
Machine Learning Algorithms for Prediction of Survival by Stress Echocardiography in Chronic Coronary Syndromes

 , , ,
, , ,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
- (A)
- The validation conducted during the RF tuning resampling runs was conducted as follows:
- Each of the 500 trees composing the RF algorithm was developed by using a different bootstrap random sample of the data (training-set data) that was 0.632 times the entire study size.
- The out-of-basket (OOB) sample excluded during the construction of the single tree served as the test set by deriving the prediction for each observation.
- Based on the prediction derived from the single trees, survival curves for OOB patients were calculated.
- For each subject, the average survival curves across 500 runs were calculated to be considered the subject’s final survival.
- At the end of the runs, the OOB C-index performance (perfect prediction = 1) was computed by comparing the true survival with the average OOB survival.
- (B)
- The RF validation was also carried out by considering a 10-fold cross-validation (CV) procedure. The procedure consists of the subdivision of the total data set in 10 parts of equal sample size and, at every step, the 10th part of the data set becomes the validation part, whereas the remaining part constitutes the training set. The predictive tool is trained for each of the 10th parts, avoiding, therefore, problems of overfitting, but also of asymmetrical sampling (and, therefore, those affected by distortion) of the observed sample, which is typical of the subdivision of the data in only two parts (that is training/validation) [21,22]. The performance was assessed by reporting the Harrel C-index statistics. The internal validation performance was calculated also, for comparative purposes, for the conditional tree (CTree [23]), gradient boosting machine (GBM [20]), elastic net regularized Cox regression (Coxnet [24]), and extreme boosting machine (Xgboost [25]).
- (C)
- RF external validation: The RF predictive tool was also externally validated on a cohort of 1002 patients (the external study cohort details are reported in Table S2 of the Supplementary Materials). The RF predictions were calculated on the external cohort and compared with the observed survival of the external cohort data by calculating the C-index concordance measure.
- The survival curve panel is the main application section where the survival prediction is plotted according to the patient’s features selected on the left side of the webpage. The web app includes multiple patients’ profile predictions, enabling us to compare the survivals for the selected patient characteristics.
- The identified patient profiles are stored in the patient’s profile panel.
- The variable importance depth measure plot is reported in the variable importance section of the web application.
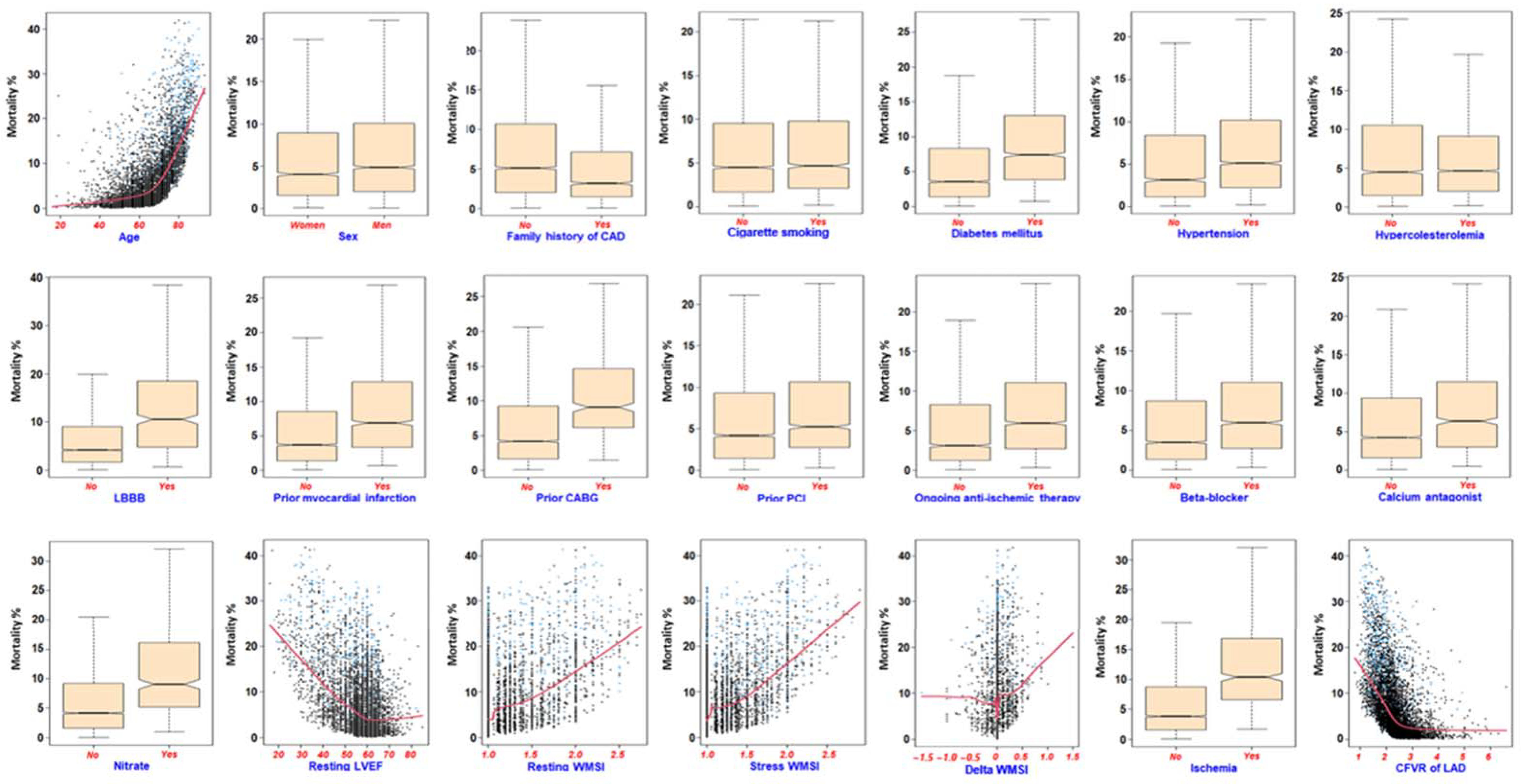
- The marginal effect plots are represented in the marginal effect section for the four leading predictors according to the minimal depth of a variable measure. The explanation of the basic issues concerning the RF algorithm is indicated in the random forest section.
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the Diagnosis and Management of Chronic Coronary Syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef]
- Pellikka, P.A.; Arruda-Olson, A.; Chaudhry, F.A.; Chen, M.H.; Marshall, J.E.; Porter, T.R.; Sawada, S.G. Guidelines for Performance, Interpretation, and Application of Stress Echocardiography in Ischemic Heart Disease: From the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2020, 33, 1–41.e8. [Google Scholar] [CrossRef] [PubMed]
- Ciampi, Q.; Zagatina, A.; Cortigiani, L.; Gaibazzi, N.; Borguezan Daros, C.; Zhuravskaya, N.; Wierzbowska-Drabik, K.; Kasprzak, J.D.; de Castro e Silva Pretto, J.L.; D’Andrea, A.; et al. Functional, Anatomical, and Prognostic Correlates of Coronary Flow Velocity Reserve During Stress Echocardiography. J. Am. Coll. Cardiol. 2019, 74, 2278–2291. [Google Scholar] [CrossRef] [PubMed]
- Cox, D.; Oakes, D. Analysis of Survival Data; Chapman & Hall Ltd.: London, UK, 1984. [Google Scholar]
- Spooner, A.; Chen, E.; Sowmya, A.; Sachdev, P.; Kochan, N.A.; Trollor, J.; Brodaty, H. A Comparison of Machine Learning Methods for Survival Analysis of High-Dimensional Clinical Data for Dementia Prediction. Sci. Rep. 2020, 10, 20410. [Google Scholar] [CrossRef]
- Du, M.; Haag, D.G.; Lynch, J.W.; Mittinty, M.N. Comparison of the Tree-Based Machine Learning Algorithms to Cox Regression in Predicting the Survival of Oral and Pharyngeal Cancers: Analyses Based on SEER Database. Cancers 2020, 12, 2802. [Google Scholar] [CrossRef]
- Jiang, F.; Jiang, Y.; Zhi, H.; Dong, Y.; Li, H.; Ma, S.; Wang, Y.; Dong, Q.; Shen, H.; Wang, Y. Artificial Intelligence in Healthcare: Past, Present and Future. Stroke Vasc. Neurol. 2017, 2, 230–243. [Google Scholar] [CrossRef] [PubMed]
- Alsharqi, M.; Upton, R.; Mumith, A.; Leeson, P. Artificial Intelligence: A New Clinical Support Tool for Stress Echocardiography. Expert Rev. Med. Devices 2018, 15, 513–515. [Google Scholar] [CrossRef] [PubMed]
- Cortigiani, L.; Rigo, F.; Gherardi, S.; Bovenzi, F.; Molinaro, S.; Picano, E.; Sicari, R. Coronary Flow Reserve During Dipyridamole Stress Echocardiography Predicts Mortality. JACC Cardiovasc. Imaging 2012, 5, 1079–1085. [Google Scholar] [CrossRef] [PubMed]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef]
- Dietrich, S.; Floegel, A.; Troll, M.; Kühn, T.; Rathmann, W.; Peters, A.; Sookthai, D.; von Bergen, M.; Kaaks, R.; Adamski, J.; et al. Random Survival Forest in Practice: A Method for Modelling Complex Metabolomics Data in Time to Event Analysis. Int. J. Epidemiol. 2016, 45, 1406–1420. [Google Scholar] [CrossRef]
- Cutler, A.; Cutler, D.R.; Stevens, J.R. Random Forests. In Ensemble Machine Learning; Zhang, C., Ma, Y., Eds.; Springer US: Boston, MA, USA, 2012; pp. 157–175. ISBN 978-1-4419-9325-0. [Google Scholar]
- Breiman, L. Random Forest. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef]
