
Anorexia Nervosa: Reduction in Depression during Inpatient Treatment Is Closely Related to Reduction in Eating Disorder Psychopathology



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
- -
- adult individuals (age 18–65 years);
- -
- admitted to the ED unit at the Psychiatric Center Ballerup, in Denmark;
- -
- a diagnosis of an ED.
2.2. Weight Restoration Treatment
2.3. Clinical and Psychometric Measures
2.4. Measurements of Depression
2.5. Eating Disorder Psychopathology
2.6. Statistical Analysis
3. Results
3.1. Participants’ Baseline Clinical Characteristics and ED Psychopathology
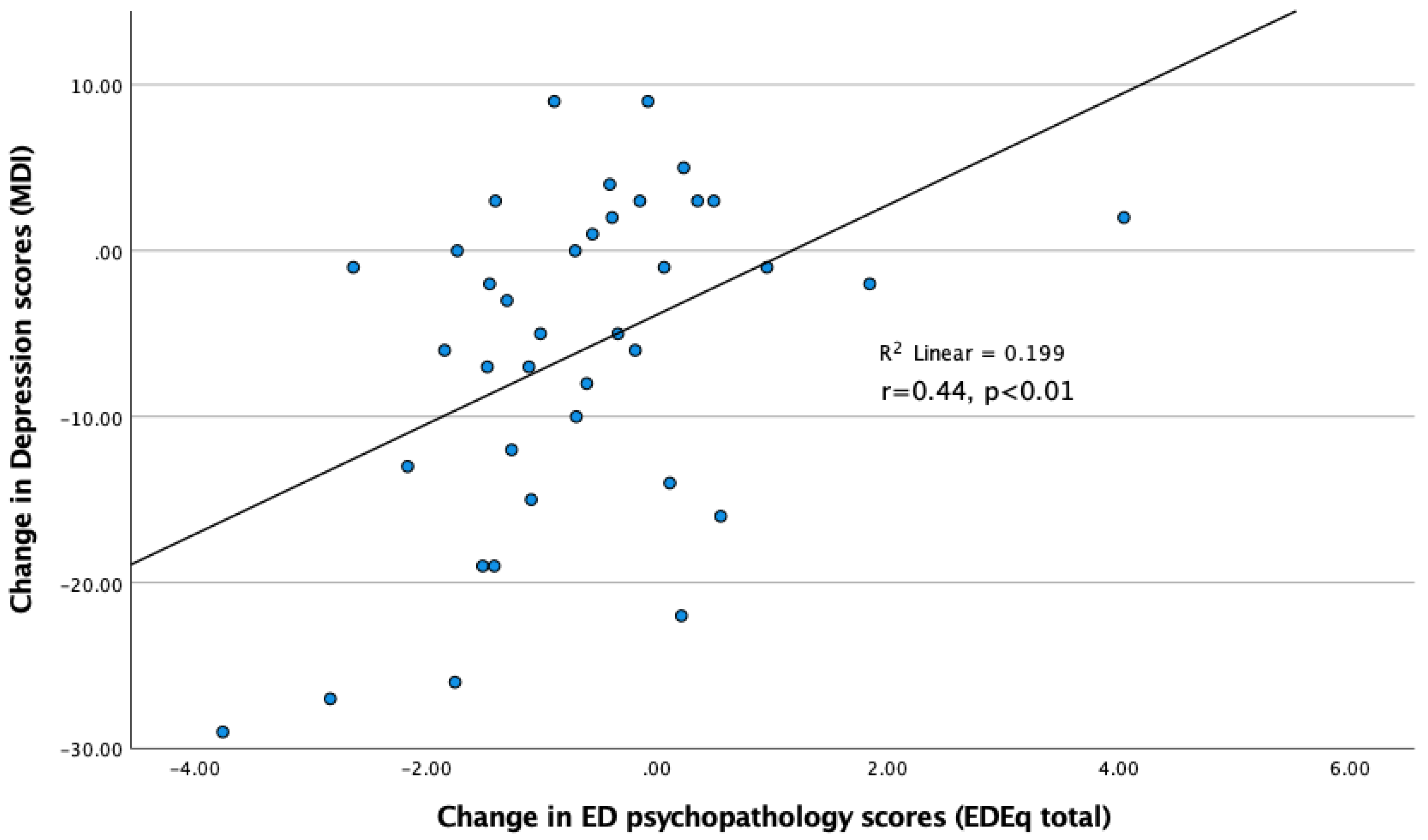
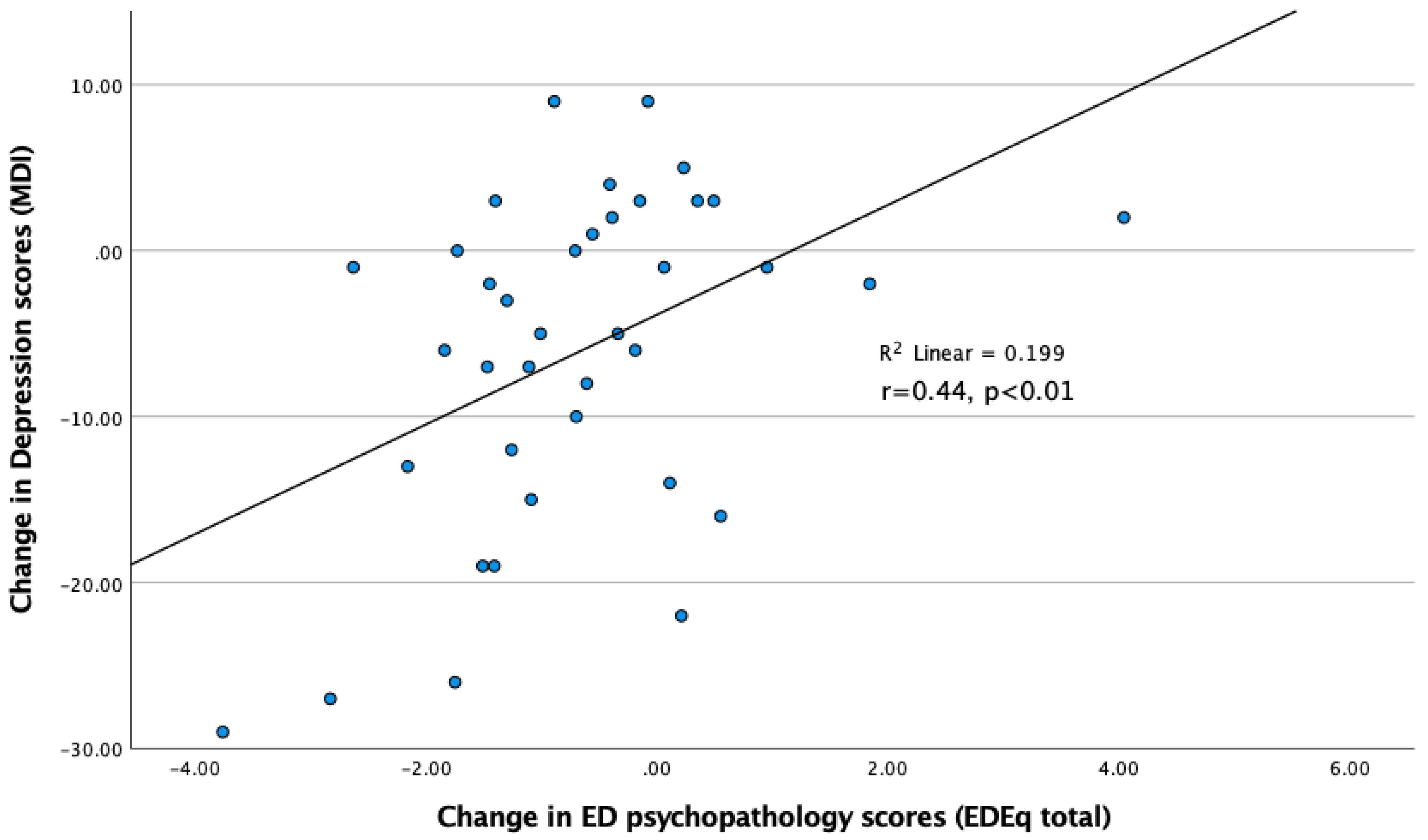
3.2. Depression Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Anatomical Therapeutic Chemical Classification System | ATC |
| Anorexia nervosa | AN |
| Body Mass Index | BMI |
| Eating Disorders | ED |
| Eating Disorder Examination Questionnaire | EDE-Q |
| Eating Disorder Inventory | EDI |
| for example | e.g. |
| value on the F distribution | f |
| ideal body weight | IBW |
| kilogram | kg |
| that is | i.e. |
| International Classification of Disorders-tenth edition | ICD-10 |
| Major Depression Inventory | MDI |
| meter | m |
| non-significant | ns |
| number of individuals | n |
| post meridiem | pm |
| PROspective Longitudinal all-comer inclusion study on Eating Disorders | PROLED |
| Psychiatric Center Ballerup | PCB |
| Standard Deviation | SD |
| Statistical Package for Social Sciences | SPSS |
| University of British Colombia | UBC |
| week | w |
References
- Zipfel, S.; Giel, K.E.; Bulik, C.M.; Hay, P.; Schmidt, U. Anorexia nervosa: Aetiology, assessment, and treatment. Lancet Psychiatry 2015, 2, 1099–1111. [Google Scholar] [CrossRef]
- Treasure, J.; Zipfel, S.; Micali, N.; Wade, T.; Stice, E.; Claudino, A.; Schmidt, U.; Frank, G.K.; Bulik, C.M.; Wentz, E. Anorexia nervosa. Nat. Rev. Dis. Primers 2015, 1, 15074. [Google Scholar] [CrossRef] [PubMed]
