Abstract
Background: Myocardial perfusion imaging via single-photon emission computed tomography (SPECT MPI) is a well-established method of diagnosing coronary artery disease (CAD). The purpose of this study was to assess the role of SPECT MPI in predicting major cardiovascular events. Methods: The study population was composed of 614 consecutive patients (mean age: 67 years, 55% male) referred for SPECT MPI due to symptoms of stable CAD. The SPECT MPI was performed using a single-day protocol. We conducted a follow-up on all patients at 12 months via a telephone interview. Results: The majority of our patients (78%) presented findings suggestive of reversible ischemia, fixed defects or both. Extensive perfusion defects were found in 18% of the population, while LV dilation was found in 7%. During the 12-month follow-up, 16 deaths, 8 non-fatal MIs and 20 non-fatal strokes were recorded. There was no significant association of SPECT findings with the combined endpoint of all-cause death, non-fatal MI and non-fatal stroke. The presence of extensive perfusion defects was an independent predictor of mortality at 12 months (HR: 2.90, 95% CI: 1.05, 8.06, p = 0.041). Conclusions: In a high-risk patient population with suspected stable CAD, only large reversible perfusion defects in SPECT MPI were independently associated with mortality at 1 year. Further trials are needed to validate our findings and refine the role of SPECT MPI findings in the diagnosis and prognosis of cardiovascular patients.
1. Introduction
Cardiovascular disease (CVD) is the leading cause of death in the western world, and coronary artery disease (CAD) is the most common form of CVD [1]. Patients with symptoms suggestive of CAD undergo a series of evaluations based on their relevant risk, ultimately assessing the need for invasive coronary angiography and the need for treatment. Diagnostic methods for coronary artery disease provide information both on the presence of angiographically significant CAD and also on the clinical prognosis of patients (i.e., mortality, non-fatal myocardial infarction, angina, etc.) [2].
Myocardial perfusion imaging (MPI) via single-photon emission computed tomography (SPECT) is a well-established nuclear cardiology method used to assess the coronary artery blood supply of the left ventricle. Performed in conjunction with a stress test (physical or pharmacological), SPECT MPI is a valuable imaging modality used to diagnose CAD, allowing for the evaluation of the extent and severity of CAD as assessed via coronary angiography [3]. The diagnostic performance of SPECT MPI has been extensively studied, with considerable heterogeneity in the estimated accuracy among studies [4]. Whether SPECT MPI findings may further improve patient risk stratification and determine the occurrence of major clinical events is still a matter of debate [3,5].
The aim of the current single-center study was to evaluate the prognostic role of SPECT MPI, in terms of predicting mortality and other major cardiovascular events at 1 year, in symptomatic patients assessed for suspected stable CAD in the modern era.
2. Patients and Methods
2.1. Study Population
The study population consisted of 614 patients referred for SPECT MPI in the Nuclear Medicine Department of a tertiary hospital over a year (1 January to 31 December 2017) due to symptoms (i.e., chest pain (CCS class I or II) or dyspnea (NYHA class I-III)) suggestive of suspected stable CAD. Patients who needed a revascularization procedure according to the MPI study results were retrospectively excluded from our analysis. A revascularization procedure based on the reference SPECT MPI study results may have an important impact on the prognosis of the patients and would complicate the association of SPECT MPI findings with the clinical outcomes. Other exclusion criteria were: a recent myocardial infarction (MI) in the last month before the test or a coronary revascularization procedure (percutaneous coronary intervention or coronary artery bypass graft) in the last two months.
2.2. Study Protocol
On the day of the test, every patient was interviewed to enable us to record all the data relevant to their cardiovascular history. This information involved cardiac-related symptoms, risk factors for CAD (smoking habits, hypertension, diabetes mellitus, dyslipidemia, obesity, family history of CAD) and a previous history of any diagnosed CVD and its management. The study protocol and the SPECT MPI procedure were explained in detail to the patients, who gave their written informed consent to participate. The study was compliant with the principles of the Helsinki Declaration and with local legislation, and was approved by the Scientific Council and Ethical Committee of the hospital.
We conducted a follow-up on all patients enrolled in the study at 12 months after the SPECT MPI via a telephone interview. The patients—or their next of kin—were asked in detail about the occurrence of clinical events of importance in the time interval since their enrollment in the study. In case a major cardiovascular event was reported, the findings were confirmed via review of the corresponding medical records. The primary endpoint of the study was the composite of all-cause mortality, nonfatal MI and nonfatal stroke. MI and stroke were defined according to the clinical criteria of hospitalization, biochemical blood tests, electrocardiography and brain imaging.
2.3. Myocardial Perfusion Imaging Protocol
The same data acquisition parameters were used in all patients. SPECT MPI was performed according to the guidelines of the European Association of Nuclear Medicine and Molecular Imaging (EANMMI) [6]. The single-day protocol was used, with stress and rest images acquired in that particular order, approximately two hours apart. Patients fasted for at least four hours before the exam and abstained from methyl-xanthine beverages and caffeine for 24 h, in order to be prepared to undergo vasodilative stress with dipyridamole, if needed. Discontinuation of medications containing nitrates, calcium channel antagonists and beta-blockers was also applied for 24 h before the test.
Maximal or symptom-limited treadmill exercise (Bruce protocol) was selected for those patients who were capable of completing this type of stress test. Intravenous pharmacological stress was applied to patients with limited physical tolerance or with contraindications for treadmill exercise. In those patients, the vasodilative substance dipyridamole (0.56 mg/kg body weight) was mostly used, either alone or in combination with a single-stage 3 min Bruce treadmill exercise. In a small proportion of patients who were ineligible to receive dipyridamole, an inotropic pharmacological stress was carried out with the IV infusion of dobutamine. All studies were performed with Technetium Tc 99m tetrofosmin (TF) (Myoview, GE Healthcare AS, Oslo, Norway), an MPI radiopharmaceutical that was labeled in-house according to the manufacturer’s instructions.
2.4. Visual Analysis of Myocardial Perfusion
The recorded raw tomographic data under stress and rest were processed and reconstructed in the three planes (short axis, horizontal long axis and vertical long axis) according to established algorithms, and assessed by two experienced board-certified nuclear medicine physicians. The readers were not blinded to the clinical information and reported jointly to reach an agreement according to routine clinical reporting protocols; possible discrepancies were resolved via consensus. A perfusion study was interpreted visually as normal when bearing no or only borderline equivocal findings. The presence of reversible perfusion deficits was characterized as ischemia, while fixed (irreversible) deficits corresponded either to myocardial necrosis (scar) or to a gravely ischemic (hibernating) myocardium. Finally, studies with coexisting ischemia and irreversible deficits were characterized as having mixed deficits. Further evaluation of each SPECT study involved the estimation of the extent of abnormal left ventricular perfusion by the number of involved myocardial segments, graded on a 3-point scale as: absent or negligible (<1 segment or <5% of the left ventricular myocardium), small to medium (1–4 segments or 5–20% left ventricular myocardium) or large (≥5 segments or >20% left ventricular myocardium) [7].
2.5. Statistical Analysis
Continuous data are presented as mean values ± standard deviation, while dichotomous data are presented as numbers (percentage). The association of SPECT MPI findings, as well other clinical parameters, with clinical outcomes was assessed using Cox’s Regression analysis, and Hazard Ratio (HR) estimates (95% confidence interval) were calculated. In multivariate analysis, only the predictive role of SPECT features with a significant univariate association with clinical outcomes was assessed. Receiver–Operator Curve analysis was used to assess the prognostic value of perfusion defects for mortality. A two-tailed p value < 0.05 was used to determine significant associations. All analyses were performed using the software IBM SPSS Statistics version 21 (IBM, Armonk, NY, USA).
3. Results
The mean age of the population was 67 years, and most patients were male (55%). The prevalence of established cardiovascular risk factors is shown in Table 1. A history of CAD was present in 34% of our patients. Patients were referred for a SPECT MPI test due to chest pain (62%) and/or dyspnea (76%). The majority of our patients (78%) presented findings in the SPECT study that were suggestive of reversible ischemia, fixed defects or both. Extensive perfusion defects were found in 18% of the patients, while left ventricular dilation was found in only 7% of the population. Based on the SPECT results and the clinical findings, 307 (50%) patients were referred for invasive coronary angiography. The finding of extensive perfusion defects was associated with the presence of significant CAD in coronary angiography (r = 0.136, p = 0.017).

Table 1.
Descriptive characteristics of enrolled patients and results of myocardial perfusion imaging SPECT study.
During the 12-month follow-up, 16 deaths (2.6%), 8 non-fatal MIs (1.3%) and 20 non-fatal strokes (3.3%) occurred. Of the patients who died, 50% had undergone a coronary angiogram; none of them had significant coronary artery disease. There was no significant association of SPECT findings with the primary endpoint (combined endpoint of all-cause death, non-fatal MI and non-fatal stroke) (Table 2).
Table 2.
Univariate associations of SPECT MPI findings with clinical outcomes at 12-month follow-up.
The presence of extensive perfusion defects and transient left ventricular dilation was significantly associated with mortality at the 12-month follow-up (Table 2 and Figure 1). After adjustment for confounders, only the presence of extensive perfusion defects remained an independent predictor of mortality at 12 months (Table 3). In the ROC analysis, the presence of large perfusion defects was associated with 1-year mortality with an AUC of 0.632, p = 0.072.
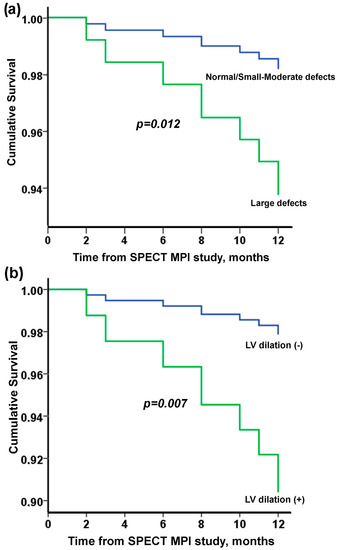
Figure 1.
Cumulative survival (Kaplan–Meier curves) according to SPECT MPI study findings: (a) extent of defects and (b) presence of LV dilation.
Table 3.
Associations of various studied parameters with all-cause mortality at 12-month follow-up.
4. Discussion
Our study involved a very high-risk cohort of consecutive symptomatic patients evaluated for suspected CAD, with almost one third of them having a history of CAD. The study patients were extensively treated with statins, antithrombotic medications and other established modern therapies for CVD. In this group of patients, we recorded a relatively high incidence of major adverse cardiovascular events and deaths (4.6% and 2.6%, respectively, at 1 year; this appears to be higher compared to some studies [8,9], although similar results have recently been reported in other studies in similar populations [10]. In the current study, the SPECT MPI findings were not found to be associated with the combined endpoint of death/non-fatal MI or stroke during a 12-month follow-up. However, a significant association of specific SPECT MPI findings (i.e., large ischemic defects and left ventricular dilatation) with all-cause mortality at 12 months was shown. After adjusting for confounders, only large ischemic defects were found to have an independent association with all-cause mortality; patients with large reversible deficits in the SPECT MPI had a ca. three times higher risk of death at 1 year compared to patients with smaller reversible deficits or no deficits.
Myocardial scintigraphy is an important tool for diagnosing CAD, and its combination with other clinical features has been suggested to lead to the more accurate stratification of prognoses and the determination of subsequent treatment policies [11]. Various recent studies have reported a significant, and probably independent, prognostic role of an abnormal SPECT MPI test in different populations, i.e., patients with diabetes mellitus, chronic kidney disease or suspected CAD, irrespective of the presence of obstructive CAD following angiography [12,13,14,15,16]. In these populations, the presence of a normal SPECT MPI study was associated with a lower occurrence of cardiovascular events. In the current study, only the presence of extensive ischemia was found to be related to all-cause mortality, but not to the occurrence of the combined endpoint (death, MI and stroke). The discordant associations observed among various studies may be attributed to differences in design and population characteristics, in the definitions of the endpoints of interest, as well as in the follow-up duration among studies.
Furthermore, it should be noted that different findings of the SPECT MPI study may provide important information for different outcomes. Besides the established role of fixed and reversible perfusion deficits in the diagnosis of suspected CAD, other findings, such as transient left ventricular dilatation and the presence of large reversible perfusion defects, may offer important prognostic information in terms of clinical events, and most importantly, mortality. Indeed, it has previously been shown that specific thresholds of the extent of SPECT MPI-detected ischemia may have a significant independent prognostic role, and thus, may lead to an improvement in the risk stratification of patients with suspected CAD and potential refinement of treatment in these patients [10,17,18,19]. The presence of transient left ventricular dilation has been associated with the diagnosis of extensive, severe CAD and poor prognosis [20]. In the absence of significant CAD, it may be a sign of severe dysfunction of the coronary microcirculation [21,22].
5. Limitations
The study was performed in a tertiary care hospital and reflects the practice settings of a single center in a specific cohort of patients, so generalizability may be limited. The exact cause of mortality was not always easy to define; thus, all-cause mortality was chosen as a clinical outcome instead of cardiovascular or other forms of cause-specific mortality. Although the SPECT MPI interpretation was performed by experienced readers, it only involved qualitative visual assessment of the left ventricular perfusion that was applied routinely in the day-to-day clinical reporting practice of this medical center.
