
Evaluation of Antibody Kinetics Following COVID-19 Vaccination in Greek SARS-CoV-2 Infected and Naïve Healthcare Workers

 ,
,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
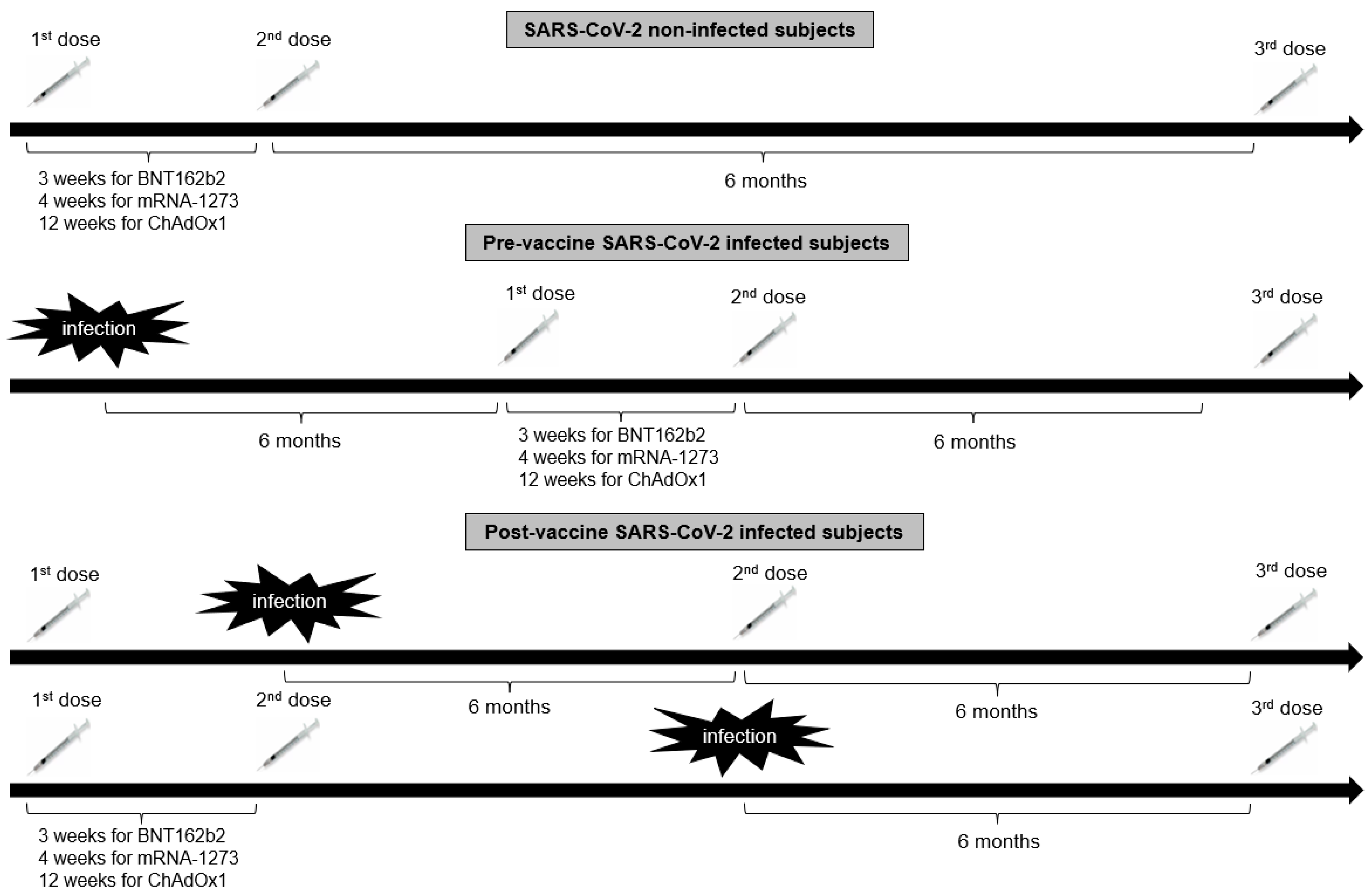
2.1. Study Design
2.2. Measurements of Antibodies
2.3. Statistical Analysis
3. Results
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 MRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the MRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and Efficacy of the ChAdOx1 NCoV-19 Vaccine (AZD1222) against SARS-CoV-2: An Interim Analysis of Four Randomised Controlled Trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against Covid-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef] [PubMed]
- Sternberg, A.; Naujokat, C. Structural Features of Coronavirus SARS-CoV-2 Spike Protein: Targets for Vaccination. Life Sci. 2020, 257, 118056. [Google Scholar] [CrossRef]
- Jagtap, S.; Ratnasri, K.; Valloly, P.; Sharma, R.; Maurya, S.; Gaigore, A.; Ardhya, C.; Biligi, D.S.; Desiraju, B.K.; Natchu, U.C.M.; et al. Evaluation of Spike Protein Antigens for SARS-CoV-2 Serology. J. Virol. Methods 2021, 296, 114222. [Google Scholar] [CrossRef] [PubMed]
- Chi, W.-Y.; Li, Y.-D.; Huang, H.-C.; Chan, T.E.H.; Chow, S.-Y.; Su, J.-H.; Ferrall, L.; Hung, C.-F.; Wu, T.-C. COVID-19 Vaccine Update: Vaccine Effectiveness, SARS-CoV-2 Variants, Boosters, Adverse Effects, and Immune Correlates of Protection. J. Biomed. Sci. 2022, 29, 82. [Google Scholar] [CrossRef]
- Yang, Z.-R.; Jiang, Y.-W.; Li, F.-X.; Liu, D.; Lin, T.-F.; Zhao, Z.-Y.; Wei, C.; Jin, Q.-Y.; Li, X.-M.; Jia, Y.-X.; et al. Efficacy of SARS-CoV-2 Vaccines and the Dose–Response Relationship with Three Major Antibodies: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Lancet Microbe 2023, 4, e236–e246. [Google Scholar] [CrossRef]
- Nielsen, K.F.; Moustsen-Helms, I.R.; Schelde, A.B.; Gram, M.A.; Emborg, H.-D.; Nielsen, J.; Hansen, C.H.; Andersen, M.A.; Meaidi, M.; Wohlfahrt, J.; et al. Vaccine Effectiveness against SARS-CoV-2 Reinfection during Periods of Alpha, Delta, or Omicron Dominance: A Danish Nationwide Study. PLoS Med. 2022, 19, e1004037. [Google Scholar] [CrossRef]
