
A Simple Algorithm Using Ventilator Parameters to Predict Successfully Rapid Weaning Program in Cardiac Intensive Care Unit Patients

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Data Source
2.3. Algorithms
2.3.1. Logistic Regression (LR)
2.3.2. Decision Trees (DT)
2.3.3. Random Forest (RF)
2.3.4. eXtreme Gradient Boosting (XGBoost)
2.3.5. Support Vector Machine (SVM)
2.3.6. Artificial Neural Network (ANN)
2.4. Statistical Analyses
2.4.1. Features Extraction
2.4.2. Analysis Procedure
3. Results
3.1. Patient Characteristics
3.2. Results of the Machine Learning Models
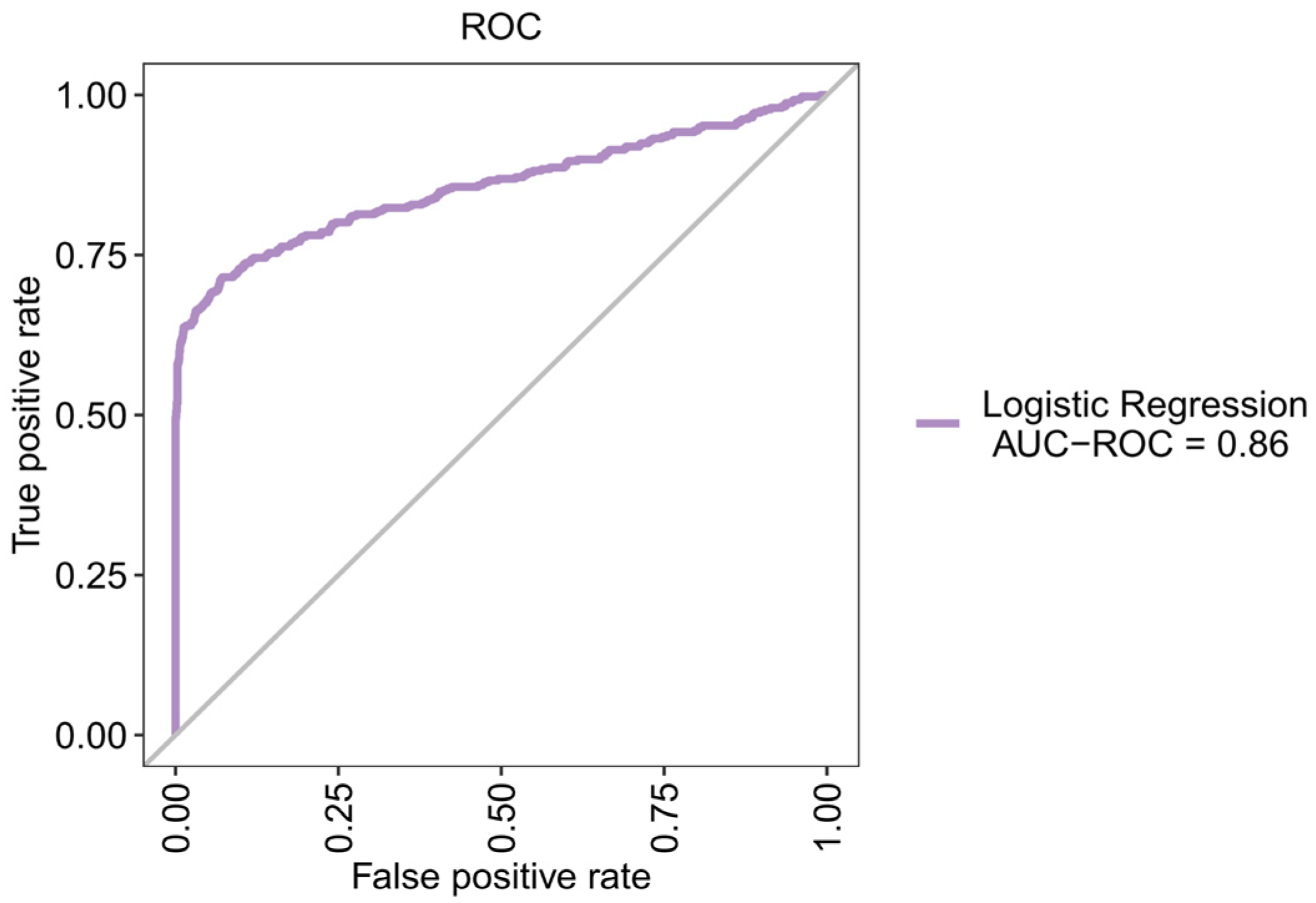
3.3. Using LR to Create a New Prediction Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boles, J.M.; Bion, J.; Connors, A.; Herridge, M.; Marsh, B.; Melot, C.; Pearl, R.; Silverman, H.; Stanchina, M.; Vieillard-Baron, A.; et al. Weaning from mechanical ventilation. Eur. Respir. J. 2007, 29, 1033–1056. [Google Scholar] [CrossRef] [PubMed]
- Wunsch, H.; Linde-Zwirble, W.T.; Angus, D.C.; Hartman, M.E.; Milbrandt, E.B.; Kahn, J.M. The epidemiology of mechanical ventilation use in the United States. Crit. Care Med. 2010, 38, 1947–1953. [Google Scholar] [CrossRef] [PubMed]
- Sidey-Gibbons, J.A.M.; Sidey-Gibbons, C.J. Machine learning in medicine: A practical introduction. BMC Med. Res. Methodol. 2019, 19, 64. [Google Scholar] [CrossRef]
- Kallet, R.H. Ventilator bundles in transition: From prevention of ventilator-associated pneumonia to prevention of ventilator-associated events. Respir. Care 2019, 64, 994–1006. [Google Scholar] [CrossRef] [PubMed]
- Kuo, H.J.; Chiu, H.W.; Lee, C.N.; Chen, T.T.; Chang, C.C.; Bien, M.Y. Improvement in the prediction of ventilator weaning outcomes by an artificial neural network in a medical ICU. Respir. Care 2015, 60, 1560–1569. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, M.H.; Hsieh, M.J.; Chen, C.M.; Hsieh, C.C.; Chao, C.M.; Lai, C.C. An artificial neural network model for predicting successful extubation in intensive care units. J. Clin. Med. 2018, 7, 240. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, M.H.; Hsieh, M.J.; Cheng, A.C.; Chen, C.M.; Hsieh, C.C.; Chao, C.M.; Lai, C.C.; Cheng, K.C.; Chou, W. Predicting weaning difficulty for planned extubation patients with an artificial neural network. Medicine 2019, 98, e17392. [Google Scholar] [CrossRef]
