

Vasopressin in Sepsis and Other Shock States: State of the Art


Abstract
:1. Introduction
- -
- AVP deficiency present in septic shock [7].
- -
- As a multimodal strategy for the sparing of catecholamines.
- -
- Its potential nephroprotective effect.
- -
- Early onset of AVP infusion.
2. Physiology
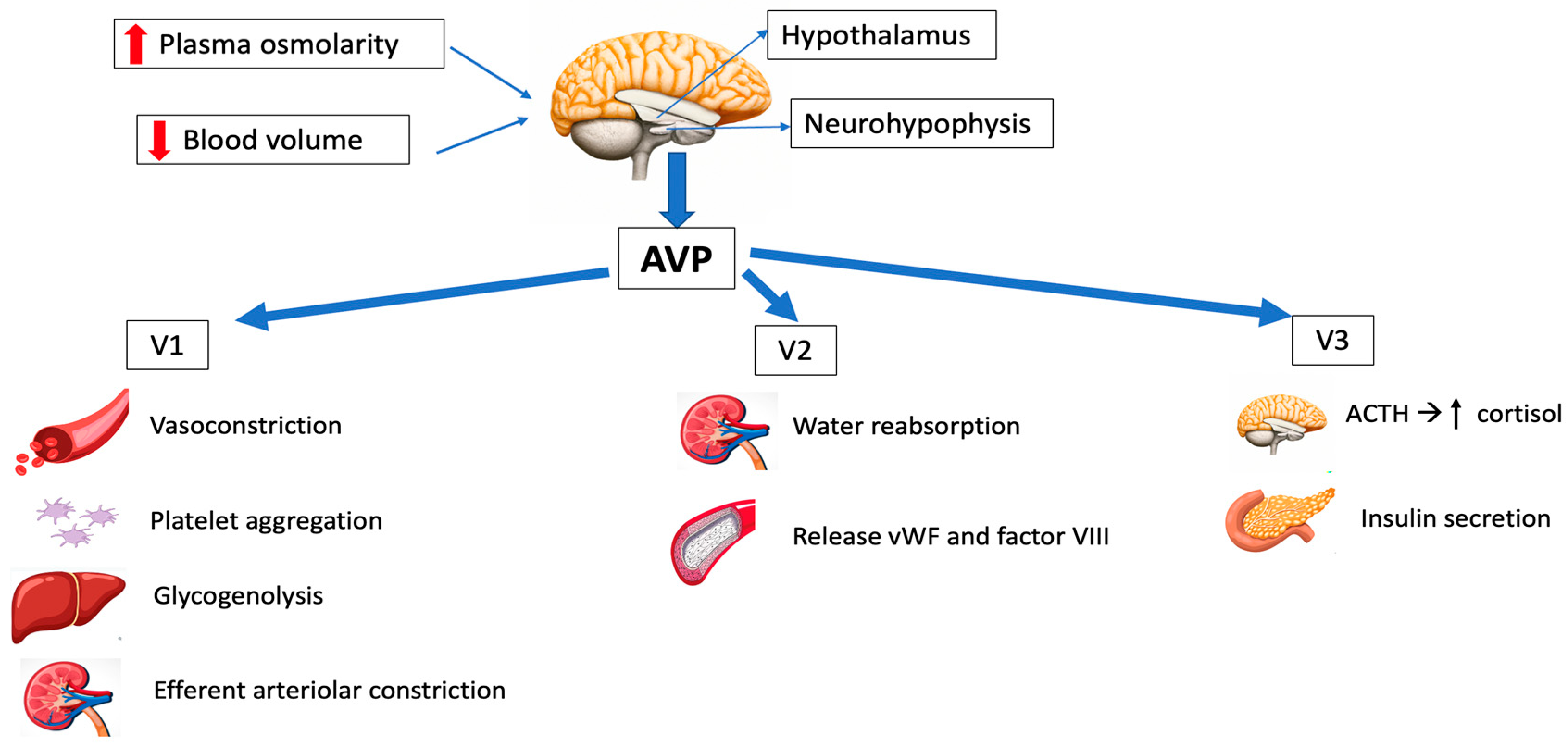
2.1. Synthesis and Release
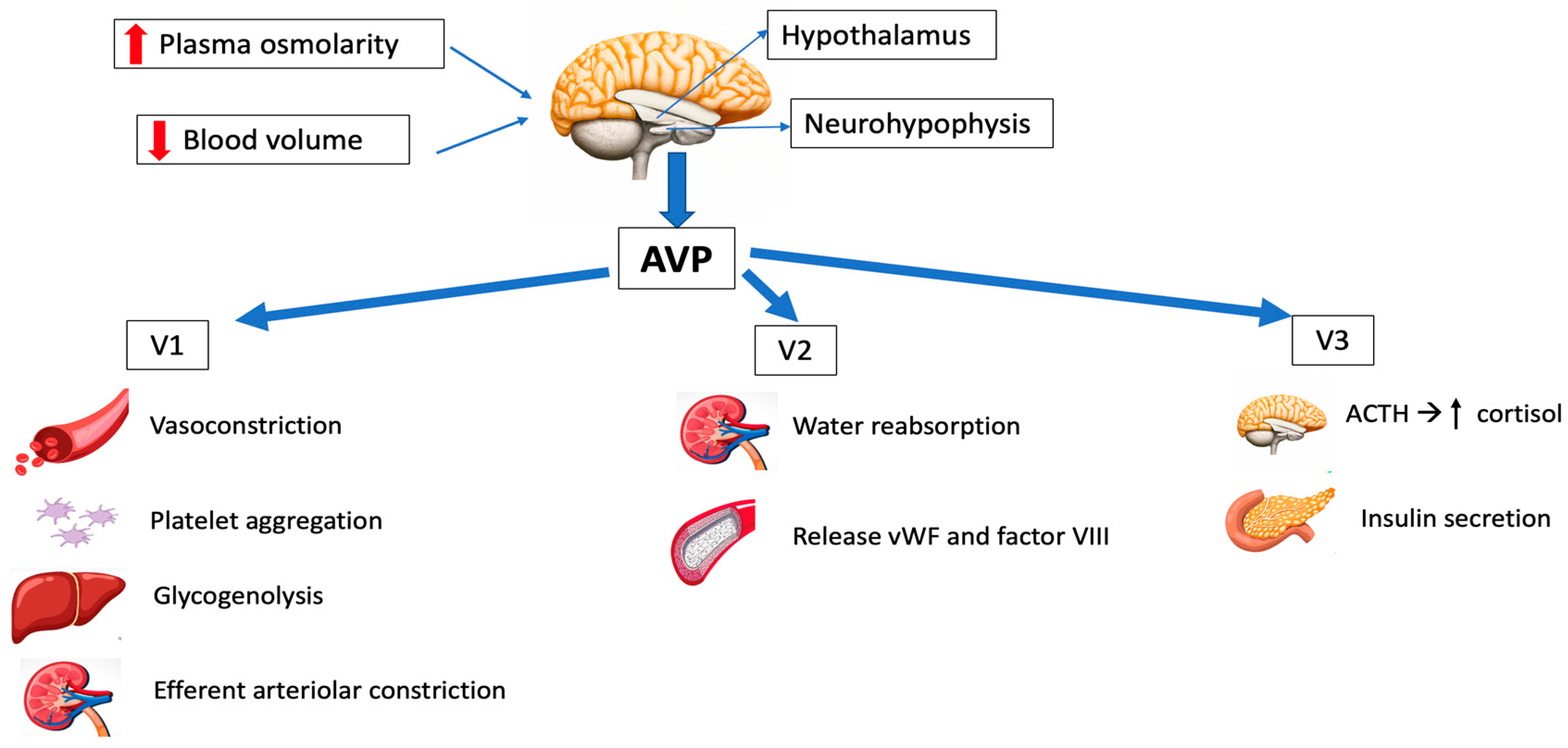
2.2. AVP Receptors and Signal Transduction
2.3. Physiological Functions
- -
- Osmoregulation
- -
- Cardiovascular control
- -
- Corticotropin secretion
- -
- Hemostasis
3. Pharmacology
- Arginine vasopressin (AVP) acts on the V1, V2 and V3 receptors, and has been employed in the management of refractory vasodilatory hypotension, cardiac arrest and septic shock. It has the great advantage of having a short half-life, so the dose can be easily titrated.
- Desmopressin acetate (DDAVP) is a synthetic agonist with V2 receptor specificity and was first used in management of central diabetes insipidus. By directly affecting the endothelial V2 receptors, DDAVP also raises the plasma factor VIII and vWF concentrations in healthy subjects.
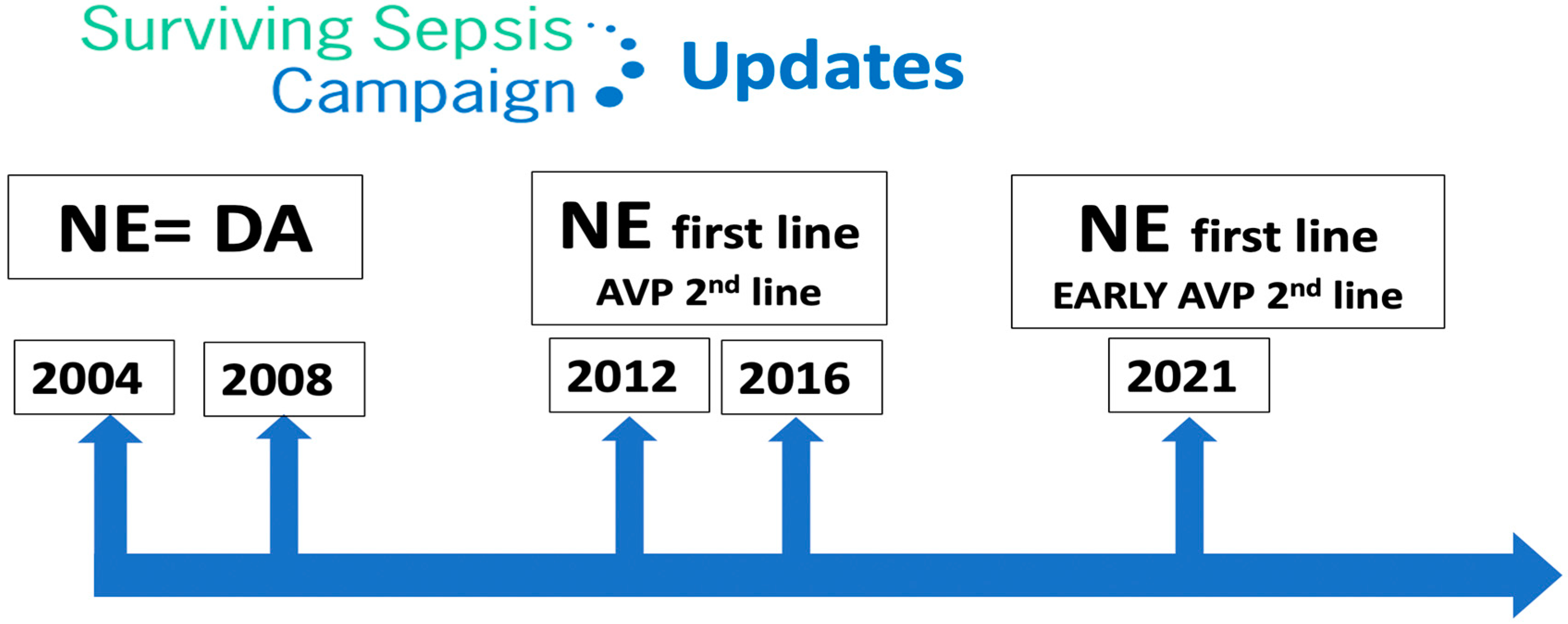
- Terlipressin (TP) has a greater selectivity for the V1 receptor than AVP. It is a prodrug of AVP and undergoes metabolism by exopeptidases to yield the active metabolite lysine vasopressin in the circulation, producing a “slow release” effect and affording a longer biological half-life (6 h). Terlipressin has been used as treatment for bleeding gastric second to esophageal varices, portal hypertension and septic shock. The drug increases blood pressure and improves the outcomes of hepatorenal syndrome (contracting the mesenteric arteries, resulting in decreased portal venous inflow and subsequently lowering portal pressure) [5]. The latest Surviving Sepsis Campaign (SSC) recommendations [21] do not advise its use in patients with septic shock, due to greater undesirable effects (more serious adverse events than NE, especially digital ischemia) [22,23].
