
Mapping the Heartbeat of America with ChatGPT-4: Unpacking the Interplay of Social Vulnerability, Digital Literacy, and Cardiovascular Mortality in County Residency Choices


Abstract
:1. Introduction
- Evaluate if SVI and DL can significantly predict cardiovascular mortality for the general US population living in various states.
- Evaluate the utility of AI tools, specifically ChatGPT, to predict cardiovascular mortality rates for different geographic locations.
2. Materials and Methods
2.1. Data Files and Merging
2.2. Selection of ChatGPT-4 and Python Integration
2.2.1. Important Consideration of Integration
Use of ChatGPT as a Beta Feature
2.2.2. Python Package
2.3. Data Integrity Assessment and Main Analytic Steps
2.4. Dependent Variables
2.4.1. Calculation of DL Measure
- No internet percentage [32] = Percent of households without internet in the county (B28002_013E: households without an internet subscription/B28002_001E: Total households) × 100;
- No education percentage = Percent of households without education (B15003_002E: no schooling completed [33]/B15003_001E: total population 25 years and over) × 100;
- Digital literacy DL = (100 − [‘No_Education_Percentage’]) × (100 − [‘No_Internet_Percentage’]). [Note—No educational attainment variable was derived from the American Survey [34] question “What is the highest degree or level of school this person has completed?” This is tabulated as B15003-002E in the data file. We adjusted the denominator to account for the overestimation of those without formal education.]
2.4.2. Justification of DL Measure
2.4.3. How Literacy Contributes to DL
- Cognitive abilities: education equips individuals with the cognitive tools to comprehend, adapt to, and utilize new technologies [38];