- Otaguro, T.; Tanaka, H.; Igarashi, Y.; Tagami, T.; Masuno, T.; Yokobori, S.; Matsumoto, H.; Ohwada, H.; Yokota, H. Machine learning for the prediction of successful extubation among patients with mechanical ventilation in the intensive care unit: A retrospective observational study. J. Nippon Med. Sch. 2021, 88, 408–417. [Google Scholar] [CrossRef]
- Hsu, C.J.; Brouhard, G.J.; François, P. Numerical parameter space compression and its application to biophysical models. Biophys. J. 2020, 118, 1455–1465. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Lemeshow, S. Applied Logistic Regression; John Wiley & Sons: New York, NY, USA, 2000. [Google Scholar]
- Friedman, J.H.; Meulman, J.J. Multiple additive regression trees with application in epidemiology. Stat. Med. 2003, 22, 1365–1381. [Google Scholar] [CrossRef]
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef]
- Zhang, Y.; Haghani, A. A gradient boosting method to improve travel time prediction. Transp. Res. Part C Emerg. Technol. 2015, 58, 308–324. [Google Scholar] [CrossRef]
- Schölkopf, B.; Smola, A.J.; Bach, F. Learning with Kernels: Support Vector Machines, Regularization, Optimization, and Beyond; MIT Press: Cambridge, MA, USA, 2002. [Google Scholar]
- Wang, S.C. Artificial Neural Network, in Interdisciplinary Computing in Java Programming; Springer: Berlin/Heidelberg, Germany, 2003; pp. 81–100. [Google Scholar]
- Derksen, S.; Keselman, H.J. Backward, forward and stepwise automated subset selection algorithms: Frequency of obtaining authentic and noise variables. Br. J. Math. Stat. Psychol. 1992, 45, 265–282. [Google Scholar] [CrossRef]
- Fabregat, A.; Magret, M.; Ferré, J.A.; Vernet, A.; Guasch, N.; Rodríguez, A.; Gómez, J.; Bodí, M. A Machine Learning decision-making tool for extubation in Intensive Care Unit patients. Comput. Methods Programs Biomed. 2021, 200, 105869. [Google Scholar] [CrossRef]
- Datta, D.; Foley, R.; Wu, R.; Grady, J.; Scalise, P. Can creatinine height index predict weaning and survival outcomes in patients on prolonged mechanical ventilation after critical illness? J. Intensive Care Med. 2018, 33, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.R.; Yen, S.Y.; Chien, J.Y.; Liu, H.C.; Wu, Y.L.; Chen, C.H. Predicting weaning and extubation outcomes in long-term mechanically ventilated patients using the modified Burns Wean Assessment Program scores. Respirology 2014, 19, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Miwa, K.; Mitsuoka, M.; Takamori, S.; Hayashi, A.; Shirouzu, K. Continuous monitoring of oxygen consumption in patients undergoing