

Quality of Life and Audiological Benefits in Pediatric Cochlear Implant Users in Romania: Systematic Review and Cohort Study


Abstract
:1. Introduction
- A systematic review of the current literature regarding the QoL of CI users was conducted to obtain an overview of the generic QoL questionnaires utilized in the literature, and to see which questionnaires were employed for pediatric CI users.
- The generic QoL of the Romanian CI user study cohort was assessed, and they were compared with age- and gender-matched peers with normal hearing.
- Data from the study cohort were collected to assess the level of speech comprehension and hearing ability of pediatric CI users in Romania using the translated and recorded HSM sentence test and pure tone audiometry.
- Possible influencing factors, such as early-implanted (≤3 years) CI users versus late-implanted (>3 years) children, were investigated.
- Finally, possible correlations between the generic and health-related quality of life questionnaires were assessed.
2. Materials and Methods
2.1. Systematic Review
2.2. Data Collection from the Study Cohort in Romania
2.2.1. Participants
2.2.2. Data Collection
2.2.3. Quality of Life Assessments
Assessment of Quality of Life (AQoL-6D)
Speech, Spatial and Qualities of Hearing Scale (SSQ12)
2.2.4. Audiological Measurements
Sound Field Audiometry (Clinical Set-Up)
Speech Audiometry (Camp Set-Up)
2.2.5. Data Analysis
3. Results
3.1. Systematic Review
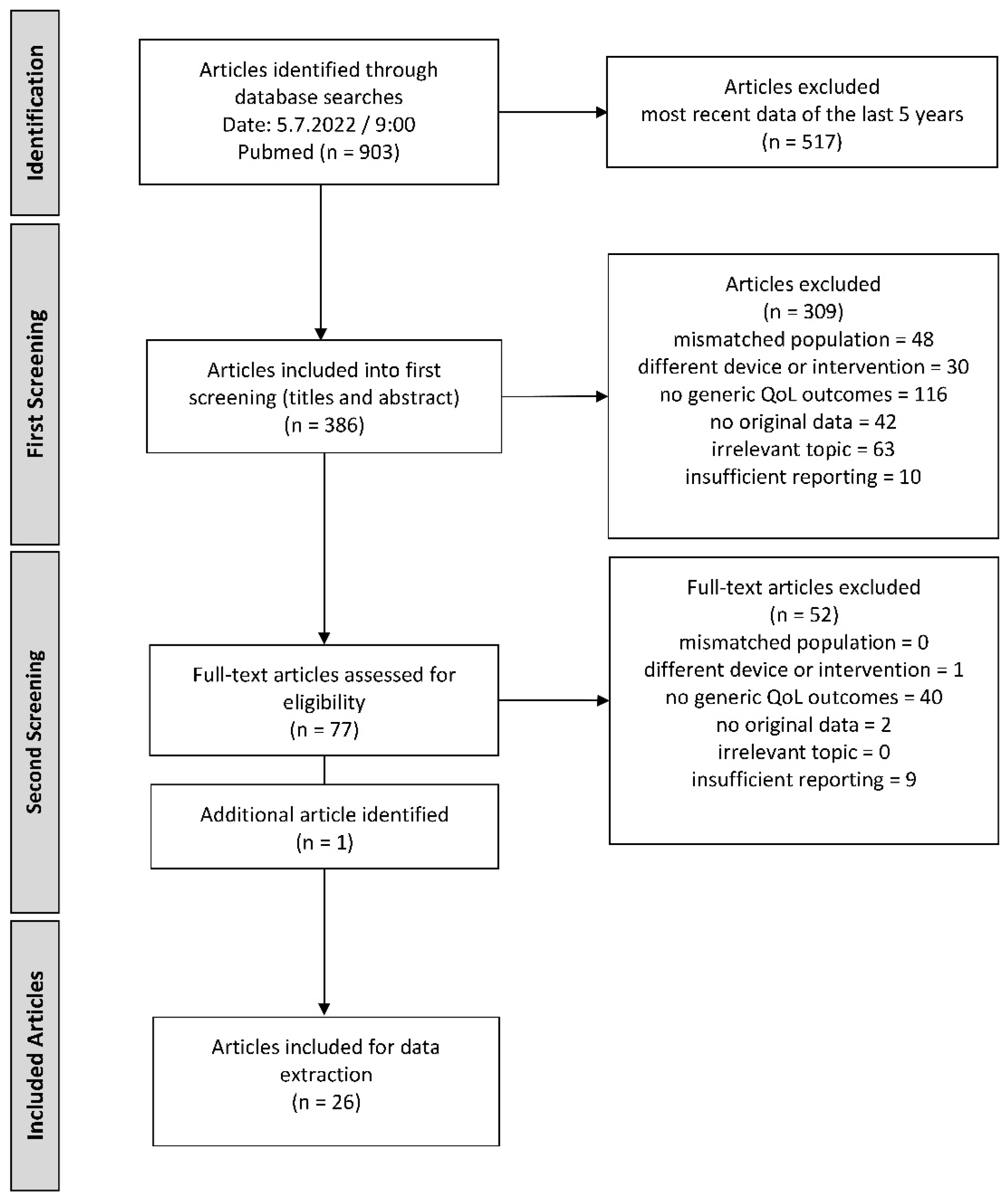
3.1.1. Screening Process
3.1.2. Adult CI Users and Their Generic QoL