- Klump, K.L.; Bulik, C.M.; Kaye, W.H.; Treasure, J.; Tyson, E. Academy for eating disorders position paper: Eating disorders are serious mental illnesses. Int. J. Eat. Disord. 2009, 42, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Jagielska, G.; Kacperska, I. Outcome, comorbidity and prognosis in anorexia nervosa. Psychiatr. Pol. 2017, 51, 205–218. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulos, F.C.; Ekbom, A.; Brandt, L.; Ekselius, L. Excess mortality, causes of death and prognostic factors in anorexia nervosa. Br. J. Psychiatry 2009, 194, 10–17. [Google Scholar] [CrossRef] [Green Version]
- Redgrave, G.W.; Schreyer, C.C.; Coughlin, J.W.; Fischer, L.K.; Pletch, A.; Guarda, A.S. Discharge Body Mass Index, Not Illness Chronicity, Predicts 6-Month Weight Outcome in Patients Hospitalized With Anorexia Nervosa. Front. Psychiatry 2021, 12, 641861. [Google Scholar] [CrossRef]
- Blinder, B.J.; Cumella, E.J.; Sanathara, V.A. Psychiatric comorbidities of female inpatients with eating disorders. Psychosom. Med. 2006, 68, 454–462. [Google Scholar] [CrossRef]
- Plana-Ripoll, O.; Pedersen, C.B.; Holtz, Y.; Benros, M.E.; Dalsgaard, S.; de Jonge, P.; Fan, C.C.; Degenhardt, L.; Ganna, A.; Greve, A.N.; et al. Exploring Comorbidity Within Mental Disorders Among a Danish National Population. JAMA Psychiatry 2019, 76, 259–270. [Google Scholar] [CrossRef] [Green Version]
- Kask, J.; Ekselius, L.; Brandt, L.; Kollia, N.; Ekbom, A.; Papadopoulos, F.C. Mortality in Women With Anorexia Nervosa: The Role of Comorbid Psychiatric Disorders. Psychosom. Med. 2016, 78, 910–919. [Google Scholar] [CrossRef]
- Mattar, L.; Huas, C.; group, E.; Godart, N. Relationship between affective symptoms and malnutrition severity in severe Anorexia Nervosa. PLoS ONE 2012, 7, e49380. [Google Scholar] [CrossRef] [Green Version]
- Pleple, A.; Lalanne, C.; Huas, C.; Mattar, L.; Hanachi, M.; Flament, M.F.; Carchon, I.; Jouen, F.; Berthoz, S.; Godart, N. Nutritional status and anxious and depressive symptoms in anorexia nervosa: A prospective study. Sci. Rep. 2021, 11, 771. [Google Scholar] [CrossRef]
- El Ghoch, M.; Milanese, C.; Calugi, S.; Pellegrini, M.; Battistini, N.C.; Dalle Grave, R. Body composition, eating disorder psychopathology, and psychological distress in anorexia nervosa: A longitudinal study. Am. J. Clin. Nutr. 2014, 99, 771–778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayer, L.; Walsh, B.T.; Pierson, R.N., Jr.; Heymsfield, S.B.; Gallagher, D.; Wang, J.; Parides, M.K.; Leibel, R.L.; Warren, M.P.; Killory, E.; et al. Body fat redistribution after weight gain in women with anorexia nervosa. Am. J. Clin. Nutr. 2005, 81, 1286–1291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, E.S.; Kim, Y.H.; Beck, S.H.; Lee, S.; Oh, S.W. Depressive mood and abdominal fat distribution in overweight premenopausal women. Obes. Res. 2005, 13, 320–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bornstein, S.R.; Schuppenies, A.; Wong, M.L.; Licinio, J. Approaching the shared biology of obesity and depression: The stress axis as the locus of gene-environment interactions. Mol. Psychiatry 2006, 11, 892–902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayer, L. Body composition and anorexia nervosa: Does physiology explain psychology? Am. J. Clin. Nutr. 2001, 73, 851–852. [Google Scholar] [CrossRef] [Green Version]
- Eskild-Jensen, M.; Stoving, R.K.; Flindt, C.F.; Sjogren, M. Comorbid depression as a negative predictor of weight gain during treatment of anorexia nervosa: A systematic scoping review. Eur. Eat. Disord. Rev. 2020, 28, 605–619. [Google Scholar] [CrossRef]
- Sjögren, M.; Kizilkaya, I.; Støving, R.K. Inpatient Weight Restoration Treatment Is Associated with Decrease in Post-Meal Anxiety. J. Pers. Med. 2021, 11, 1079. [Google Scholar] [CrossRef]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 10th ed.; World Health Organization: Geneva, Switzerland, 1992; Volume 2019. [Google Scholar]
- Bech, P.; Christensen, E.M.; Vinberg, M.; Ostergaard, S.D.; Martiny, K.; Kessing, L.V. The performance of the revised Major Depression Inventory for self-reported severity of depression--implications for the DSM-5 and ICD-11. Psychother. Psychosom. 2013, 82, 187–188. [Google Scholar] [CrossRef]
- Fairburn, C.G. Assessment of eating disorders: Interview or self-report questionnaire? Int. J. Eat. Disord. 1994, 16, 363–370. [Google Scholar] [CrossRef]
- Garner, D.M.; Olmstead, M.P.; Polivy, J. Development and validation of a multidimensional eating disorder inventory for anorexia nervosa and bulimia. Int. J. Eat. Disord. 1983, 2, 15–34. [Google Scholar] [CrossRef]
- Bech, P.; Bille, J.; Moller, S.B.; Hellstrom, L.C.; Ostergaard, S.D. Psychometric validation of the Hopkins Symptom Checklist (SCL-90) subscales for depression, anxiety, and interpersonal sensitivity. J. Affect. Disord. 2014, 160, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Janca, A.; Ustun, T.B.; Early, T.S.; Sartorius, N. The ICD-10 symptom checklist: A companion to the ICD-10 classification of mental and behavioural disorders. Soc. Psychiatry Psychiatr. Epidemiol. 1993, 28, 239–242. [Google Scholar] [CrossRef]
- Morgan, J.F.; Lacey, J.H.; Reid, F. Anorexia nervosa: Changes in sexuality during weight restoration. Psychosom. Med. 1999, 61, 541–545. [Google Scholar] [CrossRef]
- Meehan, K.G.; Loeb, K.L.; Roberto, C.A.; Attia, E. Mood change during weight restoration in patients with anorexia nervosa. Int. J. Eat. Disord. 2006, 39, 587–589. [Google Scholar] [CrossRef] [PubMed]
- Steinhausen, H.C.; Villumsen, M.D.; Horder, K.; Winkler, L.A.; Bilenberg, N.; Stoving, R.K. Comorbid mental disorders during long-term course in a nationwide cohort of patients with anorexia nervosa. Int. J. Eat. Disord. 2021, 54, 1608–1618. [Google Scholar] [CrossRef]
- Hay, P.J.; Touyz, S.; Claudino, A.M.; Lujic, S.; Smith, C.A.; Madden, S. Inpatient versus outpatient care, partial hospitalisation and waiting list for people with eating disorders. Cochrane Database Syst. Rev. 2019, 1, CD010827. [Google Scholar] [CrossRef]
- Hubert, T.; Pioggiosi, P.; Huas, C.; Wallier, J.; Maria, A.S.; Apfel, A.; Curt, F.; Falissard, B.; Godart, N. Drop-out from adolescent and young adult inpatient treatment for anorexia nervosa. Psychiatry Res. 2013, 209, 632–637. [Google Scholar] [CrossRef]
- Abd Elbaky, G.B.; Hay, P.J.; le Grange, D.; Lacey, H.; Crosby, R.D.; Touyz, S. Pre-treatment predictors of attrition in a randomised controlled trial of psychological therapy for severe and enduring anorexia nervosa. BMC Psychiatry 2014, 14, 69. [Google Scholar] [CrossRef] [Green Version]
- Konstantinidis, A.; Martiny, K.; Bech, P.; Kasper, S. A comparison of the Major Depression Inventory (MDI) and the Beck Depression Inventory (BDI) in severely depressed patients. Int. J. Psychiatry Clin. Pract. 2011, 15, 56–61. [Google Scholar] [CrossRef]
- Winkler, L.A.-D.; Gudex, C.; Lichtenstein, M.B.; Røder, M.E.; Adair, C.E.; Sjögren, J.M.; Støving, R.K. Explanatory Factors for Disease-Specific Health-Related Quality of Life in Women with Anorexia Nervosa. J. Clin. Med. 2021, 10, 1592. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | Mean | SD |
|---|---|---|
| Age (years) | 24.3 | 7.5 |
| Duration of illness (years) | 6.5 | 7.1 |
| BMI week 1 | 14.8 | 1.7 |
| BMI week 2 | 15.1 | 1.7 |
| BMI week 3 | 15.6 | 1.6 |
| BMI week 4 | 16.1 | 1.7 |
| BMI week 5 | 16.4 | 1.8 |
| BMI week 6 | 16.7 | 1.7 |
| BMI week 7 | 16.9 | 1.8 |
| BMI week 8 | 17.2 | 1.8 |
| EDEQ-Restraint | 3.4 | 1.6 |
| EDEQ-Eating concern | 3.4 | 1.5 |
| EDEQ-Shape concern | 4.8 | 1.3 |
| EDEQ-Weight concern | 4.3 | 1.5 |
| EDEQ-Global score | 4 | 1.3 |
| EDI | 174.2 | 57.6 |
| Characteristics | Mean | SD |
|---|---|---|
| MDI week 1 | 34 | 1.3 |
| MDI week 2 | 31.8 | 1.4 |
| MDI week 3 | 30.8 | 1.5 |
| MDI week 4 | 28.7 | 1.5 |
| MDI week 5 | 28.6 | 1.6 |
| MDI week 6 | 28.6 | 1.7 |
| MDI week 7 | 27.9 | 1.7 |
| MDI week 8 | 27.6 | 1.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sjögren, M.; Støving, R.K. Anorexia Nervosa: Reduction in Depression during Inpatient Treatment Is Closely Related to Reduction in Eating Disorder Psychopathology. J. Pers. Med. 2022, 12, 682. https://doi.org/10.3390/jpm12050682
Sjögren M, Støving RK. Anorexia Nervosa: Reduction in Depression during Inpatient Treatment Is Closely Related to Reduction in Eating Disorder Psychopathology. Journal of Personalized Medicine. 2022; 12(5):682. https://doi.org/10.3390/jpm12050682
Chicago/Turabian StyleSjögren, Magnus, and Rene Klinkby Støving. 2022. "Anorexia Nervosa: Reduction in Depression during Inpatient Treatment Is Closely Related to Reduction in Eating Disorder Psychopathology" Journal of Personalized Medicine 12, no. 5: 682. https://doi.org/10.3390/jpm12050682
APA StyleSjögren, M., & Støving, R. K. (2022). Anorexia Nervosa: Reduction in Depression during Inpatient Treatment Is Closely Related to Reduction in Eating Disorder Psychopathology. Journal of Personalized Medicine, 12(5), 682. https://doi.org/10.3390/jpm12050682