weaning from mechanical ventilation. Respiration 2003, 70, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Savi, A.; Teixeira, C.; Silva, J.M.; Borges, L.G.; Pereira, P.A.; Pinto, K.B.; Gehm, F.; Moreira, F.C.; Wickert, R.; Trevisan, C.B.E.; et al. Weaning predictors do not predict extubation failure in simple-to-wean patients. J. Crit. Care 2012, 27, 221.e1–221.e8. [Google Scholar] [CrossRef]
- Capdevïla, X.J.; Perrigault, P.F.; Perey, P.J.; d’Athis, F. Occlusion pressure and its ratio to maximum inspiratory pressure are useful predictors for successful extubation following T-piece weaning trial. Chest 1995, 108, 482–489. [Google Scholar] [CrossRef]
- Scheinhorn, D.J.; Hassenpflug, M.; Artinian, B.M.; LaBree, L.; Catlin, J.L. Predictors of weaning after 6 weeks of mechanical ventilation. Chest 1995, 107, 500–505. [Google Scholar] [CrossRef]
- Vassilakopoulos, T.; Zakynthinos, S.; Roussos, C. The tension-time index and the frequency/tidal volume ratio are the major pathophysiologic determinants of weaning failure and success. Am. J. Respir. Crit. Care Med. 1998, 158, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Chatila, W.; Jacob, B.; Guaglionone, D.; Manthous, C.A. The unassisted respiratory rate-tidal volume ratio accurately predicts weaning outcome. Am. J. Med. 1996, 101, 61–67. [Google Scholar] [CrossRef]
- Cohen, J.D.; Shapiro, M.; Grozovski, E.; Singer, P. Automatic tube compensation-assisted respiratory rate to tidal volume ratio improves the prediction of weaning outcome. Chest 2002, 122, 980–984. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Jiang, H.; Li, T. Inhibition of bleomycin-induced pulmonary fibrosis by Okam extract J201. Chest 2004, 126, 889S. [Google Scholar] [CrossRef] [PubMed]
- Kuo, P.H.; Kuo, S.H.; Yang, P.C.; Wu, H.D.; Lu, B.Y.; Chen, M.T. Predictive Value of Rapid Shallow Breathing Index Measured at Initiation and Termination of a 2-hour Spontaneous Breathing Trial for Weaning Outcome in ICU Patients. J. Formos. Med. Assoc. 2006, 105, 390–398. [Google Scholar] [CrossRef][Green Version]
- Mabrouk, A.A.; Mansour, O.F.; Abd El-Aziz, A.A.; Elhabashy, M.M.; Alasdoudy, A.A. Evaluation of some predictors for successful weaning from mechanical ventilation. Egypt. J. Chest Dis. Tuberc. 2015, 64, 703–707. [Google Scholar] [CrossRef]
- Papanikolaou, J.; Makris, D.; Saranteas, T.; Karakitsos, D.; Zintzaras, E.; Karabinis, A.; Kostopanagiotou, G.; Zakynthinos, E. New insights into weaning from mechanical ventilation: Left ventricular diastolic dysfunction is a key player. Intensive Care Med. 2011, 37, 1976–1985. [Google Scholar] [CrossRef]
- Segal, L.N.; Oei, E.; Oppenheimer, B.W.; Goldring, R.M.; Bustami, R.T.; Ruggiero, S.; Berger, K.I.; Fiel, S.B. Evolution of pattern of breathing during a spontaneous breathing trial predicts successful extubation. Intensive Care Med. 2010, 36, 487–495. [Google Scholar] [CrossRef]
- Smina, M.; Salam, A.; Khamiees, M.; Gada, P.; Amoateng-Adjepong, Y.; Manthous, C.A. Cough peak flows and extubation outcomes. Chest 2003, 124, 262–268. [Google Scholar] [CrossRef]
- Upadya, A.; Tilluckdharry, L.; Muralidharan, V.; Amoateng-Adjepong, Y.; Manthous, C.A. Fluid balance and weaning outcomes. Intensive Care Med. 2005, 31, 1643–1647. [Google Scholar] [CrossRef]
- Wysocki, M.; Cracco, C.; Teixeira, A.; Mercat, A.; Diehl, J.L.; Lefort, Y.; Derenne, J.P.; Similowski, T. Reduced breathing variability as a predictor of unsuccessful patient separation from mechanical ventilation. Crit. Care Med. 2006, 34, 2076–2083. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos Bien, U.; Souza, G.F.; Campos, E.S.; De Carvalho, E.F.; Fernandes, M.G.; Santoro, I.; Costa, D.; Arena, R.; Sampaio, L.M.M. Maximum inspiratory pressure and rapid shallow breathing index as predictors of successful ventilator weaning. J. Phys. Ther. Sci. 2015, 27, 3723–3727. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Weaned within 24 h (n = 1042) | Not Weaned within 24 h (n = 397) | p-Value | |
|---|---|---|---|---|
| Gender | 0.069 | |||
| Males | 714 (68.5%) | 252 (63.5%) | ||
| Females | 328 (31.5%) | 145 (36.5%) | ||
| age, mean ± SD | 65.05 ± 12.53 | 68.34 ± 15.18 | <0.001 | * |
| Smoking, n (%) | <0.001 | * | ||
| No | 805 (77.3%) | 250 (63.0%) | ||
| Yes | 198 (19.0%) | 113 (28.5%) | ||
| Yes, quit smoking | 39 (3.7%) | 34 (8.6%) | ||
| Ventilation set, mean ± SD | ||||
| Ventilation rate set, 30/min | 12.23 ± 1.08 | 14.77 ± 8.77 | <0.001 | * |
| Inspiration time, breath/min | 1.00 ± 0.00 | 4.08 ± 8.72 | <0.001 | * |
| Pressure limit high, cmH2O | 40.72 ± 1.89 | 37.00 ± 6.75 | <0.001 | * |
| Pressure limit low, cmH2O | 2.99 ± 0.40 | 3.91 ± 1.10 | <0.001 | * |
| Spontaneous respiratory rate, % | 13.38 ± 2.92 | 20.22 ± 6.45 | <0.001 | * |
| Inspiratory pressure, cmH2O | 20.74 ± 2.52 | 19.69 ± 5.84 | <0.001 | * |
| PEEP, cmH2O | 5.47 ± 0.92 | 4.37 ± 2.69 | <0.001 | * |
| Ramp, mS | 0.01 ± 0.13 | 0.24 ± 0.73 | <0.001 | * |
| