
MicroRNAs—A Promising Tool for Asthma Diagnosis and Severity Assessment: A Systematic Review

 ,
,  ,
, 

Abstract
:1. Introduction
2. Objectives
3. Methods
3.1. Search Strategy
3.2. Eligibility
3.2.1. Inclusion Criteria
3.2.2. Studies Were Excluded If
3.3. Study Selection
3.4. Data Extraction
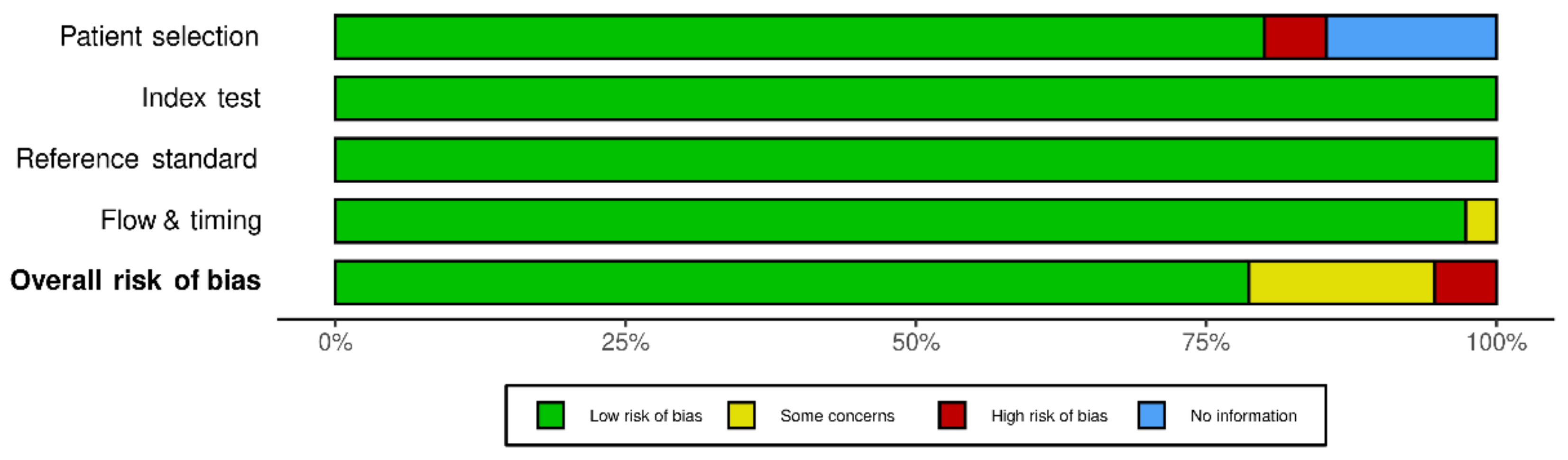
3.5. Quality Assessment and Risk of Bias for Publications
4. Results
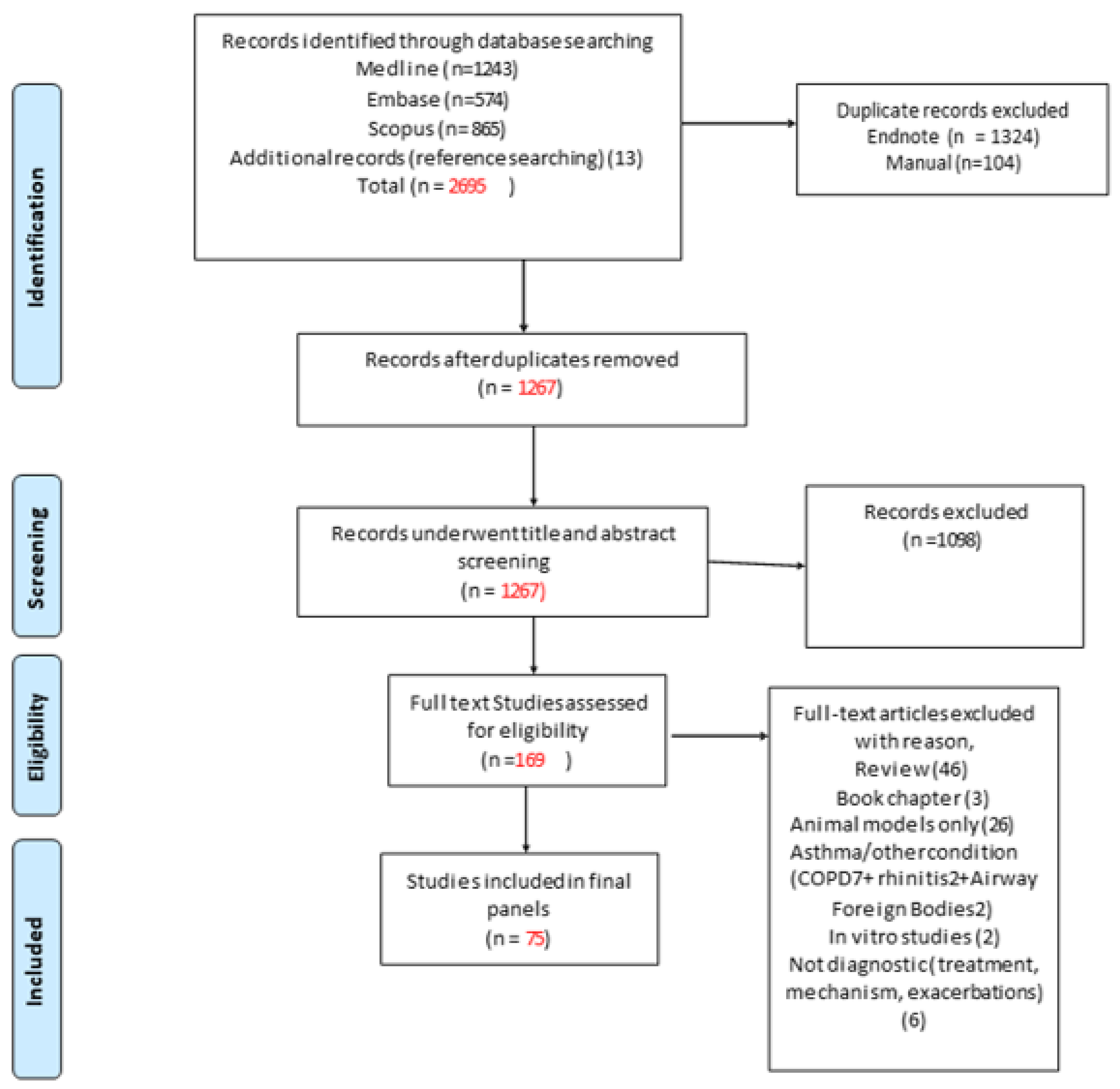
4.1. Publication Selection
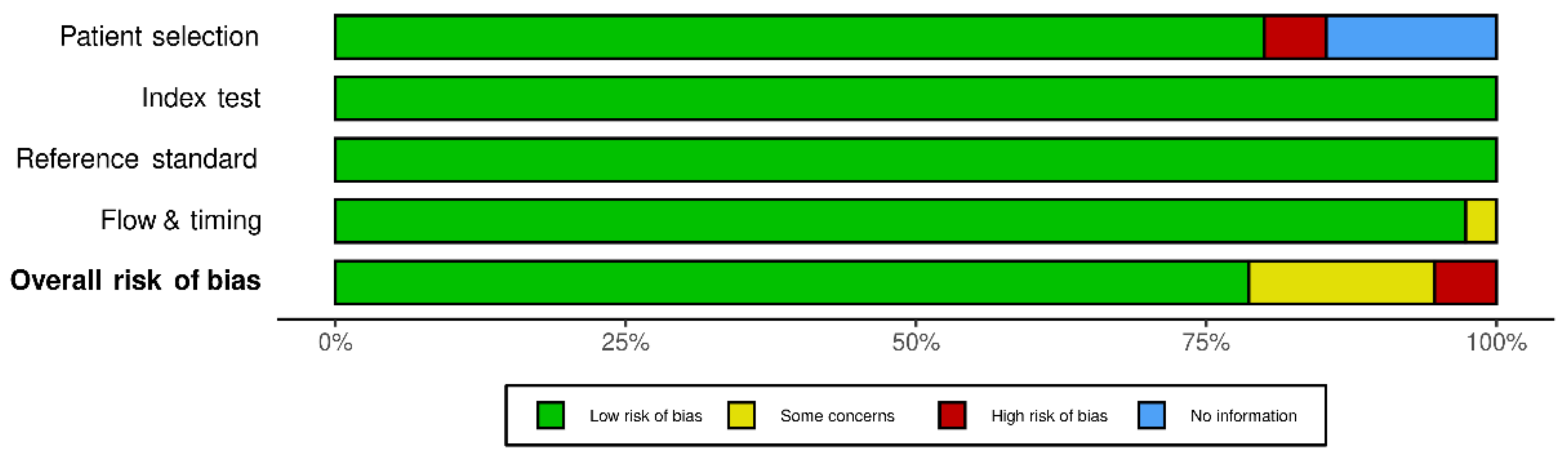
4.2. Quality Assessment (Risk of Bias)
- miRNAs for asthma diagnosis.
- miRNAs for severity-risk assessment.
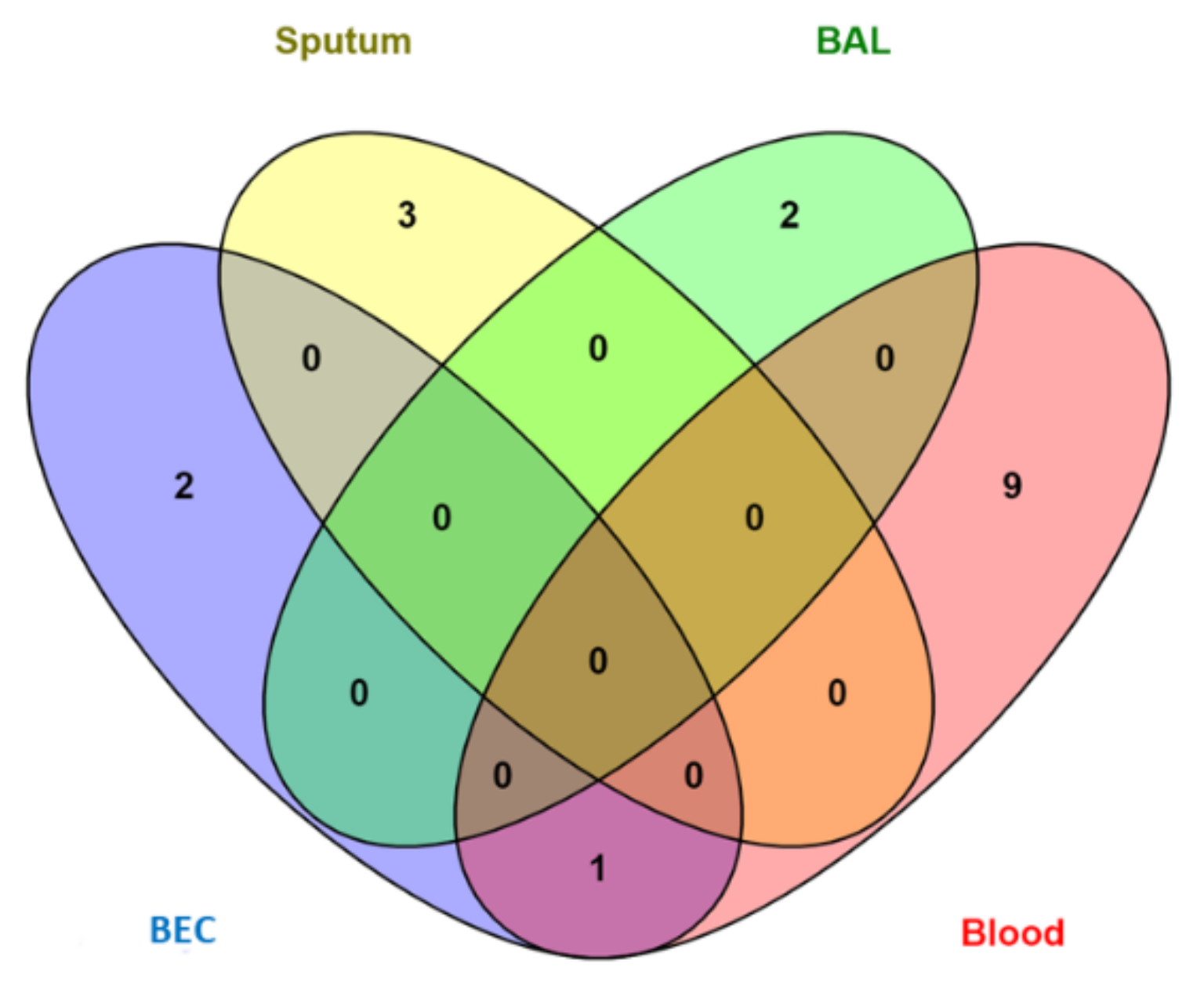
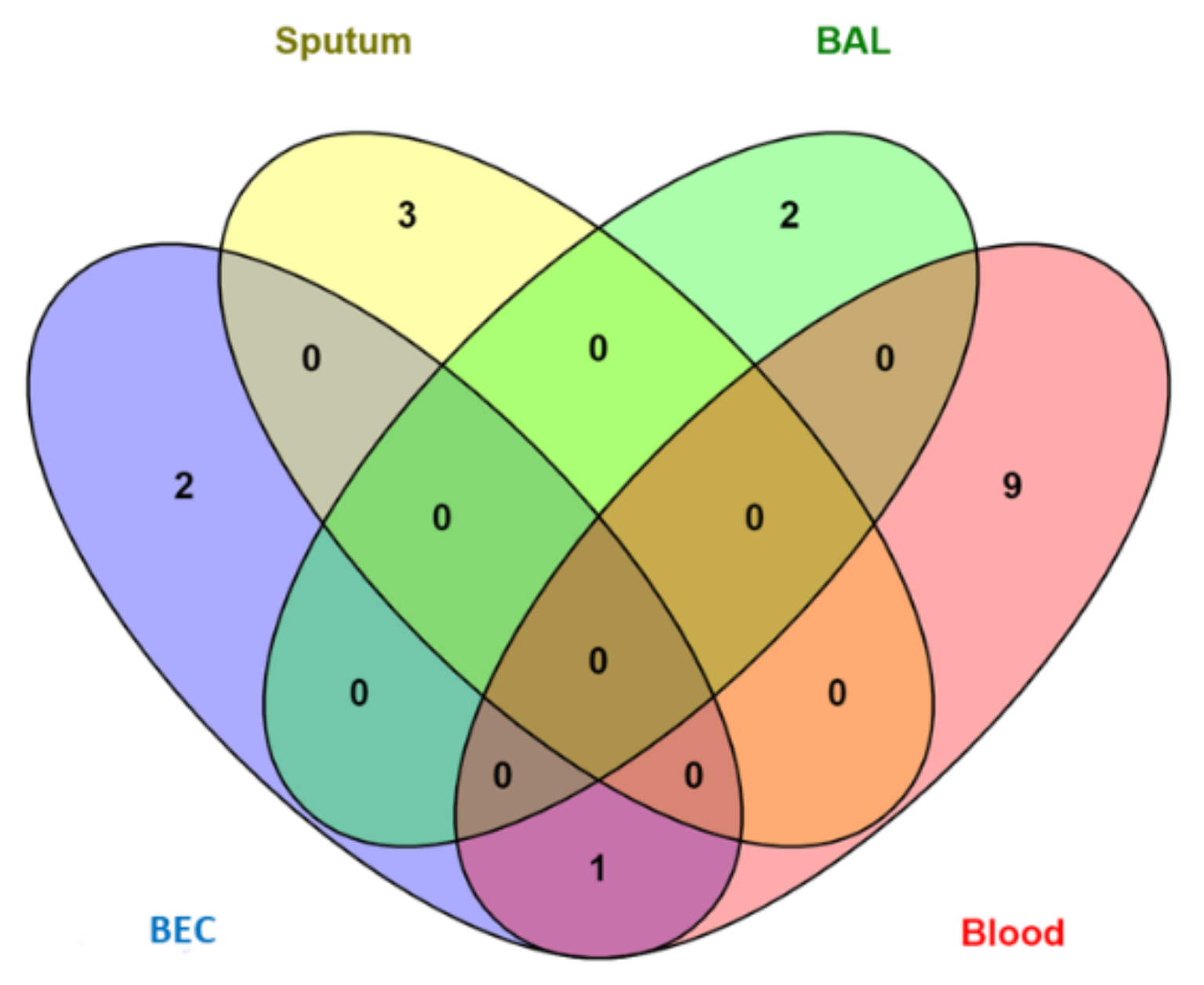
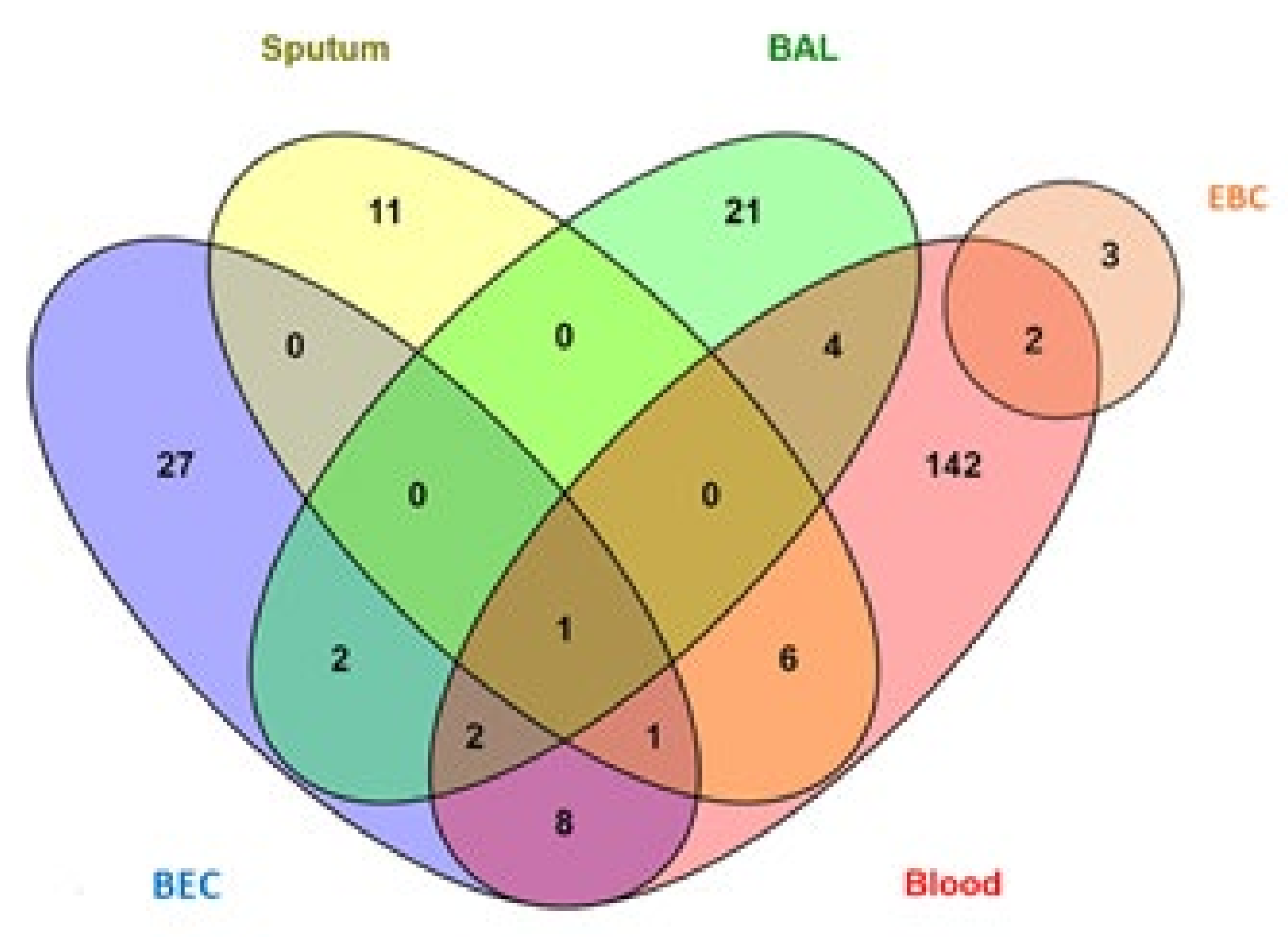
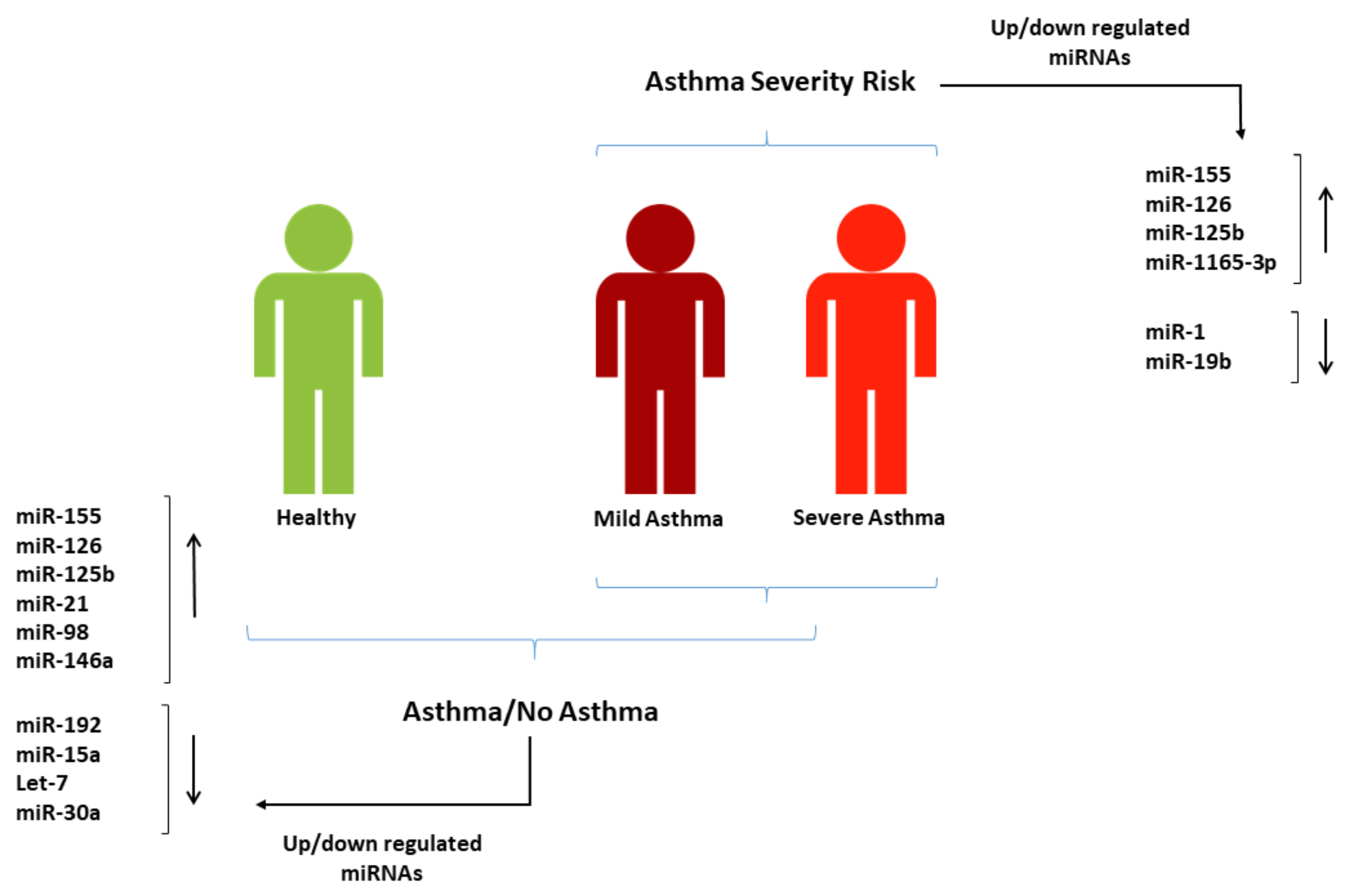
4.3. miRNAs for Asthma Diagnosis
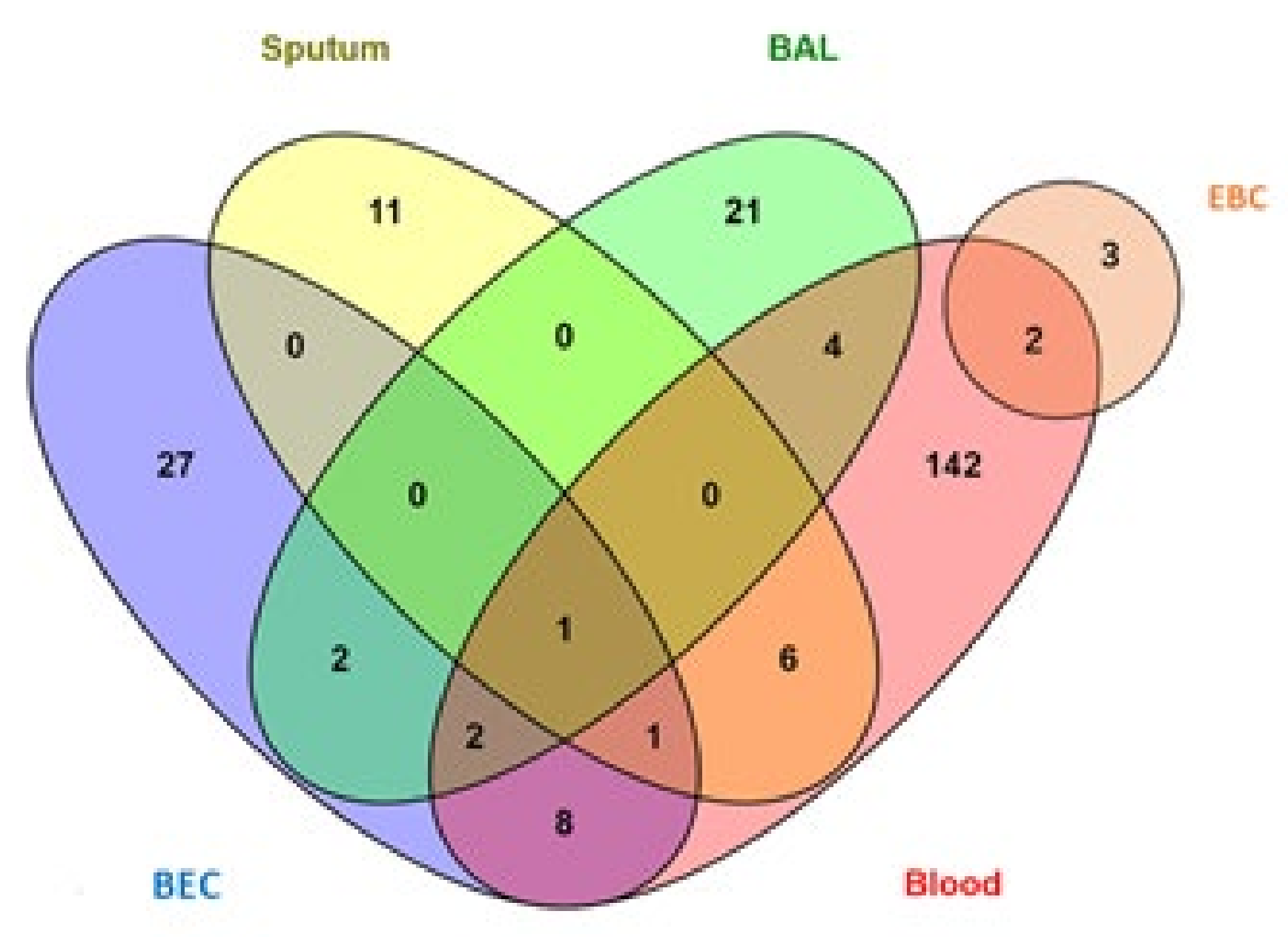
4.4. miRNAs for Asthma Severity-Risk Assessment
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Global Asthma Network. The Global Asthma Report 2018; Global Asthma Network: Auckland, New Zealand, 2018. [Google Scholar]
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Chung, K.F.; Wenzel, S.E.; Brozek, J.L.; Bush, A.; Castro, M.; Sterk, P.J.; Adcock, I.M.; Bateman, E.D.; Bel, E.H.; Bleecker, E.R.; et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur. Respir. J. 2013, 43, 343–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asthma UK. Living in Limbo: The Scale of Unmet Need in Difficult and Severe Asthma; Asthma UK: London, UK, 2019; pp. 1–20. [Google Scholar]
- Asthma UK. Severe Asthma: The Unmet Need and the Global Challenge; Asthma UK: London, UK, 2017. [Google Scholar]
- Cortez, M.A.; Bueso-Ramos, C.; Ferdin, J.; Lopez-Berestein, G.; Sood, A.K.; Calin, G.A. MicroRNAs in body fluids—the mix of hormones and biomarkers. Nat. Rev. Clin. Oncol. 2011, 8, 467–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, M.; Schaefer, A.; Steiner, I.; Kempkensteffen, C.; Stephan, C.; Erbersdobler, A.; Jung, K. Robust MicroRNA Stability in Degraded RNA Preparations from Human Tissue and Cell Samples. Clin. Chem. 2010, 56, 998–1006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witwer, K.W. Circulating MicroRNA Biomarker Studies: Pitfalls and Potential Solutions. Clin. Chem. 2015, 61, 56–63. [Google Scholar] [CrossRef]
- Panganiban, R.P.L.; Pinkerton, M.H.; Maru, S.Y.; Jefferson, S.J.; Roff, A.N.; Ishmael, F.T. Differential microRNA epression in asthma and the role of miR-1248 in regulation of IL-5. Am. J. Clin. Exp. Immunol. 2012, 1, 154–165. [Google Scholar]