6. Conclusions
In conclusion, in this contemporary cohort of a high-risk patient population (treated with modern treatment modalities as suggested by the guidelines) with symptoms suggestive of CAD, SPECT MPI findings of large reversible defects were independently associated with increased mortality 1 year after the study. Several aspects of the SPECT MPI study should be taken into account, not only for CAD diagnosis, but also for its prognosis in various populations. Further trials are needed to validate our findings and refine the role of SPECT MPI findings in the diagnosis and prognosis of cardiovascular patients.
Author Contributions
Conceptualization, P.Z., K.K.N., L.K.M. and A.F.; data curation, P.Z., A.B., S.T., X.X., K.P., L.L., A.R. and J.K.-E.; formal analysis, P.Z., A.B., K.K.N., S.T. and A.R.; investigation, P.Z., K.K.N., J.K.-E., L.K.M. and A.F.; methodology, P.Z., S.T., X.X., K.P., L.L., J.K.-E. and A.F.; supervision, K.K.N., L.K.M. and A.F.; writing—original draft, P.Z., A.B., S.T., K.K.N., L.K.M. and A.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of the University Hospital of Ioannina (1123/20-12-2016).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available from the authors upon request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Townsend, N.; Wilson, L.; Bhatnagar, P.; Wickramasinghe, K.; Rayner, M.; Nichols, M. Cardiovascular disease in Europe: Epidemiological update 2016. Eur. Heart J. 2016, 37, 3232–3245. [Google Scholar] [CrossRef]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Shah, B.N.; Khattar, R.S.; Senior, R. The hibernating myocardium: Current concepts, diagnostic dilemmas, and clinical challenges in the post-STICH era. Eur. Heart J. 2013, 34, 1323–1336. [Google Scholar] [CrossRef] [PubMed]
- Medical Advisory Secretariat. Single photon emission computed tomography for the diagnosis of coronary artery disease: An evidence-based analysis. Ont. Health Technol. Assess Ser. 2010, 10, 1–64. [Google Scholar]
- Abdel Fattah, A.; Kamal, A.M.; Pancholy, S.; Ghods, M.; Russell, J.; Cassel, D.; Wasserleben, V.; Heo, J.; Iskandrian, A.S. Prognostic implications of normal exercise tomographic thallium images in patients with angiographic evidence of significant coronary artery disease. Am. J. Cardiol. 1994, 74, 769–771. [Google Scholar] [CrossRef] [PubMed]
- Verberne, H.J.; Acampa, W.; Anagnostopoulos, C.; Ballinger, J.; Bengel, F.; De Bondt, P.; Buechel, R.R.; Cuocolo, A.; van Eck-Smit, B.L.F.; Flotats, A.; et al. EANM procedural guidelines for radionuclide myocardial perfusion imaging with SPECT and SPECT/CT: 2015 revision. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1929–1940. [Google Scholar] [CrossRef]
- Tilkemeier, P.L.; Bourque, J.; Doukky, R.; Sanghani, R.; Weinberg, R.L. ASNC imaging guidelines for nuclear cardiology procedures: Standardized reporting of nuclear cardiology procedures. J. Nucl. Cardiol. 2017, 24, 2064–2128. [Google Scholar] [CrossRef]
- Betancur, J.; Otaki, Y.; Motwani, M.; Fish, M.B.; Lemley, M.; Dey, D.; Gransar, H.; Tamarappoo, B.; Germano, G.; Sharir, T.; et al. Prognostic Value of Combined Clinical and Myocardial Perfusion Imaging Data Using Machine Learning. JACC Cardiovasc. Imaging 2018, 11, 1000–1009. [Google Scholar] [CrossRef]
- Otaki, Y.; Betancur, J.; Sharir, T.; Hu, L.H.; Gransar, H.; Liang, J.X.; Azadani, P.N.; Einstein, A.J.; Fish, M.B.; Ruddy, T.D.; et al. 5-Year Prognostic Value of Quantitative Versus Visual MPI in Subtle Perfusion Defects: Results from REFINE SPECT. JACC Cardiovasc. Imaging 2020, 13, 774–785. [Google Scholar] [CrossRef]
- Kato, T.; Momose, M.; Uemura, Y.; Naya, M.; Matsumoto, N.; Hida, S.; Yamauchi, T.; Nakajima, T.; Suzuki, E.; Inoko, M.; et al. Association of the extent of myocardial ischemia with outcomes in patients with suspected coronary artery disease in Japan. J. Cardiol. 2022, 80, 475–481. [Google Scholar] [CrossRef]