- Favresse, J.; Bayart, J.-L.; Mullier, F.; Elsen, M.; Eucher, C.; Van Eeckhoudt, S.; Roy, T.; Wieers, G.; Laurent, C.; Dogné, J.-M.; et al. Antibody Titres Decline 3-Month Post-Vaccination with BNT162b2. Emerg. Microbes Infect. 2021, 10, 1495–1498. [Google Scholar] [CrossRef]
- Salvagno, G.L.; Henry, B.M.; Pighi, L.; de Nitto, S.; Lippi, G. Total Anti-SARS-CoV-2 Antibodies Measured 6 Months after Pfizer-BioNTech COVID-19 Vaccination in Healthcare Workers. J. Med. Biochem. 2022, 41, 199–203. [Google Scholar] [CrossRef]
- Romero-Ibarguengoitia, M.E.; Rivera-Salinas, D.; Hernández-Ruíz, Y.G.; Armendariz-Vázquez, A.G.; González-Cantú, A.; Barco-Flores, I.A.; González-Facio, R.; Montelongo-Cruz, L.P.; Del Rio-Parra, G.F.; Garza-Herrera, M.R.; et al. Effect of the Third Dose of BNT162b2 Vaccine on Quantitative SARS-CoV-2 Spike 1–2 IgG Antibody Titers in Healthcare Personnel. PLoS ONE 2022, 17, e0263942. [Google Scholar] [CrossRef] [PubMed]
- Doria-Rose, N.; Suthar, M.S.; Makowski, M.; O’Connell, S.; McDermott, A.B.; Flach, B.; Ledgerwood, J.E.; Mascola, J.R.; Graham, B.S.; Lin, B.C.; et al. Antibody Persistence through 6 Months after the Second Dose of MRNA-1273 Vaccine for Covid-19. N. Engl. J. Med. 2021, 384, 2259–2261. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, D.; Clementi, N.; Criscuolo, E.; Ambrosi, A.; Corea, F.; Di Resta, C.; Tomaiuolo, R.; Mancini, N.; Locatelli, M.; Plebani, M.; et al. Antibody Titer Kinetics and SARS-CoV-2 Infections Six Months after Administration with the BNT162b2 Vaccine. Vaccines 2021, 9, 1357. [Google Scholar] [CrossRef]
- Ferrari, D.; Ambrosi, A.; Di Resta, C.; Tomaiuolo, R.; Locatelli, M.; Banfi, G. Evaluation of Antibody Titer Kinetics and SARS-CoV-2 Infections in a Large Cohort of Healthcare Professionals Ten Months after Administration of the BNT162b2 Vaccine. J. Immunol. Methods 2022, 506, 113293. [Google Scholar] [CrossRef] [PubMed]
- Bates, T.A.; McBride, S.K.; Leier, H.C.; Guzman, G.; Lyski, Z.L.; Schoen, D.; Winders, B.; Lee, J.-Y.; Lee, D.X.; Messer, W.B.; et al. Vaccination before or after SARS-CoV-2 Infection Leads to Robust Humoral Response and Antibodies That Effectively Neutralize Variants. Sci. Immunol. 2022, 7, eabn8014. [Google Scholar] [CrossRef]
- Wang, Z.; Muecksch, F.; Schaefer-Babajew, D.; Finkin, S.; Viant, C.; Gaebler, C.; Hoffmann, H.-H.; Barnes, C.O.; Cipolla, M.; Ramos, V.; et al. Naturally Enhanced Neutralizing Breadth against SARS-CoV-2 One Year after Infection. Nature 2021, 595, 426–431. [Google Scholar] [CrossRef]
- English, E.; Cook, L.E.; Piec, I.; Dervisevic, S.; Fraser, W.D.; John, W.G. Performance of the Abbott SARS-CoV-2 IgG II Quantitative Antibody Assay Including the New Variants of Concern, VOC 202012/V1 (United Kingdom) and VOC 202012/V2 (South Africa), and First Steps towards Global Harmonization of COVID-19 Antibody Methods. J. Clin. Microbiol. 2021, 59, e00288-21. [Google Scholar] [CrossRef]
- Rodda, L.B.; Netland, J.; Shehata, L.; Pruner, K.B.; Morawski, P.A.; Thouvenel, C.D.; Takehara, K.K.; Eggenberger, J.; Hemann, E.A.; Waterman, H.R.; et al. Functional SARS-CoV-2-Specific Immune Memory Persists after Mild COVID-19. Cell 2021, 184, 169–183.e17. [Google Scholar] [CrossRef]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological Memory to SARS-CoV-2 Assessed for up to 8 Months after Infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef]
- Trougakos, I.P.; Terpos, E.; Zirou, C.; Sklirou, A.D.; Apostolakou, F.; Gumeni, S.; Charitaki, I.; Papanagnou, E.-D.; Bagratuni, T.; Liacos, C.-I.; et al. Comparative Kinetics of SARS-CoV-2 Anti-Spike Protein RBD IgGs and Neutralizing Antibodies in Convalescent and Naïve Recipients of the BNT162b2 MRNA Vaccine versus COVID-19 Patients. BMC Med. 2021, 19, 208. [Google Scholar] [CrossRef] [PubMed]
- Ogrič, M.; Žigon, P.; Podovšovnik, E.; Lakota, K.; Sodin-Semrl, S.; Rotar, Ž.; Čučnik, S. Differences in SARS-CoV-2-Specific Antibody Responses After the First, Second, and Third Doses of BNT162b2 in Naïve and Previously Infected Individuals: A 1-Year Observational Study in Healthcare Professionals. Front. Immunol. 2022, 13, 876533. [Google Scholar] [CrossRef] [PubMed]
- Shrotri, M.; Navaratnam, A.M.D.; Nguyen, V.; Byrne, T.; Geismar, C.; Fragaszy, E.; Beale, S.; Fong, W.L.E.; Patel, P.; Kovar, J.; et al. Spike-Antibody Waning after Second Dose of BNT162b2 or ChAdOx1. Lancet 2021, 398, 385–387. [Google Scholar] [CrossRef] [PubMed]