3.1.3. Pediatric CI Users and Their Generic QoL
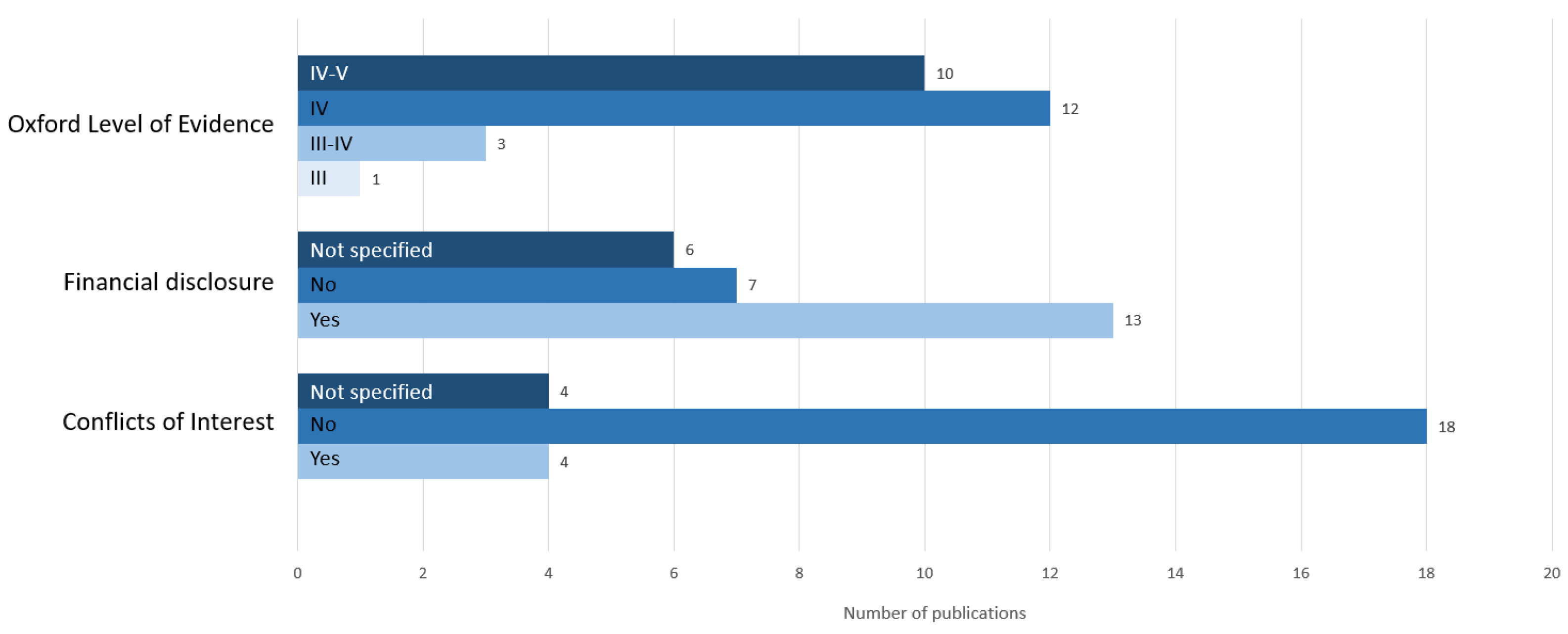
3.1.4. Quality Evaluation of Extracted Publications
3.2. Data Collection from Study Cohort in Romania
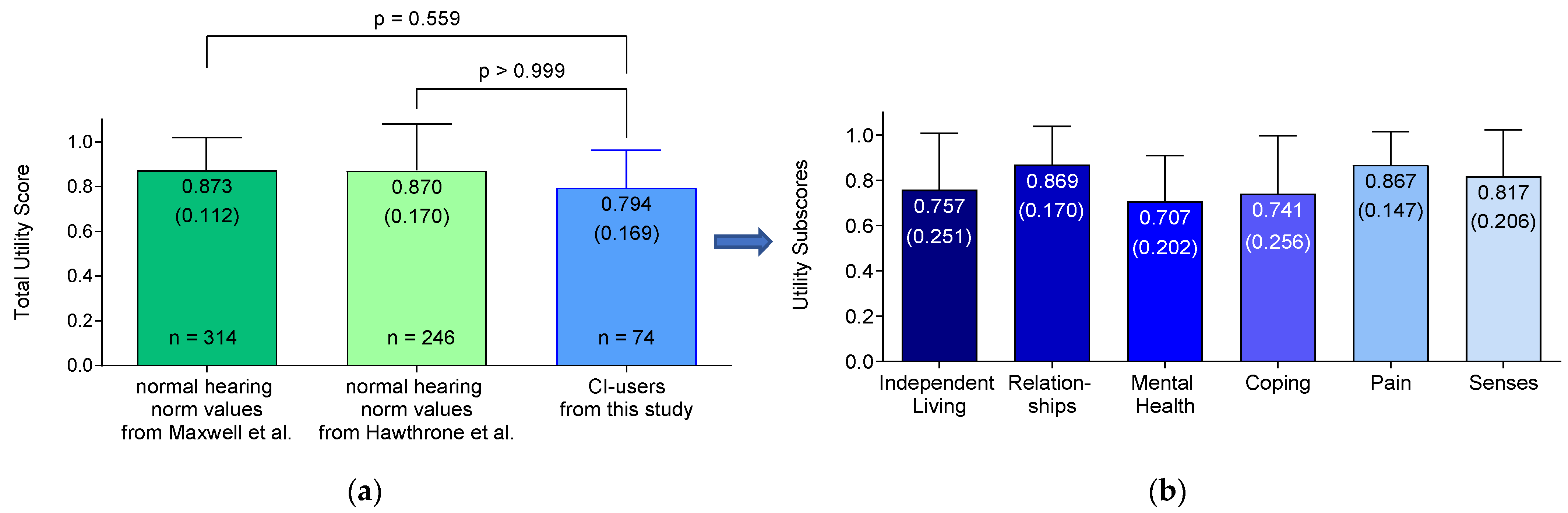
3.2.1. Assessment of Quality of Life (AQoL-6D)
3.2.2. Speech Spatial Qualities of Hearing Scale (SSQ12)
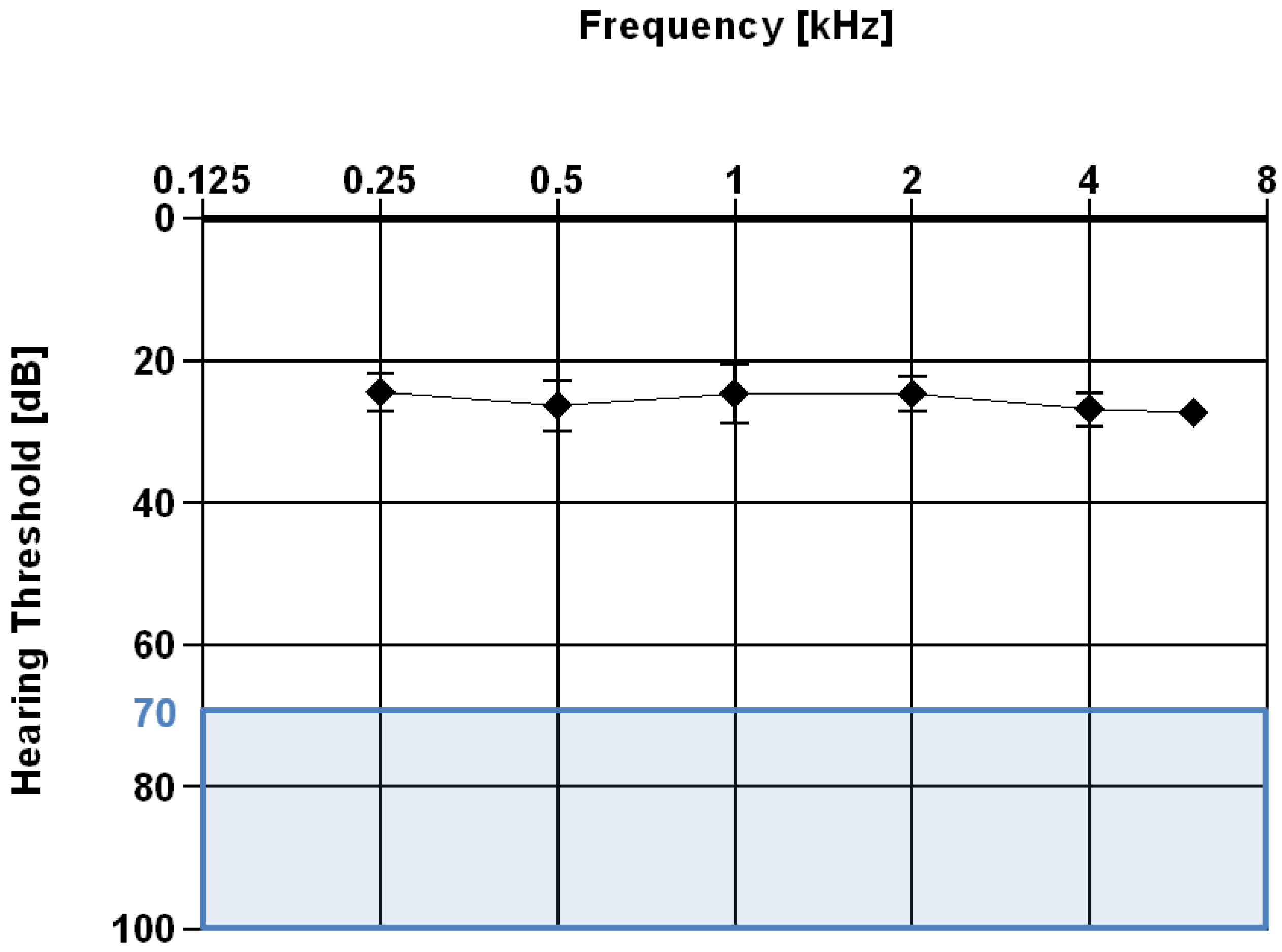
3.2.3. Pure Tone Audiometry
3.2.4. Speech Audiometry
3.2.5. Implantation Timepoint
3.2.6. Generic and Health-Related Quality of Life
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Alnuhayer, O.; Alshawi, Y.; Julaidan, B.; Alromaih, N.; Alakeel, N.; Alballaa, A. Quality of Life and Cochlear Implant: Results in Saudi Children. Cureus 2020, 12, e11968. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Report on Hearing; World Health Organization: Geneva, Switzerland, 2021; ISBN 978-92-4-002048-1. [Google Scholar]
- World Health Organization. Deafness and Hearing Loss. Available online: https://www.who.int/news-room/fact-sheets/detail/deafness-and-hearing-loss (accessed on 29 August 2022).
- Lee, Y.; Sim, H. Bilateral Cochlear Implantation versus Unilateral Cochlear Implantation in Deaf Children: Effects of Sentence Context and Listening Conditions on Recognition of Spoken Words in Sentences. Int. J. Pediatr. Otorhinolaryngol. 2020, 137, 110237. [Google Scholar] [CrossRef] [PubMed]
- Zeng, F.-G. Celebrating the One Millionth Cochlear Implant. JASA Express Lett. 2022, 2, 077201. [Google Scholar] [CrossRef] [PubMed]