- Selepressin, another synthetic vasopressin analog, is a short-acting selective V1 receptor agonist. It may present benefits compared to AVP due its ability to induce pure vasoconstriction; it also has reduced antidiuretic effects, a lower risk of thrombotic complications (because of reduced release of vWF) and affords superior protection from increased permeability. However, recently, a trial was stopped due to futility criteria, because no difference was observed in vasopressor- and ventilator-free days [24]. The drug is currently not approved for clinical use.
4. Vasopressin in Septic Shock
4.1. Pathophysiology of Peripheral Vasodilation in Septic Shock
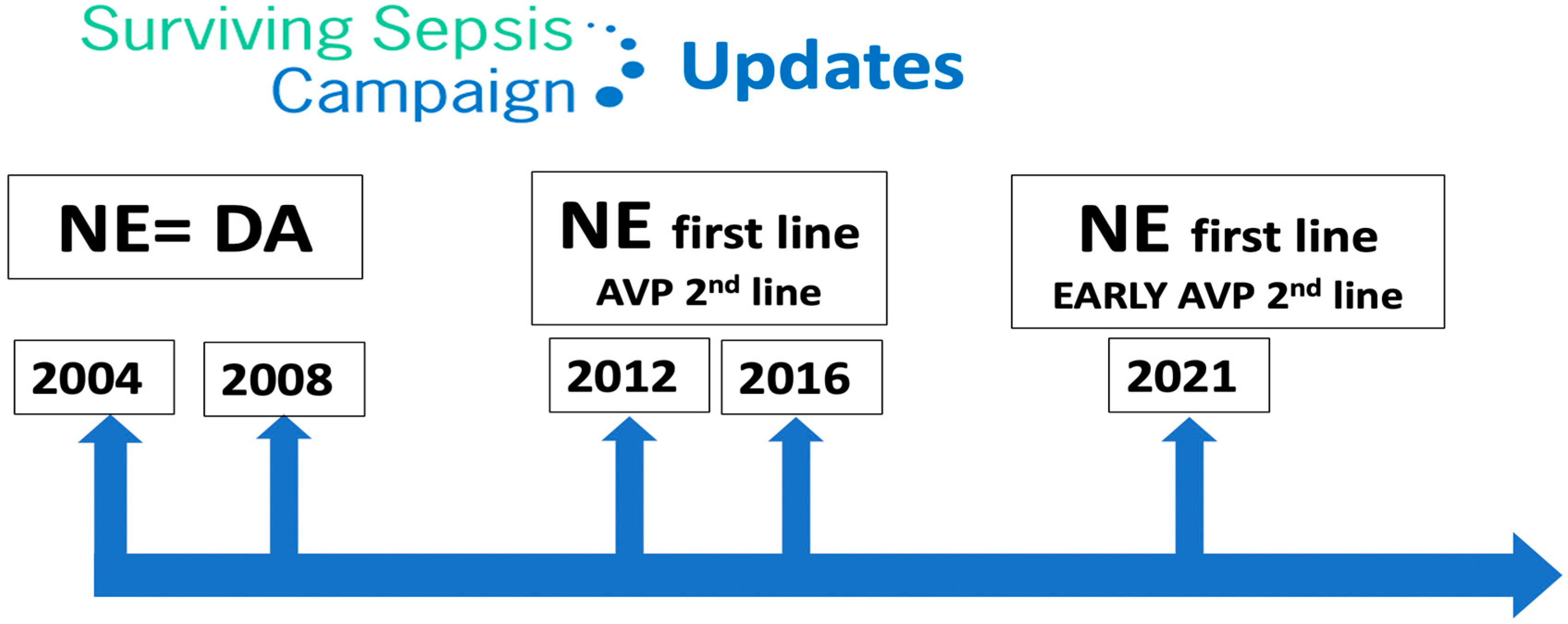
4.2. Treatment of Vasodilation in Septic Shock
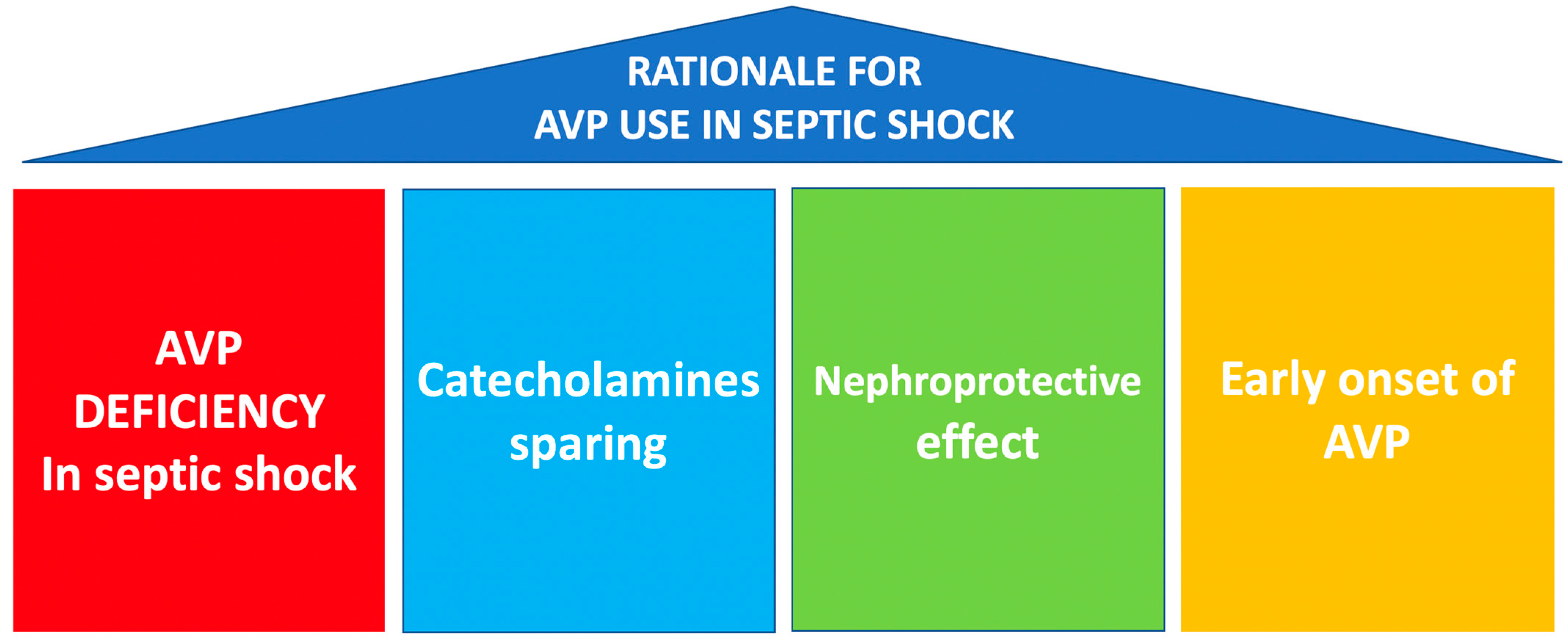
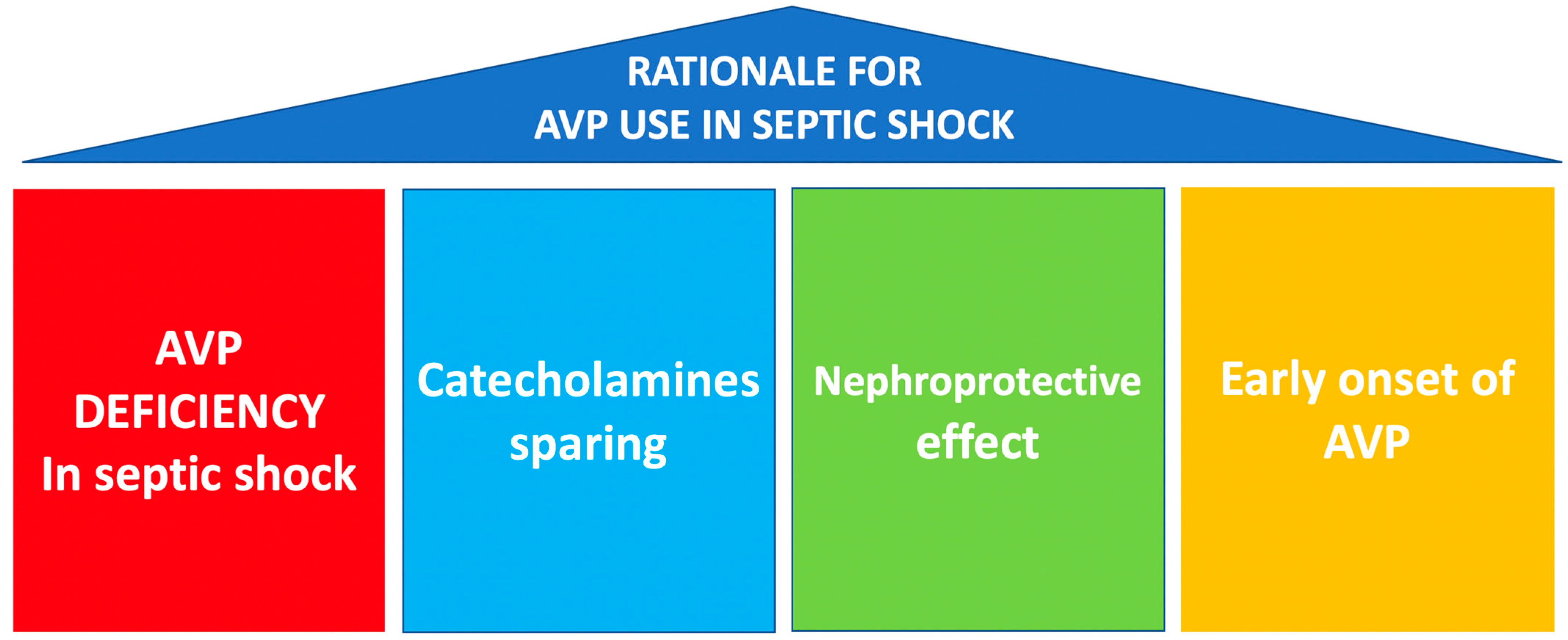
4.3. Rationale for AVP Use in Septic Shock
- AVP deficiency present in septic shock [6].
- As a multimodal strategy for the sparing of catecholamines.
- Its potential nephroprotective effect.
- Early onset of AVP infusion.