- Sakatani, T.; Nakajima, K.; Nishimura, T. Cardiovascular event risk estimated by myocardial perfusion SPECT combined with clinical data. J. Cardiol. 2021, 80, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Abdu, F.A.; Yin, G.; Xu, B.; Mohammed, A.-Q.; Xu, S.; Lv, X.; Luo, Y.; Zu, L.; Yang, C.; et al. Prognostic value of myocardial perfusion imaging with D-SPECT camera in patients with ischemia and no obstructive coronary artery disease (INOCA). J. Nucl. Cardiol. 2020, 28, 3025–3037. [Google Scholar] [CrossRef] [PubMed]
- Javaid, A.; Ahmed, A.I.; Han, Y.; Al Rifai, M.; Saad, J.M.; Alfawara, M.S.; Alahdab, F.; El Nihum, L.; Jimenez, Y.; Newstorm, E.; et al. Incremental prognostic value of spect over CCTA. Int. J. Cardiol. 2022, 358, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Caobelli, F.; Haaf, P.; Haenny, G.; Pfisterer, M.; Zellweger, M.J. Prognostic value of myocardial perfusion scintigraphy in asymptomatic patients with diabetes mellitus at high cardiovascular risk: 5-year follow-up of the prospective multicenter BARDOT trial. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 3512–3521. [Google Scholar] [CrossRef] [PubMed]
- Cantoni, V.; Green, R.; Acampa, W.; Assante, R.; Zampella, E.; Nappi, C.; Gaudieri, V.; Mannarino, T.; D’Antonio, A.; Petretta, M.; et al. Prognostic value of myocardial perfusion imaging in patients with chronic kidney disease: A systematic review and meta-analysis. J. Nucl. Cardiol. 2022, 29, 141–154. [Google Scholar] [CrossRef]
- Djaileb, L.; Seiller, A.; Canu, M.; De Leiris, N.; Martin, A.; Poujol, J.; Fraguas-Rubio, A.; Leenhardt, J.; Carabelli, A.; Calizzano, A.; et al. Prognostic value of SPECT myocardial perfusion entropy in high-risk type 2 diabetic patients. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1813–1821. [Google Scholar] [CrossRef]
- Hachamovitch, R.; Hayes, S.W.; Friedman, J.D.; Cohen, I.; Berman, D.S. A prognostic score for pre-diction of cardiac mortality risk after adenosine stress myocardial perfusion scintigraphy. J. Am. Coll. Cardiol. 2005, 45, 722–729. [Google Scholar] [CrossRef]
- Chan, H.P.; Chang, C.C.; Hu, C.; Wang, W.H.; Peng, N.J.; Tyan, Y.C.; Yang, M.H. The Evaluation of Left Ventricle Ischemic Extent in Patients with Significantly Suspicious Cardiovascular Disease by (99m)Tc-Sestamibi Dynamic SPECT/CT and Myocardial Perfusion Imaging: A Head-to-Head Comparison. Diagnostics 2021, 11, 1101. [Google Scholar] [CrossRef]
- Georgiopoulos, G.; Mavraganis, G.; Aimo, A.; Giorgetti, A.; Cavaleri, S.; Fabiani, I.; Giannoni, A.; Emdin, M.; Gimelli, A. Sex-specific associations of myocardial perfusion imaging with outcomes in patients with suspected chronic coronary syndrome. Hellenic J. Cardiol. 2022. [Google Scholar] [CrossRef]
- Alama, M.; Labos, C.; Emery, H.; Iwanochko, R.M.; Freeman, M.; Husain, M.; Lee, D.S. Diagnostic and prognostic significance of transient ischemic dilation (TID) in myocardial perfusion imaging: A systematic review and meta-analysis. J. Nucl. Cardiol. 2018, 25, 724–737. [Google Scholar] [CrossRef]
- Emmett, L.; Ng, A.; Ha, L.; Russo, R.; Mansberg, R.; Zhao, W.; Chow, S.V.; Kritharides, L. Comparative assessment of rest and post-stress left ventricular volumes and left ventricular ejection fraction on gated myocardial perfusion imaging (MPI) and echocardiography in patients with transient ischaemic dilation on adenosine MPI: Myocardial stunning or subendocardial hypoperfusion? J. Nucl. Cardiol. 2012, 19, 735–742. [Google Scholar] [PubMed]
- Chen, L.; Zhang, M.; Jiang, J.; Lei, B.; Sun, X. Coronary microvascular dysfunction: An important interpretation on the clinical significance of transient ischemic dilation of the left ventricle on myocardial perfusion imaging. J. X-Ray Sci. Technol. 2021, 29, 347–360. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).