
Resting State EEG Correlates of Suicide Ideation and Suicide Attempt




Abstract
1. Introduction
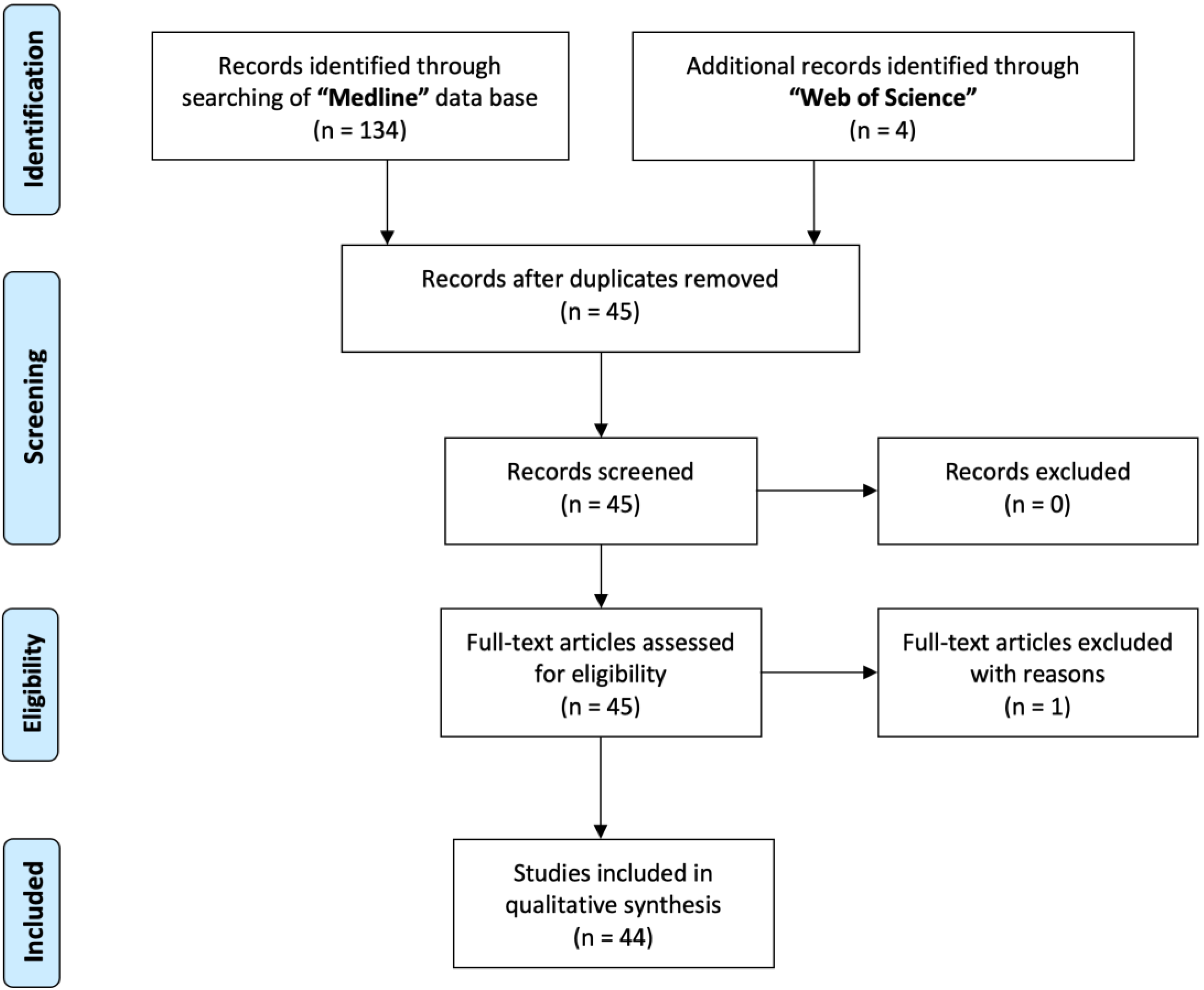
2. Methods
3. Results
3.1. Delta
3.2. Theta
3.3. Alpha
3.4. Beta and Gamma
3.5. Frontal Alpha Asymmetry
4. Discussion
5. Limitations
6. Conclusions
7. Future Directions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Williams, J.M.; Broadbent, K. Distraction by emotional stimuli: Use of a Stroop task with suicide attempters. Br. J. Clin. Psychol. 1986, 25 Pt 2, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Becker, E.S.; Strohbach, D.; Rinck, M. A specific attentional bias in suicide attempters. J. Nerv. Ment. Dis. 1999, 187, 730–735. [Google Scholar] [CrossRef]
- Keilp, J.G.; Sackeim, H.A.; Brodsky, B.S.; Oquendo, M.A.; Malone, K.M.; Mann, J.J. Neuropsychological dysfunction in depressed suicide attempters. Am. J. Psychiatry 2001, 158, 735–741. [Google Scholar] [CrossRef] [PubMed]
- WHO. Creating Hope through Action. Available online: https://www.who.int/campaigns/world-suicide-prevention-day/2022 (accessed on 10 March 2023).
- Hooley, J.M.; Parker, H.A. Measuring expressed emotion: An evaluation of the shortcuts. J. Fam. Psychol. 2006, 20, 386–396. [Google Scholar] [CrossRef] [PubMed]
- Balon, R. Rating scales for anxiety/anxiety disorders. Curr. Psychiatry Rep. 2007, 9, 271–277. [Google Scholar] [CrossRef]
- Furukawa, T.A. Assessment of mood: Guides for clinicians. J. Psychosom. Res. 2010, 68, 581–589. [Google Scholar] [CrossRef]
- Hall, J.A. Clinicians’ accuracy in perceiving patients: Its relevance for clinical practice and a narrative review of methods and correlates. Patient Educ. Couns. 2011, 84, 319–324. [Google Scholar] [CrossRef]
- Swann, A.C.; Dougherty, D.M.; Pazzaglia, P.J.; Pham, M.; Steinberg, J.L.; Moeller, F.G. Increased impulsivity associated with severity of suicide attempt history in patients with bipolar disorder. Am. J. Psychiatry 2005, 162, 1680–1687. [Google Scholar] [CrossRef]
- Claassen, C.A.; Harvilchuck-Laurenson, J.D.; Fawcett, J. Prognostic models to detect and monitor the near-term risk of suicide: State of the science. Am. J. Prev. Med. 2014, 47, S181–S185. [Google Scholar] [CrossRef]
- Johnston, J.N.; Campbell, D.; Caruncho, H.J.; Henter, I.D.; Ballard, E.D.; Zarate, C.A. Suicide Biomarkers to Predict Risk, Classify Diagnostic Subtypes, and Identify Novel Therapeutic Targets: 5 Years of Promising Research. Int. J. Neuropsychopharmacol. 2022, 25, 197–214. [Google Scholar] [CrossRef]
- Bani-Fatemi, A.; Tasmim, S.; Graff-Guerrero, A.; Gerretsen, P.; Strauss, J.; Kolla, N.; Spalletta, G.; De Luca, V. Structural and functional alterations of the suicidal brain: An updated review of neuroimaging studies. Psychiatry Res. Neuroimaging 2018, 278, 77–91. [Google Scholar] [CrossRef]
- Jollant, F.; Lawrence, N.L.; Olié, E.; Guillaume, S.; Courtet, P. The suicidal mind and brain: A review of neuropsychological and neuroimaging studies. World J. Biol. Psychiatry 2011, 12, 319–339. [Google Scholar] [CrossRef]
- Abi-Dargham, A.; Horga, G. The search for imaging biomarkers in psychiatric disorders. Nat. Med. 2016, 22, 1248–1255. [Google Scholar] [CrossRef] [PubMed]
- van Beek, E.J.R.; Kuhl, C.; Anzai, Y.; Desmond, P.; Ehman, R.L.; Gong, Q.; Gold, G.; Gulani, V.; Hall-Craggs, M.; Leiner, T.; et al. Value of MRI in medicine: More than just another test? J. Magn. Reson. Imaging 2019, 49, e14–e25. [Google Scholar] [CrossRef]
- Fenton, G.W. The electroencephalogram in psychiatry: Clinical and research applications. Psychiatr. Dev. 1984, 2, 53–75. [Google Scholar]
- Newson, J.J.; Thiagarajan, T.C. EEG Frequency Bands in Psychiatric Disorders: A Review of Resting State Studies. Front. Hum. Neurosci. 2018, 12, 521. [Google Scholar] [CrossRef]
- Buzsáki, G. Rhythms of the Brain; Oxford University Press: Oxford, UK, 2006. [Google Scholar]
- Britton, J.W.; Frey, L.C.; Hopp, J.L.; Korb, P.; Koubeissi, M.Z.; Lievens, W.E.; Pestana-Knight, E.M.; St. Louis, E.K. Electroencephalography (EEG): An Introductory Text and Atlas of Normal and Abnormal Findings in Adults, Children, and Infants; St. Louis, E.K., Frey, L.C., Eds.; American Epilepsy Society: Chicago, IL, USA, 2016. [Google Scholar]
- O’Sullivan, S.S.; Mullins, G.M.; Cassidy, E.M.; McNamara, B. The role of the standard EEG in clinical psychiatry. Hum. Psychopharmacol. 2006, 21, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Livint Popa, L.; Dragos, H.; Pantelemon, C.; Verisezan Rosu, O.; Strilciuc, S. The Role of Quantitative EEG in the Diagnosis of Neuropsychiatric Disorders. J. Med. Life 2020, 13, 8–15. [Google Scholar] [CrossRef]
- Meerwijk, E.L.; Ford, J.M.; Weiss, S.J. Resting-state EEG delta power is associated with psychological pain in adults with a history of depression. Biol. Psychol. 2015, 105, 106–114. [Google Scholar] [CrossRef]
- Meerwijk, E.L.; Weiss, S.J. Does suicidal desire moderate the association between frontal delta power and psychological pain? PeerJ 2016, 4, e1538. [Google Scholar] [CrossRef] [PubMed]
- Hawton, K.; Casanas, I.C.C.; Haw, C.; Saunders, K. Risk factors for suicide in individuals with depression: A systematic review. J. Affect Disord. 2013, 147, 17–28. [Google Scholar] [CrossRef]
- Bradvik, L. Suicide Risk and Mental Disorders. Int. J. Environ. Res. Public Health 2018, 15, 2028. [Google Scholar] [CrossRef] [PubMed]
- Jandl, M.; Steyer, J.; Kaschka, W.P. Suicide risk markers in major depressive disorder: A study of electrodermal activity and event-related potentials. J. Affect Disord. 2010, 123, 138–149. [Google Scholar] [CrossRef] [PubMed]
- Graae, F.; Tenke, C.; Bruder, G.; Rotheram, M.J.; Piacentini, J.; Castro-Blanco, D.; Leite, P.; Towey, J. Abnormality of EEG alpha asymmetry in female adolescent suicide attempters. Biol. Psychiatry 1996, 40, 706–713. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.S.; Youn, T.; Jung, H.Y. Right hemisphere abnormalities in major depression: Quantitative electroencephalographic findings before and after treatment. J. Affect Disord. 1996, 40, 169–173. [Google Scholar] [CrossRef]
- Jaworska, N.; Blier, P.; Fusee, W.; Knott, V. alpha Power, alpha asymmetry and anterior cingulate cortex activity in depressed males and females. J. Psychiatr. Res. 2012, 46, 1483–1491. [Google Scholar] [CrossRef]
- Suetsugi, M.; Mizuki, Y.; Ushijima, I.; Kobayashi, T.; Tsuchiya, K.; Aoki, T.; Watanabe, Y. Appearance of frontal midline theta activity in patients with generalized anxiety disorder. Neuropsychobiology 2000, 41, 108–112. [Google Scholar] [CrossRef]
- Cook, I.A.; Hunter, A.M.; Korb, A.S.; Leuchter, A.F. Do prefrontal midline electrodes provide unique neurophysiologic information in Major Depressive Disorder? J. Psychiatric Res. 2014, 53, 69–75. [Google Scholar] [CrossRef]
- Gold, C.; Fachner, J.; Erkkila, J. Validity and reliability of electroencephalographic frontal alpha asymmetry and frontal midline theta as biomarkers for depression. Scand. J. Psychol. 2013, 54, 118–126. [Google Scholar] [CrossRef]
- Lee, S.M.; Jang, K.I.; Chae, J.H. Electroencephalographic Correlates of Suicidal Ideation in the Theta Band. Clin. EEG Neurosci. 2017, 48, 316–321. [Google Scholar] [CrossRef]
- Stubner, S.; Grohmann, R.; Greil, W.; Zhang, X.; Muller-Oerlinghausen, B.; Bleich, S.; Ruther, E.; Moller, H.J.; Engel, R.; Falkai, P.; et al. Suicidal Ideation and Suicidal Behavior as Rare Adverse Events of Antidepressant Medication: Current Report from the AMSP Multicenter Drug Safety Surveillance Project. Int. J. Neuropsychopharmacol. 2018, 21, 814–821. [Google Scholar] [CrossRef]
- Iosifescu, D.V.; Greenwald, S.; Devlin, P.; Perlis, R.H.; Denninger, J.W.; Alpert, J.E.; Fava, M. Pretreatment frontal EEG and changes in suicidal ideation during SSRI treatment in major depressive disorder. Acta Psychiatr. Scand. 2008, 117, 271–276. [Google Scholar] [CrossRef]
- Sinclair, L.I.; Christmas, D.M.; Hood, S.D.; Potokar, J.P.; Robertson, A.; Isaac, A.; Srivastava, S.; Nutt, D.J.; Davies, S.J. Antidepressant-induced jitteriness/anxiety syndrome: Systematic review. Br. J. Psychiatry 2009, 194, 483–490. [Google Scholar] [CrossRef]
- Hantouche, E.; Angst, J.; Azorin, J.M. Explained factors of suicide attempts in major depression. J. Affect. Disord. 2010, 127, 305–308. [Google Scholar] [CrossRef]
- Montgomery, S.A. Treatment-resistant depression: No panacea, many uncertainties. Adverse effects are a major factor in treatment choice. Prescrire Int. 2011, 20, 128–133. [Google Scholar]
- Olin, B.; Jayewardene, A.K.; Bunker, M.; Moreno, F. Mortality and suicide risk in treatment-resistant depression: An observational study of the long-term impact of intervention. PLoS ONE 2012, 7, e48002. [Google Scholar] [CrossRef]
- Papakostas, G.I.; Petersen, T.; Pava, J.; Masson, E.; Worthington, J.J., 3rd; Alpert, J.E.; Fava, M.; Nierenberg, A.A. Hopelessness and suicidal ideation in outpatients with treatment-resistant depression: Prevalence and impact on treatment outcome. J. Nerv. Ment. Dis. 2003, 191, 444–449. [Google Scholar] [CrossRef]
- Hunter, A.M.; Leuchter, A.F.; Cook, I.A.; Abrams, M. Brain functional changes (QEEG cordance) and worsening suicidal ideation and mood symptoms during antidepressant treatment. Acta Psychiatric Scand. 2010, 122, 461–469. [Google Scholar] [CrossRef]
- Beck, A.T. Cognitive Therapy of Depression; Guilford Press: New York, NY, USA, 1979. [Google Scholar]
- Stange, J.P.; Hamilton, J.L.; Burke, T.A.; Kleiman, E.M.; O’Garro-Moore, J.K.; Seligman, N.D.; Abramson, L.Y.; Alloy, L.B.J.P.R. Negative cognitive styles synergistically predict suicidal ideation in bipolar spectrum disorders: A 3-year prospective study. Psychiatry Res. 2015, 226, 162–168. [Google Scholar] [CrossRef]
- Kleiman, E.M.; Riskind, J.H.; Stange, J.P.; Hamilton, J.L.; Alloy, L.B.J.B.T. Cognitive and interpersonal vulnerability to suicidal ideation: A weakest link approach. Behav. Ther. 2014, 45, 778–790. [Google Scholar] [CrossRef]
- Duan, M.; Wang, L.; Liu, X.; Su, F.; An, L.; Liu, S. Abnormal brain activity in fronto-central regions in mental disorders with suicide: An EEG Study. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2021, 2021, 1035–1038. [Google Scholar] [CrossRef]
- Iznak, A.F.; Iznak, E.V.; Damyanovich, E.V.; Oleichik, I.V. Differences of EEG Frequency and Spatial Parameters in Depressive Female Adolescents With Suicidal Attempts and Non-suicidal Self-injuries. Clin. EEG Neurosci. 2021, 52, 406–413. [Google Scholar] [CrossRef]
- Benschop, L.; Baeken, C.; Vanderhasselt, M.A.; Van de Steen, F.; Van Heeringen, K.; Arns, M. Electroencephalogram Resting State Frequency Power Characteristics of Suicidal Behavior in Female Patients With Major Depressive Disorder. J. Clin. Psychiatry 2019, 80, 18m12661. [Google Scholar] [CrossRef] [PubMed]
- Roh, S.C.; Kim, J.S.; Kim, S.; Kim, Y.; Lee, S.H. Frontal Alpha Asymmetry Moderated by Suicidal Ideation in Patients with Major Depressive Disorder: A Comparison with Healthy Individuals. Clin. Psychopharmacol. Neurosci. 2020, 18, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Barnhofer, T.; Duggan, D.; Crane, C.; Hepburn, S.; Fennell, M.J.; Williams, J.M. Effects of meditation on frontal alpha-asymmetry in previously suicidal individuals. Neuroreport 2007, 18, 709–712. [Google Scholar] [CrossRef] [PubMed]
- Swann, A.C.; Lijffijt, M.; O’Brien, B.; Mathew, S.J. Impulsivity and Suicidal Behavior. Curr. Top Behav. Neurosci. 2020, 47, 179–195. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Chen, X.; Chen, J.; Ai, M.; Gan, Y.; He, J.; Kuang, L. The Association Between Resting State Functional Connectivity and the Trait of Impulsivity and Suicidal Ideation in Young Depressed Patients With Suicide Attempts. Front. Psychiatry 2021, 12, 567976. [Google Scholar] [CrossRef]
- Broyd, S.J.; Demanuele, C.; Debener, S.; Helps, S.K.; James, C.J.; Sonuga-Barke, E.J. Default-mode brain dysfunction in mental disorders: A systematic review. Neurosci. Biobehav. Rev. 2009, 33, 279–296. [Google Scholar] [CrossRef]
- Raichle, M.E.; MacLeod, A.M.; Snyder, A.Z.; Powers, W.J.; Gusnard, D.A.; Shulman, G.L. A default mode of brain function. Proc. Natl. Acad. Sci. USA 2001, 98, 676–682. [Google Scholar] [CrossRef]
- Meerwijk, E.L.; Chesla, C.A.; Weiss, S.J. Psychological pain and reduced resting-state heart rate variability in adults with a history of depression. Psychophysiology 2014, 51, 247–256. [Google Scholar] [CrossRef]
- Aldao, A.; Nolen-Hoeksema, S.; Schweizer, S. Emotion-regulation strategies across psychopathology: A meta-analytic review. Clin. Psychol. Rev. 2010, 30, 217–237. [Google Scholar] [CrossRef] [PubMed]
- Webb, T.L.; Miles, E.; Sheeran, P. Dealing with feeling: A meta-analysis of the effectiveness of strategies derived from the process model of emotion regulation. Psychol. Bull. 2012, 138, 775–808. [Google Scholar] [CrossRef] [PubMed]
- Sarkinaite, M.; Gleizniene, R.; Adomaitiene, V.; Dambrauskiene, K.; Raskauskiene, N.; Steibliene, V. Volumetric MRI Analysis of Brain Structures in Patients with History of First and Repeated Suicide Attempts: A Cross Sectional Study. Diagnostics 2021, 11, 488. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, K.; Nemoto, K.; Shiratori, Y.; Sodeyama, N.; Kodama, K.; Usuniwa, H.; Yamada, N.; Yaguchi, C.; Hori, T.; Arai, T.; et al. Aberrant resting-state functional connectivity of major depressive disorder with higher risk of suicide. Psychiatry Clin. Neurosci. Rep. 2022, 1, e35. [Google Scholar] [CrossRef]
- Harmon-Jones, E.; Allen, J.J. Anger and frontal brain activity: EEG asymmetry consistent with approach motivation despite negative affective valence. J. Pers. Soc. Psychol. 1998, 74, 1310–1316. [Google Scholar] [CrossRef]
- Dillon, K.H.; Van Voorhees, E.E.; Elbogen, E.B. Associations between anger and suicidal ideation and attempts: A prospective study using the National Epidemiologic Survey on Alcohol and Related Conditions. J. Psychiatric Res. 2020, 122, 17–21. [Google Scholar] [CrossRef]
- Peterson, C.K.; Shackman, A.J.; Harmon-Jones, E. The role of asymmetrical frontal cortical activity in aggression. Psychophysiology 2008, 45, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Miller, N.S.; Mahler, J.C.; Gold, M.S. Suicide risk associated with drug and alcohol dependence. J. Addict. Dis. 1991, 10, 49–61. [Google Scholar] [CrossRef]
- Schneider, B. Substance use disorders and risk for completed suicide. Arch. Suicide Res. Off. J. Int. Acad. Suicide Res. 2009, 13, 303–316. [Google Scholar] [CrossRef]
- Li, D.; Yang, X.; Ge, Z.; Hao, Y.; Wang, Q.; Liu, F.; Gu, D.; Huang, J. Cigarette smoking and risk of completed suicide: A meta-analysis of prospective cohort studies. J. Psychiatric Res. 2012, 46, 1257–1266. [Google Scholar] [CrossRef]
- Li, K.; Zhou, G.; Xiao, Y.; Gu, J.; Chen, Q.; Xie, S.; Wu, J. Risk of Suicidal Behaviors and Antidepressant Exposure Among Children and Adolescents: A Meta-Analysis of Observational Studies. Front. Psychiatry 2022, 13, 880496. [Google Scholar] [CrossRef] [PubMed]
- Hengartner, M.P.; Amendola, S.; Kaminski, J.A.; Kindler, S.; Bschor, T.; Plöderl, M. Suicide risk with selective serotonin reuptake inhibitors and other new-generation antidepressants in adults: A systematic review and meta-analysis of observational studies. J. Epidemiol. Community Health 2021. [Google Scholar] [CrossRef] [PubMed]
- van Heeringen, K.; Wu, G.R.; Vervaet, M.; Vanderhasselt, M.A.; Baeken, C. Decreased resting state metabolic activity in frontopolar and parietal brain regions is associated with suicide plans in depressed individuals. J. Psychiatr. Res. 2017, 84, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Campos, A.I.; Van Velzen, L.S.; Veltman, D.J.; Pozzi, E.; Ambrogi, S.; Ballard, E.D.; Banaj, N.; Basgoze, Z.; Bellow, S.; Benedetti, F.; et al. Concurrent validity and reliability of suicide risk assessment instruments: A meta-analysis of 20 instruments across 27 international cohorts. Neuropsychology 2023, 37, 315–329. [Google Scholar] [CrossRef] [PubMed]
- Miller, P.R.; Dasher, R.; Collins, R.; Griffiths, P.; Brown, F. Inpatient diagnostic assessments: 1. Accuracy of structured vs. unstructured interviews. Psychiatry Res. 2001, 105, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Ceballos, N.A.; Bauer, L.O.; Houston, R.J. Recent EEG and ERP findings in substance abusers. Clin. EEG Neurosci. 2009, 40, 122–128. [Google Scholar] [CrossRef]
- Saletu, B.; Grunberger, J.; Rajna, P. Pharmaco-EEG profiles of antidepressants. Pharmacodynamic studies with fluvoxamine. Br. J. Clin. Pharmacol. 1983, 15 (Suppl. S3), S369–S383. [Google Scholar] [CrossRef]
- Reeves, R.R.; Ladner, M.E. Antidepressant-induced suicidality: An update. CNS Neurosci. Ther. 2010, 16, 227–234. [Google Scholar] [CrossRef]
- Jang, K.I.; Lee, S.; Lee, S.H.; Chae, J.H. Frontal Alpha Asymmetry, Heart Rate Variability, and Positive Resources in Bereaved Family Members with Suicidal Ideation after the Sewol Ferry Disaster. Psychiatry Investig. 2018, 15, 1168–1173. [Google Scholar] [CrossRef]
- van Heeringen, K. Stress-Diathesis Model of Suicidal Behavior. In The Neurobiological Basis of Suicide; Dwivedi, Y., Ed.; Frontiers in Neuroscience: Boca Raton, FL, USA, 2012. [Google Scholar]
- Diago, M.; Vila-Badia, R.; Serra-Arumí, C.; Butjosa, A.; Del Cacho, N.; Esteban Sanjusto, M.; Colomer-Salvans, A.; Sánchez, L.; Dolz, M.; Muñoz-Samons, D.; et al. Emotional abuse and perceived stress: The most relevant factors in suicide behavior in first-episode psychosis patients. Psychiatry Res. 2022, 315, 114699. [Google Scholar] [CrossRef]
- Bahk, Y.C.; Jang, S.K.; Choi, K.H.; Lee, S.H. The Relationship between Childhood Trauma and Suicidal Ideation: Role of Maltreatment and Potential Mediators. Psychiatry Investig. 2017, 14, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Pérez-González, A.; Pereda, N. Systematic review of the prevalence of suicidal ideation and behavior in minors who have been sexually abused. Actas Esp. Psiquiatr. 2015, 43, 149–158. [Google Scholar] [PubMed]
- Lopez-Castroman, J.; Melhem, N.; Birmaher, B.; Greenhill, L.; Kolko, D.; Stanley, B.; Zelazny, J.; Brodsky, B.; Garcia-Nieto, R.; Burke, A.K.; et al. Early childhood sexual abuse increases suicidal intent. World Psychiatry 2013, 12, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Ng, Q.X.; Yong, B.Z.J.; Ho, C.Y.X.; Lim, D.Y.; Yeo, W.S. Early life sexual abuse is associated with increased suicide attempts: An update meta-analysis. J. Psychiatr. Res. 2018, 99, 129–141. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.T.; Chesin, M.; Fertuck, E.; Keilp, J.; Brodsky, B.; Mann, J.J.; Sonmez, C.C.; Benjamin-Phillips, C.; Stanley, B. Heart rate variability and suicidal behavior. Psychiatry Res. 2016, 240, 241–247. [Google Scholar] [CrossRef]


{kind=link}
| Study | Population | Methods | Design | Results |
|---|---|---|---|---|
| [27] | Female suicide attempters (SA = 16) and matched healthy participants (HC = 22). | Eyes open and eyes closed | Mixed design. Between group cross-sectional analysis and within-subject design | 1. The HC group had greater alpha power in the right hemisphere, whereas suicidal adolescents had no asymmetry in the opposite direction. 2. Alpha asymmetry over posterior regions correlated with ratings of SI but not depression severity. |
| [33] | Patients with higher (SSI = 33) and a lower score (SSI = 57) of suicide ideation. | Eyes closed | Mixed design. Between group cross-sectional analysis and within-subject design | 1. Theta absolute and relative power in all channels was positively correlated with SSI, except Fp1, F7 and F8. 2. The high SSI group had higher theta relative power at F3, Fz, FCz, and Cz, when compared to the low SSI group. 3. Fronto-central theta relative power was greater in the high SSI group when compared to the low SSI group. 4. The SSI score was the most powerful predictor of fronto-central theta power. |
| [45] | Patients with a history of suicide attempt (SA = 14), no history of suicide attempt (NSA = 14), and healthy controls (HC = 14). | Eyes closed and eyes open | Between group cross-sectional analysis | 1. The SA group had higher absolute delta, beta and gamma power when compared to the NSA and HC groups. 2. Fronto-central synchronization between beta and gamma power was weaker in the SA when compared to the NSA group. |
| [46] | Female adolescents with solely non-suicidal self-injuries (NSSI = 21), and with combined NSSI + history of suicide attempt (NSSI + SA = 24) | Eyes closed | Mixed design. Between group cross-sectional analysis and within-subject design | 1. In the NSSI + SA group, the parieto–occipital power of alpha-2 (9–11 Hz) was higher and its focus was localized in the right hemisphere. 2. In the NSSI + SA group, alpha-3 (11–13 Hz) spectral power was higher than alpha-1 (8–9 Hz). 3. In the NSSI group, alpha-1 power was higher than alpha-3, 4. In the NSSI group, the foci of alpha-2 and alpha-3 were localized in the left hemisphere. 5. EEG coherence was higher in the NSSI + SA group, especially in fronto–central–parietal regions. |
| [47] | Female MDD patients with SA, only SI and no SI or SA (SI = 36; SA = 19; non-suicidal = 23) | Eyes open and eyes closed | Between group cross-sectional analysis | 1. When compared with the non-suicidal group, the SI and SA groups had lower beta and low gamma activity in the frontal regions. 2. The SI group had increased alpha power over the posterior regions as well as increased high beta and lower gamma activity over the left occipital region when compared to the non-suicidal group. 3. The SA group had lower beta and gamma power over the right temporal region when compared to the SI group. 4. When compared with the non-suicidal group, the SI and SA groups had lower frontal activity within the orbito-, medial-, middle-, superior-, and inferior-frontal areas and the anterior cingulate cortex. 5. When compared with the non-suicidal group, the SA group had reduced right temporal activity within the right inferior-, middle-, and superior-temporal cortices and the fusiform gyrus. |
| [48] | Patients with major depressive disorder (MDD) with and without suicide ideation (SI), and HC (MDD = 44; MDD + SI = 23; HC = 60) | Eyes open | Mixed design. Between group cross-sectional analysis and within-subject design | 1. Frontal alpha asymmetry (FAA) (reduced alpha power in the left frontal region) was lower in the MDD + SI group when compared with the MDD group. 2. Depression and anxiety symptoms were correlated with FAA only in the MDD + SI group. 3. SI moderated the effects of depressive symptom on FAA in the MDD group. |
| [49] | Patients with a history of suicidal depression before mindfulness-based cognitive therapy (MBCT = 10) or treatment-as-usual (TAU = 12). | Eyes open and eyes closed | Mixed design. Between group cross-sectional analysis and within-subject design | After, treatment, the TAU group showed increased prefrontal alpha asymmetry associated with a decrease in positive affective style; there was no change in the MBCT group. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amico, F.; Frye, R.E.; Shannon, S.; Rondeau, S. Resting State EEG Correlates of Suicide Ideation and Suicide Attempt. J. Pers. Med. 2023, 13, 884. https://doi.org/10.3390/jpm13060884
Amico F, Frye RE, Shannon S, Rondeau S. Resting State EEG Correlates of Suicide Ideation and Suicide Attempt. Journal of Personalized Medicine. 2023; 13(6):884. https://doi.org/10.3390/jpm13060884
Chicago/Turabian StyleAmico, Francesco, Richard E. Frye, Scott Shannon, and Steve Rondeau. 2023. "Resting State EEG Correlates of Suicide Ideation and Suicide Attempt" Journal of Personalized Medicine 13, no. 6: 884. https://doi.org/10.3390/jpm13060884
APA StyleAmico, F., Frye, R. E., Shannon, S., & Rondeau, S. (2023). Resting State EEG Correlates of Suicide Ideation and Suicide Attempt. Journal of Personalized Medicine, 13(6), 884. https://doi.org/10.3390/jpm13060884