- Hirschfelder, A.; Gräbel, S.; Olze, H. The impact of cochlear implantation on quality of life. The role of audiologic performance and variables. Otolaryngol. Head Neck Surg. 2008, 138, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Gatehouse, S.; Noble, W. The Speech, Spatial and Qualities of Hearing Scale (SSQ). Int. J. Audiol. 2004, 43, 85–99. [Google Scholar] [CrossRef]
- Bess, F.H.; Humes, L. Audiology: The Fundamentals, 4th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008; ISBN 978-0-7817-6643-2. [Google Scholar]
- Hochmair-Desoyer, I.; Schulz, E.; Moser, L.; Schmidt, M. The HSM Sentence Test as a Tool for Evaluating the Speech Understanding in Noise of Cochlear Implant Users. Am. J. Otol. 1997, 18, S83. [Google Scholar]
- Haraldstad, K.; Wahl, A.; Andenæs, R.; Andersen, J.R.; Andersen, M.H.; Beisland, E.; Borge, C.R.; Engebretsen, E.; Eisemann, M.; Halvorsrud, L.; et al. A Systematic Review of Quality of Life Research in Medicine and Health Sciences. Qual. Life Res. 2019, 28, 2641–2650. [Google Scholar] [CrossRef]
- Real Life Gains: The Importance of Quality of Life|ExpertsONLINE. 2022. Available online: https://www.youtube.com/watch?v=hQMgpqxWfww&t=2s (accessed on 2 July 2023).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Ball, C.; Phillips, R.; Guyatt, G. OCEBM Levels of Evidence—Centre for Evidence-Based Medicine (CEBM). Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence (accessed on 24 August 2022).
- Iezzi, A. Homepage of the Assessment of Quality of Life. Available online: https://www.aqol.com.au/ (accessed on 17 August 2022).
- Rostkowska, J.; Skarzynski, P.H.; Kobosko, J.; Gos, E.; Skarzynski, H. Health-Related Quality of Life in Adults with Profound Postlingual Hearing Loss before and after Cochlear Implantation. Eur. Arch. Otorhinolaryngol. 2021, 278, 3393–3399. [Google Scholar] [CrossRef]
- Sarant, J.; Harris, D.; Busby, P.; Maruff, P.; Schembri, A.; Dowell, R.; Briggs, R. The Effect of Cochlear Implants on Cognitive Function in Older Adults: Initial Baseline and 18-Month Follow Up Results for a Prospective International Longitudinal Study. Front. Neurosci. 2019, 13, 789. [Google Scholar] [CrossRef]
- Noble, W.; Jensen, N.S.; Naylor, G.; Bhullar, N.; Akeroyd, M.A. A Short Form of the Speech, Spatial and Qualities of Hearing Scale Suitable for Clinical Use: The SSQ12. Int. J. Audiol. 2013, 52, 409–412. [Google Scholar] [CrossRef] [PubMed]
- ASHA. Sound Field Measurement Tutorial. Available online: https://www.asha.org/policy/rp1991-00025/ (accessed on 1 March 2023).
- Gates, G.; Hoffman, H. What the Numbers Mean: An Epidemiological Perspective on Hearing. Available online: https://www.nidcd.nih.gov/health/statistics/what-numbers-mean-epidemiological-perspective-hearing (accessed on 27 February 2023).
- Herzog, M.; Schön, F.; Müller, J.; Knaus, C.; Scholtz, L.; Helms, J. Langzeitergebnisse nach Cochlear-Implant-Versorgung älterer Patienten. Laryngorhinootologie 2003, 82, 490–493. [Google Scholar] [CrossRef] [PubMed]
- Louw, C.; Swanepoel, D.W.; Eikelboom, R.H. Self-Reported Hearing Loss and Pure Tone Audiometry for Screening in Primary Health Care Clinics. J. Prim. Care Commun. Health 2018, 9, 2150132718803156. [Google Scholar] [CrossRef]
- Anzivino, R.; Conti, G.; Di Nardo, W.; Fetoni, A.R.; Picciotti, P.M.; Marra, C.; Guglielmi, V.; Fortunato, S.; Forli, F.; Paludetti, G.; et al. Prospective Evaluation of Cognitive Functions After Rehabilitation with Cochlear Implant or Hearing Aids: Preliminary Results of a Multicentric Study on Elderly Patients. Am. J. Audiol. 2019, 28, 762–774. [Google Scholar] [CrossRef] [PubMed]
- Calvino, M.; Sánchez-Cuadrado, I.; Gavilán, J.; Gutiérrez-Revilla, M.A.; Polo, R.; Lassaletta, L. Effect of Cochlear Implantation on Cognitive Decline and Quality of Life in Younger and Older Adults with Severe-to-Profound Hearing Loss. Eur. Arch. Otorhinolaryngol. 2022, 279, 4745–4759. [Google Scholar] [CrossRef]
- Hey, M.; Wesarg, T.; Mewes, A.; Helbig, S.; Hornung, J.; Lenarz, T.; Briggs, R.; Marx, M.; Ramos, A.; Stöver, T.; et al. Objective, Audiological and Quality of Life Measures with the CI532 Slim Modiolar Electrode. Cochlear Implant. Int. 2019, 20, 80–90. [Google Scholar] [CrossRef]
- Sivonen, V.; Sinkkonen, S.T.; Willberg, T.; Lamminmäki, S.; Jääskelä-Saari, H.; Aarnisalo, A.A.; Dietz, A. Improvements in Hearing and in Quality of Life after Sequential Bilateral Cochlear Implantation in a Consecutive Sample of Adult Patients with Severe-to-Profound Hearing Loss. J. Clin. Med. 2021, 10, 2394. [Google Scholar] [CrossRef]
- Sorrentino, T.; Donati, G.; Nassif, N.; Pasini, S.; Redaelli de Zinis, L.O. Cognitive Function and Quality of Life in Older Adult Patients with Cochlear Implants. Int. J. Audiol. 2020, 59, 316–322. [Google Scholar] [CrossRef]
- Tang, L.; Thompson, C.B.; Clark, J.H.; Ceh, K.M.; Yeagle, J.D.; Francis, H.W. Rehabilitation and Psychosocial Determinants of Cochlear Implant Outcomes in Older Adults. Ear Hear. 2017, 38, 663–671. [Google Scholar] [CrossRef]
- Forli, F.; Lazzerini, F.; Fortunato, S.; Bruschini, L.; Berrettini, S. Cochlear Implant in the Elderly: Results in Terms of Speech Perception and Quality of Life. Audiol. Neurootol. 2019, 24, 77–83. [Google Scholar] [CrossRef]
- Peters, J.P.M.; van Heteren, J.A.A.; Wendrich, A.W.; van Zanten, G.A.; Grolman, W.; Stokroos, R.J.; Smit, A.L. Short-Term Outcomes of Cochlear Implantation for Single-Sided Deafness Compared to Bone Conduction Devices and Contralateral Routing of Sound Hearing Aids-Results of a Randomised Controlled Trial (CINGLE-Trial). PLoS ONE 2021, 16, e0257447. [Google Scholar] [CrossRef]
- Chen, S.L.; Chan, K.C.; Hu, C.Y.; Fang, H.Y.; Wu, C.M. Experience of Adult Cochlear Implantation at a Tertiary Hospital. J. Chin. Med. Assoc. 2022, 85, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Peter, N.; Kleinjung, T.; Probst, R.; Hemsley, C.; Veraguth, D.; Huber, A.; Caversaccio, M.; Kompis, M.; Mantokoudis, G.; Senn, P.; et al. Cochlear Implants in Single-Sided Deafness—Clinical Results of a Swiss Multicentre Study. Swiss Med. Wkly. 2019, 149, w20171. [Google Scholar] [CrossRef] [PubMed]
- Saraç, E.T.; Batuk, M.O.; Sennaroglu, G. Evaluation of the Quality of Life in Adults with Cochlear Implants: As Good as the Healthy Adults? Am. J. Otolaryngol. 2019, 40, 720–723. [Google Scholar] [CrossRef] [PubMed]
- Sousa, A.F.; Couto, M.I.V.; Martinho-Carvalho, A.C. Quality of Life and Cochlear Implant: Results in Adults with Postlingual Hearing Loss. Braz. J. Otorhinolaryngol. 2018, 84, 494–499. [Google Scholar] [CrossRef]
- Issing, C.; Baumann, U.; Pantel, J.; Stöver, T. Cochlear Implant Therapy Improves the Quality of Life in Older Patients—A Prospective Evaluation Study. Otol. Neurotol. 2020, 41, 1214–1221. [Google Scholar] [CrossRef]
- Issing, C.; Holtz, S.; Loth, A.G.; Baumann, U.; Pantel, J.; Stöver, T. Long-Term Effects on the Quality of Life Following Cochlear Implant Treatment in Older Patients. Eur. Arch. Otorhinolaryngol. 2022, 279, 5135–5144. [Google Scholar] [CrossRef]
- Völter, C.; Götze, L.; Dazert, S.; Falkenstein, M.; Thomas, J.P. Can Cochlear Implantation Improve Neurocognition in the Aging Population? Clin. Interv. Aging 2018, 13, 701–712. [Google Scholar] [CrossRef]
- Forli, F.; Turchetti, G.; Giuntini, G.; Bellelli, S.; Fortunato, S.; Bruschini, L.; Barillari, M.R.; Berrettini, S. Cochlear Implant in Prelingually Deafened Oralist Adults: Speech Perception Outcomes, Subjective Benefits and Quality of Life Improvement. Acta Otorhinolaryngol. Ital. 2017, 37, 416–422. [Google Scholar] [CrossRef]
- Piromchai, P.; Tanamai, N.; Kiatthanabumrung, S.; Kaewsiri, S.; Thongyai, K.; Atchariyasathian, V.; Thanawirattananit, P.; Wacharasindhu, C.; Mukkun, T.; Isipradit, P.; et al. Multicentre Cohort Study of Cochlear Implantation Outcomes in Thailand. BMJ Open 2021, 11, e054041. [Google Scholar] [CrossRef]
- Hendriksma, M.; Bruijnzeel, H.; Bezdjian, A.; Kay-Rivest, E.; Daniel, S.J.; Topsakal, V. Quality of Life (QoL) Evaluation of Children Using Cochlear Implants: Agreement between Pediatric and Parent Proxy-QoL Reports. Cochlear Implant. Int. 2020, 21, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Aldriweesh, B.; Alharbi, M.; Alzahrani, M. Correlation of Quality of Life with Speech and Hearing Performance after Pediatric Cochlear Implantation. Int. J. Pediatr. Otorhinolaryngol. 2021, 150, 110889. [Google Scholar] [CrossRef] [PubMed]
- Dev, A.N.; Nahas, G.; Pappas, A.; Ambrose, T.; Craun, P.; Fustos, E.; Reilly, B.K.; Preciado, D. Underinsurance in Children Is Associated with Worsened Quality of Life after Cochlear Implantation. Int. J. Pediatr. Otorhinolaryngol. 2022, 157, 111119. [Google Scholar] [CrossRef]
- Vermi Sli Peker, S.; Demi, R.K.F.; Cukurova, I. Quality of Life and Parental Care Burden in Cochlear Implanted Children: A Case-Control Study. Int. J. Pediatr. Otorhinolaryngol. 2020, 136, 110164. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, A.; Özmen, M.; Iezzi, A.; Richardson, J. Deriving Population Norms for the AQoL-6D and AQoL-8D Multi-Attribute Utility Instruments from Web-Based Data. Qual. Life Res. 2016, 25, 3209–3219. [Google Scholar] [CrossRef] [PubMed]
- Hawthorne, G.; Osborne, R. Population Norms and Meaningful Differences for the Assessment of Quality of Life (AQoL) Measure. Aust. N. Z. J. Public. Health 2005, 29, 136–142. [Google Scholar] [CrossRef] [PubMed]
- MED-EL. Medical Electronics Indications—MED-EL Pro. Available online: https://www.medel.pro/indications (accessed on 16 April 2023).
- Clark, J.G. Degree of Hearing Loss. Available online: https://www.asha.org/public/hearing/degree-of-hearing-loss/ (accessed on 9 August 2022).
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation Coefficients: Appropriate Use and Interpretation. Anesth. Analg. 2018, 126, 1763. [Google Scholar] [CrossRef] [PubMed]
- Khadka, J.; Kwon, J.; Petrou, S.; Lancsar, E.; Ratcliffe, J. Mind the (Inter-Rater) Gap. An Investigation of Self-Reported versus Proxy-Reported Assessments in the Derivation of Childhood Utility Values for Economic Evaluation: A Systematic Review. Soc. Sci. Med. 2019, 240, 112543. [Google Scholar] [CrossRef]
- Rauch, A.-K.; Arndt, S.; Aschendorff, A.; Beck, R.; Speck, I.; Ketterer, M.C.; Jakob, T.F.; Hassepass, F. Long-Term Results of Cochlear Implantation in Children with Congenital Single-Sided Deafness. Eur. Arch. Otorhinolaryngol. 2021, 278, 3245–3255. [Google Scholar] [CrossRef]
- Falcón Benítez, N.; Falcón González, J.C.; Ramos Macías, Á.; Borkoski Barreiro, S.; Ramos de Miguel, Á. Cochlear Implants in Single-Sided Deafness. Comparison Between Children and Adult Populations with Post-Lingually Acquired Severe to Profound Hearing Loss. Front. Neurol. 2021, 12, 760831. [Google Scholar] [CrossRef]
- Beijen, J.-W.; Snik, A.F.M.; Mylanus, E.A.M. Sound Localization Ability of Young Children with Bilateral Cochlear Implants. Otol. Neurotol. 2007, 28, 479. [Google Scholar] [CrossRef] [PubMed]
- Galvin, K.L.; Hughes, K.C.; Mok, M. Can Adolescents and Young Adults with Prelingual Hearing Loss Benefit from a Second, Sequential Cochlear Implant? Int. J. Audiol. 2010, 49, 368–377. [Google Scholar] [CrossRef] [PubMed]
- Cleveland Clinic. Medical Professional Unilateral Hearing Loss (Single-Sided Deafness): Symptoms & Management. Available online: https://my.clevelandclinic.org/health/diseases/21625-unilateral-hearing-loss-single-sided-deafness (accessed on 12 April 2023).
- Wick, C.C.; Kallogjeri, D.; McJunkin, J.L.; Durakovic, N.; Holden, L.K.; Herzog, J.A.; Firszt, J.B.; Buchman, C.A. Hearing and Quality-of-Life Outcomes After Cochlear Implantation in Adult Hearing Aid Users 65 Years or Older: A Secondary Analysis of a Nonrandomized Clinical Trial. JAMA Otolaryngol. Head Neck Surg. 2020, 146, 925–932. [Google Scholar] [CrossRef] [PubMed]
- Marx, M.; Mosnier, I.; Venail, F.; Mondain, M.; Uziel, A.; Bakhos, D.; Lescanne, E.; N’Guyen, Y.; Bernardeschi, D.; Sterkers, O.; et al. Cochlear Implantation and Other Treatments in Single-Sided Deafness and Asymmetric Hearing Loss: Results of a National Multicenter Study Including a Randomized Controlled Trial. Audiol. Neurootol. 2021, 26, 414–424. [Google Scholar] [CrossRef] [PubMed]
- Moschner, D.B. Forschen mit Jungen Kindern—Eine Herausforderung; Universität Oldenburg: Oldenburg, Germany, 2012. [Google Scholar]
- Tajudeen, B.A.; Waltzman, S.B.; Jethanamest, D.; Svirsky, M.A. Speech Perception in Congenitally Deaf Children Receiving Cochlear Implants in the First Year of Life. Otol. Neurotol. 2010, 31, 1254–1260. [Google Scholar] [CrossRef] [PubMed]
- Colletti, L.; Mandalà, M.; Zoccante, L.; Shannon, R.V.; Colletti, V. Infants versus Older Children Fitted with Cochlear Implants: Performance over 10 Years. Int. J. Pediatr. Otorhinolaryngol. 2011, 75, 504–509. [Google Scholar] [CrossRef] [PubMed]
- Naik, A.N.; Varadarajan, V.V.; Malhotra, P.S. Early Pediatric Cochlear Implantation: An Update. Laryngoscope Investig. Otolaryngol. 2021, 6, 512–521. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Search Steps | Search Terms | Hits |
|---|---|---|
| 1 | ((Quality of Life) AND (cochlea * implant *)) | 903 |
| 2 | Limit NOT (Health Related Quality of Life) | 903 |
| 3 | Filter: last five years for recent data (from 05/07/2017 to 05/07/2022) | 386 |
| Inclusion Criteria | |
| Population | Subjects of any age, gender, or ethnicity with any hearing loss or single-sided deafness (SSD), as well as and their legal representatives |
| Intervention/treatment | Cochlear implantation |
| Comparator | Not applicable |
| Outcomes | Generic quality of life scores |
| Study design | All studies with original data, including case series, case–control, and longitudinal studies. Systematic reviews without original data, as well as acknowledgements, recommendations, or general topic descriptions were excluded. |
| Exclusion Criteria | |
| Different device or treatment Not a clinical study in humans Other type of hearing loss (not SNHL, MHL, or SSD) Topic not related to hearing loss or its treatment Publication lacking sufficient information for evaluation Overlap of data | |
| Range | Category | Evaluation Time | Mean Score | SD | Median | Range | n Specific Test for | Age Mean [years] | Age SD [years] | n Whole Study Cohort | n Publications Included | Publications | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean Values | Median Values | ||||||||||||
| 1. GBI (=Glasgow Benefit Inventory) | |||||||||||||
| −100 to +100 | Total | Postoperative | 39.6 | 9.99 | - | - | 240 | - | 56.4 | 11.6 | 280 | 6 | Anzivino et al., 2019 [22] Calvino et al., 2022 [23] Hey et al., 2019 [24] Sivonen et al., 2021 [25] Sorrentino et al., 2020 [26] Tang et al., 2017 [27] |
| General | 51.19 | 14.40 | 25 | 10.8–33.33 | 322 | 27 | 57.0 | 11.2 | 391 | 7 | Calvino et al., 2022 [23] Forli et al., 2019 [28] Hey et al., 2019 [24] Peters et al., 2021 [29] Sivonen et al., 2021 [25] Sorrentino et al., 2020 [26] Tang et al., 2017 [27] | ||
| Social | 28.65 | 11.86 | 0 | 0–8.33 | |||||||||
| Physical | 13.70 | 17.79 | 0 | 0–0 | |||||||||
| Total | postoperative short term (<12 months) | 38.00 | 9.80 | - | - | 67 | 63.6 | 2.9 | 70 | 2 | Anzivino et al., 2019 [22] Hey et al., 2019 [24] | ||
| General | 38.80 | 27.70 | 25 | 10.8–33.33 | 42 | 27 | 57.0 | 3.8 | 74 | 2 | Hey et al., 2019 [24] Peters et al., 2021 [29] | ||
| Social | 10.50 | 29.70 | 0 | 0–8.33 | |||||||||
| Physical | 3.20 | 15.70 | 0 | 0–0 | |||||||||
| Total | postoperative long term (≥12 months) | 40.06 | 10.00 | - | - | 173 | - | 54.0 | 12.4 | 210 | 4 | Calvino et al., 2022 [23] Sivonen et al., 2021 [25] Sorrentino et al., 2020 [26] Tang et al., 2017 [27] | |
| General | 52.43 | 14.54 | 280 | 57.0 | 12.3 | 317 | 5 | Calvino et al., 2022 [23] Forli et al., 2019 [28] Sivonen et al., 2021 [25] Sorrentino et al., 2020 [26] Tang et al., 2017 [27] | |||||
| Social | 30.46 | 10.88 | |||||||||||
| Physical | 14.75 | 18.33 | |||||||||||
| 2. WHOQOL (=World Health Organisation, Quality of Life) | |||||||||||||
| WHOQOL-BREF (short form) | |||||||||||||
| 0–100 | Total | Postoperative | 66.00 | 11.75 | - | - | 97 | - | 44.4 | 3.6 | 97 | 4 | Chen et al., 2022 [30] Peter et al., 2019 [31] Saraç et al., 2019 [32] Sousa et al., 2018 [33] |
| Environment | 59.70 | 4.60 | |||||||||||
| Social realitionships | 59.17 | 7.93 | |||||||||||
| Physical health | 63.50 | 6.82 | |||||||||||
| Psychosocial health | 61.40 | 10.09 | |||||||||||
| WHOQOL-OLD (for old age) | |||||||||||||
| 0–100 | Total | Preoperative | 60.00 | 15.70 | - | - | 34 | - | 73.5 | 4.9 | 34 | 1 | Issing et al., 2020 [34] |
| Sensory Abilities | 38.10 | 22.60 | |||||||||||
| Autonomy | 63.20 | 17.60 | |||||||||||
| Past, Present, Future Activities | 66.20 | 18.00 | |||||||||||
| Social Participation | 61.40 | 21.00 | |||||||||||
| Death and Dying | 61.90 | 30.00 | |||||||||||
| Intimacy | 69.30 | 20.20 | |||||||||||
| Total | Postoperative | 69.04 | 3.41 | - | - | 151 | - | 71.5 | 4.1 | 178 | 3 | Issing et al., 2020 [34] Issing et al., 2022 [35] Völter et al., 2018 [36] | |
| Sensory Abilities | 55.18 | 1.65 | - | - | 118 | - | 74.4 | 0.9 | 118 | 2 | Issing et al., 2020 [34] Issing et al., 2022 [35] | ||
| Autonomy | 69.80 | 3.36 | |||||||||||
| Past, Present, Future Activities | 71.63 | 3.00 | |||||||||||
| Social Participation | 68.90 | 2.49 | |||||||||||
| Death and Dying | 65.53 | 5.69 | |||||||||||
| Intimacy | 73.73 | 1.39 | |||||||||||
| 3. SF-36 (=Short Form Health Survey with 36 items) | |||||||||||||
| 0–100 | Physical health | Preoperative | 61.51 | 13.21 | - | - | 55 | - | 56.2 | 10.2 | 55 | 2 | Anzivino et al., 2019 [22] Chen et al., 2022 [30] |
| Mental health | 55.05 | 2.06 | |||||||||||
| Physical Functioning | - | - | 57.20 | 55.1–57.2 | - | 30 | median: 35 | range: 16–54 | 30 | 1 | Forli et al., 2017 [37] | ||
| Role-Physical | 56.20 | 49.2–56.2 | |||||||||||
| Body Pain | 62.80 | 47.3–62.8 | |||||||||||
| General Health | 57.90 | 50.9–61.7 | |||||||||||
| Vitality | 53.80 | 46.7–60.9 | |||||||||||
| Social Functioning | 46.30 | 35.4–57.2 | |||||||||||
| Role-Emotional | 55.30 | 44.8–55.3 | |||||||||||
| Mental Health | 45.90 | 39.1–55.0 | |||||||||||
| Physical health | Postoperative | 69.20 | 9.30 | - | - | 55 | - | 56.2 | 10.2 | 55 | 2 | Anzivino et al., 2019 [22] Chen et al., 2022 [30] | |
| Mental health | 66.43 | 5.37 | |||||||||||
| Physical Functioning | - | - | 57.20 | 55.1–57.2 | - | 30 | median: 35 | range: 16–54 | 30 | 1 | Forli et al., 2017 [37] | ||
| Role-Physical | 56.20 | 49.2–56.2 | |||||||||||
| Body Pain | 62.80 | 51.6–62.8 | |||||||||||
| General Health | 60.30 | 54.6–61.7 | |||||||||||
| Vitality | 56.20 | 51.1–63.3 | |||||||||||
| Social Functioning | 49.00 | 40.9–57.1 | |||||||||||
| Role-Emotional | 55.30 | 55.3–55.3 | |||||||||||
| Mental Health | 52.70 | 45.9–55.0 | |||||||||||
| 4. GHSI (=Glasgow Health Status Inventory) | |||||||||||||
| −100 to +100 | Total | postoperative | 66.00 | 2.00 | 23 | 44.2 | range: 19.5–64.8 | 27 | 1 | Sivonen et al., 2021 [25] | |||
| 5. EQ-5D-5L (=European Quality of Life in 5 Dimensions, 5 Level Version) | |||||||||||||
| 0–5 | Mobility | postoperative shortterm (<12 months) | 1.65 | 0.95 | - | - | 20 | - | 3.0 | 5.8 | 458 | 1 | Piromchai et al., 2021 [38] |
| Self-care | 1.15 | 0.67 | |||||||||||
| Usual activities | 1.45 | 0.83 | |||||||||||
| Pain/discomfort | 1.55 | 0.60 | |||||||||||
| Anxiety/depression | 1.65 | 0.99 | |||||||||||
| Mobility | postoperative longterm (≥12 months) | 1.29 | 0.59 | - | - | 17 | |||||||
| Self-care | 1.12 | 0.33 | |||||||||||
| Usual activities | 1.47 | 0.72 | |||||||||||
| Pain/discomfort | 1.47 | 0.51 | |||||||||||
| Anxiety/depression | 1.18 | 0.39 | |||||||||||
| 6. HUI 3 (=Health Utilities Index) | |||||||||||||
| 0–1 | Total | preoperative | 0.56 | - | - | - | 59 | - | 72.3 | 6.8 | 59 | 1 | Sarant et al., 2019 [16] |
| postoperative | 0.67 | - | 20 | ||||||||||
| 7. AQoL-8D (=Assessment of Quality of Life in 8 Dimensions) | |||||||||||||
| 0–1 | Total | Preoperative | 0.50 | 0.23 | - | 0.17–0.99 | 104 | - | 34.8 | 16.6 | 104 | 1 | Rostkowska et al., 2021 [15] |
| Physical superdimension | 0.50 | 0.20 | 0.15–0.91 | ||||||||||
| Psycho-social superdimension | 0.27 | 0.19 | 0.05–0.92 | ||||||||||
| Independent living | 0.78 | 0.15 | 0.39–1 | ||||||||||
| Pain | 0.76 | 0.24 | 0.15–1 | ||||||||||
| Senses | 0.53 | 0.18 | 0.25–0.97 | ||||||||||
| Mental health | 0.53 | 0.16 | 0.25–1 | ||||||||||
| Happiness | 0.64 | 0.18 | 0.24–1 | ||||||||||
| Coping | 0.72 | 0.17 | 0.38–1 | ||||||||||
| Relationships | 0.60 | 0.14 | 0.47–1 | ||||||||||
| Self-worth | 0.64 | 0.21 | 0.28–1 | ||||||||||
| Total | Postoperative | 0.66 | 0.19 | - | 0.21–0.99 | ||||||||
| Physical superdimension | 0.62 | 0.20 | 0.18–0.96 | ||||||||||
| Psycho-social superdimension | 0.37 | 0.18 | 0.09–1 | ||||||||||
| Independent living | 0.86 | 0.14 | 0.35–1 | ||||||||||
| Pain | 0.78 | 0.22 | 0.21–1 | ||||||||||
| Senses | 0.71 | 0.16 | 0.35–0.97 | ||||||||||
| Mental health | 0.60 | 0.13 | 0.29–1 | ||||||||||
| Happiness | 0.73 | 0.13 | 0.36–1 | ||||||||||
| Coping | 0.80 | 0.12 | 0.52–1 | ||||||||||
| Relationships | 0.70 | 0.14 | 0.47–1 | ||||||||||
| Self-worth | 0.81 | 0.14 | 0.39–1 | ||||||||||
| Range | Category | Evaluation Time | Mean Score | SD | Median | Range | n Specific Test for | Age Mean [years] | Age SD [years] | n Whole Study Cohort | n Publications Included | Publications | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean Values | Median Values | ||||||||||||
| 8. PedsQL (=Pediatric Quality of Life Inventory) | |||||||||||||
| 0–100 | Physical | postoperative shortterm (<12 months) | 74.59 | 23.67 | 23 | 2.96 | 5.83 | 458 | 1 | Piromchai et al., 2021 [38] | |||
| Emotional | 56.96 | 18.63 | |||||||||||
| Social | 50.22 | 22.94 | |||||||||||
| School | 50.94 | 32.08 | |||||||||||
| Total | postoperative longterm (≥12 months) | 87.08 | 11.10 | 79.31 | 34.78–100 | 73 | 34 | 4.79 | 1.22 | 107 | 2 | Alnuhayer et al., 2020 [1] Hendriksma et al., 2020 [39] | |
| Physical | 90.04 | 2.93 | 89.36 | 40.63–100 | 81 | 34 | 3.88 | 0.92 | 566 | 3 | Alnuhayer et al., 2020 [1] Hendriksma et al., 2020 [39] Piromchai et al., 2021 [38] | ||
| Emotional | 72.07 | 15.19 | 73.33 | 25–100 | |||||||||
| Social | 75.23 | 12.10 | 78.24 | 10–100 | |||||||||
| School | 66.20 | 14.53 | 76.50 | 37.5–100 | |||||||||
| 9. GCBI (=Glasgow Children’s Benefit Inventory) | |||||||||||||
| −100 to +100 | Total | postoperative | 58.12 | 5.89 | 127 | 3.54 | 0.24 | 127 | 2 | Aldriweesh et al., 2021 [40] Dev et al., 2022 [41] | |||
| Physical health | 44.30 | 14.10 | 57 | 3.30 | 1.9 | 57 | 1 | Dev et al., 2022 [41] | |||||
| Emotion | 68.10 | 13.20 | |||||||||||
| Learning | 78.90 | 10.70 | |||||||||||
| Vitality | 64.70 | 12.10 | |||||||||||
| 10. KINDL | |||||||||||||
| 0–100 | Total | postoperative | 46.90 | 12.00 | 34 | 5.33 | 0.98 | 34 | 1 | Vermi Sli Peker et al., 2020 [42] | |||
| Physical well-being | 67.70 | 16.20 | |||||||||||
| Self-esteem | 42.70 | 22.70 | |||||||||||
| School/Kindergarten | 41.20 | 22.10 | |||||||||||
| Social Relations (Friends) | 45.40 | 17.90 | |||||||||||
| Emotional Well-Being | 41.00 | 17.10 | |||||||||||
| Family | 44.90 | 19.10 | |||||||||||
| Frequency (kHz) | Hearing Threshold, Mean (dB) | SD | n (Ears) | Degree of Hearing Loss according to ASHA |
|---|---|---|---|---|
| 0.25 | 24.4 | 2.62 | 55 | Slight HL |
| 0.5 | 26.3 | 3.47 | 56 | Mild HL |
| 1 | 24.6 | 4.06 | 55 | Slight HL |
| 2 | 24.6 | 2.34 | 55 | Slight HL |
| 4 | 26.8 | 2.21 | 51 | Mild HL |
| 6 | 27.3 | 1.52 | 45 | Mild HL |
| Properties | Scores |
|---|---|
| Participants (n) | 41 |
| Mean (%) | 71.6 |
| Standard deviation (%) | 23.8 |
| Minimum (%) | 15.1 |
| Maximum (%) | 100 |
| Comparison Parameters | Early Implantation ≤3 Years | n | Late Implantation >3 Years | n | p-Value | Significantly Different (p < 0.05) |
|---|---|---|---|---|---|---|
| AQoL-6D | 0.78 (0.19) | 37 | 0.81 (0.14) | 37 | 0.7252 | No |
| SSQ12 | 5.97 (1.79) | 41 | 6.13 (1.47) | 38 | 0.5995 | No |
| PTA | 25.6 dB (12.8 dB) | 27 | 21.2 dB (7.01 dB) | 20 | 0.1127 | No |
| HSM sentence test | 72.9% (24.5%) | 22 | 70.1% (23.5%) | 19 | 0.6283 | No |
| Correlation Parameter | n Pairs | Spearman ρ | Correlation Strength | p-Value | Correlation Significant (p < 0.05) |
|---|---|---|---|---|---|
| AQoL-6D and SSQ12 | 72 | 0.4370 | moderate | 0.0001 | Yes |
| AQoL-6D Senses and SSQ12 | 72 | 0.6739 | moderate | <0.0001 | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gundacker, G.; Trales, D.E.; Stefanescu, H.E. Quality of Life and Audiological Benefits in Pediatric Cochlear Implant Users in Romania: Systematic Review and Cohort Study. J. Pers. Med. 2023, 13, 1610. https://doi.org/10.3390/jpm13111610
Gundacker G, Trales DE, Stefanescu HE. Quality of Life and Audiological Benefits in Pediatric Cochlear Implant Users in Romania: Systematic Review and Cohort Study. Journal of Personalized Medicine. 2023; 13(11):1610. https://doi.org/10.3390/jpm13111610
Chicago/Turabian StyleGundacker, Gina, Delia Emilia Trales, and Horatiu Eugen Stefanescu. 2023. "Quality of Life and Audiological Benefits in Pediatric Cochlear Implant Users in Romania: Systematic Review and Cohort Study" Journal of Personalized Medicine 13, no. 11: 1610. https://doi.org/10.3390/jpm13111610
APA StyleGundacker, G., Trales, D. E., & Stefanescu, H. E. (2023). Quality of Life and Audiological Benefits in Pediatric Cochlear Implant Users in Romania: Systematic Review and Cohort Study. Journal of Personalized Medicine, 13(11), 1610. https://doi.org/10.3390/jpm13111610