
Patterns and Characteristics of SKYLINE-Lumipoint Feature in the Catheter Ablation of Atypical Atrial Flutter: Insight from a Novel Lumipoint Module of Rhythmia Mapping System

 , , ,
, , , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Electrophysiological Study and HDM with Rhythmia System
2.3. Definition and Classification of aAFL
2.4. Catheter Ablation
2.5. Offline HDM Lumipoint Algorithm and SKYLINE Analyses
2.6. Statistical Analyses
3. Results
3.1. Patient Clinical Characteristics and Outcomes
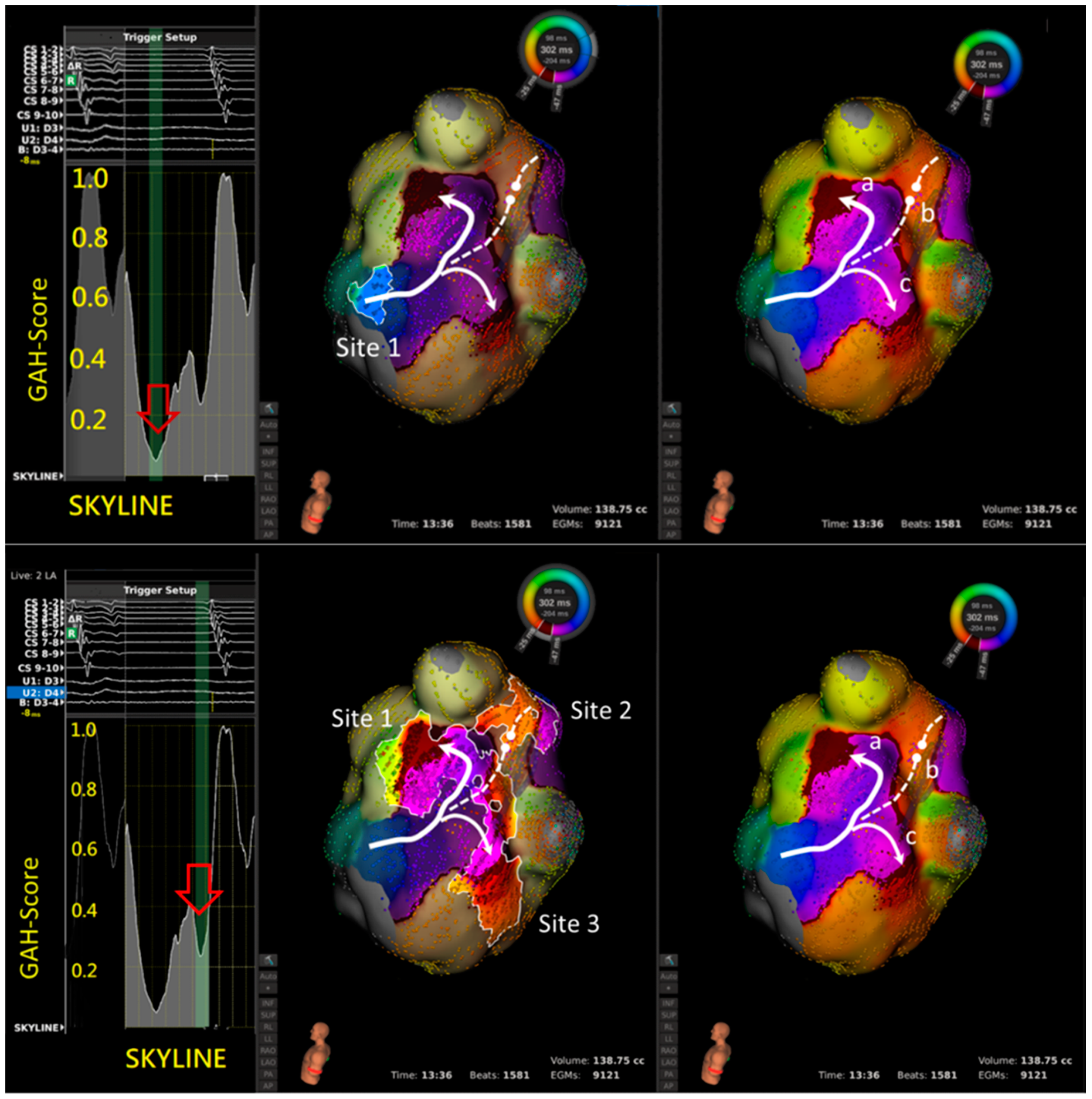
3.2. GAH-Valleys and Corresponding Highlighted Areas
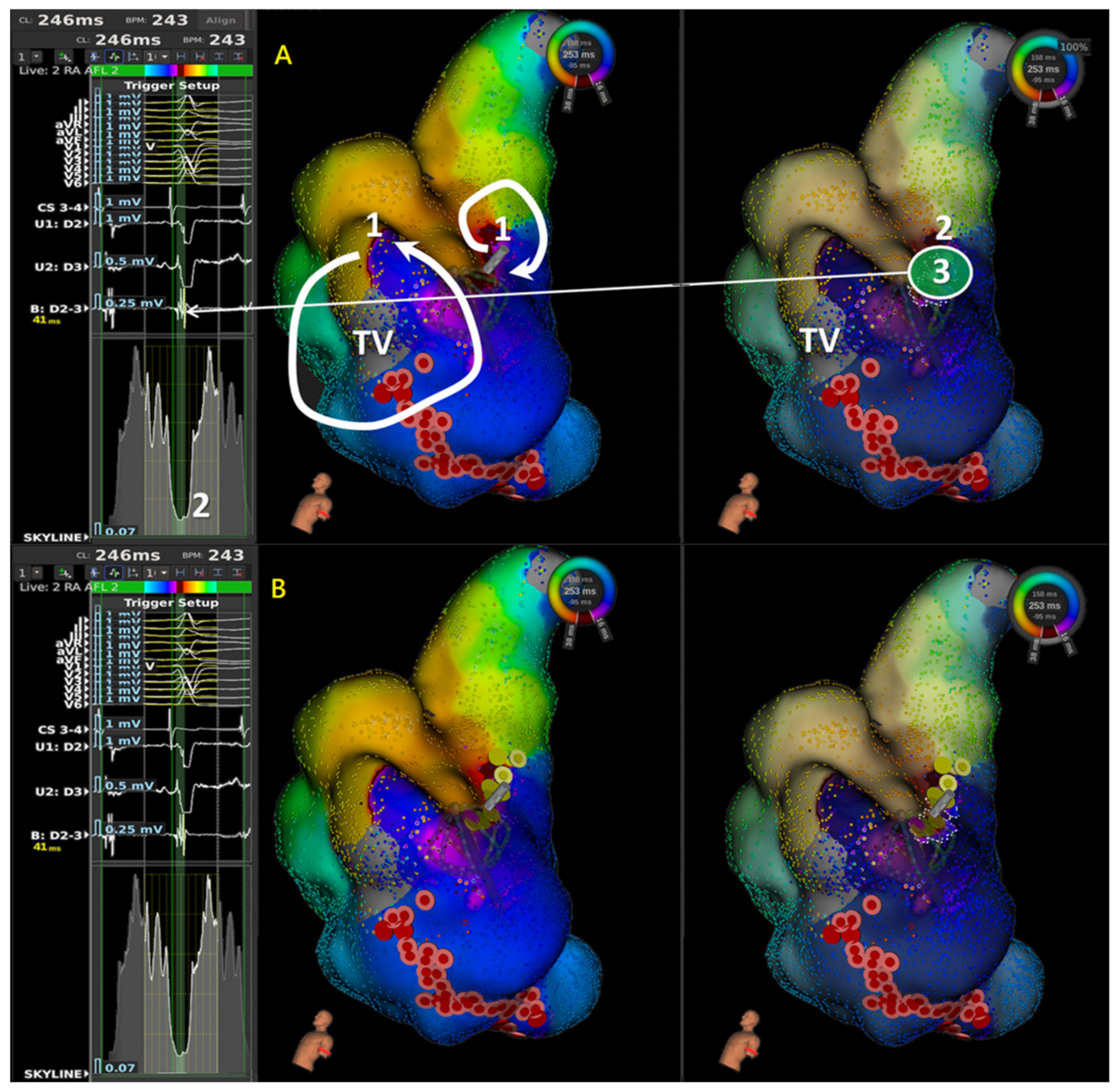
3.3. Activation Wave-Front Characteristics of Highlighted Areas Corresponding to GAH-Valleys
- In 14 aAFLs of macro-reentry, 51 areas were highlighted based on 27 lowest GAH-Valleys (Table 2). The electrophysiological properties of the lowest GAH-Valley corresponding area was shown in Table 3. Twenty-three areas showed signs of slow conduction, 20 of wave-front collision, 5 of lines of block, and 3 of others, i.e., wave-front breakout. Of the 23 slow conductions, 19 (83%) occurred within the aAFL circuit (Table 3A).
3.4. Practical Ablation Sites and Outcome
4. Discussion
4.1. Major Findings
- SKYLINE feature of most reentry aAFLs displayed a multi-deflected peak with an average of 1.5 GAH-valleys.
- In the aAFL patients, these GAH-valleys were usually steep, instead of solitary peak and plateau. Its corresponding highlighted area harbored the comparable incidence of slow conductions (30, 47%) and wave-front collisions (26, 41%).
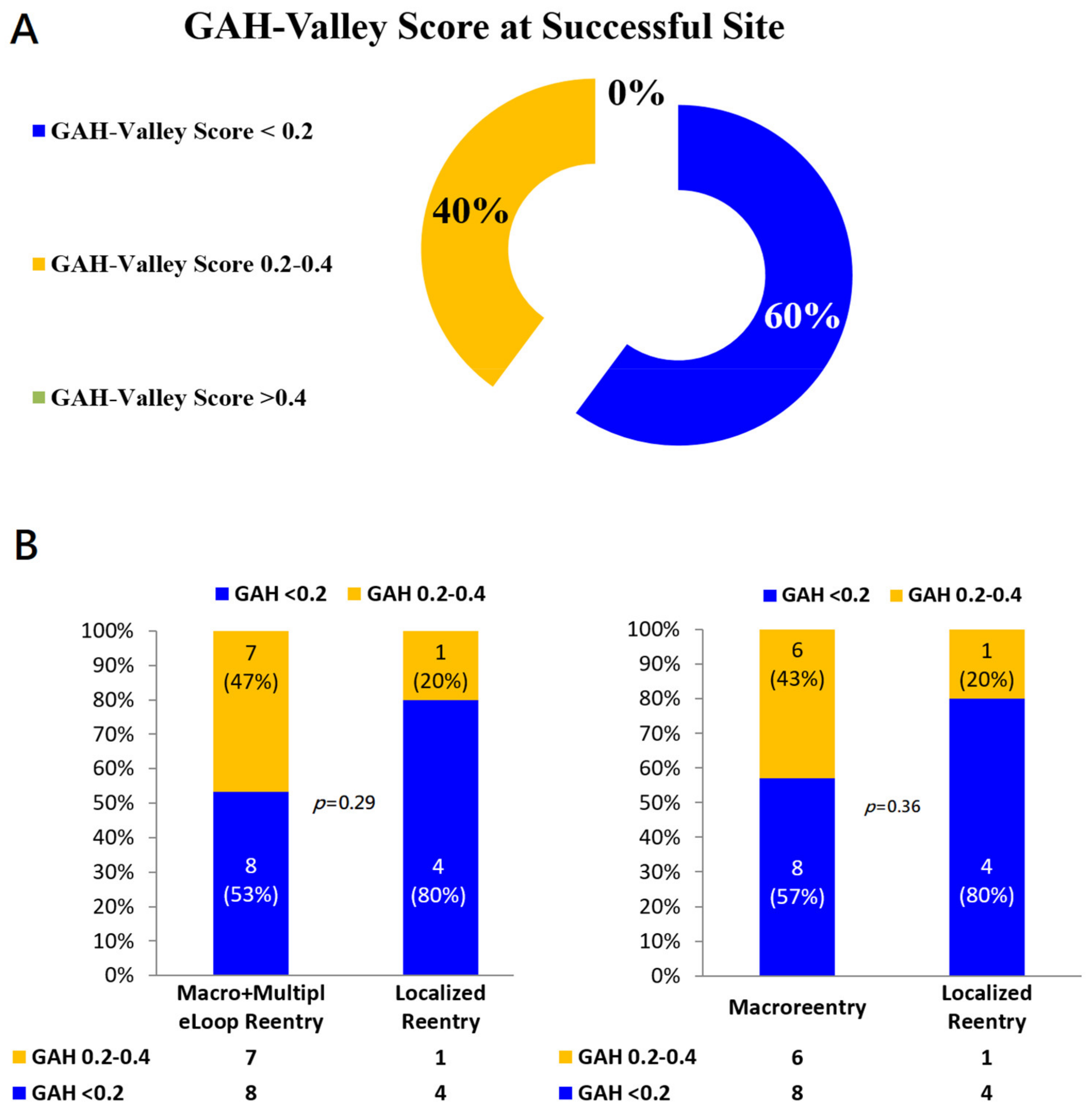
- In localized reentry related aAFLs, areas with a GAH-valley <0.2 in SKYLINE usually indicated the successful ablation site.
- In macro-reentry, successful sites were areas with a GAH-valley score <0.4, not limited to areas with a GAH-valley <0.2.
- Taken together, in these 20 aAFLs, successful ablation sites all occurred at areas showing GAH-valleys <0.4.
4.2. Patterns and Characteristics of SKYLINE
4.3. Valley in SKYLINE (GAH-Valley)—Conduction ‘Deceleration’
4.4. LUMIPOINT Algorithm as an Automatic Search for Practical Ablation Sites
4.5. Clinical Implications
4.6. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Wasmer, K.; Monnig, G.; Bittner, A.; Dechering, D.; Zellerhoff, S.; Milberg, P.; Kobe, J.; Eckardt, L. Incidence, characteristics, and outcome of left atrial tachycardias after circumferential antral ablation of atrial fibrillation. Heart Rhythm. 2012, 9, 1660–1666. [Google Scholar] [CrossRef] [PubMed]
- Rostock, T.; Drewitz, I.; Steven, D.; Hoffmann, B.A.; Salukhe, T.V.; Bock, K.; Servatius, H.; Aydin, M.A.; Meinertz, T.; Willems, S. Characterization, mapping, and catheter ablation of recurrent atrial tachycardias after stepwise ablation of long-lasting persistent atrial fibrillation. Circ. Arrhythm. Electrophysiol. 2010, 3, 160–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohari, M.; Pap, R. Atrial tachycardias occurring late after open heart surgery. Curr. Cardiol. Rev. 2015, 11, 134–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saghy, L.; Tutuianu, C.; Szilagyi, J. Atrial tachycardias following atrial fibrillation ablation. Curr. Cardiol. Rev. 2015, 11, 149–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oral, H.; Knight, B.P.; Morady, F. Left atrial flutter after segmental ostial radiofrequency catheter ablation for pulmonary vein isolation. Pacing Clin. Electrophysiol. 2003, 26, 1417–1419. [Google Scholar] [CrossRef] [PubMed]
- Chugh, A.; Oral, H.; Lemola, K.; Hall, B.; Cheung, P.; Good, E.; Tamirisa, K.; Han, J.; Bogun, F.; Pelosi, F., Jr.; et al. Prevalence, mechanisms, and clinical significance of macroreentrant atrial tachycardia during and following left atrial ablation for atrial fibrillation. Heart Rhythm. 2005, 2, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Mesas, C.E.; Pappone, C.; Lang, C.C.; Gugliotta, F.; Tomita, T.; Vicedomini, G.; Sala, S.; Paglino, G.; Gulletta, S.; Ferro, A.; et al. Left atrial tachycardia after circumferential pulmonary vein ablation for atrial fibrillation: Electroanatomic characterization and treatment. J. Am. Coll. Cardiol. 2004, 44, 1071–1079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, Y.; Takahashi, A.; Miyazaki, S.; Kuwahara, T.; Takei, A.; Fujino, T.; Fujii, A.; Kusa, S.; Yagishita, A.; Nozato, T.; et al. Electrophysiological characteristics of localized reentrant atrial tachycardia occurring after catheter ablation of long-lasting persistent atrial fibrillation. J. Cardiovasc. Electrophysiol. 2009, 20, 623–629. [Google Scholar] [CrossRef] [PubMed]
- Wazni, O.M.; Saliba, W.; Fahmy, T.; Lakkireddy, D.; Thal, S.; Kanj, M.; Martin, D.O.; Burkhardt, J.D.; Schweikert, R.; Natale, A. Atrial arrhythmias after surgical maze: Findings during catheter ablation. J. Am. Coll. Cardiol. 2006, 48, 1405–1409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weerasooriya, R.; Jais, P.; Wright, M.; Matsuo, S.; Knecht, S.; Nault, I.; Sacher, F.; Deplagne, A.; Bordachar, P.; Hocini, M.; et al. Catheter ablation of atrial tachycardia following atrial fibrillation ablation. J. Cardiovasc. Electrophysiol. 2009, 20, 833–838. [Google Scholar] [CrossRef] [PubMed]
- Saoudi, N.; Cosio, F.; Waldo, A.; Chen, S.A.; Iesaka, Y.; Lesh, M.; Saksena, S.; Salerno, J.; Schoels, W. Classification of atrial flutter and regular atrial tachycardia according to electrophysiologic mechanism and anatomic bases: A statement from a joint expert group from the Working Group of Arrhythmias of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. J. Cardiovasc. Electrophysiol. 2001, 12, 852–866. [Google Scholar] [PubMed]
- Sanders, P.; Hocini, M.; Jais, P.; Hsu, L.F.; Takahashi, Y.; Rotter, M.; Scavee, C.; Pasquie, J.L.; Sacher, F.; Rostock, T.; et al. Characterization of focal atrial tachycardia using high-density mapping. J. Am. Coll. Cardiol. 2005, 46, 2088–2099. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, H.; Ikeda, A.; Sharma, T.; Lazzara, R.; Jackman, W.M. Rapid high resolution electroanatomical mapping: Evaluation of a new system in a canine atrial linear lesion model. Circ. Arrhythm. Electrophysiol. 2012, 5, 417–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anter, E.; Tschabrunn, C.M.; Contreras-Valdes, F.M.; Li, J.; Josephson, M.E. Pulmonary vein isolation using the Rhythmia mapping system: Verification of intracardiac signals using the Orion mini-basket catheter. Heart Rhythm. 2015, 12, 1927–1934. [Google Scholar] [CrossRef] [PubMed]
- Bollmann, A.; Hilbert, S.; John, S.; Kosiuk, J.; Hindricks, G. Insights from preclinical ultra high-density electroanatomical sinus node mapping. Europace 2015, 17, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.A.; Takigawa, M.; Martin, R.; Maury, P.; Meyer, C.; Wong, T.; Shi, R.; Gajendragadkar, P.; Frontera, A.; Cheniti, G.; et al. Use of Novel Electrogram “Lumipoint” Algorithm to Detect Critical Isthmus and Abnormal Potentials for Ablation in Ventricular Tachycardia. JACC Clin. Electrophysiol. 2019, 5, 470–479. [Google Scholar] [CrossRef] [PubMed]
- Solimene, F.; Maddaluno, F.; Malacrida, M.; Schillaci, V. Pseudo-reentry due to automatic annotation of dissociated activity unmasked by the new Lumipoint algorithm. Clin. Case Rep. 2020, 8, 38–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takigawa, M.; Martin, C.A.; Derval, N.; Denis, A.; Vlachos, K.; Kitamura, T.; Frontera, A.; Martin, R.; Cheniti, G.; Lam, A.; et al. Insights from atrial surface activation throughout atrial tachycardia cycle length: A new mapping tool. Heart Rhythm. 2019, 16, 1652–1660. [Google Scholar] [CrossRef] [PubMed]
- Latcu, D.G.; Bun, S.S.; Viera, F.; Delassi, T.; El Jamili, M.; Al Amoura, A.; Saoudi, N. Selection of Critical Isthmus in Scar-Related Atrial Tachycardia Using a New Automated Ultrahigh Resolution Mapping System. Circ. Arrhythm. Electrophysiol. 2017, 10, e004510. [Google Scholar] [CrossRef] [PubMed]
- Alken, F.A.; Klatt, N.; Muenkler, P.; Scherschel, K.; Jungen, C.; Akbulak, R.O.; Kahle, A.K.; Gunawardene, M.; Jularic, M.; Dinshaw, L. Advanced mapping strategies for ablation therapy in adults with congenital heart disease. Cardiovasc. Diagn. Ther. 2019, 9, S247–S263. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Charateristics | |
|---|---|
| Age (years) | 65.3 ± 10.7 |
| Male (n,%) | 9 (60%) |
| SHD | 9 (60%) |
| CHF | 6 (40%) |
| Hypertension | 6 (40%) |
| Diabetes Mellitus | 3 (20%) |
| CAD | 5 (33%) |
| Stroke | 1 (7%) |
| CHA2DS2-VASc score | 2.6 ± 2 |
| LVEF (%) | 52.1 ± 10.8% |
| Prior Procedure | 12 (80%) |
| Post-cardiovascular Surgery | 7 (47%) |
| Post-AF/AFL Ablation | 6 (40%) |
| No. of Previous Procedure | 0.8 ± 1.0 |
| PVI | 6 (40%) |
| Roof Line | 5 (33%) |
| Mitral Isthmus Line | 5 (33%) |
| Cavo-tricuspid Isthmus Line | 8 (53%) |
| Defragmentation in LA (CFAE ablation) | 1 (7%) |
| Follow-up (m) | 12.5 ± 9.3 |
| aAFL characteristics (n = 20) | n(%) |
| Macro-reentry AFL | 14 (70%) |
| Anatomical AFL | 8 (40%) |
| Peri-mitral | 4 |
| Peri-tricuspid | 1 |
| Roof-dependent | 2 |
| Between Aortic groove & mitral | 1 |
| Surgical Scar-related | 3 (15%) |
| Other atypical AFL (gap related, inter-atrial septum) | 3 (15%) |
| Localized reentry (micro-reentry) | 5 (25%) |
| Multiple loop AFL | 1 (5%) |
| Total No. of GAH-Valley | No. of GAH-Valley per AFL | No. of Highlighted Areas | No. of Highlighted Areas per GAH-Valley | No. of Highlighted Areas per AFL | Successful Termination Site Corresponding to Highlighted Area | |
|---|---|---|---|---|---|---|
| Macroreentry AFL (n = 14) | 27 | 2 (1-2) | 51 | 2 (1-2) | 3 (2–5) | 8/14 |
| Localized reentry AFL (n = 5) | 6 | 1 (1–1) | 11 | 1.5 (1–3) | 1 (1–3) | 4/5 |
| Multiple loop AFL (n = 1) | 1 | 1 | 1 | 1 | 1 | 0/1 |
| Total (n = 20) | 34 | 1.5 (1-2) | 63 | 2 (1-2) | 3 (1–4.5) | 12/20 |
| (A) 14 Macroreentry AFL | Slow Conduction (n = 23) | Wavefront Collision (n = 20) | Line of Block (n = 5) | Others (n = 3) |
|---|---|---|---|---|
| In the circuit (n = 20) | 19/23 (83) | 0 | 0 | 1/3 (33) |
| Out of the circuit (n = 31) | 4/23 (17) | 20/20 (100) | 5/5 (100) | 2/3 (67) |
| Total (n = 51) | 23 (45) | 20 (39) | 5 (10) | 3 (6) |
| (B) 5 Localized AFL | Slow Conduction (n = 6) | Wavefront Collision (n = 5) | Line of Block (n = 0) | Others (n = 0) |
| In the circuit (n = 6) | 6/6 (100) | 0/5 (0) | 0 | 0 |
| Out of the circuit (n = 5) | 0/6 (0) | 5/5 (100) | 0 | 0 |
| Total (n = 11) | 6 (55) | 5 (45) | 0 | 0 |
| (C) 1 Multiple loop AFL | Slow conduction (n = 1) | Wavefront Collision (n = 0) | Line of Block (n = 0) | Others (n = 0) |
| In the circuit (n = 1) | 1/1 (100) | 0 | 0 | 0 |
| Out of the circuit (n = 1) | 0/0 (0) | 0 | 0 | 0 |
| Total (n = 2) | 1/1 (100) | 0 | 0 | 0 |
| (D) Total 20 AFL | Slow conduction (n = 30) | Wavefront Collision (n = 26) | Line of Block (n = 5) | Others (n = 3) |
| In the circuit (n = 27) | 26/30 (87) | 0/26 (0) | 0/5 (0) | 1/3 (33) |
| Out of the circuit (n = 37) | 4/30 (13) | 26/26 (100) | 5/5 (100) | 2/3 (67) |
| Total (n = 64) | 30 (47) | 26 (41) | 5 (8) | 3 (5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, C.-H.; Lo, L.-W.; Jain, A.; Hsieh, Y.-C.; Lin, Y.-J.; Chang, S.-L.; Chung, F.-P.; Hu, Y.-F.; Chao, T.-F.; Liao, J.-N.; et al. Patterns and Characteristics of SKYLINE-Lumipoint Feature in the Catheter Ablation of Atypical Atrial Flutter: Insight from a Novel Lumipoint Module of Rhythmia Mapping System. J. Pers. Med. 2022, 12, 1102. https://doi.org/10.3390/jpm12071102
Li C-H, Lo L-W, Jain A, Hsieh Y-C, Lin Y-J, Chang S-L, Chung F-P, Hu Y-F, Chao T-F, Liao J-N, et al. Patterns and Characteristics of SKYLINE-Lumipoint Feature in the Catheter Ablation of Atypical Atrial Flutter: Insight from a Novel Lumipoint Module of Rhythmia Mapping System. Journal of Personalized Medicine. 2022; 12(7):1102. https://doi.org/10.3390/jpm12071102
Chicago/Turabian StyleLi, Cheng-Hung, Li-Wei Lo, Ankit Jain, Yu-Cheng Hsieh, Yenn-Jiang Lin, Shih-Lin Chang, Fa-Po Chung, Yu-Feng Hu, Tze-Fan Chao, Jo-Nan Liao, and et al. 2022. "Patterns and Characteristics of SKYLINE-Lumipoint Feature in the Catheter Ablation of Atypical Atrial Flutter: Insight from a Novel Lumipoint Module of Rhythmia Mapping System" Journal of Personalized Medicine 12, no. 7: 1102. https://doi.org/10.3390/jpm12071102
APA StyleLi, C.-H., Lo, L.-W., Jain, A., Hsieh, Y.-C., Lin, Y.-J., Chang, S.-L., Chung, F.-P., Hu, Y.-F., Chao, T.-F., Liao, J.-N., Chang, T.-Y., Lin, C.-Y., Lugtu, I. C., Ton, A. N.-K., Liu, S.-H., Cheng, W.-H., Liu, C.-M., Wu, C.-I., & Chen, S.-A. (2022). Patterns and Characteristics of SKYLINE-Lumipoint Feature in the Catheter Ablation of Atypical Atrial Flutter: Insight from a Novel Lumipoint Module of Rhythmia Mapping System. Journal of Personalized Medicine, 12(7), 1102. https://doi.org/10.3390/jpm12071102