- Access to resources: schools and colleges often provide computer labs, internet facilities, and formal information and communications technology (ICT) courses, giving students exposure and opportunities to become digitally literate [39]; Instructional experience: the structured curriculum in educational settings often includes components of DL, either embedded within subjects or as standalone courses [40]
2.5. Regression Model for Age-Adjusted Mortality for 2020 (Model 2)
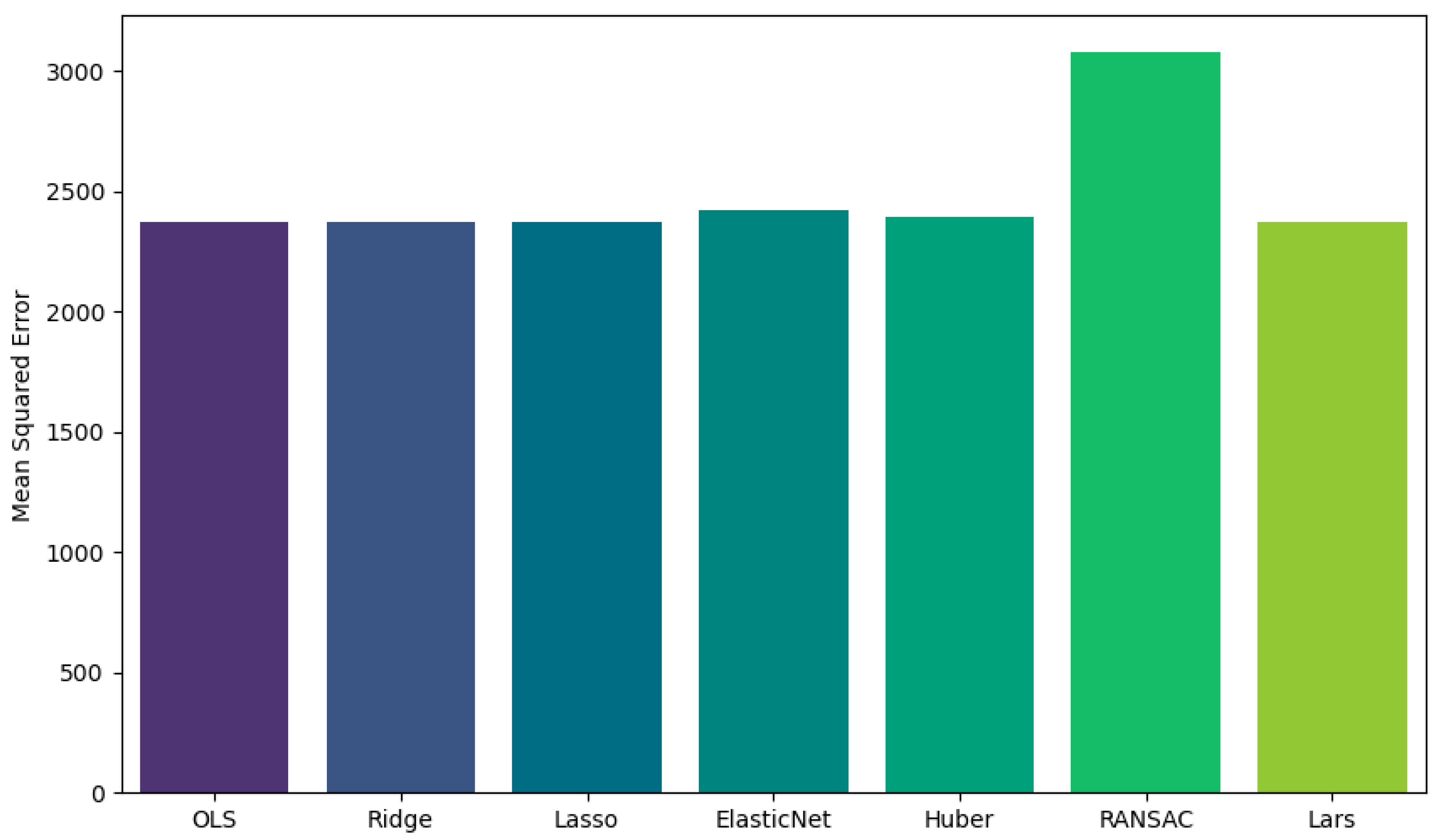
2.6. Assessing Best Regression Model Using Mean Squared Error as the ‘Loss Function’ (Lower Value Better) for Model 2
2.7. Machine-Learning Steps for Age-Adjusted Mortality for the Year 2020
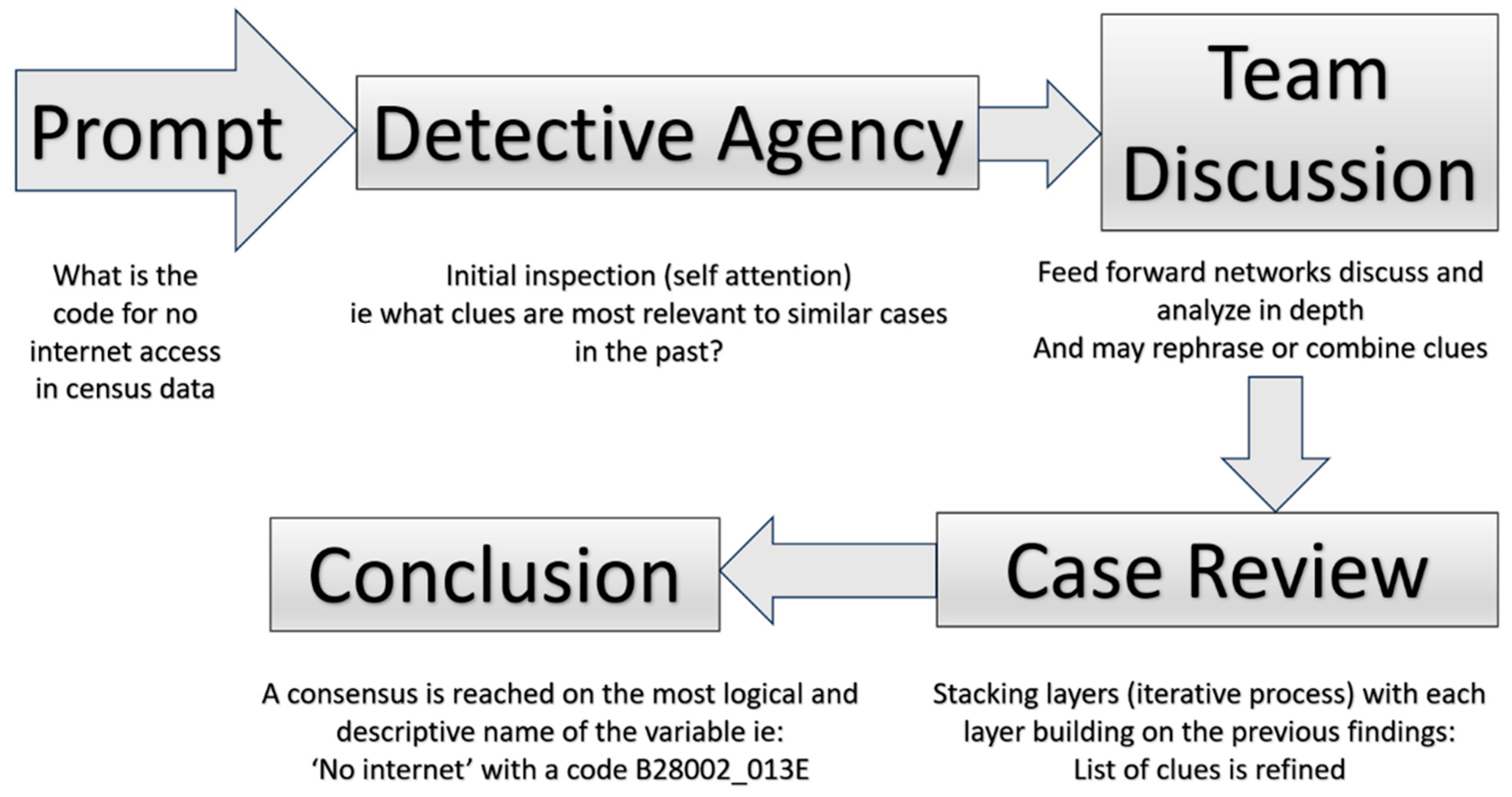
2.8. Large Language Model—Chat GPT4 as a Detective Agency
The Detective’s Context
3. Results
3.1. Rural–Urban Level Analysis of Crude Cardiovascular Mortality Data (1999 to 2020)
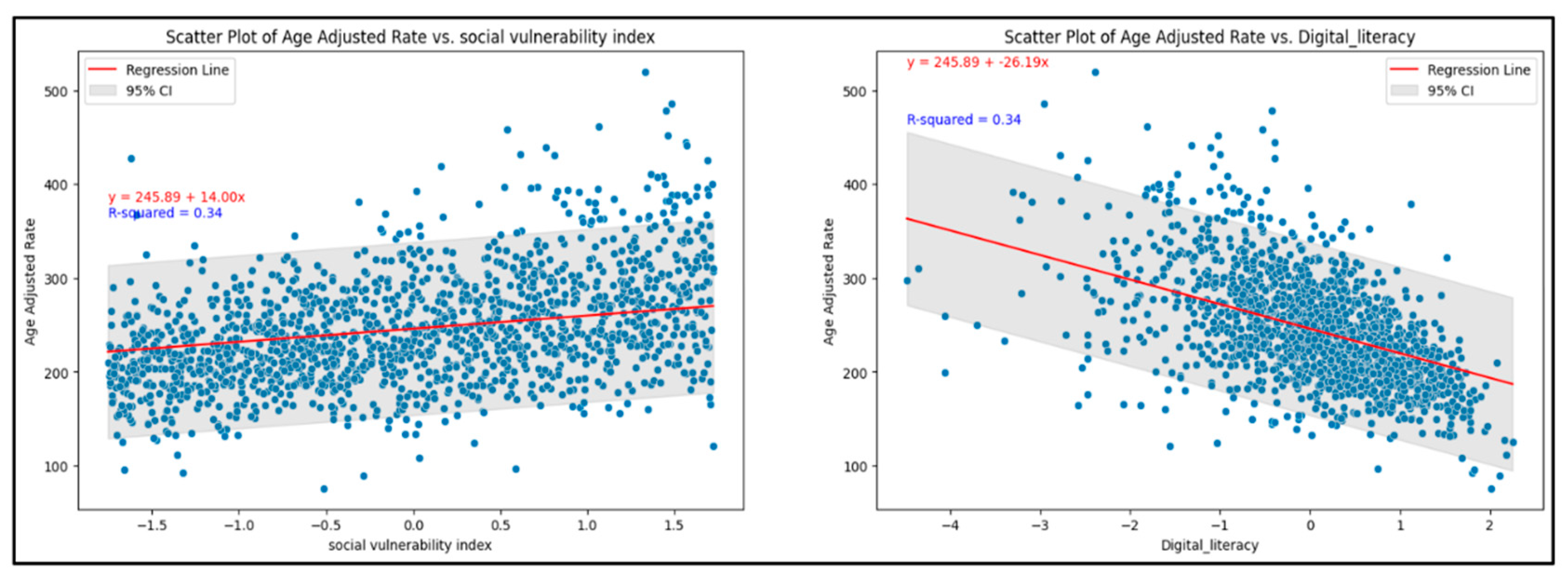
3.1.1. Exploratory Data Analysis Leading to Model 1
3.1.2. Mixed-Effects Model of Crude Cardiovascular Mortality Data (1999 to 2020, Model 1)
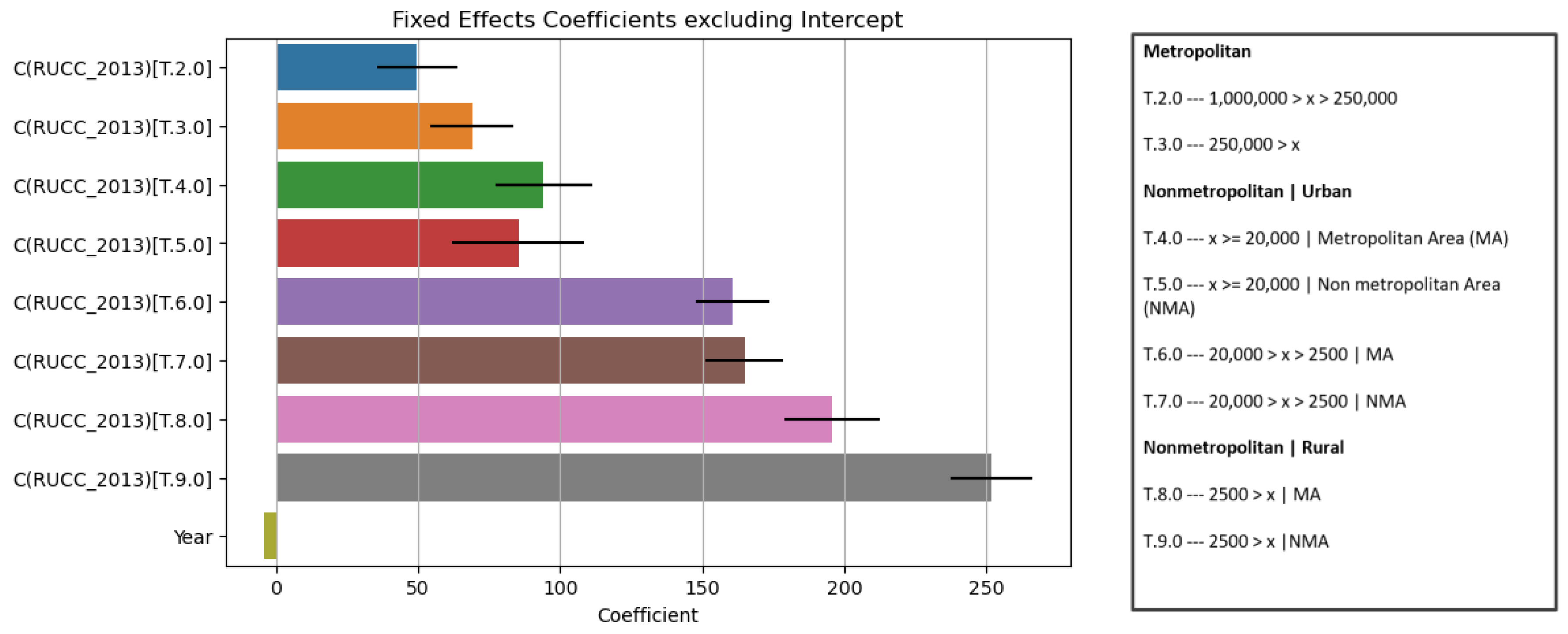
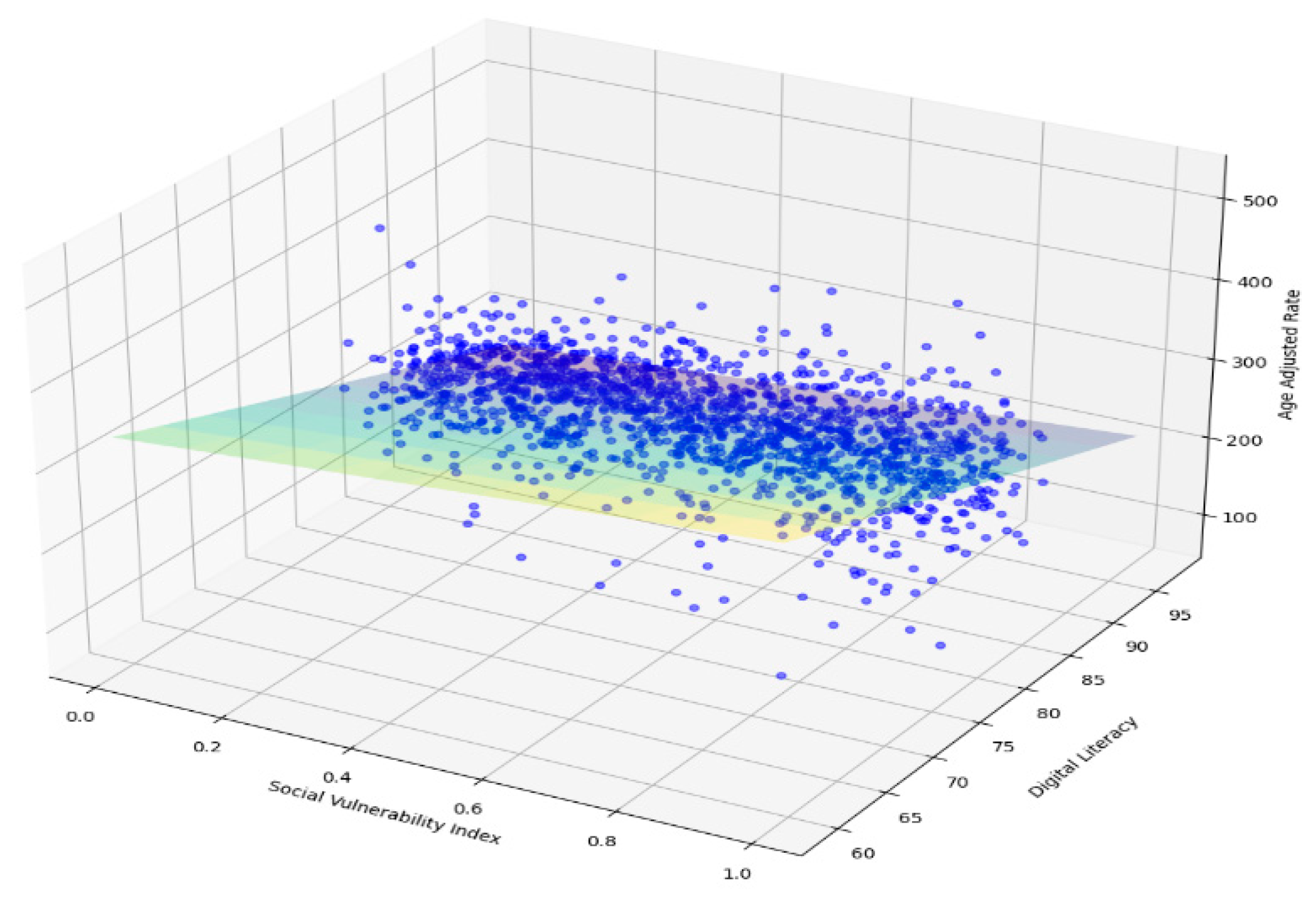
3.1.3. Comprehensive Regression Model for Age-Adjusted Mortality for 2020 (Model 2)
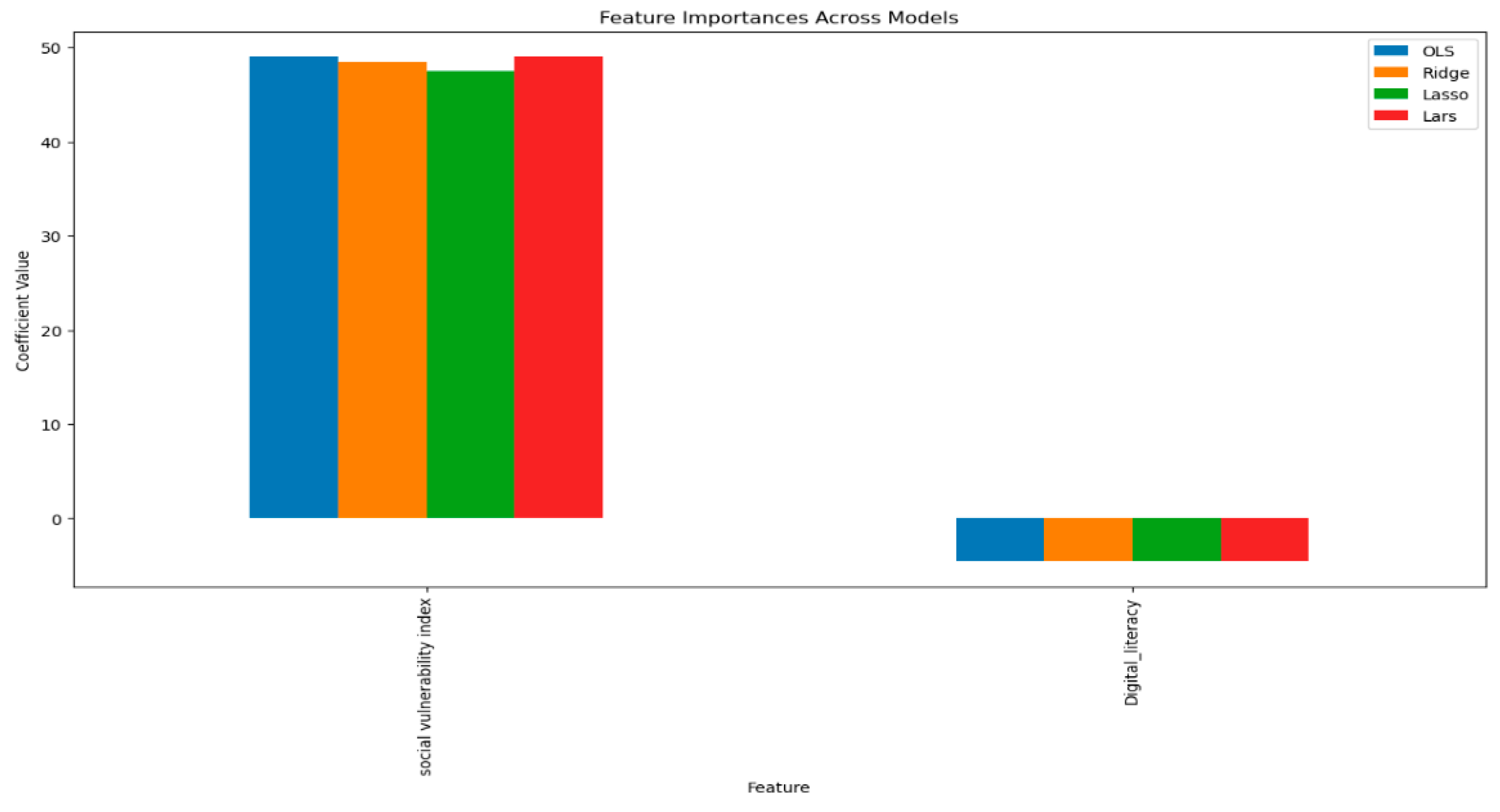
3.1.4. Regression Model for Age-Adjusted Mortality for 2020 (Model 2a)
3.1.5. Age-Adjusted Mortality Prediction per County Using Model 2 and Machine Learning
4. Discussion
4.1. Innovation in This Study
4.2. Strengths of Our Study
4.3. Limitation of Our Study
4.3.1. Potential Biases
4.3.2. Generalizability
4.4. Public Health and Policy Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gala, D.; Makaryus, A.N. The Utility of Language Models in Cardiology: A Narrative Review of the Benefits and Concerns of ChatGPT-4. Int. J. Environ. Res. Public Health 2023, 20, 6438. [Google Scholar] [CrossRef]
- Yu, K.-H.; Beam, A.L.; Kohane, I.S. Artificial Intelligence in Healthcare. Nat. Biomed. Eng. 2018, 2, 719–731. [Google Scholar] [CrossRef]
- Linardatos, P.; Papastefanopoulos, V.; Kotsiantis, S. Explainable AI: A Review of Machine Learning Interpretability Methods. Entropy 2020, 23, 18. [Google Scholar] [CrossRef]
- Tustumi, F.; Andreollo, N.A.; de Aguilar-Nascimento, J.E. Future of the Language Models in Healthcare: The Role of ChatGPT. Arq. Bras. Cir. Dig. 2023, 36, e1727. [Google Scholar] [CrossRef]
- Siontis, K.C.; Noseworthy, P.A.; Attia, Z.I.; Friedman, P.A. Artificial Intelligence-Enhanced Electrocardiography in Cardiovascular Disease Management. Nat. Rev. Cardiol. 2021, 18, 465–478. [Google Scholar] [CrossRef]
- Battina, D.S. A Review Analysis on the Potential for Artificial Intelligence in Healthcare. SSRN Electron. J. 2017, 5, 774–778. [Google Scholar]
- Shakibfar, S.; Nyberg, F.; Li, H.; Zhao, J.; Nordeng, H.M.E.; Sandve, G.K.F.; Pavlovic, M.; Hajiebrahimi, M.; Andersen, M.; Sessa, M. Artificial Intelligence-Driven Prediction of COVID-19-Related Hospitalization and Death: A Systematic Review. Front. Public Health 2023, 11, 1183725. [Google Scholar] [CrossRef]
- Xin, Y.; Li, H.; Zhou, Y.; Yang, Q.; Mu, W.; Xiao, H.; Zhuo, Z.; Liu, H.; Wang, H.; Qu, X.; et al. The Accuracy of Artificial Intelligence in Predicting COVID-19 Patient Mortality: A Systematic Review and Meta-Analysis. BMC Med. Inform. Decis. Mak. 2023, 23, 155. [Google Scholar] [CrossRef]
- Ngiam, K.Y.; Khor, I.W. Big Data and Machine Learning Algorithms for Health-Care Delivery. Lancet Oncol. 2019, 20, e262–e273. [Google Scholar] [CrossRef]
- Schwalbe, N.; Wahl, B. Artificial Intelligence and the Future of Global Health. Lancet 2020, 395, 1579–1586. [Google Scholar] [CrossRef]
- Poverty and Access to Internet, by County. Available online: https://www.ahrq.gov/sdoh/data-analytics/sdoh-tech-poverty.html (accessed on 12 September 2023).
- Health Online 2013. Available online: https://www.pewresearch.org/internet/2013/01/15/health-online-2013-2/ (accessed on 10 September 2023).
- Improving Digital Health Literacy. Available online: https://www.ruralhealthinfo.org/toolkits/health-literacy/2/digital-literacy (accessed on 10 September 2023).
- Gilster, P.; Glister, P. Digital Literacy. Available online: https://www.academia.edu/download/8413655/diglit.pdf (accessed on 10 September 2023).
- Campanozzi, L.L.; Gibelli, F.; Bailo, P.; Nittari, G.; Sirignano, A.; Ricci, G. The Role of Digital Literacy in Achieving Health Equity in the Third Millennium Society: A Literature Review. Front. Public Health 2023, 11, 1109323. [Google Scholar] [CrossRef]
- CDC/ATSDR Social Vulnerability Index. Available online: https://www.atsdr.cdc.gov/placeandhealth/svi/index.html (accessed on 7 September 2023).
- Marmot, M. Social Determinants of Health Inequalities. Lancet 2005, 365, 1099–1104. [Google Scholar] [CrossRef]
- World Health Organization. The World Health Report: 2004: Changing History. Available online: https://apps.who.int/iris/bitstream/handle/10665/42891/924156265X.pdf (accessed on 26 October 2023).
- Phelan, J.C.; Link, B.G.; Tehranifar, P. Social Conditions as Fundamental Causes of Health Inequalities: Theory, Evidence, and Policy Implications. J. Health Soc. Behav. 2010, 51, S28–S40. [Google Scholar] [CrossRef]
