
Interplay between Comprehensive Inflammation Indices and Redox Biomarkers in Testicular Germ-Cell Tumors

 ,
, 
 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Biochemical Assessment
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Elzinga-Tinke, J.E.; Dohle, G.R.; Looijenga, L.H.J. Etiology and early pathogenesis of malignant testicular germ cell tumors: Towards possibilities for preinvasive diagnosis. Asian J. Androl. 2015, 17, 381. [Google Scholar] [CrossRef] [PubMed]
- Winter, C.; Albers, P. Testicular germ cell tumors: Pathogenesis, diagnosis and treatment. Nat. Rev. Endocrinol. 2011, 7, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Batool, A.; Karimi, N.; Wu, X.N.; Chen, S.R.; Liu, Y.X. Testicular germ cell tumor: A comprehensive review. Cell. Mol. Life Sci. 2019, 76, 1713–1727. [Google Scholar] [CrossRef] [PubMed]
- Diakos, C.I.; Charles, K.A.; McMillan, D.C.; Clarke, S.J. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014, 15, e493–e503. [Google Scholar] [CrossRef]
- Proctor, M.J.; Morrison, D.S.; Talwar, D.; Balmer, S.M.; Fletcher, C.D.; O’reilly, D.S.J.; Foulis, A.K.; Horgan, P.G.; Mcmillan, D.C. A comparison of inflammation-based prognostic scores in patients with cancer. A Glasgow Inflammation Outcome Study. Eur. J. Cancer 2011, 47, 2633–2641. [Google Scholar] [CrossRef]
- Yan, Q.; Ertao, Z.; Zhimei, Z.; Weigang, D.; Jianjun, P.; Jianhui, C.; Chuangqi, C. Systemic immune-inflammation index (SII): A More Promising Inflammation-Based Prognostic Marker for Patients with synchronic colorectal peritoneal carcinomatosis. J. Cancer 2020, 11, 5264. [Google Scholar] [CrossRef]
- Yamamoto, T.; Kawada, K.; Obama, K. Inflammation-related biomarkers for the prediction of prognosis in colorectal cancer patients. Int. J. Mol. Sci. 2021, 22, 8002. [Google Scholar] [CrossRef]
- Zhong, J.-H.; Huang, D.-H.; Chen, Z.-Y. Prognostic role of systemic immune-inflammation index in solid tumors: A systematic review and meta-analysis. Oncotarget 2017, 8, 75381–75388. [Google Scholar] [CrossRef] [Green Version]
- Hu, X.; Shao, Y.X.; Yang, Z.Q.; Dou, W.C.; Xiong, S.C.; Li, X. Preoperative systemic immune-inflammation index predicts prognosis of patients with non-metastatic renal cell carcinoma: A propensity score-matched analysis. Cancer Cell Int. 2020, 20, 222. [Google Scholar] [CrossRef]
- Ying, H.Q.; Liao, Y.C.; Sun, F.; Peng, H.X.; Cheng, X.X. The role of cancer-elicited inflammatory biomarkers in predicting early recurrence within stage ii–iii colorectal cancer patients after curable resection. J. Inflamm. Res. 2021, 14, 115–129. [Google Scholar]
- Ohno, Y. Role of systemic inflammatory response markers in urological malignancy. Int. J. Urol. 2019, 26, 31–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mjaess, G.; Chebel, R.; Karam, A.; Moussa, I.; Pretot, D.; Abi Tayeh, G.; Sarkis, J.; Semaan, A.; Peltier, A.; Aoun, F.; et al. Prognostic role of neutrophil-to-lymphocyte ratio (NLR) in urological tumors: An umbrella review of evidence from systematic reviews and meta-analyses. Acta Oncol. 2021, 60, 704–713. [Google Scholar] [CrossRef] [PubMed]
- Bumbasirevic, U.; Bojanic, N.; Pljesa-Ercegovac, M.; Zivkovic, M.; Djukic, T.; Zekovic, M.; Milojevic, B.; Kajmakovic, B.; Janicic, A.; Simic, T.; et al. The Polymorphisms of Genes Encoding Catalytic Antioxidant Proteins Modulate the Susceptibility and Progression of Testicular Germ Cell Tumor. Cancers 2022, 14, 1068. [Google Scholar] [CrossRef] [PubMed]
- Paner, G.P.; Stadler, W.M.; Hansel, D.E.; Montironi, R.; Lin, D.W.; Amin, M.B. Updates in the Eighth Edition of the Tumor-Node-Metastasis Staging Classification for Urologic Cancers. Eur. Urol. 2018, 73, 560–569. [Google Scholar] [CrossRef] [PubMed]
- Williamson, S.R.; Delahunt, B.; Magi-Galluzzi, C.; Algaba, F.; Egevad, L.; Ulbright, T.M.; Tickoo, S.K.; Srigley, J.R.; Epstein, J.I.; Berney, D.M. The World Health Organization 2016 classification of testicular germ cell tumours: A review and update from the International Society of Urological Pathology Testis Consultation Panel. Histopathology 2017, 70, 335–346. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. (Eds.) TNM Classification of Malignant Tumours, 8th ed.; John Wiley & Sons: Hoboken, NJ, USA, 2017; pp. 1–272. [Google Scholar]
- Laguna, M.; Albers, P.; Algaba, F.; Bokemeyer, C.; Boormans, J.; Fischer, S.; Fizazi, K.; Gremmels, H.; Leão, R.; Nicol, D.; et al. EAU Guidelines on Testicular Cancer. In Proceedings of the 36th Annual EAU Congress, Milan, Italy, 19–23 March 2021. [Google Scholar]
- Jocelyn, P.C. Spectrophotometric assay of thiols. In Methods in Enzymology; Elsevier: Amsterdam, The Netherlands, 1987; Volume 143, pp. 44–67. [Google Scholar]
- Walmsley, T.A.; Abernethy, M.H.; Fitzgerald, H.P. Effect of daylight on the reaction of thiols with Ellman’s reagent, 5,5′-dithiobis(2-nitrobenzoic acid). Clin. Chem. 1987, 33, 1928–1931. [Google Scholar] [CrossRef]
- Sionov, R.V.; Fridlender, Z.G.; Granot, Z. The Multifaceted Roles Neutrophils Play in the Tumor Microenvironment. Cancer Microenviron. 2015, 8, 125. [Google Scholar] [CrossRef] [Green Version]
- Bao, Y.; Liu, Z.; Guo, M.; Li, B.; Sun, X.; Wang, L. Extramedullary hematopoiesis secondary to malignant solid tumors: A case report and literature review. Cancer Manag. Res. 2018, 10, 1461. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Zhang, W.; Yuan, X.; Fu, M.; Qian, H.; Xu, W. Neutrophils in cancer development and progression: Roles, mechanisms, and implications (Review). Int. J. Oncol. 2016, 49, 857–867. [Google Scholar] [CrossRef] [Green Version]
- Hedrick, C.C.; Malanchi, I. Neutrophils in cancer: Heterogeneous and multifaceted. Nat. Rev. Immunol. 2021, 22, 73–187. [Google Scholar] [CrossRef] [PubMed]
- Schepisi, G.; Santoni, M.; Massari, F.; Gurioli, G.; Salvi, S.; Conteduca, V.; Montironi, R.; De Giorgi, U. Urothelial Cancer: Inflammatory Mediators and Implications for Immunotherapy. BioDrugs 2016, 30, 263–273. [Google Scholar] [CrossRef] [PubMed]
- Menter, D.G.; Kopetz, S.; Hawk, E.; Sood, A.K.; Loree, J.M.; Gresele, P.; Honn, K.V. Platelet “First Responders” in Wound Response, Cancer, and Metastasis. Cancer Metastasis Rev. 2017, 36, 199. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.; Karin, M.; Sun, B. Targeting cancer-promoting inflammation—Have anti-inflammatory therapies come of age? Nat. Rev. Clin. Oncol. 2021, 18, 261–279. [Google Scholar] [CrossRef] [PubMed]
- Gay, L.J.; Felding-Habermann, B. Contribution of Platelets to Tumor Metastasis. Nat. Rev. Cancer 2011, 11, 123. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; She, D.L.; Xiong, H.; Fu, S.J.; Yang, L. Pretreatment neutrophil to lymphocyte ratio as a prognostic predictor of urologic tumors: A systematic review and meta-analysis. Medicine 2015, 94, e1670. [Google Scholar] [CrossRef]
- Wei, Y.; Jiang, Y.Z.; Qian, W.H. Prognostic Role of NLR in Urinary Cancers: A Meta-Analysis. PLoS ONE 2014, 9, e92079. [Google Scholar] [CrossRef]
- Huang, Y.; Gao, Y.; Wu, Y.; Lin, H. Prognostic value of systemic immune-inflammation index in patients with urologic cancers: A meta-analysis. Cancer Cell Int. 2020, 20, 499. [Google Scholar] [CrossRef]
- Yuksel, O.H.; Verit, A.; Sahin, A.; Urkmez, A.; Uruc, F. White blood cell counts and neutrophil to lymphocyte ratio in the diagnosis of testicular cancer: A simple secondary serum tumor marker. Int. Braz. J. Urol. 2016, 42, 53–59. [Google Scholar] [CrossRef]
- Gokcen, K.; Dundar, G.; Gulbahar, H.; Gokce, G.; Gultekin, E. Can routine peripheral blood counts like neutrophil-to-lymphocyte ratio be beneficial in prediagnosis of testicular cancer and its stages? J. Res. Med. Sci. 2018, 23, 64. [Google Scholar]
