 | 19.9% | 289 | 80.1% | 361 | |
| Clinical Symptoms/Findings | Intubation | ||||||
|---|---|---|---|---|---|---|---|
| Difficult | Regular | Total | p Value | ||||
| n/% | n/% | ||||||
| dysphagia | yes | 3 | 25% | 9 | 75% | 12 | ** 0.7123 |
| no | 69 | 19.8% | 280 | 80.2% | 349 | ||
| dyspnea | yes | 3 | 25% | 9 | 75% | 12 | ** 0.7123 |
| no | 69 | 19.8% | 280 | 80.2% | 349 | ||
| stridor | yes | 2 | 50% | 2 | 50% | 4 | ** 0.1791 |
| no | 70 | 19.6% | 287 | 80.4% | 357 | ||
| mandibular rim | not palpable | 62 | 21.% | 233 | 79% | 295 | * 0.2810 |
| palpable | 10 | 15.2% | 56 | 84.8% | 66 | ||
| restricted mouth opening | yes | 66 | 18.9% | 272 | 81.1% | 348 | ** 0.031 |
| no | 6 | 46.1% | 7 | 53.9% | 13 | ||
| Total | 72 | 19.9% | 289 | 80.1% | 361 | ||
| Mallampati Score | Intubation | |||||
|---|---|---|---|---|---|---|
| Difficult | Regular | Total | p Value | |||
| n/% | n/% | |||||
| 1 | 1 | 3.5% | 28 | 96.5% | 29 | * < 0.0001 |
| 2 | 10 | 10.2% | 88 | 89.8% | 98 | |
| 3 | 12 | 20.3% | 47 | 79.7% | 59 | |
| 4 | 20 | 47.65 | 22 | 52.4% | 42 | |
| 5 | 1 | 100% | 0 | 0% | 1 | |
| No ascertainable | 28 | 21.2% | 104 | 78.8% | 132 | |
| Total | 72 | 19.9% | 289 | 80.1% | 361 | |
| Cormack–Lehane grade | Intubation | |||||
| difficult | regular | Total | p value | |||
| n/% | n/% | |||||
| 1 | 5 | 3% | 162 | 97% | 167 | * < 0.0001 |
| 2 | 7 | 7.7% | 84 | 92.3% | 91 | |
| 3 | 27 | 47.4% | 30 | 52.6% | 57 | |
| 4 | 11 | 91.7% | 1 | 8.3% | 12 | |
| No ascertainable | 22 | 64.7% | 12 | 35.3% | 34 | |
| Total | 72 | 289 | 361 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sakkas, A.; Weiß, C.; Zink, W.; Rodriguez, C.A.; Scheurer, M.; Pietzka, S.; Wilde, F.; Thiele, O.C.; Mischkowski, R.A.; Ebeling, M. Airway Management of Orofacial Infections Originating in the Mandible. J. Pers. Med. 2023, 13, 950. https://doi.org/10.3390/jpm13060950
Sakkas A, Weiß C, Zink W, Rodriguez CA, Scheurer M, Pietzka S, Wilde F, Thiele OC, Mischkowski RA, Ebeling M. Airway Management of Orofacial Infections Originating in the Mandible. Journal of Personalized Medicine. 2023; 13(6):950. https://doi.org/10.3390/jpm13060950
Chicago/Turabian StyleSakkas, Andreas, Christel Weiß, Wolfgang Zink, Camila Alejandra Rodriguez, Mario Scheurer, Sebastian Pietzka, Frank Wilde, Oliver Christian Thiele, Robert Andreas Mischkowski, and Marcel Ebeling. 2023. "Airway Management of Orofacial Infections Originating in the Mandible" Journal of Personalized Medicine 13, no. 6: 950. https://doi.org/10.3390/jpm13060950
APA StyleSakkas, A., Weiß, C., Zink, W., Rodriguez, C. A., Scheurer, M., Pietzka, S., Wilde, F., Thiele, O. C., Mischkowski, R. A., & Ebeling, M. (2023). Airway Management of Orofacial Infections Originating in the Mandible. Journal of Personalized Medicine, 13(6), 950. https://doi.org/10.3390/jpm13060950