
Clinical Utility of Personalized Serum IgG Subclass Ratios for the Differentiation of IgG4-Related Sclerosing Cholangitis (IgG4-SC) from Primary Sclerosing Cholangitis (PSC) and Cholangiocarcinoma (CCA)

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection and Definitions
2.3. Statistical Analysis
3. Results
3.1. Clinical Characteristics of the Study Population
3.2. Performance of the Serum IgG Subclass Combinations for the Differential Diagnosis of IgG4-SC from PSC
3.3. Performance of the Serum IgG Subclass Combinations for the Differential Diagnosis of IgG4-SC from CCA
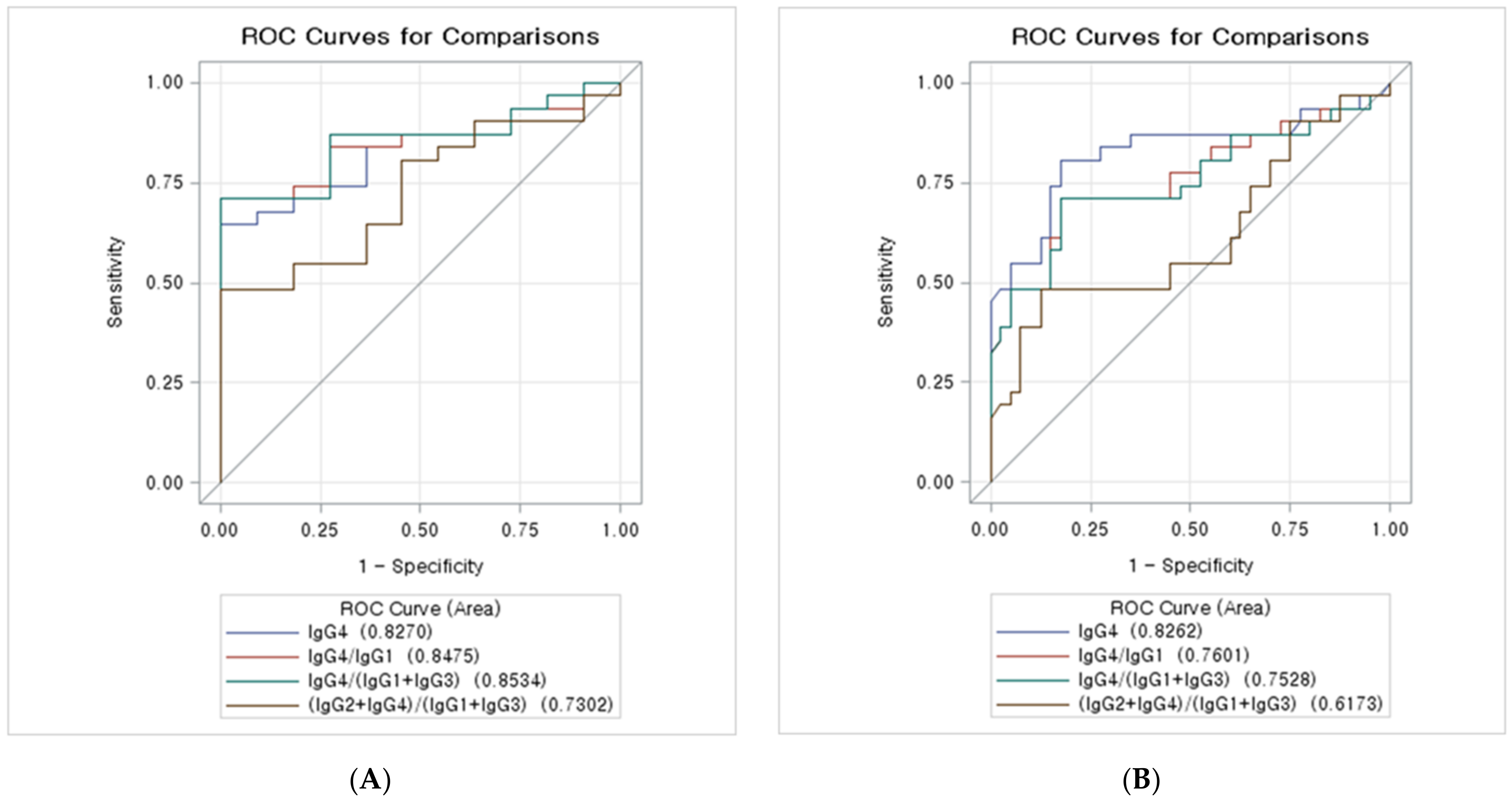
3.4. ROC Curves of the IgG Subclass Combinations for the Diagnosis of IgG4-SC from PSC
3.5. ROC Curves of the IgG Subclass Combinations for the Diagnosis of IgG4-SC from CCA
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- O’Reilly, D.A.; Malde, D.J.; Duncan, T.; Rao, M.; Filobbos, R. Review of the diagnosis, classification and manage ment of autoimmune pancreatitis. World J. Gastrointest. Pathophysiol. 2014, 5, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Ghazale, A.; Chari, S.T.; Zhang, L.; Smyrk, T.C.; Takahashi, N.; Levy, M.J.; Topazian, M.D.; Clain, J.E.; Pearson, R.K.; Petersen, B.T.; et al. Immunoglobulin G4-associated cholangitis: Clinical profile and response to therapy. Gastroenterology 2008, 134, 706–715. [Google Scholar] [CrossRef] [PubMed]
- Beuers, U.; Hubers, L.M.; Doorenspleet, M.; Maillette de Buy Wenniger, L.; Klarenbeek, P.L.; Boonstra, K.; Ponsioen, C.; Rauws, E.; de Vries, N. IgG4-Associated Cholangitis—A Mimic of PSC. Dig. Dis. 2015, 33, 176–180. [Google Scholar] [CrossRef] [PubMed]
- Nakazawa, T.; Shimizu, S.; Naitoh, I. IgG4-Related Sclerosing Cholangitis. Semin. Liver Dis. 2016, 36, 216–228. [Google Scholar] [CrossRef]
- Nakazawa, T.; Naitoh, I.; Hayashi, K.; Okumura, F.; Miyabe, K.; Yoshida, M.; Yamashita, H.; Ohara, H.; Joh, T. Diagnostic criteria for IgG4-related sclerosing cholangitis based on cholangiographic classification. J. Gastroenterol. 2012, 47, 79–87. [Google Scholar] [CrossRef]
- Ohara, H.; Okazaki, K.; Tsubouchi, H.; Inui, K.; Kawa, S.; Kamisawa, T.; Tazuma, S.; Uchida, K.; Hirano, K.; Yoshida, H.; et al. Clinical diagnostic criteria of IgG4-related sclerosing cholangitis 2012. J. Hepatobiliary Pancreat. Sci. 2012, 19, 536–542. [Google Scholar] [CrossRef]
- Chari, S.T.; Smyrk, T.C.; Levy, M.J.; Topazian, M.D.; Takahashi, N.; Zhang, L.; Clain, J.E.; Pearson, R.K.; Petersen, B.T.; Vege, S.S.; et al. Diagnosis of autoimmune pancreatitis: The Mayo Clinic experience. Clin. Gastroenterol. Hepatol. 2006, 4, 1010–1016. quiz 1934. [Google Scholar] [CrossRef]