4.3.1. AVP Deficiency in Septic Shock
4.3.2. Sparing of Catecholamines/Decatecholaminization
- Adrenoceptors become less responsive or downregulated as a result of high circulating catecholamines levels [39], so vasodilation persists despite increased plasma catecholamine concentrations. Arginine vasopressin binds to V1 receptors and non-catecholamine receptors, causing vasoconstriction, and enhances vascular responsiveness to catecholamines [61].
- Arginine vasopressin can block the K-ATP channels and interfere with NO signaling, potentiating the effects of adrenergic drugs at vascular smooth muscle in shock states [62].
- AVP might also be considered in the presence of acidosis, as AVP receptor sensitivity tends to be relatively more preserved in an acidic environment when compared to adrenergic receptors [63].
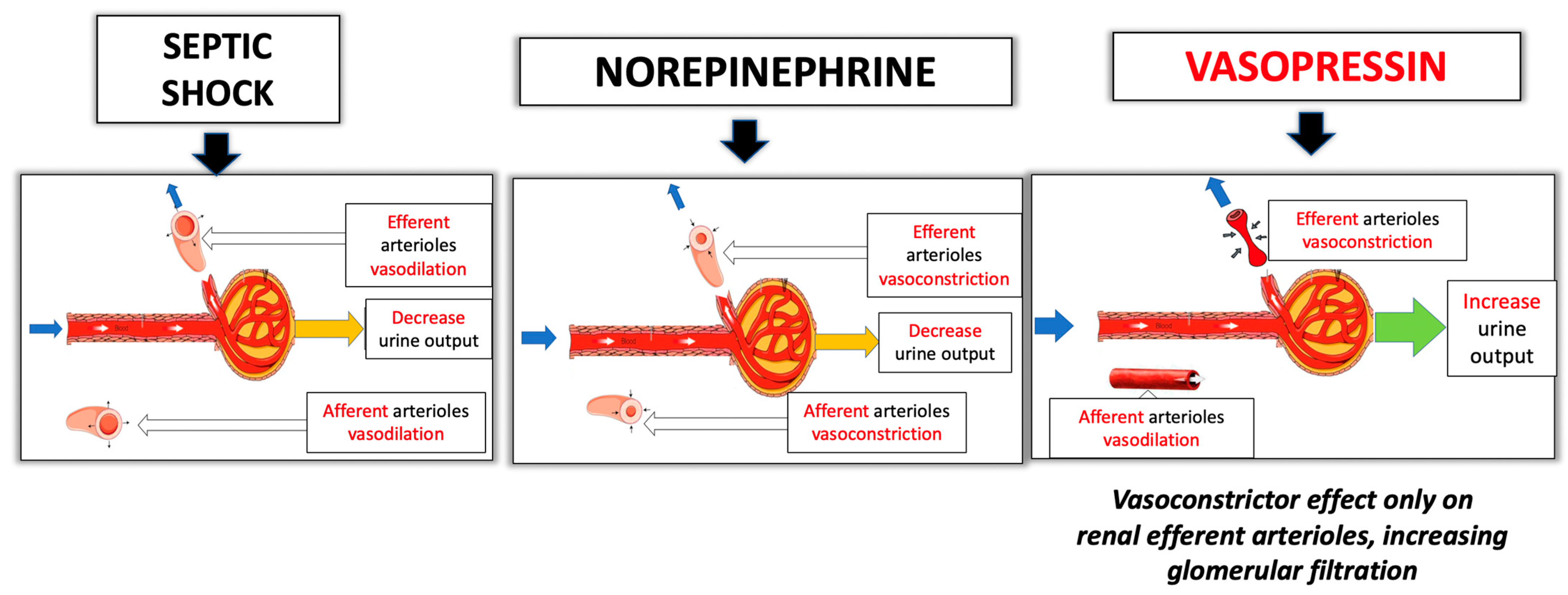
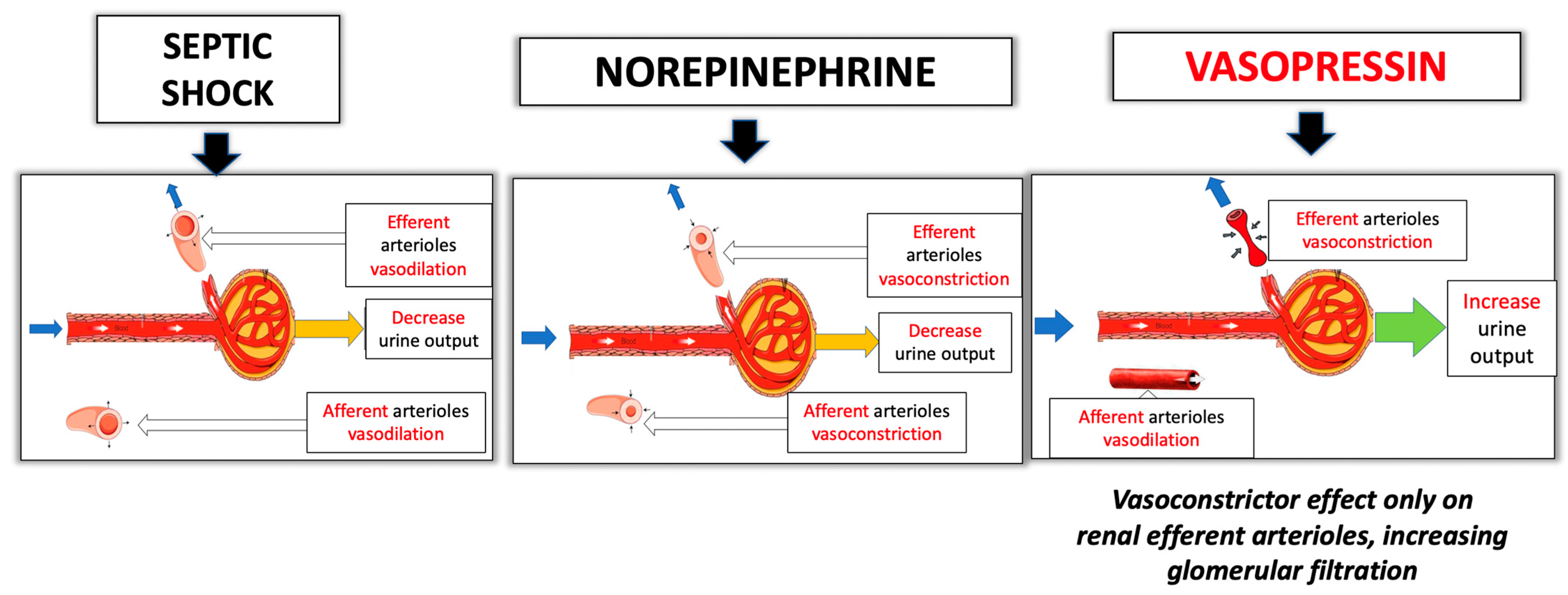
4.3.3. Nephroprotective Effect
4.3.4. Early onset of AVP Infusion
4.4. Interactions of AVP and Corticosteroid Treatment in Septic Shock
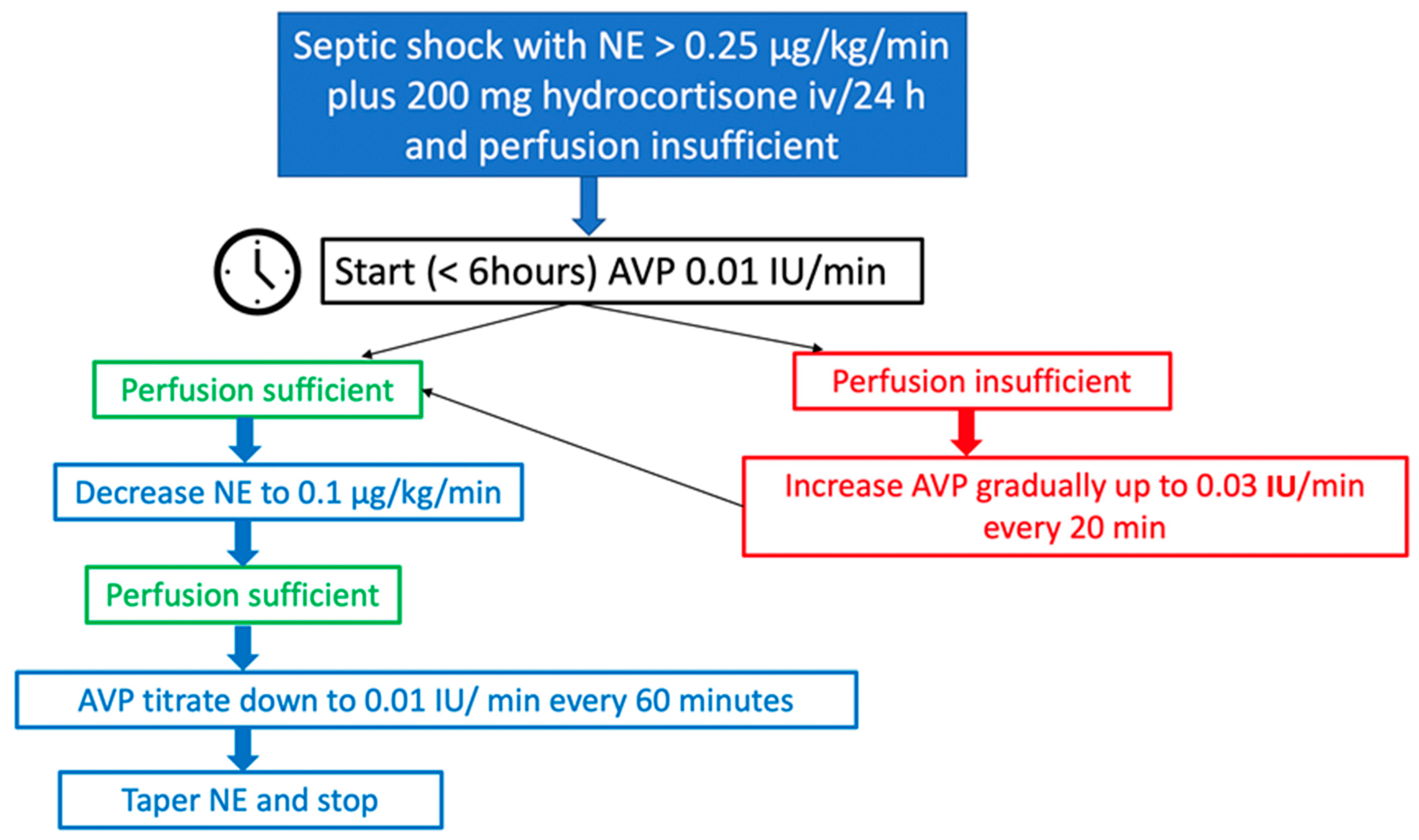
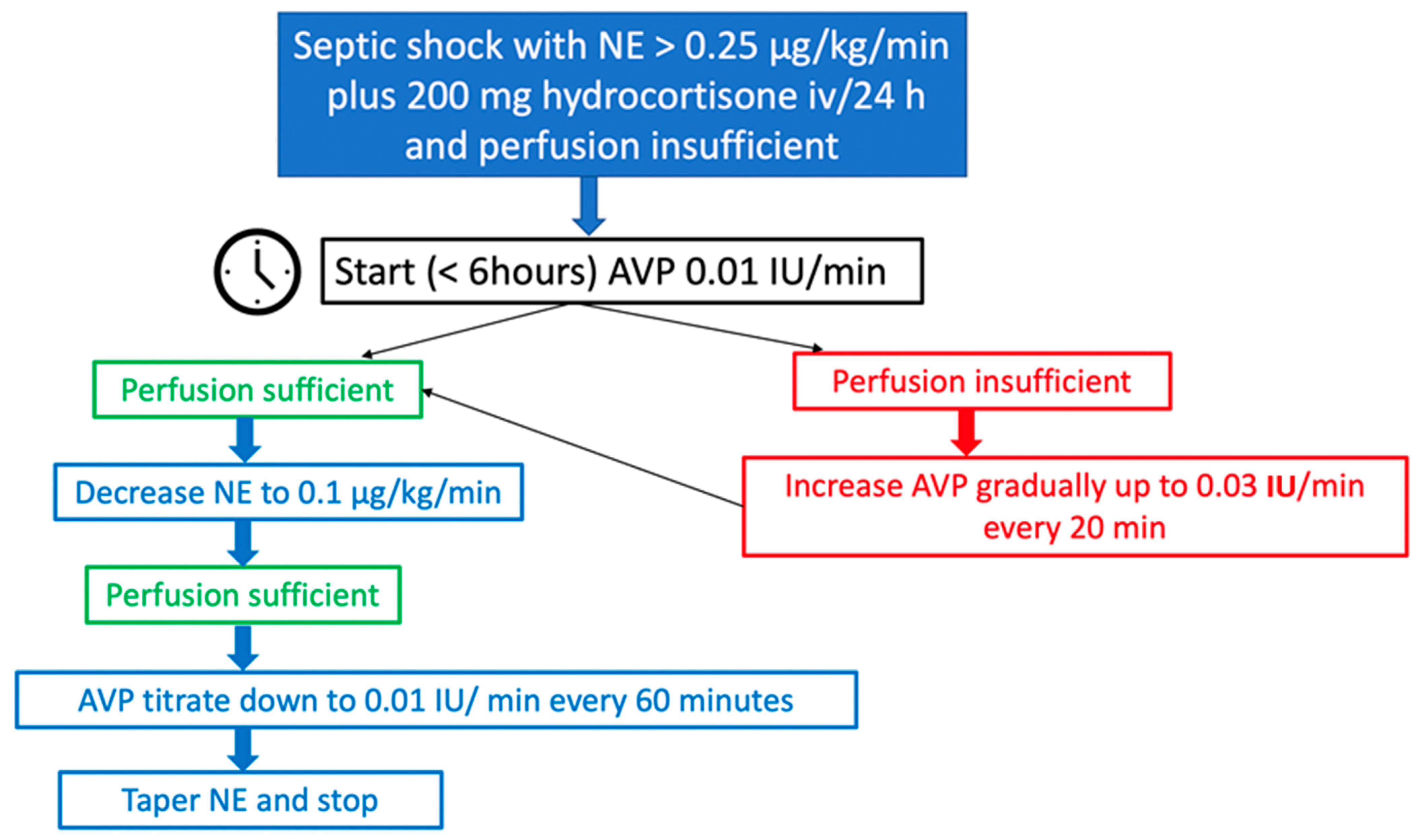
4.5. Personal Recommendations for the Use of AVP in Septic Shock in Clinical Practice
4.6. Use of Higher Doses of AVP in Septic Shock?
4.7. Future Directions
- Genetic variations in ARDβ2, which encodes the β2-adrenergic receptor, have been linked to higher mortality rates and greater organ dysfunction in septic shock (with greater NE requirements, increased renal, hematological, hepatic and neurologic dysfunction, and increased 28-day mortality) [101].
- Genetic variations in LNPEP (leucyl and cystinyl aminopeptidase), also known as vasopressinase, have been associated with higher plasma clearance of AVP, serum sodium regulation and increased 28-day mortality [102].
- It has been proposed that plasma AVP levels could serve as a guide for AVP therapy, aiming to target physiological levels while avoiding higher concentrations that may lead to adverse effects [103]. Nevertheless, the ideal serum AVP concentration for septic shock remains uncertain. Measuring plasma AVP levels presents challenges due to its short half-life and ex vivo instability. On the other hand, the copeptin, i.e., the C-terminal of AVP precursor, is stable in plasma, easier to assay than AVP and exhibits a strong correlation with AVP plasma concentration. Therefore, future studies are necessary to assess the potential utility of copeptin levels for guiding AVP therapy [81].
5. AVP in Vasodilatory Shock in Heart Surgery
5.1. Pathophysiology of Vasoplegic Shock in Heart Surgery
5.2. Rationale for AVP Use in Heart Surgery
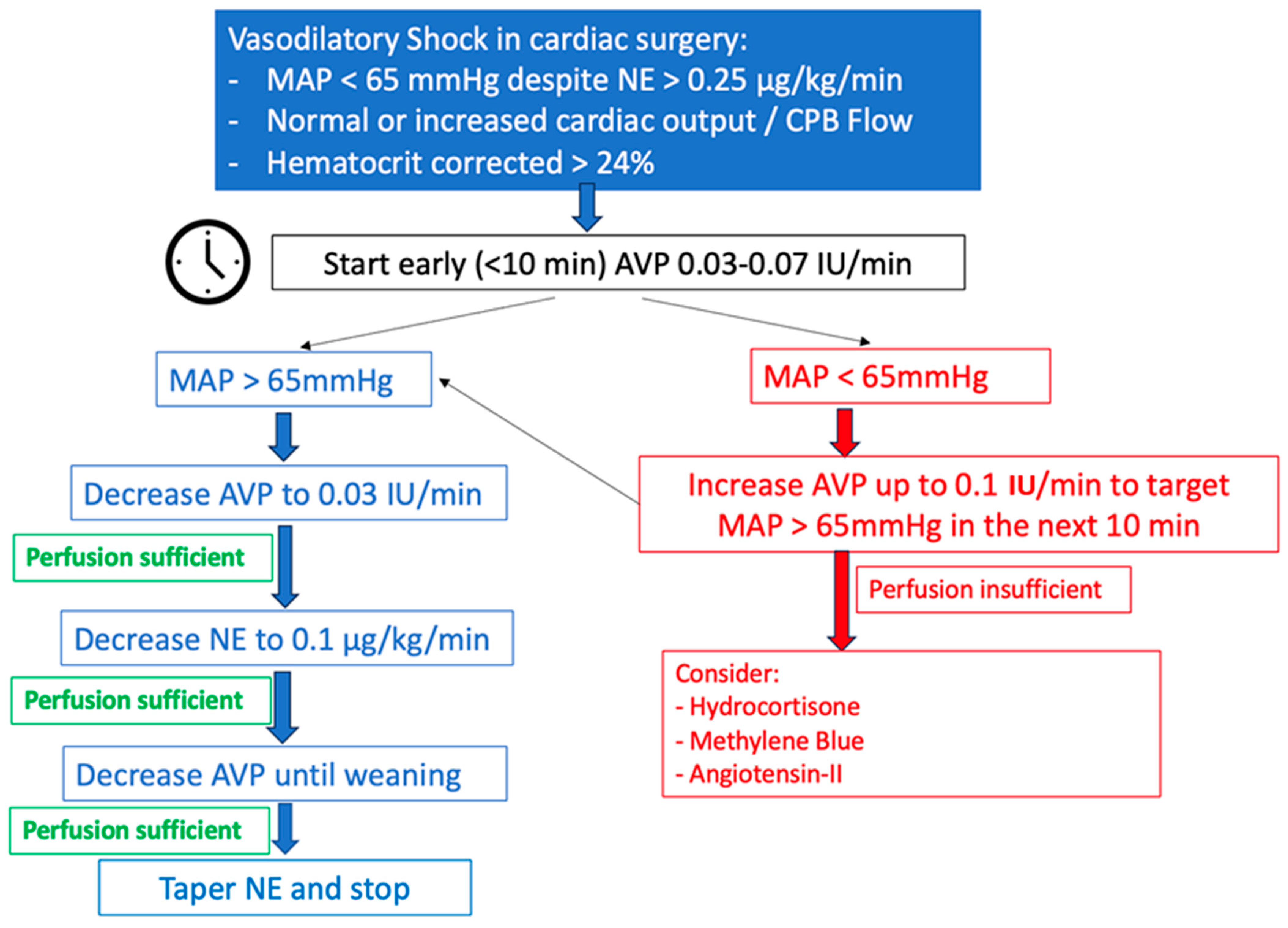
5.3. Personal Recommendations for the Use of AVP in Vasoplegic Syndrome in Heart Surgery (Figure 6)
5.3.1. Preoperative Period
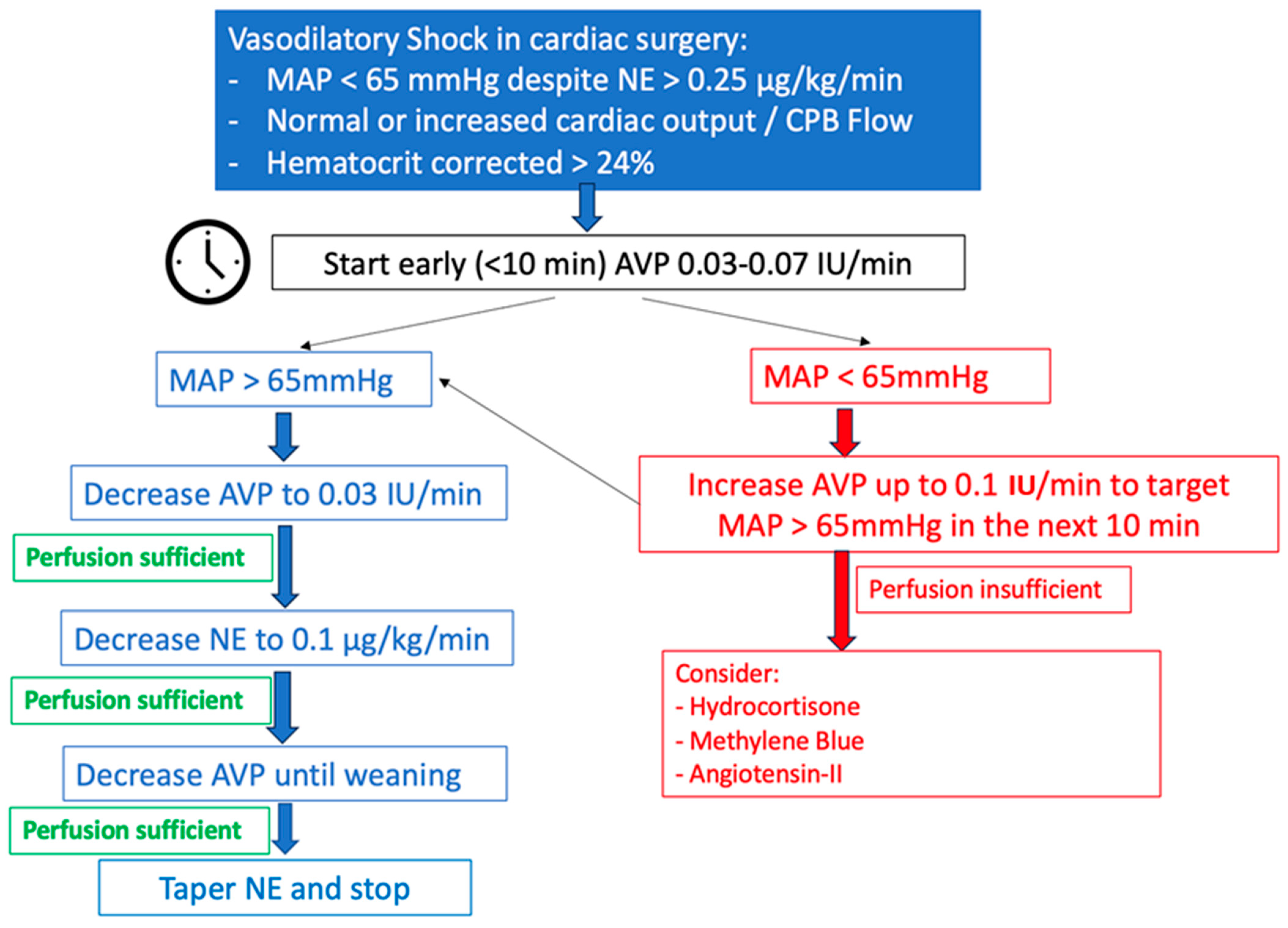
5.3.2. Intra- and Postoperative Period
5.3.3. Weaning from AVP
6. AVP in Cardiac Arrest
7. Authorized Indications and Dosages in Europe and the United States of America (USA)
8. Adverse Effects of AVP
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Oliver, G.; Schäfer, E.A. On the Physiological Action of Extracts of Pituitary Body and Certain Other Glandular Organs: Preliminary Communication. J. Physiol. 1895, 18, 277–279. [Google Scholar] [CrossRef] [PubMed]
- Dünser, M.W.; Lindner, K.H.; Wenzel, V. A Century of Arginine Vasopressin Research Leading to New Therapeutic Strategies. Anesthesiology 2006, 105, 444–445. [Google Scholar] [CrossRef]
- Czakó, L.; Mezei, G.; László, F.A. Treatment of Diabetes Insipidus with 1-Deamino-8-d-Arginine Vasopressin. Acta Med. Acad. Sci. Hung. 1975, 32, 75–84. [Google Scholar]
- Kehne, J.H.; Hughes, F.A.; Gompertz, M.L. The Use of Surgical Pituitrin in the Control of Esophageal Varix Bleeding; an Experimental Study and Report of Two Cases. Surgery 1956, 39, 917–925. [Google Scholar]
- Park, K.S.; Yoo, K.Y. Role of Vasopressin in Current Anesthetic Practice. Korean J. Anesthesiol. 2017, 70, 245. [Google Scholar] [CrossRef]
- Sharshar, T.; Blanchard, A.; Paillard, M.; Raphael, J.C.; Gajdos, P.; Annane, D. Circulating Vasopressin Levels in Septic Shock. Crit. Care Med. 2003, 31, 1752–1758. [Google Scholar] [CrossRef] [PubMed]
- Holmes, C.L.; Patel, B.M.; Russell, J.A.; Walley, K.R. Physiology of Vasopressin Relevant to Management of Septic Shock. Chest 2001, 120, 989–1002. [Google Scholar] [CrossRef] [PubMed]
- Treschan, T.A.; Peters, J.; Warltier, D.C. The Vasopressin System. Anesthesiology 2006, 105, 599–612. [Google Scholar] [CrossRef]
- Sklar, A.H.; Schrier, R.W. Central Nervous System Mediators of Vasopressin Release. Physiol. Rev. 1983, 63, 1243–1280. [Google Scholar] [CrossRef]
- Sai, Y.; Okamura, T.; Amakata, Y.; Toda, N. Comparison of Responses of Canine Pulmonary Artery and Vein to Angiotensin II, Bradykinin and Vasopressin. Eur. J. Pharmacol. 1995, 282, 235–241. [Google Scholar] [CrossRef]
- Evora, P.R.B.; Pearson, P.J.; Rodrigues, A.J.; Viaro, F.; Schaff, H.V. Effect of Arginine Vasopressin on the Canine Epicardial Coronary Artery: Experiments on V1-Receptor-Mediated Production of Nitric Oxide. Arq. Bras. Cardiol. 2003, 80, 483–494. [Google Scholar] [CrossRef]
- Rotondo, F.; Butz, H.; Syro, L.V.; Yousef, G.M.; Di Ieva, A.; Restrepo, L.M.; Quintanar-Stephano, A.; Berczi, I.; Kovacs, K. Arginine Vasopressin (AVP): A Review of Its Historical Perspectives, Current Research and Multifunctional Role in the Hypothalamo-Hypophysial System. Pituitary 2016, 19, 345–355. [Google Scholar] [CrossRef] [PubMed]
- Demiselle, J.; Fage, N.; Radermacher, P.; Asfar, P. Vasopressin and Its Analogues in Shock States: A Review. Ann. Intensive Care 2020, 10, 9. [Google Scholar] [CrossRef]
- Birnbaumer, M. The V2 Vasopressin Receptor Mutations and Fluid Homeostasis. Cardiovasc. Res. 2001, 51, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Pivonello, R.; De Bellis, A.; Faggiano, A.; Di Salle, F.; Petretta, M.; Di Somma, C.; Perrino, S.; Altucci, P.; Bizzarro, A.; Bellastella, A.; et al. Central Diabetes Insipidus and Autoimmunity: Relationship between the Occurrence of Antibodies to Arginine Vasopressin-Secreting Cells and Clinical, Immunological, and Radiological Features in a Large Cohort of Patients with Central Diabetes Insipidus of Known and Unknown Etiology. J. Clin. Endocrinol. Metab. 2003, 88, 1629–1636. [Google Scholar] [CrossRef]
- Christ-Crain, M.; Gaisl, O. Diabetes Insipidus. Presse Medicale Paris Fr. 2021, 50, 104093. [Google Scholar] [CrossRef]
- Schurr, J.W.; Szumita, P.M.; DeGrado, J.R. Neuroendocrine Derangements in Early Septic Shock: Pharmacotherapy for Relative Adrenal and Vasopressin Insufficiency. Shock Augusta Ga 2017, 48, 284–293. [Google Scholar] [CrossRef]
- Russell, J.A.; Walley, K.R. Vasopressin and Its Immune Effects in Septic Shock. J. Innate Immun. 2010, 2, 446–460. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, M. Review of Clinical Experience of Desmopressin in Patients with Congenital and Acquired Bleeding Disorders. Eur. J. Anaesthesiol. Suppl. 1997, 14, 10–14; discussion 14–18. [Google Scholar] [CrossRef] [PubMed]
- Glavaš, M.; Gitlin-Domagalska, A.; Dębowski, D.; Ptaszyńska, N.; Łęgowska, A.; Rolka, K. Vasopressin and Its Analogues: From Natural Hormones to Multitasking Peptides. Int. J. Mol. Sci. 2022, 23, 3068. [Google Scholar] [CrossRef]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef] [PubMed]
- Mårtensson, J.; Gordon, A.C. Terlipressin or Norepinephrine, or Both in Septic Shock? Intensive Care Med. 2018, 44, 1964–1966. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.-M.; Chen, J.; Kou, Q.; Lin, Q.; Huang, X.; Tang, Z.; Kang, Y.; Li, K.; Zhou, L.; Song, Q.; et al. Terlipressin versus Norepinephrine as Infusion in Patients with Septic Shock: A Multicentre, Randomised, Double-Blinded Trial. Intensive Care Med. 2018, 44, 1816–1825. [Google Scholar] [CrossRef] [PubMed]
- Laterre, P.-F.; Berry, S.M.; Blemings, A.; Carlsen, J.E.; François, B.; Graves, T.; Jacobsen, K.; Lewis, R.J.; Opal, S.M.; Perner, A.; et al. Effect of Selepressin vs Placebo on Ventilator- and Vasopressor-Free Days in Patients with Septic Shock: The SEPSIS-ACT Randomized Clinical Trial. JAMA 2019, 322, 1476–1485. [Google Scholar] [CrossRef] [PubMed]
- Assaf, A. Adhesions after Laparoscopic Myomectomy: Effect of the Technique Used: ADHESIONS AFTER LAPAROSCOPIC MYOMECTOMY. Gynaecol. Endosc. 1999, 8, 225–229. [Google Scholar] [CrossRef]
- Ojeda-Yuren, A.S.; Cerda-Reyes, E.; Herrero-Maceda, M.R.; Castro-Narro, G.; Piano, S. An Integrated Review of the Hepatorenal Syndrome. Ann. Hepatol. 2021, 22, 100236. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801. [Google Scholar] [CrossRef]
- Cohen, J.; Vincent, J.-L.; Adhikari, N.K.J.; Machado, F.R.; Angus, D.C.; Calandra, T.; Jaton, K.; Giulieri, S.; Delaloye, J.; Opal, S.; et al. Sepsis: A Roadmap for Future Research. Lancet Infect. Dis. 2015, 15, 581–614. [Google Scholar] [CrossRef]
- Vincent, J.-L.; Marshall, J.C.; Ñamendys-Silva, S.A.; François, B.; Martin-Loeches, I.; Lipman, J.; Reinhart, K.; Antonelli, M.; Pickkers, P.; Njimi, H.; et al. Assessment of the Worldwide Burden of Critical Illness: The Intensive Care Over Nations (ICON) Audit. Lancet Respir. Med. 2014, 2, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Gamper, G.; Havel, C.; Arrich, J.; Losert, H.; Pace, N.L.; Müllner, M.; Herkner, H. Vasopressors for Hypotensive Shock. Cochrane Database Syst. Rev. 2016. [CrossRef] [PubMed]
- Annane, D.; Vignon, P.; Renault, A.; Bollaert, P.-E.; Charpentier, C.; Martin, C.; Troché, G.; Ricard, J.-D.; Nitenberg, G.; Papazian, L.; et al. Norepinephrine plus Dobutamine versus Epinephrine Alone for Management of Septic Shock: A Randomised Trial. Lancet Lond. Engl. 2007, 370, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Russell, J.A.; Walley, K.R.; Singer, J.; Gordon, A.C.; Hébert, P.C.; Cooper, D.J.; Holmes, C.L.; Mehta, S.; Granton, J.T.; Storms, M.M.; et al. Vasopressin versus Norepinephrine Infusion in Patients with Septic Shock. N. Engl. J. Med. 2008, 358, 877–887. [Google Scholar] [CrossRef] [PubMed]
- Gordon, A.C.; Mason, A.J.; Thirunavukkarasu, N.; Perkins, G.D.; Cecconi, M.; Cepkova, M.; Pogson, D.G.; Aya, H.D.; Anjum, A.; Frazier, G.J.; et al. Effect of Early Vasopressin vs Norepinephrine on Kidney Failure in Patients with Septic Shock: The VANISH Randomized Clinical Trial. JAMA 2016, 316, 509. [Google Scholar] [CrossRef] [PubMed]
- De Backer, D.; Biston, P.; Devriendt, J.; Madl, C.; Chochrad, D.; Aldecoa, C.; Brasseur, A.; Defrance, P.; Gottignies, P.; Vincent, J.-L. Comparison of Dopamine and Norepinephrine in the Treatment of Shock. N. Engl. J. Med. 2010, 362, 779–789. [Google Scholar] [CrossRef] [PubMed]
- Khanna, A.; English, S.W.; Wang, X.S.; Ham, K.; Tumlin, J.; Szerlip, H.; Busse, L.W.; Altaweel, L.; Albertson, T.E.; Mackey, C.; et al. Angiotensin II for the Treatment of Vasodilatory Shock. N. Engl. J. Med. 2017, 377, 419–430. [Google Scholar] [CrossRef] [PubMed]
- Myburgh, J.A.; Higgins, A.; Jovanovska, A.; Lipman, J.; Ramakrishnan, N.; Santamaria, J. CAT Study investigators A Comparison of Epinephrine and Norepinephrine in Critically Ill Patients. Intensive Care Med. 2008, 34, 2226–2234. [Google Scholar] [CrossRef] [PubMed]
- Font, M.D.; Thyagarajan, B.; Khanna, A.K. Sepsis and Septic Shock—Basics of Diagnosis, Pathophysiology and Clinical Decision Making. Med. Clin. N. Am. 2020, 104, 573–585. [Google Scholar] [CrossRef]
- Cecconi, M.; Evans, L.; Levy, M.; Rhodes, A. Sepsis and Septic Shock. Lancet 2018, 392, 75–87. [Google Scholar] [CrossRef]
- Hotchkiss, R.S.; Karl, I.E. The Pathophysiology and Treatment of Sepsis. N. Engl. J. Med. 2003, 348, 138–150. [Google Scholar] [CrossRef] [PubMed]
- Boomer, J.S.; To, K.; Chang, K.C.; Takasu, O.; Osborne, D.F.; Walton, A.H.; Bricker, T.L.; Jarman, S.D.; Kreisel, D.; Krupnick, A.S.; et al. Immunosuppression in Patients Who Die of Sepsis and Multiple Organ Failure. JAMA 2011, 306, 2594–2605. [Google Scholar] [CrossRef]
- Torres, L.K.; Pickkers, P.; van der Poll, T. Sepsis-Induced Immunosuppression. Annu. Rev. Physiol. 2022, 84, 157–181. [Google Scholar] [CrossRef]