- Steinberg, D.; Colla, P. CART: Classification and Regression Trees. Top Ten Algorithms Data Min. 2009, 9, 179. [Google Scholar]
- Ishwaran, H.; Kogalur, U. Fast Unified Random Forests for Survival, Regression, and Classification (RF-SRC). R Package Version 2019, 2, 1–129. [Google Scholar]
- Ishwaran, H.; Kogalur, U.B.; Blackstone, E.H.; Lauer, M.S. Random Survival Forests. Ann. Appl. Stat. 2008, 2, 841–860. [Google Scholar] [CrossRef]
- Liaw, A.; Wiener, M. Classification and Regression by RandomForest. R News 2002, 2, 18–22. [Google Scholar]
- Ishwaran, H.; Kogalur, U.B.; Gorodeski, E.Z.; Minn, A.J.; Lauer, M.S. High-Dimensional Variable Selection for Survival Data. J. Am. Stat. Assoc. 2010, 105, 205–217. [Google Scholar] [CrossRef]
- Chambers, J.M.; Hastie, T.J. (Eds.) Statistical Models in S.; Chapman & Hall: New York, NY, USA, 1992; ISBN 978-0-412-83040-2. [Google Scholar]
- Friedman, J.H. Greedy Function Approximation: A Gradient Boosting Machine. Ann. Statist. 2001, 29, 1189–1232. [Google Scholar] [CrossRef]
- Hastie, T.; Tibshirani, R.; Friedman, J.H. The Elements of Statistical Learning: Data Mining, Inference, and Prediction, 2nd ed.; Springer series in statistics; Springer: New York, NY, USA, 2009; ISBN 978-0-387-84857-0. [Google Scholar]
- James, G.; Witten, D.; Hastie, T.; Tibshirani, R. An Introduction to Statistical Learning; Springer Texts in Statistics; Springer: New York, NY, USA, 2013; Volume 103, ISBN 978-1-4614-7137-0. [Google Scholar]
- Hothorn, T.; Bretz, F.; Westfall, P. Simultaneous Inference in General Parametric Models. Biom. J. 2008, 50, 346–363. [Google Scholar] [CrossRef]
- Zou, H.; Hastie, T. Regularization and Variable Selection via the Elastic Net. J. R. Stat. Soc. B 2005, 67, 301–320. [Google Scholar] [CrossRef]
- Chen, T.; Guestrin, C. XGBoost: A Scalable Tree Boosting System. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13 August 2016; ACM: San Francisco, CA, USA; pp. 785–794. [Google Scholar]
- Sengupta, P.P.; Shrestha, S.; Berthon, B.; Messas, E.; Donal, E.; Tison, G.H.; Min, J.K.; D’hooge, J.; Voigt, J.-U.; Dudley, J.; et al. Proposed Requirements for Cardiovascular Imaging-Related Machine Learning Evaluation (PRIME): A Checklist: Reviewed by the American College of Cardiology Healthcare Innovation Council. JACC Cardiovasc. Imaging 2020, 13, 2017–2035. [Google Scholar] [CrossRef]
- Ehrlinger, J. GgRandomForests: Visually Exploring Random Forests; R CRAN: Vienna, Austria, 2016. [Google Scholar]
- Rajula, H.S.R.; Verlato, G.; Manchia, M.; Antonucci, N.; Fanos, V. Comparison of Conventional Statistical Methods with Machine Learning in Medicine: Diagnosis, Drug Development, and Treatment. Medicina 2020, 56, 455. [Google Scholar] [CrossRef] [PubMed]
- Davenport, T.; Kalakota, R. The Potential for Artificial Intelligence in Healthcare. Future Healthc. J. 2019, 6, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Cortigiani, L.; Ciampi, Q.; Lombardo, A.; Rigo, F.; Bovenzi, F.; Picano, E. Age- and Gender-Specific Prognostic Cutoff Values of Coronary Flow Velocity Reserve in Vasodilator Stress Echocardiography. J. Am. Soc. Echocardiogr. 2019, 32, 1307–1317. [Google Scholar] [CrossRef] [PubMed]