- Mendes, F.D.; Jorgensen, R.; Keach, J.; Katzmann, J.A.; Smyrk, T.; Donlinger, J.; Chari, S.; Lindor, K.D. Elevated serum IgG4 concentration in patients with primary sclerosing cholangitis. Am. J. Gastroenterol. 2006, 101, 2070–2075. [Google Scholar] [CrossRef]
- Oseini, A.M.; Chaiteerakij, R.; Shire, A.M.; Ghazale, A.; Kaiya, J.; Moser, C.D.; Aderca, I.; Mettler, T.A.; Therneau, T.M.; Zhang, L.; et al. Utility of serum immunoglobulin G4 in distinguishing immunoglobulin G4-associated cholangitis from cholangiocarcinoma. Hepatology 2011, 54, 940–948. [Google Scholar] [CrossRef]
- Schroeder, H.W., Jr.; Cavacini, L. Structure and function of immunoglobulins. J. Allergy Clin. Immunol. 2010, 125, S41–S52. [Google Scholar] [CrossRef]
- Roitt, I. Roitt’s Essential Immunology, 9th ed.; Blackwell Science: London, UK, 1997. [Google Scholar]
- Hamano, H.; Kawa, S.; Horiuchi, A.; Unno, H.; Furuya, N.; Akamatsu, T.; Fukushima, M.; Nikaido, T.; Nakayama, K.; Usuda, N.; et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N. Engl. J. Med. 2001, 344, 732–738. [Google Scholar] [CrossRef] [PubMed]
- Saeki, T.; Nishi, S.; Imai, N.; Ito, T.; Yamazaki, H.; Kawano, M.; Yamamoto, M.; Takahashi, H.; Matsui, S.; Nakada, S.; et al. Clinicopathological characteristics of patients with IgG4-related tubulointerstitial nephritis. Kidney Int. 2010, 78, 1016–1023. [Google Scholar] [CrossRef] [PubMed]
- Masaki, Y.; Dong, L.; Kurose, N.; Kitagawa, K.; Morikawa, Y.; Yamamoto, M.; Takahashi, H.; Shinomura, Y.; Imai, K.; Saeki, T.; et al. Proposal for a new clinical entity, IgG4-positive multiorgan lymphoproliferative syndrome: Analysis of 64 cases of IgG4-related disorders. Ann. Rheum. Dis. 2009, 68, 1310–1315. [Google Scholar] [CrossRef] [PubMed]
- Taguchi, M.; Kihara, Y.; Nagashio, Y.; Yamamoto, M.; Otsuki, M.; Harada, M. Decreased production of immuno globulin M and A in autoimmune pancreatitis. J. Gastroenterol. 2009, 44, 1133–1139. [Google Scholar] [CrossRef]
- Boonstra, K.; Culver, E.L.; de Buy Wenniger, L.M.; van Heerde, M.J.; van Erpecum, K.J.; Poen, A.C.; van Nieuwkerk, K.M.; Spanier, B.W.; Witteman, B.J.; Tuynman, H.A.; et al. Serum immunoglobulin G4 and immunoglobulin G1 for distinguishing immunoglobulin G4-associated cholangitis from primary sclerosing cholangitis. Hepatology 2014, 59, 1954–1963. [Google Scholar] [CrossRef]