- Hotchkiss, R.S.; Monneret, G.; Payen, D. Sepsis-Induced Immunosuppression: From Cellular Dysfunctions to Immunotherapy. Nat. Rev. Immunol. 2013, 13, 862–874. [Google Scholar] [CrossRef] [PubMed]
- Hotchkiss, R.S.; Opal, S. Immunotherapy for Sepsis—A New Approach against an Ancient Foe. N. Engl. J. Med. 2010, 363, 87–89. [Google Scholar] [CrossRef]
- Angus, D.C.; Van Der Poll, T. Severe Sepsis and Septic Shock. N. Engl. J. Med. 2013, 369, 840–851. [Google Scholar] [CrossRef]
- Russell, J.A.; Rush, B.; Boyd, J. Pathophysiology of Septic Shock. Crit. Care Clin. 2018, 34, 43–61. [Google Scholar] [CrossRef]
- Payen, D.; Bernard, C.; Beloucif, S. Nitric oxide in sepsis. Clin. Chest Med. 1996, 17, 333–350. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Li, X. Role of TRPV4 Channel in Vasodilation and Neovascularization. Microcirculation 2021, 28, e12703. [Google Scholar] [CrossRef] [PubMed]
- Holmes, C.L.; Walley, K.R.; Chittock, D.R.; Lehman, T.; Russell, J.A. The Effects of Vasopressin on Hemodynamics and Renal Function in Severe Septic Shock: A Case Series. Intensive Care Med. 2001, 27, 1416–1421. [Google Scholar] [CrossRef] [PubMed]
- Patel, B.M.; Chittock, D.R.; Russell, J.A.; Walley, K.R. Beneficial Effects of Short-Term Vasopressin Infusion during Severe Septic Shock. Anesthesiology 2002, 96, 576–582. [Google Scholar] [CrossRef]
- Dünser, M.W.; Mayr, A.J.; Ulmer, H.; Knotzer, H.; Sumann, G.; Pajk, W.; Friesenecker, B.; Hasibeder, W.R. Arginine Vasopressin in Advanced Vasodilatory Shock: A Prospective, Randomized, Controlled Study. Circulation 2003, 107, 2313–2319. [Google Scholar] [CrossRef]
- Mehta, S.; Granton, J.; Gordon, A.C.; Cook, D.J.; Lapinsky, S.; Newton, G.; Bandayrel, K.; Little, A.; Siau, C.; Ayers, D.; et al. Cardiac Ischemia in Patients with Septic Shock Randomized to Vasopressin or Norepinephrine. Crit. Care Lond. Engl. 2013, 17, R117. [Google Scholar] [CrossRef] [PubMed]
- Jentzer, J.C.; Coons, J.C.; Link, C.B.; Schmidhofer, M. Pharmacotherapy Update on the Use of Vasopressors and Inotropes in the Intensive Care Unit. J. Cardiovasc. Pharmacol. Ther. 2015, 20, 249–260. [Google Scholar] [CrossRef] [PubMed]
- Jentzer, J.C.; Vallabhajosyula, S.; Khanna, A.K.; Chawla, L.S.; Busse, L.W.; Kashani, K.B. Management of Refractory Vasodilatory Shock. Chest 2018, 154, 416–426. [Google Scholar] [CrossRef] [PubMed]
- Landry, D.W.; Levin, H.R.; Gallant, E.M.; Seo, S.; D’Alessandro, D.; Oz, M.C.; Oliver, J.A. Vasopressin Pressor Hypersensitivity in Vasodilatory Septic Shock: Crit. Care Med. 1997, 25, 1279–1282. [Google Scholar] [CrossRef] [PubMed]
- Landry, D.W.; Levin, H.R.; Gallant, E.M.; Ashton, R.C.; Seo, S.; D’Alessandro, D.; Oz, M.C.; Oliver, J.A. Vasopressin Deficiency Contributes to the Vasodilation of Septic Shock. Circulation 1997, 95, 1122–1125. [Google Scholar] [CrossRef]
- Wieruszewski, E.D.; Jones, G.M.; Samarin, M.J.; Kimmons, L.A. Predictors of Dysrhythmias with Norepinephrine Use in Septic Shock. J. Crit. Care 2021, 61, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Domizi, R.; Calcinaro, S.; Harris, S.; Beilstein, C.; Boerma, C.; Chiche, J.-D.; D’Egidio, A.; Damiani, E.; Donati, A.; Koetsier, P.M.; et al. Relationship between Norepinephrine Dose, Tachycardia and Outcome in Septic Shock: A Multicentre Evaluation. J. Crit. Care 2020, 57, 185–190. [Google Scholar] [CrossRef]
- Ammar, M.A.; Ammar, A.A.; Wieruszewski, P.M.; Bissell, B.D.; Long, M.T.; Albert, L.; Khanna, A.K.; Sacha, G.L. Timing of Vasoactive Agents and Corticosteroid Initiation in Septic Shock. Ann. Intensive Care 2022, 12, 47. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.; Medam, S.; Antonini, F.; Alingrin, J.; Haddam, M.; Hammad, E.; Meyssignac, B.; Vigne, C.; Zieleskiewicz, L.; Leone, M. NOREPINEPHRINE: NOT TOO MUCH, TOO LONG. Shock Augusta Ga 2015, 44, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Stolk, R.F.; van der Pasch, E.; Naumann, F.; Schouwstra, J.; Bressers, S.; van Herwaarden, A.E.; Gerretsen, J.; Schambergen, R.; Ruth, M.M.; van der Hoeven, J.G.; et al. Norepinephrine Dysregulates the Immune Response and Compromises Host Defense during Sepsis. Am. J. Respir. Crit. Care Med. 2020, 202, 830–842. [Google Scholar] [CrossRef]
- Barrett, L.K.; Singer, M.; Clapp, L.H. Vasopressin: Mechanisms of Action on the Vasculature in Health and in Septic Shock. Crit. Care Med. 2007, 35, 33–40. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, A.J.; Thakur, G.; Buckley, J.F.; Singer, M.; Clapp, L.H. The Pore-Forming Subunit of the K(ATP) Channel Is an Important Molecular Target for LPS-Induced Vascular Hyporeactivity in Vitro. Br. J. Pharmacol. 2005, 144, 367–375. [Google Scholar] [CrossRef]
- Jakowenko, N.D.; Murata, J.; Kopp, B.J.; Erstad, B.L. Influence of Timing and Catecholamine Requirements on Vasopressin Responsiveness in Critically Ill Patients with Septic Shock. J. Intensive Care Med. 2022, 37, 1512–1519. [Google Scholar] [CrossRef] [PubMed]
- Russell, J.A.; Lee, T.; Singer, J.; Boyd, J.H.; Walley, K.R. Vasopressin and Septic Shock Trial (VASST) Group The Septic Shock 3.0 Definition and Trials: A Vasopressin and Septic Shock Trial Experience. Crit. Care Med. 2017, 45, 940–948. [Google Scholar] [CrossRef]
- Ukor, I.-F.; Walley, K.R. Vasopressin in Vasodilatory Shock. Crit. Care Clin. 2019, 35, 247–261. [Google Scholar] [CrossRef] [PubMed]
- Sacha, G.L.; Lam, S.W.; Wang, L.; Duggal, A.; Reddy, A.J.; Bauer, S.R. Association of Catecholamine Dose, Lactate, and Shock Duration at Vasopressin Initiation with Mortality in Patients with Septic Shock. Crit. Care Med. 2022, 50, 614–623. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, W.F.; Um, K.J.; Alhazzani, W.; Lengyel, A.P.; Hajjar, L.; Gordon, A.C.; Lamontagne, F.; Healey, J.S.; Whitlock, R.P.; Belley-Côté, E.P. Association of Vasopressin Plus Catecholamine Vasopressors vs Catecholamines Alone with Atrial Fibrillation in Patients with Distributive Shock: A Systematic Review and Meta-Analysis. JAMA 2018, 319, 1889–1900. [Google Scholar] [CrossRef]
- Nagendran, M.; Russell, J.A.; Walley, K.R.; Brett, S.J.; Perkins, G.D.; Hajjar, L.; Mason, A.J.; Ashby, D.; Gordon, A.C. Vasopressin in Septic Shock: An Individual Patient Data Meta-Analysis of Randomised Controlled Trials. Intensive Care Med. 2019, 45, 844–855. [Google Scholar] [CrossRef]
- Balik, M.; Novotny, A.; Suk, D.; Matousek, V.; Maly, M.; Brozek, T.; Tavazzi, G. Vasopressin in Patients with Septic Shock and Dynamic Left Ventricular Outflow Tract Obstruction. Cardiovasc. Drugs Ther. 2020, 34, 685–688. [Google Scholar] [CrossRef]
- Neveu, H.; Kleinknecht, D.; Brivet, F.; Loirat, P.; Landais, P. Prognostic Factors in Acute Renal Failure Due to Sepsis. Results of a Prospective Multicentre Study. The French Study Group on Acute Renal Failure. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. Eur. Ren. Assoc. 1996, 11, 293–299. [Google Scholar] [CrossRef]
- Russell, J.A.; Gordon, A.C.; Williams, M.D.; Boyd, J.H.; Walley, K.R.; Kissoon, N. Vasopressor Therapy in the Intensive Care Unit. Semin. Respir. Crit. Care Med. 2021, 42, 059–077. [Google Scholar] [CrossRef] [PubMed]
- Lauzier, F.; Lévy, B.; Lamarre, P.; Lesur, O. Vasopressin or Norepinephrine in Early Hyperdynamic Septic Shock: A Randomized Clinical Trial. Intensive Care Med. 2006, 32, 1782–1789. [Google Scholar] [CrossRef] [PubMed]
- Gordon, A.C.; Russell, J.A.; Walley, K.R.; Singer, J.; Ayers, D.; Storms, M.M.; Holmes, C.L.; Hébert, P.C.; Cooper, D.J.; Mehta, S.; et al. The Effects of Vasopressin on Acute Kidney Injury in Septic Shock. Intensive Care Med. 2010, 36, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Bellomo, R.; Ronco, C.; Kellum, J.A.; Mehta, R.L.; Palevsky, P. Acute Dialysis Quality Initiative workgroup Acute Renal Failure—Definition, Outcome Measures, Animal Models, Fluid Therapy and Information Technology Needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care Lond. Engl. 2004, 8, R204–R212. [Google Scholar] [CrossRef] [PubMed]
- Nedel, W.L.; Rech, T.H.; Ribeiro, R.A.; Pellegrini, J.A.S.; Moraes, R.B. Renal Outcomes of Vasopressin and Its Analogs in Distributive Shock: A Systematic Review and Meta-Analysis of Randomized Trials. Crit. Care Med. 2019, 47, e44–e51. [Google Scholar] [CrossRef]
- Colon Hidalgo, D.; Patel, J.; Masic, D.; Park, D.; Rech, M.A. Delayed Vasopressor Initiation Is Associated with Increased Mortality in Patients with Septic Shock. J. Crit. Care 2020, 55, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Bai, X.; Yu, W.; Ji, W.; Lin, Z.; Tan, S.; Duan, K.; Dong, Y.; Xu, L.; Li, N. Early versus Delayed Administration of Norepinephrine in Patients with Septic Shock. Crit. Care Lond. Engl. 2014, 18, 532. [Google Scholar] [CrossRef]
- Hammond, D.A.; Ficek, O.A.; Painter, J.T.; McCain, K.; Cullen, J.; Brotherton, A.L.; Kakkera, K.; Chopra, D.; Meena, N. Prospective Open-Label Trial of Early Concomitant Vasopressin and Norepinephrine Therapy versus Initial Norepinephrine Monotherapy in Septic Shock. Pharmacotherapy 2018, 38, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Aksoy, M.O.; Mardini, I.A.; Yang, Y.; Bin, W.; Zhou, S.; Kelsen, S.G. Glucocorticoid Effects on the Beta-Adrenergic Receptor-Adenylyl Cyclase System of Human Airway Epithelium. J. Allergy Clin. Immunol. 2002, 109, 491–497. [Google Scholar] [CrossRef]
- Ertmer, C.; Bone, H.-G.; Morelli, A.; Van Aken, H.; Erren, M.; Lange, M.; Traber, D.L.; Westphal, M. Methylprednisolone Reverses Vasopressin Hyporesponsiveness in Ovine Endotoxemia. Shock Augusta Ga 2007, 27, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Russell, J.A. Bench-to-Bedside Review: Vasopressin in the Management of Septic Shock. Crit. Care Lond. Engl. 2011, 15, 226. [Google Scholar] [CrossRef] [PubMed]
- Annane, D. Vasopressin plus Corticosteroids: The Shock Duo! Crit. Care Med. 2009, 37, 1126–1127. [Google Scholar] [CrossRef]
- Bitton, E.; Zimmerman, S.; Azevedo, L.C.P.; Benhamou, D.; Cecconi, M.; De Waele, J.J.; Lipman, J.; Martin-Loeches, I.; Pirracchio, R.; Scheeren, T.W.L.; et al. An International Survey of Adherence to Surviving Sepsis Campaign Guidelines 2016 Regarding Fluid Resuscitation and Vasopressors in the Initial Management of Septic Shock. J. Crit. Care 2022, 68, 144–154. [Google Scholar] [CrossRef] [PubMed]
- Leone, M.; Goyer, I.; Levy, B.; Dünser, M.W.; Asfar, P.; Jentzer, J.C. Dose of Norepinephrine: The Devil Is in the Details. Intensive Care Med. 2022, 48, 638–640. [Google Scholar] [CrossRef] [PubMed]
- Kotani, Y.; Landoni, G.; Belletti, A.; Khanna, A.K. Response to: Norepinephrine Formulation for Equivalent Vasopressive Score. Crit. Care Lond. Engl. 2023, 27, 125. [Google Scholar] [CrossRef] [PubMed]
- Chawla, L.S.; Ostermann, M.; Forni, L.; Tidmarsh, G.F. Broad Spectrum Vasopressors: A New Approach to the Initial Management of Septic Shock? Crit. Care Lond. Engl. 2019, 23, 124. [Google Scholar] [CrossRef] [PubMed]
- Wieruszewski, P.M.; Khanna, A.K. Vasopressor Choice and Timing in Vasodilatory Shock. Crit. Care Lond. Engl. 2022, 26, 76. [Google Scholar] [CrossRef]
- Hammond, D.A.; Rech, M.A.; Daley, M.J.; Devlin, J.W.; Hodge, E.K.; Kooda, K.J.; Lat, I.; Personett, H.A.; Roberts, R.; Sacha, G.; et al. Perceptions Regarding Vasopressin Use and Practices in Septic Shock, and Cost Containment Strategies. JACCP J. Am. Coll. Clin. Pharm. 2019, 2, 257–267. [Google Scholar] [CrossRef]
- Lam, S.W.; Sacha, G.L.; Duggal, A.; Reddy, A.J.; Bauer, S.R. Abrupt Discontinuation Versus Down-Titration of Vasopressin in Patients Recovering from Septic Shock. Shock 2021, 55, 210–214. [Google Scholar] [CrossRef]
- Hammond, D.A.; McCain, K.; Painter, J.T.; Clem, O.A.; Cullen, J.; Brotherton, A.L.; Chopra, D.; Meena, N. Discontinuation of Vasopressin Before Norepinephrine in the Recovery Phase of Septic Shock. J. Intensive Care Med. 2019, 34, 805–810. [Google Scholar] [CrossRef] [PubMed]
- Duclos, G.; Baumstarck, K.; Dünser, M.; Zieleskiewicz, L.; Leone, M. Effects of the Discontinuation Sequence of Norepinephrine and Vasopressin on Hypotension Incidence in Patients with Septic Shock: A Meta-Analysis. Heart Lung J. Crit. Care 2019, 48, 560–565. [Google Scholar] [CrossRef] [PubMed]
- Bissell, B.D.; Magee, C.; Moran, P.; Bastin, M.L.T.; Flannery, A.H. Hemodynamic Instability Secondary to Vasopressin withdrawal in Septic Shock. J. Intensive Care Med. 2019, 34, 761–765. [Google Scholar] [CrossRef] [PubMed]
- Luckner, G.; Mayr, V.D.; Jochberger, S.; Wenzel, V.; Ulmer, H.; Hasibeder, W.R.; Dünser, M.W. Comparison of Two Dose Regimens of Arginine Vasopressin in Advanced Vasodilatory Shock. Crit. Care Med. 2007, 35, 2280–2285. [Google Scholar] [CrossRef]
- Bauer, S.R.; Sacha, G.L.; Siuba, M.T.; Wang, L.; Wang, X.; Scheraga, R.G.; Vachharajani, V. Vasopressin Response and Clinical Trajectory in Septic Shock Patients. J. Intensive Care Med. 2023, 38, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Lam, S.W.; Barreto, E.F.; Scott, R.; Kashani, K.B.; Khanna, A.K.; Bauer, S.R. Cost-Effectiveness of Second-Line Vasopressors for the Treatment of Septic Shock. J. Crit. Care 2020, 55, 48–55. [Google Scholar] [CrossRef]
- Der-Nigoghossian, C.; Hammond, D.A.; Ammar, M.A. Narrative Review of Controversies Involving Vasopressin Use in Septic Shock and Practical Considerations. Ann. Pharmacother. 2020, 54, 706–714. [Google Scholar] [CrossRef]
- Torbic, H.; Sacha, G.L.; Bauer, S.R.; Lam, S.W. Body Mass’s Impact on Response to Fixed-Dose Vasopressin in Patients with Septic Shock. Shock 2018, 50, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Hodge, E.K.; Hughes, D.W.; Attridge, R.L. Effect of Body Weight on Hemodynamic Response in Patients Receiving Fixed-Dose Vasopressin for Septic Shock. Ann. Pharmacother. 2016, 50, 816–823. [Google Scholar] [CrossRef]
- Luckner, G.; Dünser, M.W.; Jochberger, S.; Mayr, V.D.; Wenzel, V.; Ulmer, H.; Schmid, S.; Knotzer, H.; Pajk, W.; Hasibeder, W.; et al. Arginine Vasopressin in 316 Patients with Advanced Vasodilatory Shock. Crit. Care Med. 2005, 33, 2659–2666. [Google Scholar] [CrossRef]
- Baghela, A.; Pena, O.M.; Lee, A.H.; Baquir, B.; Falsafi, R.; An, A.; Farmer, S.W.; Hurlburt, A.; Mondragon-Cardona, A.; Rivera, J.D.; et al. Predicting Sepsis Severity at First Clinical Presentation: The Role of Endotypes and Mechanistic Signatures. EBioMedicine 2022, 75, 103776. [Google Scholar] [CrossRef] [PubMed]
- Nakada, T.-A.; Russell, J.A.; Boyd, J.H.; Aguirre-Hernandez, R.; Thain, K.R.; Thair, S.A.; Nakada, E.; McConechy, M.; Walley, K.R. Beta2-Adrenergic Receptor Gene Polymorphism Is Associated with Mortality in Septic Shock. Am. J. Respir. Crit. Care Med. 2010, 181, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Nakada, T.-A.; Russell, J.A.; Wellman, H.; Boyd, J.H.; Nakada, E.; Thain, K.R.; Thair, S.A.; Hirasawa, H.; Oda, S.; Walley, K.R. Leucyl/Cystinyl Aminopeptidase Gene Variants in Septic Shock. Chest 2011, 139, 1042–1049. [Google Scholar] [CrossRef] [PubMed]
- Russell, J.A. Vasopressin in Septic Shock: Crit. Care Med. 2007, 35, S609–S615. [Google Scholar] [CrossRef] [PubMed]
- Gleeson, P.J.; Crippa, I.A.; Mongkolpun, W.; Cavicchi, F.Z.; Van Meerhaeghe, T.; Brimioulle, S.; Taccone, F.S.; Vincent, J.-L.; Creteur, J. Renin as a Marker of Tissue-Perfusion and Prognosis in Critically Ill Patients. Crit. Care Med. 2019, 47, 152–158. [Google Scholar] [CrossRef]
- Bellomo, R.; Forni, L.G.; Busse, L.W.; McCurdy, M.T.; Ham, K.R.; Boldt, D.W.; Hästbacka, J.; Khanna, A.K.; Albertson, T.E.; Tumlin, J.; et al. Renin and Survival in Patients Given Angiotensin II for Catecholamine-Resistant Vasodilatory Shock. A Clinical Trial. Am. J. Respir. Crit. Care Med. 2020, 202, 1253–1261. [Google Scholar] [CrossRef] [PubMed]
- Levin, M.A.; Lin, H.-M.; Castillo, J.G.; Adams, D.H.; Reich, D.L.; Fischer, G.W. Early On-Cardiopulmonary Bypass Hypotension and Other Factors Associated with Vasoplegic Syndrome. Circulation 2009, 120, 1664–1671. [Google Scholar] [CrossRef]
- Omar, S.; Zedan, A.; Nugent, K. Cardiac Vasoplegia Syndrome: Pathophysiology, Risk Factors and Treatment. Am. J. Med. Sci. 2015, 349, 80–88. [Google Scholar] [CrossRef]
- Argenziano, M.; Chen, J.M.; Choudhri, A.F.; Cullinane, S.; Garfein, E.; Weinberg, A.D.; Smith, C.R.; Rose, E.A.; Landry, D.W.; Oz, M.C. Management of Vasodilatory Shock after Cardiac Surgery: Identification of Predisposing Factors and Use of a Novel Pressor Agent. J. Thorac. Cardiovasc. Surg. 1998, 116, 973–980. [Google Scholar] [CrossRef]
- Wan, S.; LeClerc, J.L.; Vincent, J.L. Cytokine Responses to Cardiopulmonary Bypass: Lessons Learned from Cardiac Transplantation. Ann. Thorac. Surg. 1997, 63, 269–276. [Google Scholar] [CrossRef]
- Downing, S.W.; Edmunds, L.H. Release of Vasoactive Substances during Cardiopulmonary Bypass. Ann. Thorac. Surg. 1992, 54, 1236–1243. [Google Scholar] [CrossRef]
- Kirklin, J.K. Prospects for Understanding and Eliminating the Deleterious Effects of Cardiopulmonary Bypass. Ann. Thorac. Surg. 1991, 51, 529–531. [Google Scholar] [CrossRef] [PubMed]
- Jochberger, S.; Velik-Salchner, C.; Mayr, V.D.; Luckner, G.; Wenzel, V.; Falkensammer, G.; Ulmer, H.; Morgenthaler, N.; Hasibeder, W.; Dünser, M.W. The Vasopressin and Copeptin Response in Patients with Vasodilatory Shock after Cardiac Surgery: A Prospective, Controlled Study. Intensive Care Med. 2009, 35, 489–497. [Google Scholar] [CrossRef] [PubMed]
- Yilman, M.; Erenler, A.K.; Baydin, A. Copeptin: A Diagnostic Factor for Critical Patients. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 3030–3036. [Google Scholar] [PubMed]
- Imamura, T.; Kinugawa, K.; Hatano, M.; Fujino, T.; Inaba, T.; Maki, H.; Kinoshita, O.; Nawata, K.; Kyo, S.; Ono, M.; et al. Low Cardiac Output Stimulates Vasopressin Release in Patients with Stage d Heart Failure. Circ. J. Off. J. Jpn. Circ. Soc. 2014, 78, 2259–2267. [Google Scholar] [CrossRef]
- Argenziano, M.; Choudhri, A.F.; Oz, M.C.; Rose, E.A.; Smith, C.R.; Landry, D.W. A Prospective Randomized Trial of Arginine Vasopressin in the Treatment of Vasodilatory Shock after Left Ventricular Assist Device Placement. Circulation 1997, 96, II-286–II-290. [Google Scholar]
- Dünser, M.W.; Bouvet, O.; Knotzer, H.; Arulkumaran, N.; Hajjar, L.A.; Ulmer, H.; Hasibeder, W.R. Vasopressin in Cardiac Surgery: A Meta-Analysis of Randomized Controlled Trials. J. Cardiothorac. Vasc. Anesth. 2018, 32, 2225–2232. [Google Scholar] [CrossRef]
- Hajjar, L.A.; Vincent, J.L.; Barbosa Gomes Galas, F.R.; Rhodes, A.; Landoni, G.; Osawa, E.A.; Melo, R.R.; Sundin, M.R.; Grande, S.M.; Gaiotto, F.A.; et al. Vasopressin versus Norepinephrine in Patients with Vasoplegic Shock after Cardiac Surgery: The VANCS Randomized Controlled Trial. Anesthesiology 2017, 126, 85–93. [Google Scholar] [CrossRef]
- Okamoto, Y.; Nohmi, T.; Higa, Y.; Seki, K.; Yamashita, A. Vasopressin Does Not Raise Cardiac Enzymes Following Cardiac Surgery: A Randomized Double-Blind Clinical Trial. J. Cardiothorac. Vasc. Anesth. 2015, 29, 46–51. [Google Scholar] [CrossRef]
- Porhomayon, J.; Davari-Farid, S.; Li, C.M.; Arora, P.; Pourafkari, L.; Nader, N.D. Intraoperative Administration of Vasopressin during Coronary Artery Bypass Surgery Is Associated with Acute Postoperative Kidney Injury. J. Crit. Care 2015, 30, 963–968. [Google Scholar] [CrossRef]
- Bomberg, H.; Bierbach, B.; Flache, S.; Scheuer, C.; Novák, M.; Schäfers, H.-J.; Menger, M.D. Vasopressin Induces Rectosigmoidal Mucosal Ischemia during Cardiopulmonary Bypass. J. Card. Surg. 2014, 29, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Guarracino, F.; Habicher, M.; Treskatsch, S.; Sander, M.; Szekely, A.; Paternoster, G.; Salvi, L.; Lysenko, L.; Gaudard, P.; Giannakopoulos, P.; et al. Vasopressor Therapy in Cardiac Surgery-An Experts’ Consensus Statement. J. Cardiothorac. Vasc. Anesth. 2021, 35, 1018–1029. [Google Scholar] [CrossRef] [PubMed]
- Jentzer, J.C.; Hollenberg, S.M. Vasopressor and Inotrope Therapy in Cardiac Critical Care. J. Intensive Care Med. 2021, 36, 843–856. [Google Scholar] [CrossRef]
- Gordon, R.J.; Ravin, M.; Daicoff, G.R.; Rawitscher, R.E. Effects of Hemodilution on Hypotention during Cardiopulmonary Bypass. Anesth. Analg. 1975, 54, 482–488. [Google Scholar] [CrossRef]
- Soar, J.; Berg, K.M.; Andersen, L.W.; Böttiger, B.W.; Cacciola, S.; Callaway, C.W.; Couper, K.; Cronberg, T.; D’Arrigo, S.; Deakin, C.D.; et al. Adult Advanced Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Resuscitation 2020, 156, A80–A119. [Google Scholar] [CrossRef]
- Holmberg, M.J.; Issa, M.S.; Moskowitz, A.; Morley, P.; Welsford, M.; Neumar, R.W.; Paiva, E.F.; Coker, A.; Hansen, C.K.; Andersen, L.W.; et al. Vasopressors during Adult Cardiac Arrest: A Systematic Review and Meta-Analysis. Resuscitation 2019, 139, 106–121. [Google Scholar] [CrossRef] [PubMed]
- Martikainen, T.J.; Tenhunen, J.J.; Uusaro, A.; Ruokonen, E. The Effects of Vasopressin on Systemic and Splanchnic Hemodynamics and Metabolism in Endotoxin Shock. Anesth. Analg. 2003, 97, 1756–1763. [Google Scholar] [CrossRef] [PubMed]
- Dünser, M.W.; Mayr, A.J.; Tür, A.; Pajk, W.; Barbara, F.; Knotzer, H.; Ulmer, H.; Hasibeder, W.R. Ischemic Skin Lesions as a Complication of Continuous Vasopressin Infusion in Catecholamine-Resistant Vasodilatory Shock: Incidence and Risk Factors. Crit. Care Med. 2003, 31, 1394–1398. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| VASOPRESSIN AGONISTS | STRUCTURE | RECEPTOR AFFINITY | CLINICAL APPLICATION | HALF-LIFE (min) |
|---|---|---|---|---|
| ARGININE VASOPRESSIN (AVP) | 8-Arginine vasopressin | V1, V2, V3 | Sepsis, vasodilatory shock, cardiac arrest | 5–15 |
| DESMOPRESSIN ACETATE (DDAVP) | Deamino-Cys-D-Arg vasopressin | V2 | Central diabetes insipidus, bleeding disorders | 90–190 |
| TERLIPRESSIN (TP) | N3-triglycyl-8-lysin vasopressin | V1 | Portal hypertension, bleeding gastric and esophageal varices, septic shock | 240–360 |
| SELEPRESSIN | Phe-2-Ile-3-Hgn-4-Orn-8 vasopressin | V1 | Septic shock Not approved for clinical use | 10–30 |
| ORNIPRESSIN | 8-L-Ornithine vasopressin acetate | V1 | Vasoconstricting agent during myomectomy in cirrhosis, as hepatorenal treatment | 60–120 |
| TRIAL | Intervention | Control | Intervention 28 Day Mortality | Control 28 Day Mortality | Absolute Difference (95%CI) p-Value |
|---|---|---|---|---|---|
| VASST [32] | Norepinephrine | Vasopressin | 35.4% | 39.3% | 3.9 (−2.9–10.7) 0.26 |
| VANISH [33] | Norepinephrine | Vasopressin | 30.9% | 27.5% | 3.4 (−5.4–12.3) |
| SOAP II [34] | Norepinephrine | Dopamine | 48.5% | 52.5% | 1.17 (0.97–1.42) 0.10 |
| ATHOS-3 [35] | Angiotensin II | Placebo | 46% | 54% | Hazard ratio 0.78 (0.57–1.07) 0.12 |
| CAT [36] | Epinephrine | Norepinephrine | 23% | 27% | Hazard ratio 0.87 (0.48–1.58) 0.65 |
| CATS [37] | Epinephrine | Norepinephrine + dobutamine | 40% | 34% | Relative risk 0.86 (0.65–1.14) 0.31 |
| Vasopressor | Receptor Activity | Vasa Constriction | Inotropism | Doses | Possible Predictive Biomarkers |
|---|---|---|---|---|---|
| Norepinephrine | α1 > β1, β2 | ++++ | ++ | 0.04–1 μg/kg/min | β2 receptor SNP |
| Vasopressin | V1, V2, V3 | ++++ | 0 | 0.01–0.03 IU/min | LNPEP SNP Angiopoietin 1/2 Vasopressin/copept in |
| Epinephrine | β1 > α1, β2 | ++++ | ++++ | 0.01–0.1 μg/kg/min (β) >0.1 μg/kg/min (α) | β2 receptor SNP |
| Dopamine | D1, α1, β1 | ++-+++ | ++-+++ | Inotropic: 5–10 μg/kg/min Vasopressor > 10 μg/kg/min | |
| Phenylephrine | α1 | ++++ | 0 | 0.1–1.5 μg/kg/min | |
| Angiotensin-ll | AngiotensinⅡ receptors | ++++ | 0 | 5–200 ng/kg/min | AGTRAP SNP |
| Methylene blue | Inhibits GABAA receptors | ++++ | 0 | Bolus(2 mg/kg) then infusion: 0.25–1.2 mg/kg/h |
| Predominant and independent risk factors |
|
| Other risk factors |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Álvarez, R.; Arboleda-Salazar, R. Vasopressin in Sepsis and Other Shock States: State of the Art. J. Pers. Med. 2023, 13, 1548. https://doi.org/10.3390/jpm13111548
García-Álvarez R, Arboleda-Salazar R. Vasopressin in Sepsis and Other Shock States: State of the Art. Journal of Personalized Medicine. 2023; 13(11):1548. https://doi.org/10.3390/jpm13111548
Chicago/Turabian StyleGarcía-Álvarez, Raquel, and Rafael Arboleda-Salazar. 2023. "Vasopressin in Sepsis and Other Shock States: State of the Art" Journal of Personalized Medicine 13, no. 11: 1548. https://doi.org/10.3390/jpm13111548
APA StyleGarcía-Álvarez, R., & Arboleda-Salazar, R. (2023). Vasopressin in Sepsis and Other Shock States: State of the Art. Journal of Personalized Medicine, 13(11), 1548. https://doi.org/10.3390/jpm13111548