- Israel, A.; Shenhar, Y.; Green, I.; Merzon, E.; Golan-Cohen, A.; Schäffer, A.A.; Ruppin, E.; Vinker, S.; Magen, E. Large-Scale Study of Antibody Titer Decay Following BNT162b2 MRNA Vaccine or SARS-CoV-2 Infection. Vaccines 2021, 10, 64. [Google Scholar] [CrossRef]
- Falsey, A.R.; Frenck, R.W.; Walsh, E.E.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Bailey, R.; Swanson, K.A.; Xu, X.; et al. SARS-CoV-2 Neutralization with BNT162b2 Vaccine Dose 3. N. Engl. J. Med. 2021, 385, 1627–1629. [Google Scholar] [CrossRef]
- Pape, K.A.; Taylor, J.J.; Maul, R.W.; Gearhart, P.J.; Jenkins, M.K. Different B Cell Populations Mediate Early and Late Memory during an Endogenous Immune Response. Science 2011, 331, 1203–1207. [Google Scholar] [CrossRef]
- Grupel, D.; Gazit, S.; Schreiber, L.; Nadler, V.; Wolf, T.; Lazar, R.; Supino-Rosin, L.; Perez, G.; Peretz, A.; Ben Tov, A.; et al. Kinetics of SARS-CoV-2 Anti-S IgG after BNT162b2 Vaccination. Vaccine 2021, 39, 5337–5340. [Google Scholar] [CrossRef]
- Müller, L.; Andrée, M.; Moskorz, W.; Drexler, I.; Walotka, L.; Grothmann, R.; Ptok, J.; Hillebrandt, J.; Ritchie, A.; Rabl, D.; et al. Age-Dependent Immune Response to the Biontech/Pfizer BNT162b2 Coronavirus Disease 2019 Vaccination. Clin. Infect. Dis. 2021, 73, 2065–2072. [Google Scholar] [CrossRef]
- Oliveira-Silva, J.; Reis, T.; Lopes, C.; Batista-Silva, R.; Ribeiro, R.; Marques, G.; Pacheco, V.; Rodrigues, T.; Afonso, A.; Pinheiro, V.; et al. Humoral Response to the SARS-CoV-2 BNT162b2 MRNA Vaccine: Real-World Data from a Large Cohort of Healthcare Workers. Vaccine 2022, 40, 650–655. [Google Scholar] [CrossRef]
- Bajaj, V.; Gadi, N.; Spihlman, A.P.; Wu, S.C.; Choi, C.H.; Moulton, V.R. Aging, Immunity, and COVID-19: How Age Influences the Host Immune Response to Coronavirus Infections? Front. Physiol. 2020, 11, 571416. [Google Scholar] [CrossRef]
- Terpos, E.; Trougakos, I.P.; Apostolakou, F.; Charitaki, I.; Sklirou, A.D.; Mavrianou, N.; Papanagnou, E.-D.; Liacos, C.-I.; Gumeni, S.; Rentziou, G.; et al. Age-Dependent and Gender-Dependent Antibody Responses against SARS-CoV-2 in Health Workers and Octogenarians after Vaccination with the BNT162b2 MRNA Vaccine. Am. J. Hematol. 2021, 96, E257–E259. [Google Scholar] [CrossRef] [PubMed]
- Anastassopoulou, C.; Antoni, D.; Manoussopoulos, Y.; Stefanou, P.; Argyropoulou, S.; Vrioni, G.; Tsakris, A. Age and Sex Associations of SARS-CoV-2 Antibody Responses Post BNT162b2 Vaccination in Healthcare Workers: A Mixed Effects Model across Two Vaccination Periods. PLoS ONE 2022, 17, e0266958. [Google Scholar] [CrossRef] [PubMed]
- Ward, H.; Whitaker, M.; Flower, B.; Tang, S.N.; Atchison, C.; Darzi, A.; Donnelly, C.A.; Cann, A.; Diggle, P.J.; Ashby, D.; et al. Population Antibody Responses Following COVID-19 Vaccination in 212,102 Individuals. Nat. Commun. 2022, 13, 907. [Google Scholar] [CrossRef] [PubMed]
- Bichara, C.D.A.; Queiroz, M.A.F.; da Silva Graça Amoras, E.; Vaz, G.L.; Vallinoto, I.M.V.C.; Bichara, C.N.C.; do Amaral, I.P.C.; Ishak, R.; Vallinoto, A.C.R. Assessment of Anti-SARS-CoV-2 Antibodies Post-Coronavac Vaccination in the Amazon Region of Brazil. Vaccines 2021, 9, 1169. [Google Scholar] [CrossRef]
- Michos, A.; Tatsi, E.-B.; Filippatos, F.; Dellis, C.; Koukou, D.; Efthymiou, V.; Kastrinelli, E.; Mantzou, A.; Syriopoulou, V. Association of Total and Neutralizing SARS-CoV-2 Spike -Receptor Binding Domain Antibodies with Epidemiological and Clinical Characteristics after Immunization with the 1st and 2nd Doses of the BNT162b2 Vaccine. Vaccine 2021, 39, 5963–5967. [Google Scholar] [CrossRef]
- Ciarambino, T.; Para, O.; Giordano, M. Immune System and COVID-19 by Sex Differences and Age. Women’s Health 2021, 17, 17455065211022262. [Google Scholar] [CrossRef] [PubMed]
- Poland, G.A.; Ovsyannikova, I.G.; Kennedy, R.B. Personalized Vaccinology: A Review. Vaccine 2018, 36, 5350–5357. [Google Scholar] [CrossRef]
- Pavlidis, G.; Kampolis, C.F.; Perlepe, G.; Pagonis, A.; Maniotis, C.; Koullias, E.; Kranidioti, H.; Kyritsis, A.; Pavlou, E.; Sinis, S.; et al. Do the Kinetics of Antibody Responses Predict Clinical Outcome in Hospitalized Patients With Moderate-to-Severe COVID-19? Vivo 2022, 36, 1944–1948. [Google Scholar] [CrossRef]
- Bobrovitz, N.; Ware, H.; Ma, X.; Li, Z.; Hosseini, R.; Cao, C.; Selemon, A.; Whelan, M.; Premji, Z.; Issa, H.; et al. Protective Effectiveness of Previous SARS-CoV-2 Infection and Hybrid Immunity against the Omicron Variant and Severe Disease: A Systematic Review and Meta-Regression. Lancet Infect. Dis. 2023, 23, 556–567. [Google Scholar] [CrossRef]
- Nivette, A.; Ribeaud, D.; Murray, A.; Steinhoff, A.; Bechtiger, L.; Hepp, U.; Shanahan, L.; Eisner, M. Non-Compliance with COVID-19-Related Public Health Measures among Young Adults in Switzerland: Insights from a Longitudinal Cohort Study. Soc. Sci. Med. 2021, 268, 113370. [Google Scholar] [CrossRef]
- Letizia, A.G.; Ge, Y.; Vangeti, S.; Goforth, C.; Weir, D.L.; Kuzmina, N.A.; Balinsky, C.A.; Chen, H.W.; Ewing, D.; Soares-Schanoski, A.; et al. SARS-CoV-2 Seropositivity and Subsequent Infection Risk in Healthy Young Adults: A Prospective Cohort Study. Lancet Respir. Med. 2021, 9, 712–720. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All Subjects | Pre-Vaccine SARS-CoV-2 Infected Subjects | Post-Vaccine SARS-CoV-2 Infected Subjects | SARS-CoV-2 Non-Infected Subjects | |
|---|---|---|---|---|
| n = 803 | n = 100 | n = 335 | n = 368 | |
| Age, years | 51 (40–57) | 46.5 (30–55) * | 49 (39–56) ‡‡ | 53 (43–58) ‡‡‡ |
| Sex (female), n (%) | 540 (67.2) | 62 (62) | 238 (71) | 240 (65.2) |
| Vaccine, n (%) | ||||
| BNT162b2 (Pfizer-BioNTech) | 758 (94.4) | 91 (91) | 319 (95.2) | 348 (94.6) |
| mRNA-1273 (Moderna) | 8 (1) | 2 (2) | 2 (0.6) | 4 (1.1) |
| ChAdOx1 (Oxford-AstraZeneca) | 14 (1.7) | 1 (1) | 4 (1.2) | 9 (2.5) |
| Ad26.COV2.S (Janssen) | 23 (2.9) | 6 (6) | 10 (3) | 7 (1.9) *** |
| Hospitalization, n (%) | 13 (1.6) | 8 (8) † | 5 (1.5) | - |
| Intubation, n (%) | 1 (0.1) | 1 (1) | 0 (0) | - |
| SARS-CoV-2 reinfection, n (%) | 39 (4.9) | 28 (28) ‡ | 11 (3.3) | - |
| Time from 2nd vaccine dose to first SARS-CoV-2 infection, months | - | 11.9 (8.2–14) | - | |
| Time from 2nd vaccine dose to SARS-CoV-2 reinfection, months | 11.1 (6–13.1) | 8.9 (4.6–13.4) * | 11.4 (11–12) | - |
| Co-morbidities, n (%) | ||||
| Obesity | 110 (13.7) | 14 (14) | 49 (14.6) | 47 (12.8) |
| Hypertension | 112 (13.9) | 15 (15) | 55 (16.4) | 42 (11.4) |
| Dyslipidemia | 142 (17.7) | 18 (18) | 58 (17.3) | 66 (18) |
| Diabetes mellitus | 41 (5.1) | 4 (4) | 21 (6.3) | 16 (4.3) |
| CAD | 14 (1.7) | 5 (5) * | 5 (1.5) | 4 (1.1) *** |
| COPD | 4 (0.5) | 0 (0) | 3 (0.9) | 1 (0.3) |
| Cancer | 16 (2) | 2 (2) | 4 (1.2) | 10 (2.7) |
| Immunosuppression | 7 (0.9) | 3 (3) * | 2 (0.6) | 2 (0.5) *** |
| Number of co-morbidities, n (%) | ||||
| None | 542 (67.5) | 65 (65) | 225 (67.1) | 252 (68.5) |
| 1 | 143 (17.8) | 19 (19) | 55 (16.4) | 69 (18.8) |
| 2 | 64 (8) | 9 (9) | 28 (8.4) | 27 (7.3) |
| ≥3 | 54 (6.7) | 7 (7) | 27 (8.1) | 20 (5.4) |
| Medications, n (%) | ||||
| ACEi/ARBs | 90 (11.2) | 12 (12) | 45 (13.4) | 33 (9) |
| CCB | 69 (8.6) | 8 (8) | 36 (10.7) | 25 (6.8) |
| β-Blockers | 39 (4.9) | 5 (5) | 23 (6.8) ** | 11 (3) |
| Diuretics | 31 (3.9) | 5 (5) | 12 (3.6) | 14 (3.8) |
| Antiplatelets | 26 (3.2) | 6 (6) | 10 (3) | 10 (2.7) |
| Anticoagulants | 10 (1.2) | 0 (0) | 5 (1.5) | 5 (1.4) |
| Statins | 139 (17.3) | 18 (18) | 58 (17.3) | 63 (17.2) |
| Fibrates | 3 (0.4) | 1 (1) | 2 (0.6) | 0 (0) |
| Antidiabetics | 35 (4.4) | 4 (4) | 17 (5.1) | 14 (3.8) |
| Insulin | 8 (1) | 0 (0) | 2 (0.6) | 6 (1.6) |
| Corticosteroids | 10 (1.2) | 2 (2) | 2 (0.6) | 6 (1.6) |
| Pre-vaccine SARS-CoV-2 infection (n = 100) | |
|---|---|
| n (%) | |
| One infection pre-vaccination | 72 (72) |
| Reinfection (pre- or post-vaccination) | 28 (28) |
| Post-vaccine SARS-CoV-2 infection (n = 335) | |
| n (%) | |
| Between first and second vaccine dose | 10 (3) |
| Between second and third vaccine dose | 82 (24) |
| Post-third vaccine dose | 243 (73) |
| Total SARS-CoV-2 reinfection (n = 39) | |
| n (%) | |
| Prior to vaccination | 4 (10) |
| Between first and second vaccine dose | 5 (13) |
| Between second and third vaccine dose | 9 (23) |
| Post-third vaccine dose | 21 (54) |
| All Subjects | Pre-Vaccine SARS-CoV-2 Infected Subjects | Post-Vaccine SARS-CoV-2 Infected Subjects | SARS-CoV-2 Non-Infected Subjects | |
|---|---|---|---|---|
| n = 803 | n = 100 | n = 335 | n = 368 | |
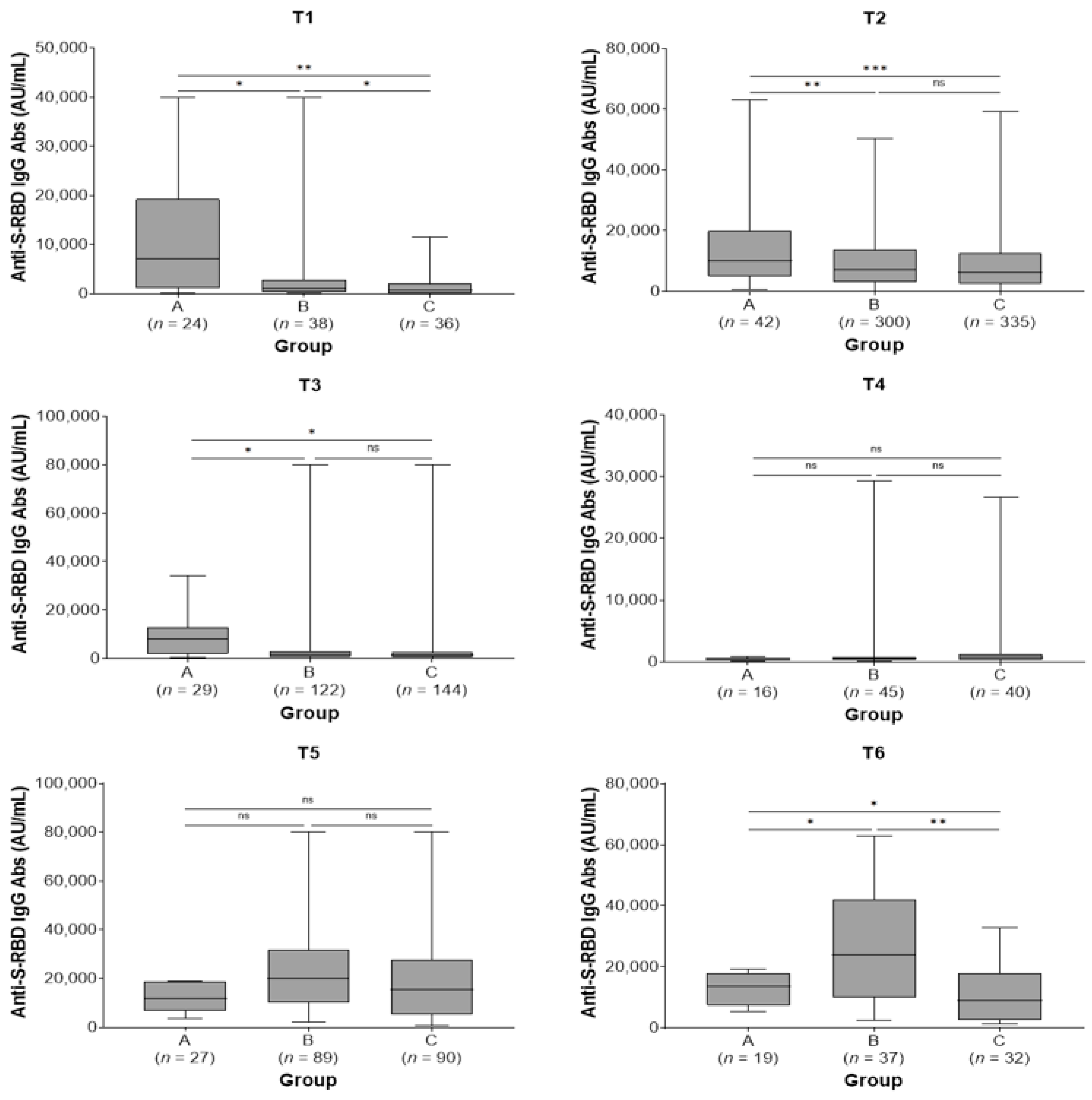
| Anti-S-RBD IgG Abs (AU/mL) pre-second vaccine dose (2 months post-first dose; T1) | 1285 (419–11,688) (n = 98) | 7181 (1120–19,257) * (n = 24) | 1136 (330–2859) ** (n = 38) | 623 (113–2190) ††† (n = 36) |
| Anti-S-RBD IgG Abs (AU/mL) at 2 months post-second vaccine dose (T2) | 6934 (2601–13,091) (n = 677) | 10,134 (4852–20,025) † (n = 42) | 7144 (2916–13,848) (n = 300) | 6169 (2399–12,554) ‡ (n = 335) |
| Anti-S-RBD IgG Abs (AU/mL) at 6 months post-second vaccine dose (T3) | 1370 (664–2864) (n = 295) | 7876 (1792–12,944) * (n = 29) | 1426 (661–2968) (n = 122) | 1266 (613–2690) *** (n = 144) |
| Anti-S-RBD IgG Abs (AU/mL) at 9 months post-second vaccine dose (pre-third dose; T4) | 560 (273–1000) (n = 101) | 432 (259–701) (n = 16) | 512 (272–833) (n = 45) | 649 (279–1257) (n = 40) |
| Anti-S-RBD IgG Abs (AU/mL) at 2 months post-third vaccine dose (T5) | 17,203 (8607–28,252) (n = 206) | 11,887 (6655–18,841) (n = 27) | 19,876 (10,077–31,755) (n = 89) | 15,524 (5385–27,710) (n = 90) |
| Anti-S-RBD IgG Abs (AU/mL) at 6 months post-third vaccine dose (T6) | 14,226 (5894–28,137) (n = 88) | 13,590 (7302–17,994) * (n = 19) | 23,848 (9829–42,075) †† (n = 37) | 8882 (2474–17,819) *** (n = 32) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pavlidis, G.; Giannoulis, V.; Pirounaki, M.; Lampropoulos, I.C.; Siafi, E.; Nitsa, A.; Pavlou, E.; Xanthaki, A.; Perlepe, G.; Fortis, S.P.; et al. Evaluation of Antibody Kinetics Following COVID-19 Vaccination in Greek SARS-CoV-2 Infected and Naïve Healthcare Workers. J. Pers. Med. 2023, 13, 910. https://doi.org/10.3390/jpm13060910
Pavlidis G, Giannoulis V, Pirounaki M, Lampropoulos IC, Siafi E, Nitsa A, Pavlou E, Xanthaki A, Perlepe G, Fortis SP, et al. Evaluation of Antibody Kinetics Following COVID-19 Vaccination in Greek SARS-CoV-2 Infected and Naïve Healthcare Workers. Journal of Personalized Medicine. 2023; 13(6):910. https://doi.org/10.3390/jpm13060910
Chicago/Turabian StylePavlidis, George, Vasileios Giannoulis, Maria Pirounaki, Ioannis C. Lampropoulos, Eirini Siafi, Alkippi Nitsa, Efthymia Pavlou, Anna Xanthaki, Garyfallia Perlepe, Sotirios P. Fortis, and et al. 2023. "Evaluation of Antibody Kinetics Following COVID-19 Vaccination in Greek SARS-CoV-2 Infected and Naïve Healthcare Workers" Journal of Personalized Medicine 13, no. 6: 910. https://doi.org/10.3390/jpm13060910
APA StylePavlidis, G., Giannoulis, V., Pirounaki, M., Lampropoulos, I. C., Siafi, E., Nitsa, A., Pavlou, E., Xanthaki, A., Perlepe, G., Fortis, S. P., Charalambous, G., Kampolis, C. F., & Pantazopoulos, I. (2023). Evaluation of Antibody Kinetics Following COVID-19 Vaccination in Greek SARS-CoV-2 Infected and Naïve Healthcare Workers. Journal of Personalized Medicine, 13(6), 910. https://doi.org/10.3390/jpm13060910