- Zhang, H.; Li, P.; Di Wu, D.X.; Hou, Y.; Wang, Q.; Li, M.; Li, Y.; Zeng, X.; Zhang, F.; Shi, Q. Serum IgG subclasses in autoimmune diseases. Medicine 2015, 94, e387. [Google Scholar] [CrossRef]
- Nakazawa, T.; Ohara, H.; Sano, H.; Ando, T.; Aoki, S.; Kobayashi, S.; Okamoto, T.; Nomura, T.; Joh, T.; Itoh, M. Clinical differences between primary sclerosing cholangitis and sclerosing cholangitis with autoimmune pancreatitis. Pancreas 2005, 30, 20–25. [Google Scholar]
- Nishino, T.; Oyama, H.; Hashimoto, E.; Toki, F.; Oi, I.; Kobayashi, M.; Shiratori, K. Clinicopathological differenti ation between sclerosing cholangitis with autoimmune pancreatitis and primary sclerosing cholangitis. J. Gastroenterol. 2007, 42, 550–559. [Google Scholar] [CrossRef]
- Engelhart, S.; Glynn, R.J.; Schur, P.H. Disease Associations with Isolated Elevations of Each of the Four IgG Sub Classes. In Seminars in Arthritis and Rheumatism; WB Saunders: Philadelphia, PA, USA, 2017; pp. 276–280. [Google Scholar]
- Chan, A.S.; Mudhar, H.; Shen, S.Y.; Lang, S.S.; Fernando, M.; Hilmy, M.H.; Guppy, N.J.; Rennie, I.; Dunkley, L.; Al Jajeh, I. Serum IgG2 and tissue IgG2 plasma cell elevation in orbital IgG4-related disease (IgG4-RD): Potential use in IgG4-RD assessment. Br. J. Ophthalmol. 2017, 101, 1576–1582. [Google Scholar] [CrossRef]
- Lee, Y.-M.; Kaplan, M.M. Primary sclerosing cholangitis. N. Engl. J. Med. 1995, 332, 924–933. [Google Scholar] [CrossRef]
- Björnsson, E.; Chari, S.; Silveira, M.; Gossard, A.; Takahashi, N.; Smyrk, T.; Lindor, K. Primary sclerosing cholan gitis associated with elevated immunoglobulinG4: Clinical characteristics and response to therapy. Am. J. Ther. 2011, 18, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Vidarsson, G.; Dekkers, G.; Rispens, T. IgG subclasses and allotypes: From structure to effector functions. Front. Immunol. 2014, 5, 520. [Google Scholar] [CrossRef] [PubMed]
- Latiff, A.H.A.; Kerr, M.A. The clinical significance of immunoglobulin A deficiency. Ann. Clin. Biochem. 2007, 44, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Lewis, J.T.; Abraham, S.C.; Smyrk, T.C.; Leung, S.; Chari, S.T.; Poterucha, J.J.; Rosen, C.B.; Lohse, C.M.; Katzmann, J.A. IgG4+ plasma cell infiltrates in liver explants with primary sclerosing cholangitis. Am. J. Surg. Pathol. 2010, 34, 88–94. [Google Scholar] [CrossRef]
- Vosskuhl, K.; Negm, A.; Framke, T.; Weismüller, T.; Manns, M.; Wedemeyer, H.; Plentz, R.; Wedemeyer, J.; Lankisch, T. Measurement of IgG4 in bile: A new approach for the diagnosis of IgG4-associated cholangiopathy. Endoscopy 2012, 44, 48–52. [Google Scholar] [CrossRef]
- Parhizkar, B.; Mohammad Alizadeh, A.H.; Asadzadeh Aghdaee, H.; Malekpour, H.; Entezari, A.H. Primary sclerosing cholangitis associated with elevated immunoglobulin-g4: A preliminary study. Int. Sch. Res. Not. 2012, 2012, 325743. [Google Scholar] [CrossRef][Green Version]
- Li, P.; Chen, H.; Deng, C.; Wu, Z.; Lin, W.; Zeng, X.; Zhang, W.; Zhang, F.; Li, Y. Establishment of a serum IgG4 cut-off value for the differential diagnosis of IgG4-related disease in Chinese population. Mod. Rheumatol. 2016, 26, 583–587. [Google Scholar] [CrossRef]
- Ang, T.L.; Fock, K.M.; Ng, T.M.; Teo, E.K.; Chua, T.S.; Tan, J.Y.L. Clinical profile of primary sclerosing cholangitis in Singapore. J. Gastroenterol. Hepatol. 2002, 17, 908–913. [Google Scholar] [CrossRef]
- Tanaka, A.; Takikawa, H. Geoepidemiology of primary sclerosing cholangitis: A critical review. J. Autoimmun. 2013, 46, 35–40. [Google Scholar] [CrossRef]
- Straub, B.K.; Esposito, I.; Gotthardt, D.; Radeleff, B.; Antolovic, D.; Flechtenmacher, C.; Schirmacher, P. IgG4-associated cholangitis with cholangiocarcinoma. Virchows Arch. 2011, 458, 761–765. [Google Scholar] [CrossRef]


{kind=link}
| Variables | IgG4-SC | PSC | CCA | p-Value |
|---|---|---|---|---|
| Number of groups | 31 | 27 | 40 | |
| Age (years) | 65.0 ± 11.9 | 50.3 ± 13.4 | 63.5 ± 8.89 | 0.008 |
| Male | 25 (80.6) | 14 (51.9) | 23 (57.5) | 0.090 |
| IgG1 (mg/dL) | 962.1 ± 460.4 | 846.7 ± 327.0 | 654.9 ± 239.8 | 0.001 |
| IgG2 (mg/dL) | 743.8 ± 343.9 | 586.2 ± 252.3 | 511.0 ± 198.2 | 0.007 |
| IgG3 (mg/dL) | 80.5 ± 79.8 | 74.2 ± 47.8 | 42.5 ± 25.8 | 0.053 |
| IgG4 (mg/dL) | 226.5 ± 184.2 | 37.3 ± 20.1 | 46.5 ± 48.7 | <0.001 |
| IgG4 ≥ 135 mg/dL | 17 (54.8) | 0 (0) | 2 (5) | <0.001 |
| Variables (%) | IgG4 ≥ 135 mg/dL | IgG4 ≥ 68 mg/dL | IgG4/IgG1 ≥ 0.087 | IgG4/(IgG1+IgG3) ≥ 0.081 | (IgG4+IgG2)/ (IgG1+IgG3) ≥ 1.159 |
|---|---|---|---|---|---|
| Sensitivity (95% CI) | 54 (37–70) | 64 (46–78) | 70 (53–83) | 70 (53–83) | 48 (31–65) |
| Specificity (95% CI) | 100 (74–100) | 100 (74–100) | 100 (74–100) | 100 (74–100) | 100 (74–100) |
| PPV (95% CI) | 100 (81–100) | 100 (83–100) | 100 (85–100) | 100 (85–100) | 100(79–100) |
| NPV (95% CI) | 44 (26–62) | 50 (30–69) | 55 (34–74) | 55 (34–74) | 40 (24–59) |
| Accuracy (95% CI) | 66 (51–78) | 73 (58–84) | 78 (64–88) | 78 (64–88) | 61 (46–75) |
| Variables (%) | IgG4 ≥ 135 mg/dL | IgG4 ≥ 52 mg/dL | IgG4/IgG1 ≥ 0.087 | IgG4/(IgG1+IgG3) ≥ 0.081 | (IgG4+IgG2)/ (IgG1+IgG3) ≥ 1.159 |