- Cortigiani, L.; Rigo, F.; Gherardi, S.; Bovenzi, F.; Picano, E.; Sicari, R. Implication of the Continuous Prognostic Spectrum of Doppler Echocardiographic Derived Coronary Flow Reserve on Left Anterior Descending Artery. Am. J. Cardiol. 2010, 105, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Lauer, M.S.; Blackstone, E.H.; Young, J.B.; Topol, E.J. Cause of Death in Clinical Research. J. Am. Coll. Cardiol. 1999, 34, 618–620. [Google Scholar] [CrossRef]
- Carpeggiani, C.; Landi, P.; Michelassi, C.; Andreassi, M.G.; Sicari, R.; Picano, E. Stress Echocardiography Positivity Predicts Cancer Death. JAHA 2017, 6, e007104. [Google Scholar] [CrossRef]
- Gaibazzi, N.; Picano, E.; Suma, S.; Garibaldi, S.; Porter, T.R.; Botti, A.; Tuttolomondo, D.; Tedeschi, A.; Lorenzoni, V. Coronary Flow Velocity Reserve Reduction Is Associated with Cardiovascular, Cancer, and Noncancer, Noncardiovascular Mortality. J. Am. Soc. Echocardiogr. 2020, 33, 594–603. [Google Scholar] [CrossRef]
- Raposeiras Roubín, S.; Cordero, A. The Two-Way Relationship Between Cancer and Atherosclerosis. Rev. Española Cardiol. (Engl. Ed.) 2019, 72, 487–494. [Google Scholar] [CrossRef]
- Scali, M.C.; Zagatina, A.; Ciampi, Q.; Cortigiani, L.; D’Andrea, A.; Daros, C.B.; Zhuravskaya, N.; Kasprzak, J.D.; Wierzbowska-Drabik, K.; Luis de Castro e Silva Pretto, J.; et al. Lung Ultrasound and Pulmonary Congestion During Stress Echocardiography. JACC Cardiovasc. Imaging 2020, 13, 2085–2095. [Google Scholar] [CrossRef]
- Ciampi, Q.; Zagatina, A.; Cortigiani, L.; Wierzbowska-Drabik, K.; Kasprzak, J.D.; Haberka, M.; Djordjevic-Dikic, A.; Beleslin, B.; Boshchenko, A.; Ryabova, T.; et al. Prognostic Value of Stress Echocardiography Assessed by the ABCDE Protocol. Eur. Heart J. 2021, 42, 3869–3878. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Alive | Death | Overall | HR | 95% CI | p-Value |
|---|---|---|---|---|---|---|
| (N = 6067) | (N = 814) | (N = 6881) | ||||
| Age (Years) | 58/66/73 | 69/76/80 | 59/67/74 | 1.1 | 1.09, 1.11 | <0.001 |
| Gender: Female | 41% (2489) | 38% (312) | 41% (2801) | - | - | - |
| Male | 59% (3578) | 62% (502) | 59% (4080) | 1.16 | 1.00, 1.33 | 0.044 |
| Family history of CAD: No | 71% (4286) | 79% (642) | 72% (4928) | - | - | - |
| Yes | 29% (1781) | 21% (172) | 28% (1953) | 0.6 | 0.51, 0.71 | <0.001 |
| Cigarette smoking: No | 71% (4325) | 73% (595) | 71% (4920) | - | - | - |
| Yes | 29% (1742) | 27% (219) | 29% (1961) | 0.99 | 0.85, 1.15 | 0.89 |
| Diabetes mellitus: No | 77% (4672) | 64% (521) | 75% (5193) | - | - | - |
| Yes | 23% (1395) | 36% (293) | 25% (1688) | 1.77 | 1.53, 2.04 | <0.001 |
| Hypertension: No | 33% (2026) | 29% (240) | 33% (2266) | - | - | - |
| Yes | 67% (4041) | 71% (574) | 67% (4615) | 1.29 | 1.11, 1.50 | <0.001 |
| Hypercholesterolemia: No | 44% (2654) | 50% (406) | 44% (3060) | - | - | - |
| Yes | 56% (3413) | 50% (408) | 56% (3821) | 0.87 | 0.76, 0.99 | 0.041 |
| LBBB: No | 93% (5650) | 88% (719) | 93% (6369) | - | - | - |
| Yes | 7% (417) | 12% (95) | 7% (512) | 2.05 | 1.65, 2.54 | <0.001 |
| Prior myocardial infarction: No | 76% (4617) | 69% (563) | 75% (5180) | - | - | - |
| Yes | 24% (1450) | 31% (251) | 25% (1701) | 1.49 | 1.28, 1.73 | <0.001 |
| Prior CABG: No | 94% (5731) | 89% (721) | 94% (6452) | - | - | - |
| Yes | 6% (336) | 11% (93) | 6% (429) | 1.81 | 1.46, 2.25 | <0.001 |
| Prior PCI: No | 74% (4511) | 75% (608) | 74% (5119) | - | - | - |
| Yes | 26% (1556) | 25% (206) | 26% (1762) | 1 | 0.85, 1.17 | 0.96 |
| Ongoing anti-ischemic therapy: No | 54% (3278) | 53% (434) | 54% (3712) | - | - | - |
| Yes | 46% (2789) | 47% (380) | 46% (3169) | 1.35 | 1.18, 1.56 | <0.001 |
| Beta blocker: No | 62% (3765) | 62% (504) | 62% (4269) | - | - | - |
| Yes | 38% (2302) | 38% (310) | 38% (2612) | 1.31 | 1.14, 1.51 | <0.001 |
| Calcium antagonist: No | 86% (5209) | 86% (703) | 86% (5912) | - | - | - |
| Yes | 14% (858) | 14% (111) | 14% (969) | 1.25 | 1.02, 1.52 | 0.035 |
| Nitrate: No | 94% (5691) | 91% (743) | 94% (6434) | - | - | - |
| Yes | 6% (376) | 9% (71) | 6% (447) | 1.64 | 1.29, 2.10 | <0.001 |
| Resting LVEF | 55/60/62 | 50/58/60 | 54/60/62 | 0.95 | 0.95, 0.96 | <0.001 |
| Resting WMSI | 1.0/1.0/1.1 | 1.0/1.0/1.4 | 1.0/1.0/1.1 | 3.2 | 2.70, 3.81 | <0.001 |
| Stress WMSI | 1.0/1.0/1.2 | 1.0/1.0/1.4 | 1.0/1.0/1.2 | 1.57 | 1.47, 1.68 | <0.001 |
| Delta WMSI | 0/0/0 | 0/0/0 | 0/0/0 | 2.66 | 1.47, 4.83 | 0.002 |
| Ischemia: No | 90% (5478) | 89% (725) | 90% (6203) | - | - | - |
| Yes | 10% (589) | 11% (89) | 10% (678) | 1.89 | 1.52, 2.36 | <0.001 |
| CFVR of LAD | 2.0/2.3/2.7 | 1.6/2.0/2.3 | 2.0/2.3/2.6 | 0.29 | 0.25, 0.33 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cortigiani, L.; Azzolina, D.; Ciampi, Q.; Lorenzoni, G.; Gaibazzi, N.; Rigo, F.; Gherardi, S.; Bovenzi, F.; Gregori, D.; Picano, E. Machine Learning Algorithms for Prediction of Survival by Stress Echocardiography in Chronic Coronary Syndromes. J. Pers. Med. 2022, 12, 1523. https://doi.org/10.3390/jpm12091523
Cortigiani L, Azzolina D, Ciampi Q, Lorenzoni G, Gaibazzi N, Rigo F, Gherardi S, Bovenzi F, Gregori D, Picano E. Machine Learning Algorithms for Prediction of Survival by Stress Echocardiography in Chronic Coronary Syndromes. Journal of Personalized Medicine. 2022; 12(9):1523. https://doi.org/10.3390/jpm12091523
Chicago/Turabian StyleCortigiani, Lauro, Danila Azzolina, Quirino Ciampi, Giulia Lorenzoni, Nicola Gaibazzi, Fausto Rigo, Sonia Gherardi, Francesco Bovenzi, Dario Gregori, and Eugenio Picano. 2022. "Machine Learning Algorithms for Prediction of Survival by Stress Echocardiography in Chronic Coronary Syndromes" Journal of Personalized Medicine 12, no. 9: 1523. https://doi.org/10.3390/jpm12091523
APA StyleCortigiani, L., Azzolina, D., Ciampi, Q., Lorenzoni, G., Gaibazzi, N., Rigo, F., Gherardi, S., Bovenzi, F., Gregori, D., & Picano, E. (2022). Machine Learning Algorithms for Prediction of Survival by Stress Echocardiography in Chronic Coronary Syndromes. Journal of Personalized Medicine, 12(9), 1523. https://doi.org/10.3390/jpm12091523