- Pinkerton, M.; Chinchilli, V.; Banta, E.; Craig, T.; August, A.; Bascom, R.; Cantorna, M.; Harvill, E.; Ishmael, F.T. Differential expression of microRNAs in exhaled breath condensates of patients with asthma, patients with chronic obstructive pulmonary disease, and healthy adults. J. Allergy Clin. Immunol. 2013, 132, 217–219.e2. [Google Scholar] [CrossRef]
- Plank, M.; Maltby, S.; Mattes, J.; Foster, P.S. Targeting translational control as a novel way to treat inflammatory disease: The emerging role of MicroRNAs. Clin. Exp. Allergy 2013, 43, 981–999. [Google Scholar] [CrossRef]
- Rebane, A.; Akdis, C.A. MicroRNAs in allergy and asthma. Curr. Allergy Asthma Rep. 2014, 14, 424. [Google Scholar] [CrossRef]
- Solberg, O.D.; Ostrin, E.J.; Love, M.; Peng, J.C.; Bhakta, N.R.; Hou, L.; Nguyen, C.; Solon, M.; Nguyen, C.; Barczak, A.J.; et al. Airway Epithelial miRNA Expression Is Altered in Asthma. Am. J. Respir. Crit. Care Med. 2012, 186, 965–974. [Google Scholar] [CrossRef]
- Woodruff, P.G. Subtypes of Asthma Defined by Epithelial Cell Expression of Messenger RNA and MicroRNA. Ann. Am. Thorac. Soc. 2013, 10, S186–S189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roff, A.N.; Craig, T.J.; August, A.; Stellato, C.; Ishmael, F.T. MicroRNA-570-3p regulates HuR and cytokine expression in airway epithelial cells. Am. J. Clin. Exp. Immunol. 2014, 3, 68–83. [Google Scholar] [PubMed]
- Rodrigo-Muñoz, J.M.; Cañas, J.A.; Sastre, B.; Rego, N.; Greif, G.; Rial, M.; Mínguez, P.; Mahíllo-Fernández, I.; Fernández-Nieto, M.; Mora, I.; et al. Asthma diagnosis using integrated analysis of eosinophil microRNAs. Allergy 2018, 74, 507–517. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Huang, Y.; Liang, Z.; Liu, D.; Lu, Y.; Dai, Y.; Feng, G.; Wang, C. Plasma miRNAs might be promising biomarkers of chronic obstructive pulmonary disease. Clin. Respir. J. 2016, 10, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRIS-MA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Tian, M.; Ji, Y.; Wang, T.; Zhang, W.; Zhou, Y.; Cui, Y. Changes in circulating microRNA-126 levels are associated with immune imbalance in children with acute asthma. Int. J. Immunopathol. Pharmacol. 2018, 32, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Panganiban, R.P.; Wang, Y.; Howrylak, J.; Chinchilli, V.M.; Craig, T.J.; August, A.; Ishmael, F.T. Circulating microRNAs as biomarkers in patients with allergic rhinitis and asthma. J. Allergy Clin. Immunol. 2016, 137, 1423–1432. [Google Scholar] [CrossRef] [Green Version]
- Liu, F.; Qin, H.B.; Xu, B.; Zhou, H.; Zhao, D.Y. Profiling of miRNAs in pediatric asthma: Upregulation of miRNA-221 and miR-NA-485-3p. Mol. Med. Rep. 2012, 6, 1178–1182. [Google Scholar] [CrossRef] [Green Version]
- Suojalehto, H.; Lindström, I.; Majuri, M.-L.; Mitts, C.; Karjalainen, J.; Wolff, H.; Alenius, H. Altered MicroRNA Expression of Nasal Mucosa in Long-Term Asthma and Allergic Rhinitis. Int. Arch. Allergy Immunol. 2014, 163, 168–178. [Google Scholar] [CrossRef]
- Wu, X.-B.; Wang, M.-Y.; Zhu, H.-Y.; Tang, S.-Q.; You, Y.-D.; Xie, Y.-Q. Overexpression of microRNA-21 and microRNA-126 in the patients of bronchial asthma. Int. J. Clin. Exp. Med. 2014, 7, 1307–1312. [Google Scholar]
- ElKashef, S.M.M.A.; Ahmad, S.E.; Soliman, Y.M.A.; Mostafa, M.S. Role of microRNA-21 and microRNA-155 as biomarkers for bron-chial asthma. Innate Immun.-Lond. 2021, 27, 61–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weidner, J.; Ekerljung, L.; Malmhall, C.; Miron, N.; Radinger, M. Circulating microRNAs correlate to clinical parameters in indi-viduals with allergic and non-allergic asthma. Respir. Res. 2020, 21, 107. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Wang, W.; Jing, W. Indoor air pollution aggravates asthma in Chinese children and induces the changes in serum level of miR-155. Int. J. Environ. Health Res. 2019, 29, 22–30. [Google Scholar] [CrossRef]
- Malmhäll, C.; Johansson, K.; Winkler, C.; Alawieh, S.; Ekerljung, L.; Rådinger, M. Altered miR-155 Expression in Allergic Asthmatic Airways. Scand. J. Immunol. 2017, 85, 300–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, X.; Wu, F.; Fan, J.; Jin, Y.; Wang, J.; Yang, G. Posttranscriptional Regulation of Interleukin-33 Expression by MicroRNA-200 in Bronchial Asthma. Mol. Ther. 2018, 26, 1808–1817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levänen, B.; Bhakta, N.R.; Paredes, P.T.; Barbeau, R.; Hiltbrunner, S.; Pollack, J.L.; Sköld, C.M.; Svartengren, M.; Grunewald, J.; Gabrielsson, S.; et al. Altered microRNA profiles in bronchoalveolar lavage fluid exosomes in asthmatic patients. J. Allergy Clin. Immunol. 2013, 131, 894–903.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, C.; Yu, H.; Sun, Q.; Zhu, W.; Xu, J.; Gao, N.; Zhang, R.; Liu, L.; Wu, X.; Yang, X.; et al. Extracellular microRNA-21 and microRNA-26a increase in body fluids from rats with antigen induced pulmonary inflammation and children with recurrent wheezing. BMC Pulm. Med. 2016, 16, 50. [Google Scholar] [CrossRef] [Green Version]
- Cai, K.J.; Ke, J.Y.; Wang, Y.G.; Chen, L.S.; Shi, L.Y.; Zeng, Y.M. MIR-194 is related to the pathogenesis of asthma by regulating TLR4 expression. Int. J. Clin. Exp. Pathol. 2016, 9, 1327–1334. [Google Scholar]
- Hammad, R.H.M.; Hamed, D.H.E.D.; Eldosoky, M.A.E.R.; Ahmad, A.A.E.S.; Osman, H.M.; Elgalil, H.M.A.; Hassan, M.M.M. Plasma microRNA-21, microRNA-146a and IL-13 expression in asthmatic children. Innate Immun. 2018, 24, 171–179. [Google Scholar] [CrossRef] [Green Version]
- Elbehidy, R.M.; Youssef, D.; El-Shal, A.S.; Shalaby, S.M.; Sherbiny, H.S.; Sherief, L.M.; Akeel, N.E. MicroRNA–21 as a novel biomarker in diagnosis and response to therapy in asthmatic children. Mol. Immunol. 2016, 71, 107–114. [Google Scholar] [CrossRef]
- Zhao, M.; Juanjuan, L.; Weijia, F.; Jing, X.; Qiuhua, H.; Hua, Z.; Fuhe, L.; Hao, P. Expression Levels of MicroRNA-125b in Serum Exosomes of Patients with Asthma of Different Severity and its Diagnostic Significance. Curr. Drug Metab. 2019, 20, 781–784. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Chen, X.; Wu, Q.; Song, J.; Wang, L.; Li, G. miR-125b inhibits goblet cell differentiation in allergic airway inflammation by targeting SPDEF. Eur. J. Pharmacol. 2016, 782, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Lambert, K.A.; Roff, A.N.; Panganiban, R.P.; Douglas, S.; Ishmael, F.T. MicroRNA-146a is induced by inflammatory stimuli in airway epithelial cells and augments the anti-inflammatory effects of glucocorticoids. PLoS ONE 2018, 13, e0205434. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xue, Y.; Liu, Y.; Song, G.; Lv, G.; Wang, Y.; Wang, Y.; Li, X.; Yang, L. MicroRNA-146a expression inhibits the proliferation and promotes the apoptosis of bronchial smooth muscle cells in asthma by directly targeting the epidermal growth factor receptor. Exp. Ther. Med. 2016, 12, 854–858. [Google Scholar] [CrossRef] [Green Version]
- Kivihall, A.; Aab, A.; Soja, J.; Sładek, K.; Sanak, M.; Altraja, A.; Jakiela, B.; Bochenek, G.; Rebane, A. Reduced expression of miR-146a in human bronchial epithelial cells alters neutrophil migration. Clin. Transl. Allergy 2019, 9, 1–13. [Google Scholar] [CrossRef]
- Tsitsiou, E.; Williams, A.E.; Moschos, S.; Patel, K.; Rossios, C.; Jiang, X.; Adams, O.-D.; Macedo, P.; Booton, R.; Gibeon, D.; et al. Transcriptome analysis shows activation of circulating CD8+ T cells in patients with severe asthma. J. Allergy Clin. Immunol. 2012, 129, 95–103. [Google Scholar] [CrossRef]
- Yamamoto, M.; Singh, A.; Ruan, J.; Gauvreau, G.M.; O’Byrne, P.M.; Carlsten, C.R.; FitzGerald, J.M.; Boulet, L.-P.; Tebbutt, S.J. Decreased miR-192 expression in peripheral blood of asthmatic individuals undergoing an allergen inhalation challenge. BMC Genom. 2012, 13, 655. [Google Scholar] [CrossRef] [Green Version]
- Zhang, D.; Wu, Y.; Sun, G. miR-192 suppresses T follicular helper cell differentiation by targeting CXCR5 in childhood asthma. Scand. J. Clin. Lab. Investig. 2018, 78, 236–242. [Google Scholar] [CrossRef]
- Nasser, M.; Fahmey, S.; Geogry, D.; Taha, G.E. Expression of Serum MicroRNAs 221, 222, 15a and Level of VEGF-A in Children with Bronchial Asthma. Egypt. J. Immunol. 2019, 26, 133–144. [Google Scholar]
- Nakano, T.; Inoue, Y.; Shimojo, N.; Yamaide, F.; Morita, Y.; Arima, T.; Tomiita, M.; Kohno, Y. Lower levels of hsa-mir-15a, which decreases VEGFA, in the CD4+ T cells of pediatric patients with asthma. J. Allergy Clin. Immunol. 2013, 132, 1224–1227.e12. [Google Scholar] [CrossRef]
- Bin Li, B.; Chen, Y.L.; Pang, F. MicroRNA-30a Targets ATG5 and Attenuates Airway Fibrosis in Asthma by Suppressing Autophagy. Inflammation 2019, 43, 44–53. [Google Scholar] [CrossRef]
- Chen, L.; Xu, J.; Chu, X.; Ju, C. MicroRNA-98 interferes with thrombospondin 1 expression in peripheral B cells of patients with asthma. Biosci. Rep. 2017, 37, BSR20170149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Midyat, L.; Gulen, F.; Karaca, E.; Ozkinay, F.; Tanac, R.; Demir, E.; Cogulu, O.; Aslan, A.; Ozkinay, C.; Onay, H.; et al. MicroRNA expression profiling in children with different asthma phenotypes. Pediatr. Pulmonol. 2015, 51, 582–587. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Nunez, R.T.; Bondanese, V.P.; Louafi, F.; Francisco-Garcia, A.S.; Rupani, H.; Bedke, N.; Holgate, S.; Howarth, P.H.; Davies, D.E.; Sanchez-Elsner, T. A MicroRNA Network Dysregulated in Asthma Controls IL-6 Production in Bronchial Epithelial Cells. PLoS ONE 2014, 9, e111659. [Google Scholar] [CrossRef] [Green Version]
- Rijavec, M.; Korošec, P.; Žavbi, M.; Kern, I.; Malovrh, M.M. Let-7a is differentially expressed in bronchial biopsies of patients with severe asthma. Sci. Rep. 2014, 4, srep06103. [Google Scholar] [CrossRef] [Green Version]
- Zhao, M.; Li, Y.-P.; Geng, X.-R.; Zhao, M.; Ma, S.-B.; Yang, Y.-H.; Deng, Z.-H.; Luo, L.-M.; Pan, X.-Q. Expression Level of MiRNA-126 in Serum Exosomes of Allergic Asthma Patients and Lung Tissues of Asthmatic Mice. Curr. Drug Metab. 2019, 20, 799–803. [Google Scholar] [CrossRef]
- Zhang, X.X.; Zhao, X.; Sun, H.M.; Yan, Y.; Huang, L.; Gu, W.; Jiang, W.; Wang, Y.; Zhu, C.; Ji, W.; et al. The role of miR-29c/B7-H3 axis in children with allergic asthma. J. Transl. Med. 2018, 16, 218. [Google Scholar] [CrossRef]
- Maes, T.; Cobos, F.A.; Schleich, F.; Sorbello, V.; Henket, M.; De Preter, K.; Bracke, K.; Conickx, G.; Mesnil, C.; Vandesompele, J.; et al. Asthma inflammatory phenotypes show differential microRNA expression in sputum. J. Allergy Clin. Immunol. 2016, 137, 1433–1446. [Google Scholar] [CrossRef] [Green Version]
- Karam, R.A.; Elrahman, D.M.A. Differential expression of miR-155 and Let-7a in the plasma of childhood asthma: Potential biomarkers for diagnosis and severity. Clin. Biochem. 2019, 68, 30–36. [Google Scholar] [CrossRef]
- Haj-Salem, I.; Fakhfakh, R.; Berube, J.C.; Jacques, E.; Plante, S.; Simard, M.J.; Bossé, Y.; Chakir, J. MicroRNA-19a enhances proliferation of bronchial epithelial cells by targeting TGF beta R2 gene in severe asthma. Allergy 2015, 70, 212–219. [Google Scholar] [CrossRef]
- Wu, C.; Xu, K.; Wang, Z.; Chen, Z.; Sun, Z.; Yu, W.; Ji, N.; Huang, M.; Zhang, M. A novel microRNA miR-1165-3p as a potential diagnostic biomarker for allergic asthma. Biomarkers 2018, 24, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Tian, M.; Zhou, Y.; Jia, H.; Zhu, X.; Cui, Y. The Clinical Significance of Changes in the Expression Levels of MicroRNA-1 and Inflammatory Factors in the Peripheral Blood of Children with Acute-Stage Asthma. BioMed Res. Int. 2018, 2018, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ding, L.Z.; Li, C.J. Downregulation of miR-19b in pediatric asthma is associated with the activation of nuclear factor-kappa B signaling pathway. Int. J. Clin. Exp. Med. 2019, 12, 10101–10108. [Google Scholar]
- Huang, H.; Lu, H.; Liang, L.; Zhi, Y.; Huo, B.; Wu, L.; Xu, L.; Shen, Z. MicroRNA-744 Inhibits Proliferation of Bronchial Epithelial Cells by Regulating Smad3 Pathway via Targeting Transforming Growth Factor-beta1 (TGF-beta1) in Severe Asthma. Med. Sci. Monit. 2019, 25, 2159–2168. [Google Scholar] [CrossRef]
- Weidner, J.; Bartel, S.; Kılıç, A.; Zissler, U.M.; Renz, H.; Schwarze, J.; Schmidt-Weber, C.B.; Maes, T.; Rebane, A.; Krauss-Etschmann, S.; et al. Spotlight on microRNAs in allergy and asthma. Allergy 2020, 76, 1661–1678. [Google Scholar] [CrossRef]
- Lu, T.X.; Hartner, J.; Lim, E.J.; Fabry, V.; Mingler, M.K.; Cole, E.T.; Orkin, S.H.; Aronow, B.J.; Rothenberg, M.E. MicroRNA-21 limits in vivo immune response-mediated activation of the IL-12/IFN-gamma pathway, Th1 polarization, and the severity of delayed-type hypersensitivity. J. Immunol. 2011, 187, 3362–3373. [Google Scholar] [CrossRef]
- Sawant, D.V.; Yao, W.; Wright, Z.; Sawyers, C.; Tepper, R.S.; Gupta, S.K.; Kaplan, M.H.; Dent, A.L. Serum MicroRNA-21 as a Biomarker for Allergic Inflammatory Disease in Children. MicroRNA 2015, 4, 36–40. [Google Scholar] [CrossRef] [Green Version]
- Lu, T.X.; Munitz, A.; Rothenberg, M.E. MicroRNA-21 Is Up-Regulated in Allergic Airway Inflammation and Regulates IL-12p35 Expression. J. Immunol. 2009, 182, 4994–5002. [Google Scholar] [CrossRef] [Green Version]
- Ariel, D.; Upadhyay, D. The role and regulation of microRNAs in asthma. Curr. Opin. Allergy Clin. Immunol. 2012, 12, 49–52. [Google Scholar] [CrossRef]
- Johansson, K.; Malmhäll, C.; Ramos-Ramírez, P.; Rådinger, M. MicroRNA-155 is a critical regulator of type 2 innate lymphoid cells and IL-33 signaling in experimental models of allergic airway inflammation. J. Allergy Clin. Immunol. 2017, 139, 1007–1016.e9. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Sun, E.; Li, X.; Zhang, M.; Tang, Z.; He, L.; Lv, K. miR-155 contributes to Df1-induced asthma by increasing the proliferative response of Th cells via CTLA-4 downregulation. Cell Immunol. 2017, 314, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Li, J.; Gao, P.; Wang, Q.; Zhang, J. miR-155: A Novel Target in Allergic Asthma. Int. J. Mol. Sci. 2016, 17, 1773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berge, M.V.D.; Tasena, H. Role of microRNAs and exosomes in asthma. Curr. Opin. Pulm. Med. 2019, 25, 87–93. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| miRNA | Tissue | Up-/DownRegulated | Ref |
|---|---|---|---|
| miR-126 | Plasma | + | [19,20] |
| Serum | + | [20] | |
| Lymphocytes | - | [21] | |
| Nasal biopsy | - | [22] | |
| EBC | + | [23] | |
| miR-155 | Serum | + | [24,25,26] |
| Sputum | - | [27] | |
| Nasal biopsy | - | [22] | |
| EBC | - | [27] | |
| BAL | - | [28] | |
| Let-7 family | BAL | - | [29,28] |
| Serum | - | [9] | |
| EBC | - | [27] | |
| Lymphocytes | - | [21] | |
| miR-21 | BAL | -/+ | exosomes [17]/total small RNA [18] |
| Plasma | + | [30,31,32] | |
| Serum | + | [33,24] | |
| EBC | + | [23] | |
| miR-125b | Plasma | + | [20] |
| Serum | + | [34] | |
| Sputum | - | [35] | |
| Lymphocytes | - | [21] | |
| miR-146a | Serum | + | [25,36] |
| Plasma | + | [32,37] | |
| PBMCs | - | [38] | |
| EBC | - | [39] | |
| miR-192 | Blood | - | [40] |
| Plasma | - | [41] | |
| Lymphocytes and CD4+ | - | [21,41] | |
| miR-15a | Serum | - | [42] |
| Lymphocytes and CD4+ | - | [21,43] | |
| miR-30a | Serum | - | [44] |
| BAL | - | [28] | |
| Lymphocytes | - | [21] | |
| miR-98 | B cells | + | [45] |
| Blood | + | [46] | |
| Lymphocytes | - | [21] |
| miRNA | +/- | Sample | Ref |
|---|---|---|---|
| miR-126 | + | Plasma and Serum | [19,20,49] |
| miR-155 | + | Serum | [24,25,26] |
| miR-21 | + | Plasma and Serum | [24,30,31,32,33] |
| miR-125b | + | Plasma and Serum | [20,34] |
| miR-98 | + | Blood | [46] |
| miR-146a | + | Plasma and Serum | [25,32,36,37] |
| miR-192 | - | Plasma | [41] |
| miR-15a | - | Serum | [42] |
| Let-7 | - | Serum | [9] |
| miR-30a | - | Serum | [44] |
| miRNA | +/- | Sample | Ref |
|---|---|---|---|
| miR-320a | + | Eosinophils | [16] |
| miR-185-5p | + | Eosinophils | [16] |
| miR-144-5p | + | Eosinophils | [16] |
| miR-629-3p | + | Sputum (Supernatant) | [51] |
| miR-223-3p | + | Sputum (Supernatant) | [51] |
| miR142-3p | + | Sputum (Supernatant) | [51] |
| miR-126 | + | Plasma | [19] |
| miR-155 | + | Plasma | [52] |
| miR-125b | + | Serum (exosomes) | [34] |
| miR-19a | + | BEC | [53] |
| miR-1165-3p | + | Serum | [54] |
| miR-200b | - | BAL | [28] |
| miR-1 | - | Plasma | [55] |
| miR-19b | - | Serum | [56] |
| Let-7a | - | BEC/plasma | [48,52] |
| miR-744 | - | BEC | [57] |
| miR-200c | - | BAL | [28] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kyyaly, M.A.; Vorobeva, E.V.; Kothalawala, D.M.; Fong, W.C.G.; He, P.; Sones, C.L.; Al-Zahrani, M.; Sanchez-Elsner, T.; Arshad, S.H.; Kurukulaaratchy, R.J. MicroRNAs—A Promising Tool for Asthma Diagnosis and Severity Assessment: A Systematic Review. J. Pers. Med. 2022, 12, 543. https://doi.org/10.3390/jpm12040543
Kyyaly MA, Vorobeva EV, Kothalawala DM, Fong WCG, He P, Sones CL, Al-Zahrani M, Sanchez-Elsner T, Arshad SH, Kurukulaaratchy RJ. MicroRNAs—A Promising Tool for Asthma Diagnosis and Severity Assessment: A Systematic Review. Journal of Personalized Medicine. 2022; 12(4):543. https://doi.org/10.3390/jpm12040543
Chicago/Turabian StyleKyyaly, Mohammed Aref, Elena Vladimirovna Vorobeva, Dilini M. Kothalawala, Wei Chern Gavin Fong, Peijun He, Collin L. Sones, Mohammad Al-Zahrani, Tilman Sanchez-Elsner, Syed Hasan Arshad, and Ramesh J. Kurukulaaratchy. 2022. "MicroRNAs—A Promising Tool for Asthma Diagnosis and Severity Assessment: A Systematic Review" Journal of Personalized Medicine 12, no. 4: 543. https://doi.org/10.3390/jpm12040543
APA StyleKyyaly, M. A., Vorobeva, E. V., Kothalawala, D. M., Fong, W. C. G., He, P., Sones, C. L., Al-Zahrani, M., Sanchez-Elsner, T., Arshad, S. H., & Kurukulaaratchy, R. J. (2022). MicroRNAs—A Promising Tool for Asthma Diagnosis and Severity Assessment: A Systematic Review. Journal of Personalized Medicine, 12(4), 543. https://doi.org/10.3390/jpm12040543