|---|---|---|---|---|---|
| Sensitivity (95% CI) | 54 (37–70) | 80 (63–90) | 70 (53–83) | 70 (53–83) | 48 (31–65) |
| Specificity (95% CI) | 95 (83–98) | 82 (68–91) | 82 (68–91) | 82 (68–91) | 87 (73–94) |
| PPV (95% CI) | 89 (68–97) | 78 (61–88) | 75 (57–87) | 75 (57–87) | 75 (53–88) |
| NPV (95% CI) | 73 (59–83) | 84 (70–92) | 78 (64–88) | 78 (64–88) | 68 (54–79) |
| Accuracy (95% CI) | 77 (66–85) | 81 (71–88) | 77 (66–85) | 77 (66–85) | 70 (58–79) |
| Variables | AUC (95% CI) |
|---|---|
| IgG4 ≥ 68 mg/dL | 0.827 (0.704–0.950) |
| IgG4/IgG1 ≥ 0.087 | 0.848 (0.732–0.963) |
| IgG4/(IgG1+IgG3) ≥ 0.081 | 0.853 (0.739–0.967) |
| (IgG4+IgG2)/(IgG1+IgG3) ≥ 1.159 | 0.730 (0.572–0.888) |
| Variables | AUC (95% CI) |
|---|---|
| IgG4 ≥ 52 (mg/dL) | 0.826 (0.717–0.935) |
| IgG4/IgG1 ≥ 0.087 | 0.760 (0.639–0.881) |
| IgG4/(IgG1+IgG3) ≥ 0.081 | 0.753 (0.629–0.876) |
| (IgG4+IgG2)/(IgG1+IgG3) ≥ 1.159 | 0.617 (0.478–0.757) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.K.; Kim, D.; Lee, J.M.; Lee, K.H.; Lee, K.T.; Park, J.K.; Lee, J.K. Clinical Utility of Personalized Serum IgG Subclass Ratios for the Differentiation of IgG4-Related Sclerosing Cholangitis (IgG4-SC) from Primary Sclerosing Cholangitis (PSC) and Cholangiocarcinoma (CCA). J. Pers. Med. 2022, 12, 855. https://doi.org/10.3390/jpm12060855
Park JK, Kim D, Lee JM, Lee KH, Lee KT, Park JK, Lee JK. Clinical Utility of Personalized Serum IgG Subclass Ratios for the Differentiation of IgG4-Related Sclerosing Cholangitis (IgG4-SC) from Primary Sclerosing Cholangitis (PSC) and Cholangiocarcinoma (CCA). Journal of Personalized Medicine. 2022; 12(6):855. https://doi.org/10.3390/jpm12060855
Chicago/Turabian StylePark, Jae Keun, Dongwuk Kim, Jeong Min Lee, Kwang Hyuck Lee, Kyu Taek Lee, Joo Kyung Park, and Jong Kyun Lee. 2022. "Clinical Utility of Personalized Serum IgG Subclass Ratios for the Differentiation of IgG4-Related Sclerosing Cholangitis (IgG4-SC) from Primary Sclerosing Cholangitis (PSC) and Cholangiocarcinoma (CCA)" Journal of Personalized Medicine 12, no. 6: 855. https://doi.org/10.3390/jpm12060855
APA StylePark, J. K., Kim, D., Lee, J. M., Lee, K. H., Lee, K. T., Park, J. K., & Lee, J. K. (2022). Clinical Utility of Personalized Serum IgG Subclass Ratios for the Differentiation of IgG4-Related Sclerosing Cholangitis (IgG4-SC) from Primary Sclerosing Cholangitis (PSC) and Cholangiocarcinoma (CCA). Journal of Personalized Medicine, 12(6), 855. https://doi.org/10.3390/jpm12060855