- Moissl, A.P.; Delgado, G.E.; Krämer, B.K.; März, W.; Kleber, M.E.; Grammer, T.B. Area-Based Socioeconomic Status and Mortality: The Ludwigshafen Risk and Cardiovascular Health Study. Clin. Res. Cardiol. 2020, 109, 103–114. [Google Scholar] [CrossRef]
- Stringhini, S.; Carmeli, C.; Jokela, M.; Avendaño, M.; McCrory, C.; d’Errico, A.; Bochud, M.; Barros, H.; Costa, G.; Chadeau-Hyam, M.; et al. Socioeconomic Status, Non-Communicable Disease Risk Factors, and Walking Speed in Older Adults: Multi-Cohort Population Based Study. BMJ 2018, 360, k1046. [Google Scholar] [CrossRef]
- Jackson, C.A.; Jones, N.R.V.; Walker, J.J.; Fischbacher, C.M.; Colhoun, H.M.; Leese, G.P.; Lindsay, R.S.; McKnight, J.A.; Morris, A.D.; Petrie, J.R.; et al. Area-Based Socioeconomic Status, Type 2 Diabetes and Cardiovascular Mortality in Scotland. Diabetologia 2012, 55, 2938–2945. [Google Scholar] [CrossRef]
- Wilson, W.E.; Mar, T.F.; Koenig, J.Q. Influence of Exposure Error and Effect Modification by Socioeconomic Status on the Association of Acute Cardiovascular Mortality with Particulate Matter in Phoenix. J. Expo. Sci. Environ. Epidemiol. 2007, 17 (Suppl. S2), S11–S19. [Google Scholar] [CrossRef]
- Kasim, S.; Malek, S.; Song, C.; Wan Ahmad, W.A.; Fong, A.; Ibrahim, K.S.; Safiruz, M.S.; Aziz, F.; Hiew, J.H.; Ibrahim, N. In-Hospital Mortality Risk Stratification of Asian ACS Patients with Artificial Intelligence Algorithm. PLoS ONE 2022, 17, e0278944. [Google Scholar] [CrossRef]
- Khamis, G.S.M.; Alanazi, S.M. Exploring Sex Disparities in Cardiovascular Disease Risk Factors Using Principal Component Analysis and Latent Class Analysis Techniques. BMC Med. Inform. Decis. Mak. 2023, 23, 101. [Google Scholar] [CrossRef]
- Journal of Machine Learning Research. Available online: https://www.jmlr.org/papers/v24/ (accessed on 26 October 2023).
- Han, C.; Kim, D.W.; Kim, S.; You, S.C.; Bae, S.; Yoon, D. Large-Language-Model-Based 10-Year Risk Prediction of Cardiovascular Disease: Insight from the UK Biobank Data. bioRxiv 2023. [Google Scholar] [CrossRef]
- Ahmad, F.B.; Cisewski, J.A.; Xu, J.; Anderson, R.N. Provisional Mortality Data—United States, 2022. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 488–492. [Google Scholar] [CrossRef]
- Clink, K. Cdc Wonder. Ref. Rev. 2017, 31, 14. [Google Scholar] [CrossRef]
- Cromartie, J. USDA ERS—Rural Classifications. Available online: https://www.ers.usda.gov/topics/rural-economy-population/rural-classifications/ (accessed on 7 September 2023).
- US Census Bureau American National Standards Institute (ANSI), Federal Information Processing Series (FIPS), and Other Standardized Geographic Codes. 2023. Available online: https://www.census.gov/library/reference/code-lists/ansi.html (accessed on 26 October 2023).
- Computers and Internet. Available online: https://censusreporter.org/topics/computer-internet/ (accessed on 12 September 2023).
- Education. Available online: https://censusreporter.org/topics/education/ (accessed on 12 September 2023).
- US Census Bureau Sample ACS & PRCS Forms and Instructions. 2022. Available online: https://www.census.gov/programs-surveys/acs/about/forms-and-instructions.html (accessed on 12 September 2023).
- The Digital Economy and Society Index (DESI). Available online: https://digital-strategy.ec.europa.eu/en/policies/desi (accessed on 25 September 2023).
- Blank, R.; Strickling, L. Exploring the Digital Nation: Computer and Internet Use at Home. Available online: https://www.ntia.doc.gov/files/ntia/publications/exploring_the_digital_nation_computer_and_internet_use_at_home_11092011.pdf (accessed on 12 September 2023).
- Office of Internet Connectivity and Growth. Available online: https://www.ntia.gov/sites/default/files/publications/office_of_internet_connectivity_and_growth_2022_annual_report.pdf (accessed on 12 September 2023).
- Lövdén, M.; Fratiglioni, L.; Glymour, M.M.; Lindenberger, U.; Tucker-Drob, E.M. Education and Cognitive Functioning across the Life Span. Psychol. Sci. Public Interest. 2020, 21, 6–41. [Google Scholar] [CrossRef]
- Leu, D.J., Jr.; Kinzer, C.K.; Coiro, J.; Cammack, D.W. Toward a Theory of New Literacies Emerging from the Internet and Other Information and Communication Technologies. In Theoretical Models and Processes of Reading; International Reading Association: Newark, DE, USA, 2005; pp. 1570–1613. ISBN 9780872075023. [Google Scholar]
- Tyner, K. Literacy in a Digital World: Teaching and Learning in the Age of Information; Routledge: Abingdon-on-Thames, UK, 2014; ISBN 9781135690847. [Google Scholar]
- De Angelis, L.; Baglivo, F.; Arzilli, G.; Privitera, G.P.; Ferragina, P.; Tozzi, A.E.; Rizzo, C. ChatGPT and the Rise of Large Language Models: The New AI-Driven Infodemic Threat in Public Health. Front. Public Health 2023, 11, 1166120. [Google Scholar] [CrossRef]
- CDC Leading Causes of Death in Rural America. Available online: https://www.cdc.gov/ruralhealth/cause-of-death.html (accessed on 17 September 2023).
- Bureau, U.S.C. Understanding and Using American Community Survey Data: What All Data Users Need to Know; US Department of Commerce, Economics and Statistics Administration: Washington, DC, USA, 2020.
- Wood, E.; Sanders, M.; Frazier, T. The Practical Use of Social Vulnerability Indicators in Disaster Management. Int. J. Disaster Risk Reduct. 2021, 63, 102464. [Google Scholar] [CrossRef]
- Chakraborty, L.; Rus, H.; Henstra, D.; Thistlethwaite, J.; Minano, A.; Scott, D. Exploring Spatial Heterogeneity and Environmental Injustices in Exposure to Flood Hazards Using Geographically Weighted Regression. Environ. Res. 2022, 210, 112982. [Google Scholar] [CrossRef]
- At A Glance: CDC/ATSDR Social Vulnerability Index. Available online: https://www.atsdr.cdc.gov/placeandhealth/svi/at-a-glance_svi.html (accessed on 17 September 2023).
- Jain, V.; Al Rifai, M.; Khan, S.U.; Kalra, A.; Rodriguez, F.; Samad, Z.; Pokharel, Y.; Misra, A.; Sperling, L.S.; Rana, J.S.; et al. Association Between Social Vulnerability Index and Cardiovascular Disease: A Behavioral Risk Factor Surveillance System Study. J. Am. Heart Assoc. 2022, 11, e024414. [Google Scholar] [CrossRef]
- Islam, S.J.; Malla, G.; Yeh, R.W.; Quyyumi, A.A.; Kazi, D.S.; Tian, W.; Song, Y.; Nayak, A.; Mehta, A.; Ko, Y.-A.; et al. County-Level Social Vulnerability Is Associated With In-Hospital Death and Major Adverse Cardiovascular Events in Patients Hospitalized with COVID-19: An Analysis of the American Heart Association COVID-19 Cardiovascular Disease Registry. Circ. Cardiovasc. Qual. Outcomes 2022, 15, e008612. [Google Scholar] [CrossRef]
- Khan, S.U.; Javed, Z.; Lone, A.N.; Dani, S.S.; Amin, Z.; Al-Kindi, S.G.; Virani, S.S.; Sharma, G.; Blankstein, R.; Blaha, M.J.; et al. Social Vulnerability and Premature Cardiovascular Mortality Among US Counties, 2014 to 2018. Circulation 2021, 144, 1272–1279. [Google Scholar] [CrossRef]
- Bevan, G.; Pandey, A.; Griggs, S.; Dalton, J.E.; Zidar, D.; Patel, S.; Khan, S.U.; Nasir, K.; Rajagopalan, S.; Al-Kindi, S. Neighborhood-Level Social Vulnerability and Prevalence of Cardiovascular Risk Factors and Coronary Heart Disease. Curr. Probl. Cardiol. 2023, 48, 101182. [Google Scholar] [CrossRef]
- Buehler, J.W.; Centers for Disease Control and Prevention. CDC’s Vision for Public Health Surveillance in the 21st Century. MMWR Morb. Mortal. Wkly. Rep. 2012, 61, 1–2. [Google Scholar]
- Thacker, S.B.; Qualters, J.R.; Lee, L.M. Public Health Surveillance in the United States: Evolution and Challenges*. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/su6103a2.htm (accessed on 17 September 2023).
