3.1. Embolization-Related Adverse Events
As most major and minor complications follow non-target embolization, a possible explanation for their absence/low rate in this report may be the increased knowledge concerning the management of extra-prostatic communications during PAE [
14,
15] and prostatic arterial anatomy [
11,
12,
13]. Three-dimensional imaging during selective angiography used as a routine practice may help to rule out extra-prostatic supplies, and its need may decrease over time and eventually be restricted to elective cases once a significant learning curve is achieved.
Early minor events ranged from 0.6 to 2.6%, which were lower than those previously reported [
7,
8,
9,
10]. Multiple adverse events previously described in the literature and meta-analyses were not observed in this study, which may suggest a significant decrease in non-target embolization and may be explained by the improvement of experience during recent years.
There was no AUR compared to the 4.55, 7, 9 and 7.8% previously described [
7,
8,
9,
10]. AUR is favored by bladder distension during and after PAE and the increase in urethral stricture and bladder outlet obstruction due to post-embolization intra-prostatic oedema. Foley catheter insertion during PAE was not necessary as less invasive measures, such as urinating moments prior to entering the Angio suite, a urinal at their disposal during the procedure, and immediate voiding after PAE, were efficient to prevent retention. Furthermore, TRA permits urination in a standing position, moments after the procedure, which facilitates micturition.
Hematuria occurred in 2.6%, which was lower compared to the 5.51, 9, 4.45, and 4.38% previously reported [
7,
8,
9,
10]. As the angiographic review reported the close proximity of the vesical arteries to the PA (at least one type-1 PA per patient), these events may suggest that non-target vesical embolization due to reflux of the embolic agent was possibly the cause of hematuria. Nonetheless, the short duration of this event (24 h in all cases except the one associated with prostatic fragment detachment) may suggest the bleeding of prostate tissue necrosis during its healing process following PAE.
One case of 24 h-lasting hematuria and no micturition symptom followed coil protection of an AIVA or a vesical anastomosis, which suggests the safety of this technique for bladder viability and confirms the findings of a previous report in the literature [
15]. On the other hand, the absence of coil protection of a vesical artery or anastomose in proximity to the prostatic artery may lead to bladder ischemia: a previous case report reported focal bladder necrosis following non-target vesical embolization during PAE using 100–300 μm microparticles, that was successfully treated by Foley catheter placement for several weeks [
23].
There was a 0.6% rate of rectorrhagia, which was lower than the 4.8, 3.9, 3.02, and 3.02% previously reported [
7,
8,
9,
10]. The hypothesis for rectal bleeding following PAE is non-target embolization and ischemic ulceration of the rectum. This was previously described in a case report for PAE using 100–300 μm particles, where coil protection was not performed, with the spontaneous resolution of ulcerations within 5 days [
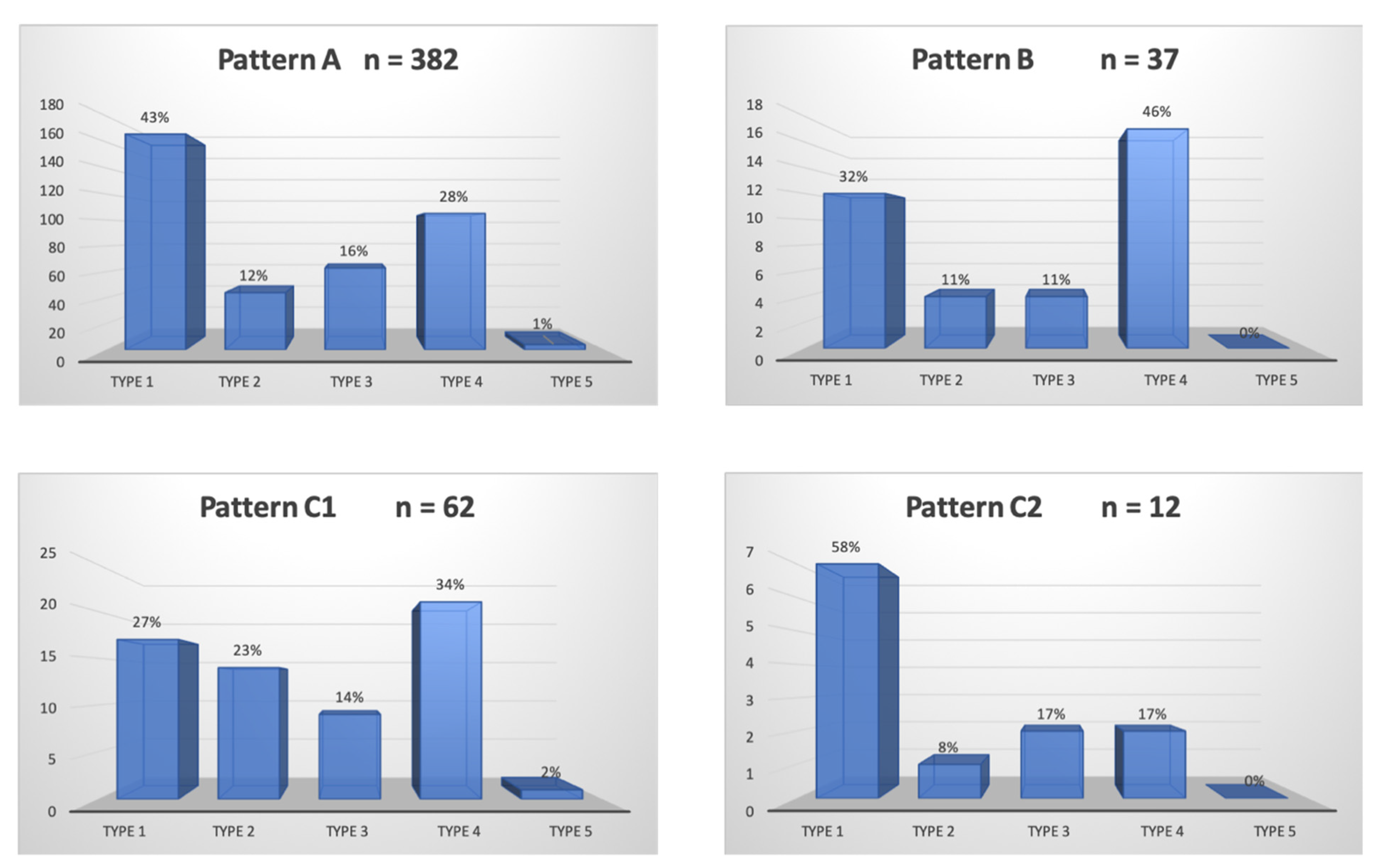
24]. In this study, both cases of rectorrhagia did not present arterial anatomy at risk of non-target rectal embolization. As the amount and duration of bleeding were negligible, the traces of blood in stool that were reported by the patients may instead be attributed to hemorrhoid hemorrhage provoked by constipation. Furthermore, there were interestingly 7/12 (58%) cases of pattern C2 PA where the accessory rectal artery could not be coil-protected and was therefore fully embolized with no post-operative complication. This may suggest that the embolization of pattern C2 PAs using 300–500 μm particles does not necessarily require coil protection. This supposition could have been stronger in case of a control group purposely not performing coil protection, but the case report mentioned regarding the above [
24] made the safety of such a design questionable.
This hypothesis will need further comparative studies for confirmation, but the safety profile of future study designs must be considered. As the size of the microparticles used may play a role in the occurrence of adverse events [
23,
24], the choice of particle size of the type of embolic should be carefully made, and choosing to use 300–500 μm particles may be the best option for future randomized trials. In our opinion, the choice of a control group performing the abstention of coil protection may be too risky, and coil protection should be compared to the balloon occlusion micro-catheter technique. Concerning small rectal arteries arising from the PA (pattern C2), the results of this study may suggest another safety profile other than vesical, penile, or large rectal extra-prostatic supplies in case of non-target embolization using 300–500 μm particles.
There was no sign of rectal ischemia following coil protection, which confirmed the results of the previous reports [
14,
15].
Balanitis was observed in 0.6%, which is comparable to the 0.6, 0.3, and 0.7% reported [
8,
9,
10]. This event occurred in a particular anatomical pattern previously described. Penile adverse events, secondary to non-target microparticle embolization, are more likely to occur in situations where the PA is close to penile vessels, such as pattern B PA, accessory distal pudendal PA, or type-4 PA, and, despite cautious microparticle delivery, can lead to ischemic balanitis or, in the worst case, necrosis of the glans penis [
25]. The findings in this study may suggest cautious particle delivery when embolizing the PA in a situation of distal pudendal PA: reflux during embolization may be at a higher risk of adverse events and should be avoided. Coil protection of pattern B PA, when possible, was safe in this study, as previously reported [
14,
15]. When coil protection is precluded, a balloon occlusion micro catheter may be of use [
21] to prevent reflux.
UTIs were found in 0.6% in this cohort, only in patients with a Foley catheter in place because of an AUR, which was lower compared to the 3.1, 2.7, and 3.32% described in the literature [
7,
9,
10]. No distinction was made in previous reports between patients with a Foley catheter or catheter-free. In several studies assessed in meta-analyses, Foley catheter insertion during PAE was performed to facilitate the procedure [
4,
26,
27], which was not the case for patients from this cohort. The findings in this study suggest that the insertion and/or presence of Foley catheter may increase the risk of UTIs.
There was one case of a transient worsening of erectile dysfunction (ED) following the coil protection of a prostato-penile artery in a situation of ipsilateral IPA occlusion. De novo ED following PAE is rare and has been reported [
5], but never occurred after coil protection [
14,
15,
28,
29,
30].
We believe that coil protection should be avoided in situations of poor IPA vasculature. IPA revascularization may also be considered [
31] to permit safe bilateral PAE in a two-step process.
There was one case of the detachment of prostate fragments three months after PAE. This rare event was reported in three case reports and a retrospective report in a total of 8 patients and occurred at 2 to 10 weeks: spontaneous tissue elimination of fragment(s) ranging from a 10 to 15 mm diameter and up to 60 mm long was reported after PAE using 250 μm (1 case) [
32] or 100–300 ± 300–500 μm microparticles (3 cases) [
33], and 4 cases of detachment following 250 μm particles PAE [
34,
35] required cystoscopic removal of multiple fragments. In the latter (3/48 patients, 6.3%), predictors for the detachment of prostatic tissue were proposed, such as indwelling catheter, high central gland index, and inflammation. Detachment seems to be correlated with the use of small size embolics <300 μm. Torres et al. reported in a randomized study no clinical benefit of 100–300 μm compared to 300–500 μm trisacryl microparticles, and more frequent minor adverse events [
17].
Hematospermia was observed in 2.6%, compared to the 3.63, 4.09, and 5.2 reported [
7,
8,
9]. Occurrence may vary from a study to another as its identification relies on sexual activity. Previous reports link its occurrence to the non-target embolization of seminal vesicles [
2]. Ischemia of the seminal vesicles following PAE was described [
36,
37], but as all control MRI in this study did not show morphological/enhancement abnormalities of the SV in patients manifesting hematospermia, bleeding from necrotic prostatic tissue during ejaculation may not be excluded. This is why it was decided in this report to consider hematospermia as a post-embolization symptom rather than an adverse event.
No case of anejaculation was reported. There is, to our knowledge, no report of anejaculation following PAE using 300–500 μm trisacryl microparticles. Anejaculation following PAE ranges in the radiologic literature from 0 to 2.3% [
7,
8,
9,
10]. The reasons are unclear. A recent urological report of PAE using 250–400 μm polyzene microparticles [
38] reported an unexpected 4/25 (16%) rate of anejaculation and 40% of decreased ejaculation volume assessed by a 4-item sexual questionnaire 3 months after PAE. Among patients facing anejaculation, 3/4 had undergone endoscopic enucleation of the prostate following symptomatic detachment of prostatic tissue after PAE. Furthermore, longer follow-up (>3 months) on ejaculation was not available.
3.4. Follow-Up
There was a 12.2% (38/311) rate of loss to follow-up at one month, and 84.9% and 85.2% (264/311 and 265/311) at 6 and 12 months. The amount of missing data after the one-month follow-up needs to be considered. Still, as all but one adverse events were monitored at one month because they occurred during the first days following PAE and had, except for a few rare events, resolved within the first month prior to the one-month follow-up visit, the loss of follow-up may not have a significant impact on estimating the overall occurrence of adverse events and only limits the results on mid-term functional outcomes and clinical success. Furthermore, patients manifesting adverse events lasting longer than one month or occurring between months 1 and 6, such as transient decreased ejaculate volume, prostate fragment detachment, or radial artery occlusion, were all observed in the clinic at 6- and 12-month visits.
This report has some limitations, including its retrospective nature, the limited number of studied patients, the loss of follow-up at mid-term visits, and the short period of follow-up time. Additionally, this study lacks control groups, especially concerning measures used for the protection of extra-prostatic arterial supplies. Most adverse events were retrospectively monitored and based on patient testimony only, and were not confirmed by clinical examination or assessed by urinary/blood tests or imaging at the time of occurrence. This may have led to the over- or underestimation of their occurrence.


 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}