- Tan, Y.G.; Sia, J.; Huang, H.H.; Lau, W.K.O. Neutrophil-to-lymphocyte ratio independently predicts advanced pathological staging and poorer survival outcomes in testicular cancer. Investig. Clin. Urol. 2019, 60, 176. [Google Scholar] [CrossRef] [PubMed]
- Herraiz-Raya, L.; Moreillo-Vicente, L.; Martínez-Ruiz, J.; Agustí-Martínez, A.; Fernández-Anguita, P.J.; Esper-Rueda, J.A.; Salce-Marte, L.; Armas-Álvarez, A.; Díaz de Mera-Sánchez Migallón, I.; Martínez-Alfaro, C.; et al. Leukocyte and platelet counts as prognostic values of testicular germ cell tumours. Actas Urol. Esp. 2019, 43, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Jankovich, M.; Jankovichova, T.; Ondrus, D.; Breza, J. Neutrophil-to-lymphocyte ratio as a predictor of preoperative tumor staging in testicular germ cell tumors. Bratisl. Lek. Listy 2017, 118, 510–512. [Google Scholar] [CrossRef] [PubMed]
- Fankhauser, C.D.; Sander, S.; Roth, L.; Gross, O.; Eberli, D.; Sulser, T.; Seifert, B.; Beyer, J.; Hermanns, T. Systemic inflammatory markers have independent prognostic value in patients with metastatic testicular germ cell tumours undergoing first-line chemotherapy. Br. J. Cancer 2018, 118, 825–830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juan, C.A.; de la Lastra, J.M.P.; Plou, F.J.; Pérez-Lebeña, E. The Chemistry of Reactive Oxygen Species (ROS) Revisited: Outlining Their Role in Biological Macromolecules (DNA, Lipids and Proteins) and Induced Pathologies. Int. J. Mol. Sci. 2021, 22, 4642. [Google Scholar] [CrossRef] [PubMed]
- Baba, S.P.; Bhatnagar, A. Role Of Thiols in Oxidative Stress. Curr. Opin. Toxicol. 2018, 7, 133. [Google Scholar] [CrossRef] [PubMed]
- Hanikoglu, F.; Hanikoglu, A.; Kucuksayan, E.; Alisik, M.; Gocener, A.A.; Erel, O.; Baykara, M.; Cuoghi, A.; Tomasi, A.; Ozben, T. Dynamic thiol/disulphide homeostasis before and after radical prostatectomy in patients with prostate cancer. Free. Radic. Res. 2016, 50, S79–S84. [Google Scholar] [CrossRef] [Green Version]
- Dirican, N.; Dirican, A.; Sen, O.; Aynali, A.; Atalay, S.; Bircan, H.A.; Oztürk, O.; Erdogan, S.; Cakir, M.; Akkaya, A. Thiol/disulfide homeostasis: A prognostic biomarker for patients with advanced non-small cell lung cancer? Redox Rep. 2016, 21, 197–203. [Google Scholar] [CrossRef] [Green Version]
- Bilgin, B.; Sendur, M.A.; Hizal, M.; Kandil, S.U.; Yaman, S.; Akıncı, M.B.; Dede, D.Ş.; Neselioglu, S.; Erel, Ö.; Yalçın, B. Evaluation of dynamic serum thiol-disulphide homeostasis in colorectal cancer. J. Oncol. Sci. 2019, 5, 60–64. [Google Scholar] [CrossRef]
- Mukthapura, A.; Shimogga, A.; Sudha, K.V.; Shetty, B.; Rao, G.M. Oxidative products of proteins and antioxidant potential of thiols in gastric carcinoma patients. J. Med. Biochem. 2010, 29, 102–106. [Google Scholar] [CrossRef] [Green Version]
- Suh, B.; Park, S.; Shin, D.W.; Yun, J.M.; Keam, B.; Yang, H.K.; Ahn, E.; Lee, H.; Park, J.H.; Cho, B. Low albumin-to-globulin ratio associated with cancer incidence and mortality in generally healthy adults. Ann. Oncol. 2014, 25, 2260–2266. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Chen, S.; Geng, Q.; Liu, X.; Kong, P.; Zhan, Y.; Xu, D. Prognostic value of pretreatment albumin–globulin ratio in predicting long-term mortality in gastric cancer patients who underwent D2 resection. Onco. Targets. Ther. 2017, 10, 2155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabata, F.; Wada, Y.; Kawakami, S.; Miyaji, K. Serum albumin redox states: More than oxidative stress biomarker. Antioxidants 2021, 10, 503. [Google Scholar] [CrossRef] [PubMed]
- Rajab, I.M.; Hart, P.C.; Potempa, L.A. How C-Reactive Protein Structural Isoforms With Distinctive Bioactivities Affect Disease Progression. Front. Immunol. 2020, 11, 2126. [Google Scholar] [CrossRef]
- Hart, P.C.; Rajab, I.M.; Alebraheem, M.; Potempa, L.A. C-Reactive Protein and Cancer—Diagnostic and Therapeutic Insights. Front. Immunol. 2020, 11, 595835. [Google Scholar] [CrossRef]
- Bartsch, H.; Nair, J. Chronic inflammation and oxidative stress in the genesis and perpetuation of cancer: Role of lipid peroxidation, DNA damage, and repair. Langenbeck’s Arch. Surg. 2006, 391, 499–510. [Google Scholar]
- Biswas, S.K. Does the Interdependence between Oxidative Stress and Inflammation Explain the Antioxidant Paradox? Oxid. Med. Cell. Longev. 2016, 2016, 5698931. [Google Scholar] [CrossRef] [Green Version]
- Kino, K.; Hirao-Suzuki, M.; Morikawa, M.; Sakaga, A.; Miyazawa, H. Generation, repair and replication of guanine oxidation products. Genes Environ. 2017, 39, 21. [Google Scholar] [CrossRef]
- Singh, A.; Kukreti, R.; Saso, L.; Kukreti, S. Oxidative stress: Role and response of short guanine tracts at genomic locations. Int. J. Mol. Sci. 2019, 20, 4258. [Google Scholar] [CrossRef] [Green Version]
- Kino, K.; Kawada, T.; Hirao-Suzuki, M.; Morikawa, M.; Miyazawa, H. Products of oxidative guanine damage form base pairs with guanine. Int. J. Mol. Sci. 2020, 21, 7645. [Google Scholar] [CrossRef]
- Valavanidis, A.; Vlachogianni, T.; Fiotakis, C. 8-Hydroxy-2′ -deoxyguanosine (8-OHdG): A critical biomarker of oxidative stress and carcinogenesis. J. Environ. Sci. Health Part C 2009, 27, 120–139. [Google Scholar] [CrossRef] [Green Version]
- Wiseman, H.; Halliwell, B. Damage to DNA by reactive oxygen and nitrogen species: Role in inflammatory disease and progression to cancer. Biochem. J. 1996, 313, 17–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shukla, S.; Srivastava, J.K.; Shankar, E.; Kanwal, R.; Nawab, A.; Sharma, H.; Bhaskaran, N.; Ponsky, L.E.; Fu, P.; MacLennan, G.T.; et al. Oxidative stress and antioxidant status in high-risk prostate cancer subjects. Diagnostics 2020, 10, 126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chuma, M.; Hige, S.; Nakanishi, M.; Ogawa, K.; Natsuizaka, M.; Yamamoto, Y.; Asaka, M. 8-Hydroxy-2′-deoxy-guanosine is a risk factor for development of hepatocellular carcinoma in patients with chronic hepatitis C virus infection. J. Gastroenterol. Hepatol. 2008, 23, 1431–1436. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.; Wang, F.; Zhao, Y.S.; Pan, H.Z. Evaluation of oxidative stress in colorectal cancer patients. Biomed. Environ. Sci. 2008, 21, 286–289. [Google Scholar] [CrossRef]
- Bahar, G.; Feinmesser, R.; Shpitzer, T.; Popovtzer, A.; Nagler, R.M. Salivary analysis in oral cancer patients: DNA and protein oxidation, reactive nitrogen species, and antioxidant profile. Cancer 2007, 109, 54–59. [Google Scholar] [CrossRef]
- Kubo, N.; Morita, M.; Nakashima, Y.; Kitao, H.; Egashira, A.; Saeki, H.; Oki, E.; Kakeji, Y.; Oda, Y.; Maehara, Y. Oxidative DNA damage in human esophageal cancer: Clinicopathological analysis of 8-hydroxydeoxyguanosine and its repair enzyme. Dis. Esophagus 2014, 27, 285–293. [Google Scholar] [CrossRef]
- Ma, Y.; Zhang, L.; Rong, S.; Qu, H.; Zhang, Y.; Chang, D.; Pan, H.; Wang, W. Relation between gastric cancer and protein oxidation, DNA damage, and lipid peroxidation. Oxid. Med. Cell. Longev. 2013, 2013, 543760. [Google Scholar] [CrossRef]
- Kumar, A.; Pant, M.C.; Singh, H.S.; Khandelwal, S. Determinants of oxidative stress and DNA damage (8-OhdG) in squamous cell carcinoma of head and neck. Indian J. Cancer 2012, 49, 309–315. [Google Scholar]
- Qing, X.; Shi, D.; Lv, X.; Wang, B.; Chen, S.; Shao, Z. Prognostic significance of 8-hydroxy-2′-deoxyguanosine in solid tumors: A meta-analysis. BMC Cancer 2019, 19, 997. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Parameters | Patients with Testicular GCT, n = 88 |
|---|---|
| Age (years) | 34 (19–54) 1 |
| Charlsoncomorbidity index, CCI | 0 (0–1) 1 |
| Body mass index, n (%) 2 | 24.9 (17.6–36.1) 1 |
| <30 kg/m2 | 73 (88) |
| >30 kg/m2 | 10 (12) |
| Smoking status, n (%) 2 | |
| Non-smokers | 36 (44) |
| Smokers | 45 (56) |
| Tumor type, n (%) | |
| Seminoma | 52 (59) |
| Non-seminoma | 36 (41) |
| Clinical stage, n (%) | |
| I | 61 (69) |
| II | 18 (21) |
| III | 9 (10) |
| Laboratory Parameter | Stage I | Stages II + III | p-Value |
|---|---|---|---|
| Neutrophils (n × 109/L) | 4.55 (1.80–13.00) | 5.20 (2.70–12.22) | 0.077 |
| Lymphocytes (n × 109/L) | 1.90 (1.10–3.00) | 1.60 (0.40–3.32) | 0.183 |
| NLR | 2.28 (0.72–11.82) | 3.28 (1.65–16.00) | 0.005 * |
| dNLR | 1.71 (0.58–4.64) | 2.18 (1.18–5.77) | 0.031 * |
| Platelets (n × 109/L) | 234.00 (102.00–412.00) | 260.00 (148.00–562.00) | 0.177 |
| PLR | 123.68 (67.27–283.64) | 163.50 (51.61–640.00) | 0.008 * |
| SII (×109/L) | 533.33 (145.71–3687.27) | 824.26 (268.39–4096.00) | 0.001 * |
| SIRI (×109/L) | 1.06 (0.29–16.36) | 1.65 (0.58–6.42) | 0.001 * |
| Monocytes (n × 109/L) | 0.48 (0.10–1.30) | 0.50 (0.30–1.45) | 0.117 |
| LMR | 4.20 (0.85–13.00) | 3.20 (1.00–5.33) | 0.001 * |
| CRP (mg/L) | 0.80 (0.20–301.00) | 2.45 (0.20–197.50) | 0.008 * |
| AGR | 1.84 (1.23–2.78) | 1.62 (0.88–2.35) | 0.009 * |
| 8-OHdG (ng/mL) | 9.25 (5.07–49.50) | 8.51 (4.29–16.48) | 0.373 |
| Thiol groups (ng/mL) | 9.65 (4.98–218.86) | 10.16 (5.93–14.89) | 0.914 |
| MDA (ng/mL) | 94.01 (41.02–302.85) | 98.02 (55.34–372.06) | 0.208 |
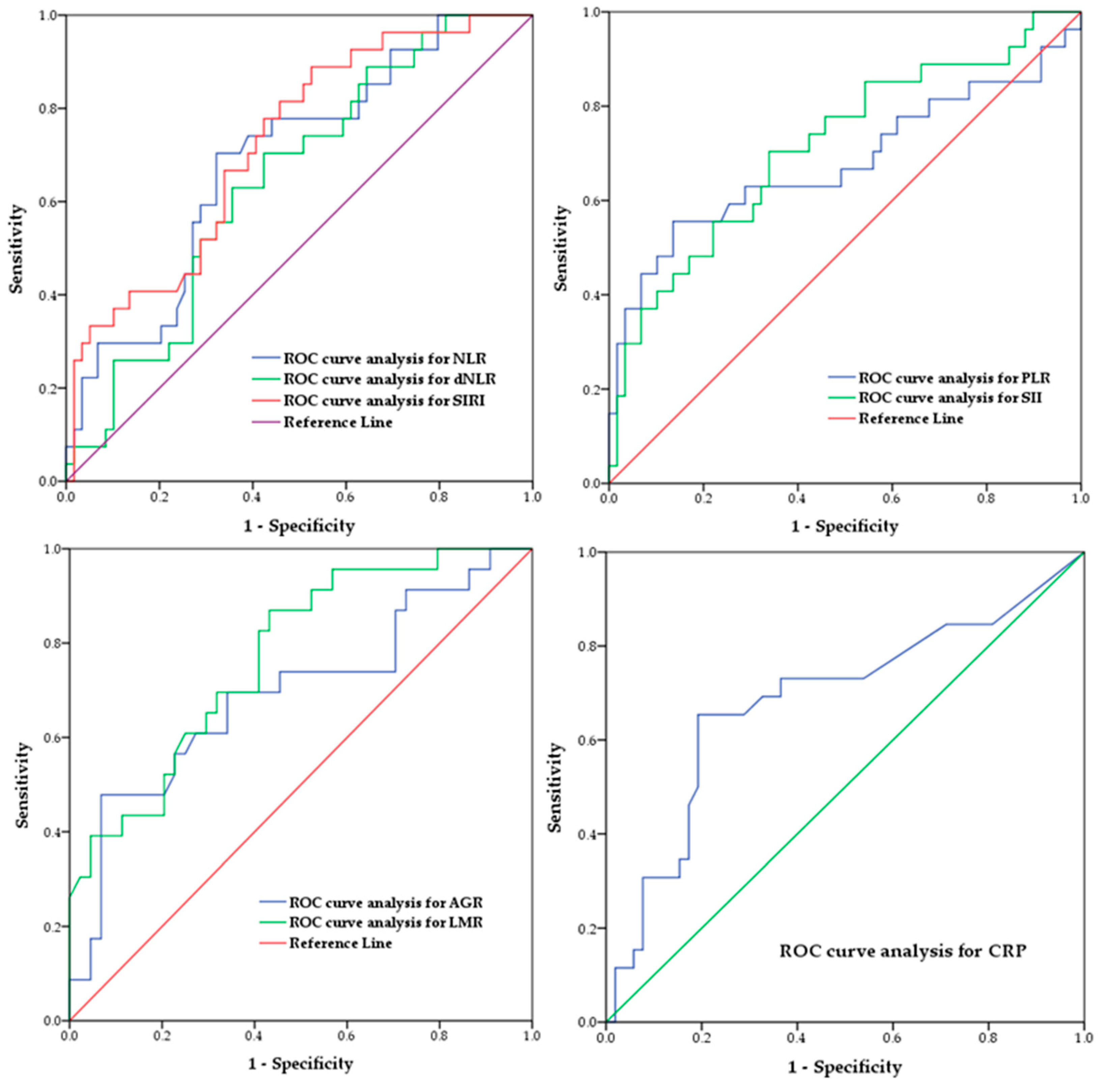
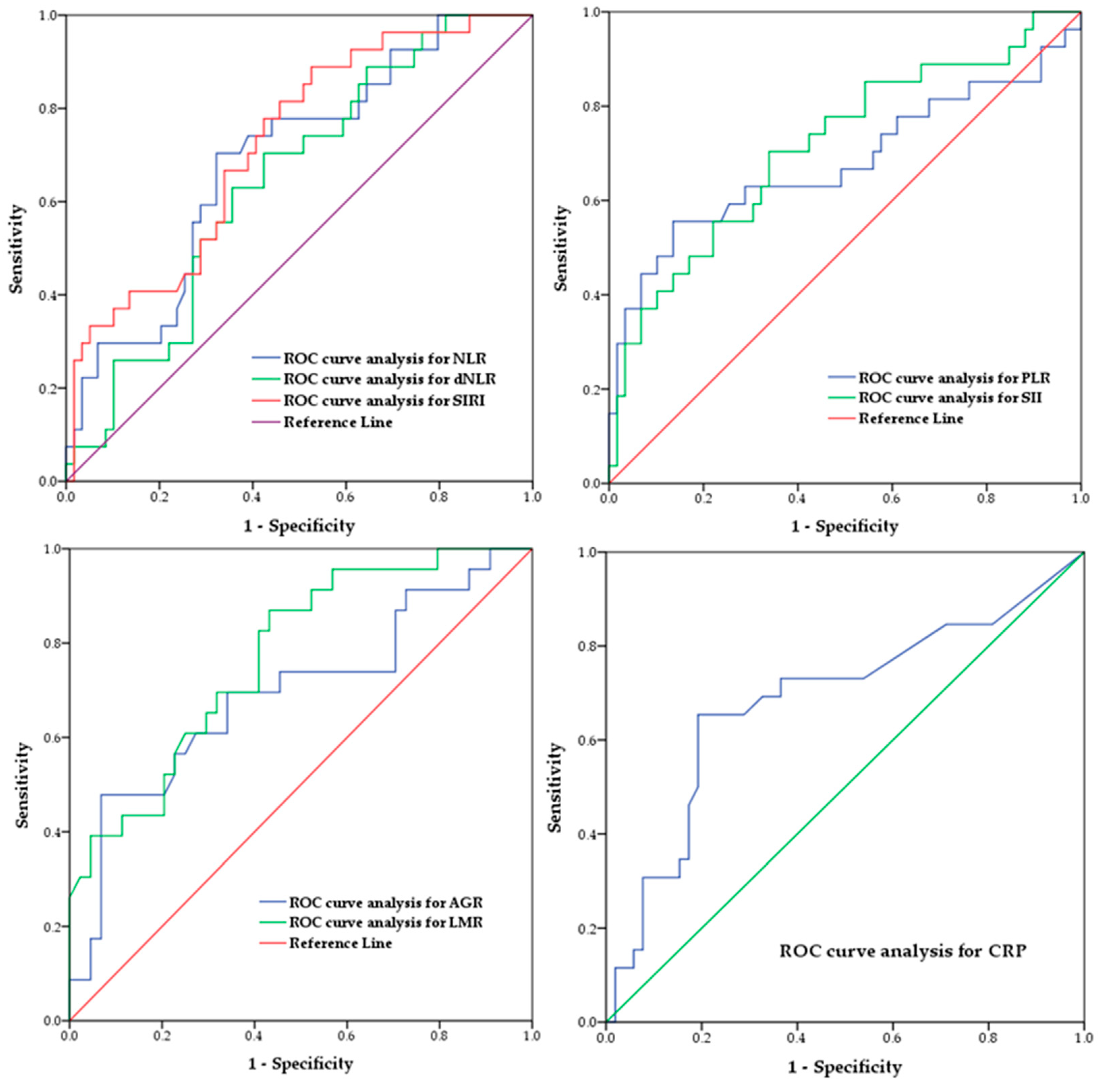
| Inflammatory Index | Cut-Off Point | AUC | p-Value | CI | Specificity (%) | Sensitivity (%) |
|---|---|---|---|---|---|---|
| NLR | 2.685 | 0.691 | 0.05 * | 0.573–0.809 | 67.79 | 70.37 |
| dNLR | 1.775 | 0.646 | 0.031 * | 0.527–0.765 | 57.62 | 70.37 |
| PLR | 160.170 | 0.680 | 0.008 * | 0.539–0.820 | 86.44 | 55.55 |
| LMR | 4.145 | 0.730 | 0.001 * | 0.618–0.842 | 50.84 | 85.18 |
| SII (×109/L) | 683.21 | 0.714 | 0.001 * | 0.549–0.836 | 66.10 | 70.37 |
| SIRI (×109/L) | 1.005 | 0.723 | 0.001 * | 0.612–0.835 | 47.45 | 88.88 |
| CRP (mg/L) | 2.100 | 0.684 | 0.008 * | 0.549–0.819 | 80.76 | 65.38 |
| AGR | 1.530 | 0.695 | 0.009 * | 0.554–0.838 | 93.18 | 44.82 |
| Laboratory Parameter | 8-OHdG (ng/mL) Rho/p-Value | Thiol Groups (µmol/g) Rho/p-Value | MDA (ng/mL) Rho/p-Value |
|---|---|---|---|
| Neutrophils (n × 109/L) | 0.157/0.172 | −0.173/0.115 | 0.050/0.666 |
| Lymphocytes (n × 109/L) | −0.142/0.217 | −0.142/0.197 | −0.062/0.595 |
| NLR | 0.210/0.067 | −0.069/0.531 | 0.153/0.187 |
| dNLR | 0.214/0.061 | −0.062/0.575 | 0.130/0.262 |
| Platelets (n × 109/L) | 0.004/0.974 | −0.183/0.096 | 0.088/0.450 |
| PLR | 0.132/0.252 | 0.000/0.997 | 0.194/0.094 |
| SII (×109/L) | 0.209/0.068 | −0.118/0.299 | 0.182/0.116 |
| SIRI (×109/L) | 0.144/0.210 | −0.129/0.243 | 0.101/0.385 |
| Monocytes (n × 109/L) | −0.078/0.499 | −0.132/0.233 | −0.080/0.493 |
| LMR | −0.115/0.320 | 0.003/0.975 | −0.094/0.417 |
| CRP (mg/L) | 0.109/0.361 | −0.234/0.042 * | −0.049/0.688 |
| AGR | −0.041/0.753 | 0.278/0.025 * | 0.002/0.987 |
| Laboratory Parameter | Tumor Maximal Dimension Rho/p-Value |
|---|---|
| Neutrophils (n × 109/L) | 0.175/0.107 |
| Lymphocytes (n × 109/L) | −0.038/0.730 |
| NLR | 0.174/0.110 |
| dNLR | 0.173/0.110 |
| Platelets (n × 109/L) | 0.018/0.869 |
| PLR | −0.004/0.971 |
| SII (×109/L) | 0.104/0.339 |
| SIRI (×109/L) | 0.120/0.273 |
| Monocytes (n × 109/L) | 0.094/0.389 |
| LMR | −0.041/0.711 |
| CRP (mg/L) | 0.246/0.030 * |
| AGR | −0.263/0.031 * |
| 8-OHdG (ng/mL) | 0.040/0.729 |
| Thiol groups(ng/mL) | 0.064/0.556 |
| MDA (ng/mL) | 0.160/0.162 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bumbasirevic, U.; Bojanic, N.; Simic, T.; Milojevic, B.; Zivkovic, M.; Kosanovic, T.; Kajmakovic, B.; Janicic, A.; Durutovic, O.; Radovanovic, M.; et al. Interplay between Comprehensive Inflammation Indices and Redox Biomarkers in Testicular Germ-Cell Tumors. J. Pers. Med. 2022, 12, 833. https://doi.org/10.3390/jpm12050833
Bumbasirevic U, Bojanic N, Simic T, Milojevic B, Zivkovic M, Kosanovic T, Kajmakovic B, Janicic A, Durutovic O, Radovanovic M, et al. Interplay between Comprehensive Inflammation Indices and Redox Biomarkers in Testicular Germ-Cell Tumors. Journal of Personalized Medicine. 2022; 12(5):833. https://doi.org/10.3390/jpm12050833
Chicago/Turabian StyleBumbasirevic, Uros, Nebojsa Bojanic, Tatjana Simic, Bogomir Milojevic, Marko Zivkovic, Tijana Kosanovic, Boris Kajmakovic, Aleksandar Janicic, Otas Durutovic, Milan Radovanovic, and et al. 2022. "Interplay between Comprehensive Inflammation Indices and Redox Biomarkers in Testicular Germ-Cell Tumors" Journal of Personalized Medicine 12, no. 5: 833. https://doi.org/10.3390/jpm12050833
APA StyleBumbasirevic, U., Bojanic, N., Simic, T., Milojevic, B., Zivkovic, M., Kosanovic, T., Kajmakovic, B., Janicic, A., Durutovic, O., Radovanovic, M., Santric, V., Zekovic, M., & Coric, V. (2022). Interplay between Comprehensive Inflammation Indices and Redox Biomarkers in Testicular Germ-Cell Tumors. Journal of Personalized Medicine, 12(5), 833. https://doi.org/10.3390/jpm12050833