- Nsubuga, P.; White, M.E.; Thacker, S.B.; Anderson, M.A.; Blount, S.B.; Broome, C.V.; Chiller, T.M.; Espitia, V.; Imtiaz, R.; Sosin, D.; et al. Public Health Surveillance: A Tool for Targeting and Monitoring Interventions; The International Bank for Reconstruction and Development, The World Bank: Bretton Woods, NH, USA, 2006. [Google Scholar]
- U.S. Census Bureau Explore Census Data. Available online: https://data.census.gov/ (accessed on 17 September 2023).
- Wong, J.S.; Bouchard, J. Do Meta-Analyses of Intervention/prevention Programs in the Field of Criminology Meet the Tests of Transparency and Reproducibility? Trauma. Violence Abus. 2023, 24, 1522–1542. [Google Scholar] [CrossRef]
- Smith, E.P.; Cairns, J., Jr. Extrapolation Methods for Setting Ecological Standards for Water Quality: Statistical and Ecological Concerns. Ecotoxicology 1993, 2, 203–219. [Google Scholar] [CrossRef]
- Warren, J.; Argentesi, F.; Avenhaus, R.; Franklin, M.; Shipley, J.P. Mathematical and Statistical Methods in Nuclear Safeguards. Technometrics 1990, 32, 360. [Google Scholar] [CrossRef]
- Thirunavukarasu, A.J.; Ting, D.S.J.; Elangovan, K.; Gutierrez, L.; Tan, T.F.; Ting, D.S.W. Large Language Models in Medicine. Nat. Med. 2023, 29, 1930–1940. [Google Scholar] [CrossRef]
- Alaa, A.M.; Bolton, T.; Di Angelantonio, E.; Rudd, J.H.F.; van der Schaar, M. Cardiovascular Disease Risk Prediction Using Automated Machine Learning: A Prospective Study of 423,604 UK Biobank Participants. PLoS ONE 2019, 14, e0213653. [Google Scholar] [CrossRef]
- Goldstein, B.A.; Navar, A.M.; Carter, R.E. Moving beyond Regression Techniques in Cardiovascular Risk Prediction: Applying Machine Learning to Address Analytic Challenges. Eur. Heart J. 2017, 38, 1805–1814. [Google Scholar] [CrossRef]
- Rosenblatt, R.A.; Hart, L.G. Physicians and Rural America. West. J. Med. 2000, 173, 348–351. [Google Scholar] [CrossRef]
- 35th Bethesda Conference. Cardiology’s Workforce Crisis: A Pragmatic Approach. Bethesda, Maryland, 17–18 October 2003. J. Am. Coll. Cardiol. 2004, 44, 216–275. [CrossRef]
- Rural Health Disparities. Available online: https://www.ruralhealthinfo.org/topics/rural-health-disparities (accessed on 30 October 2023).
- Cheng, H.-W. Challenges and Limitations of ChatGPT and Artificial Intelligence for Scientific Research: A Perspective from Organic Materials. AI 2023, 4, 401–405. [Google Scholar] [CrossRef]
- van Smeden, M.; Heinze, G.; Van Calster, B.; Asselbergs, F.W.; Vardas, P.E.; Bruining, N.; de Jaegere, P.; Moore, J.H.; Denaxas, S.; Boulesteix, A.L.; et al. Critical Appraisal of Artificial Intelligence-Based Prediction Models for Cardiovascular Disease. Eur. Heart J. 2022, 43, 2921–2930. [Google Scholar] [CrossRef]
- US Census Bureau Urban and Rural Classification Press Kit. 2023. Available online: https://www.census.gov/newsroom/press-kits/2022/urban-rural-classification.html (accessed on 3 October 2023).
- Lavery, M.R.; Acharya, P.; Sivo, S.A.; Xu, L. Number of Predictors and Multicollinearity: What Are Their Effects on Error and Bias in Regression? Commun. Stat. Simul. Comput. 2019, 48, 27–38. [Google Scholar] [CrossRef]
- Shreffler, J.; Huecker, M.R. Type I and Type II Errors and Statistical Power; StatPearls Publishing: St. Petersburg, FL, USA, 2023. [Google Scholar]
- Rodriguez, F.; Hastings, K.G.; Boothroyd, D.B.; Echeverria, S.; Lopez, L.; Cullen, M.; Harrington, R.A.; Palaniappan, L.P. Disaggregation of Cause-Specific Cardiovascular Disease Mortality Among Hispanic Subgroups. JAMA Cardiol. 2017, 2, 240–247. [Google Scholar] [CrossRef]
- McNaughton, C.D.; Cawthon, C.; Kripalani, S.; Liu, D.; Storrow, A.B.; Roumie, C.L. Health Literacy and Mortality: A Cohort Study of Patients Hospitalized for Acute Heart Failure. J. Am. Heart Assoc. 2015, 4, e001799. [Google Scholar] [CrossRef]
- Baker, D.W.; Wolf, M.S.; Feinglass, J.; Thompson, J.A.; Gazmararian, J.A.; Huang, J. Health Literacy and Mortality among Elderly Persons. Arch. Intern. Med. 2007, 167, 1503–1509. [Google Scholar] [CrossRef]
- Health and Economic Costs of Chronic Diseases. Available online: https://www.cdc.gov/chronicdisease/about/costs/index.htm (accessed on 19 September 2023).
- Virani, S.S.; Callaway, C.W.; Chamberlain, A.M. Heart Disease and Stroke statistics—2018 Update: A Report from the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar]
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of Potentially Modifiable Risk Factors Associated with Myocardial Infarction in 52 Countries (the INTERHEART Study): Case-Control Study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef]
- Mathur, P.; Srivastava, S.; Xu, X.; Mehta, J.L. Artificial Intelligence, Machine Learning, and Cardiovascular Disease. Clin. Med. Insights Cardiol. 2020, 14, 1179546820927404. [Google Scholar] [CrossRef]
- Piazza, M. Billions of Dollars Have Been Set aside to Try to Narrow the Digital Divide by Expanding Access to Broadband Internet Connectivity. How Is That Money Being Spent? Ask the Expert 2023. Available online: https://www.clevelandfed.org/publications/ask-the-expert/2023/ate-20231114-piazza (accessed on 31 October 2023).
- Lee, Nicol Turner, James Seddon, Brooke Tanner and Samantha Lai. Why the Federal Government Needs to Step up Efforts to Close the Rural Broadband Divide. Brookings Institution, 2022. Available online: https://www.brookings.edu/articles/why-the-federal-government-needs-to-step-up-their-efforts-to-close-the-rural-broadband-divide/ (accessed on 31 October 2023).
- Mukhopadhyay, S.; Basak, R.; Khairat, S.; Carney, T.J. Revisiting Provider Role in Patient Use of Online Medical Records. Appl. Clin. Inform. 2021, 12, 1110–1119. [Google Scholar] [CrossRef]
- Smart Villages: How to Ensure That Digital Strategies Benefit Rural Communities. Available online: https://regiosuisse.ch/en/documents/smart-villages-how-ensure-digital-strategies-benefit-rural-communities (accessed on 3 October 2023).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Headings under Request Form Tab on wonder.cdc.gov (Accessed on 31 October 2023) | Data Selected |
|---|---|
| 1. Organize table layout: |
|
| 2. Location |
|
| 3. Demographics |
|
| 4. Select year and months | Appropriate year(s) chosen |
| 5. Weekday autopsy and place of death |
|
| 6. Select Cause of death |
|
| Description of Variables | Coefficient (β) | Intercept |
|---|---|---|
| y (Age-adjusted mortality) | NA | c = 602.77 |
| x1 = SVI | 49.01 | |
| x2 = DLI | −4.51 |
| Process | Example | Description | Simili | |
|---|---|---|---|---|
| ENCODER | User Prompt leads to tokenization | “What is the Code for no internet in the census?” | Tokenization involves breaking down sentences into smaller units known as tokens. The tokens are compared to model-trained parameters. Self-inspection identifies the crucial text. | This is similar to the first detective who reviews clues and consults the agency’s database to find the most relevant clues compared to past cases |
| Feed Forward Network | Identified tokens are analyzed, with some being combined and others discarded. | This is analogous to a team of detectives refining the case based on prior cases. | ||
| Stacking layers | An iterative process, each layer builds on the findings of the previous layer using attention mechanisms and backpropagation. | This is similar to clues being continuously refined in terms of their significance. | ||
| DECODER | Conclusion | The process concludes by suggesting a variable name as the output. | This is similar to a process in which detectives reach a consensus and generate an output. | |
| Contextualization | The model considers the ‘n’ most recent tokens to keep the process in context. | This is similar to a detective who keeps the case history, especially when the investigation is part of a larger context. |
| Description of Variables | Coefficient (β) | p-Value |
|---|---|---|
| y (age-adjusted mortality) | ||
| x1 = SVI | 50.28 | 0 |
| x2 = DVI | −3.83 | 0 |
| x3 = RUCC 2 (metro areas with a population of 250,000 to 1,000,000) | 0.11 | 0.975 |
| x4 = RUCC 3 (metro areas with a population of less than 250,000) | 0.59 | 0.86 |
| x5 = RUCC 4 (nonmetro area adjacent to a metro area with a population of 20,000 or more) | 7.67 | 0.053 |
| x6 = RUCC 5 (nonmetro area not adjacent to a metro area with a population of 20,000 or more) | 0.41 | 0.94 |
| x7 = RUCC 6 (urban population of 2500 to 19,999 adjacent to a metro area) | 11.44 | 0 |
| x8 = RUCC 7 (urban population of 2500 to 19,999 not adjacent to a metro area) | 3.92 | 0.23 |
| x9 = RUCC 8 (completely rural or less than 2500 urban population adjacent to a metro area) | 4.23 | 0.316 |
| x10 = RUCC 9 (completely rural or less than 2500 urban population not adjacent to a metro area) | 4.08 | 0.265 |
| Social Vulnerability Index | Digital Literacy | Predicted Age-Adjusted Mortality Rate per 100,000 (OLS Model) | Predicted Age-Adjusted Rate per 100,000 (LGBMregressor) | |
|---|---|---|---|---|
| Greene County, Ohio | 0.16 | 92.17 | 232 | 240.83 |
| Midland County, Michigan | 0.15 | 88.2 | 247.89 | 241.4 |
| Polk County, Minnesota | 0.4 | 88.02 | 260.62 | 242.6 |
| Mariposa County, California | 0.83 | 87.01 | 285.95 | 242.6 |
| Grand Isle County, Vermont | 0.01 | 94.85 | 213.44 | 237.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali, M.M.; Gandhi, S.; Sulaiman, S.; Jafri, S.H.; Ali, A.S. Mapping the Heartbeat of America with ChatGPT-4: Unpacking the Interplay of Social Vulnerability, Digital Literacy, and Cardiovascular Mortality in County Residency Choices. J. Pers. Med. 2023, 13, 1625. https://doi.org/10.3390/jpm13121625
Ali MM, Gandhi S, Sulaiman S, Jafri SH, Ali AS. Mapping the Heartbeat of America with ChatGPT-4: Unpacking the Interplay of Social Vulnerability, Digital Literacy, and Cardiovascular Mortality in County Residency Choices. Journal of Personalized Medicine. 2023; 13(12):1625. https://doi.org/10.3390/jpm13121625
Chicago/Turabian StyleAli, Mohammed M., Subi Gandhi, Samian Sulaiman, Syed H. Jafri, and Abbas S. Ali. 2023. "Mapping the Heartbeat of America with ChatGPT-4: Unpacking the Interplay of Social Vulnerability, Digital Literacy, and Cardiovascular Mortality in County Residency Choices" Journal of Personalized Medicine 13, no. 12: 1625. https://doi.org/10.3390/jpm13121625
APA StyleAli, M. M., Gandhi, S., Sulaiman, S., Jafri, S. H., & Ali, A. S. (2023). Mapping the Heartbeat of America with ChatGPT-4: Unpacking the Interplay of Social Vulnerability, Digital Literacy, and Cardiovascular Mortality in County Residency Choices. Journal of Personalized Medicine, 13(12), 1625. https://doi.org/10.3390/jpm13121625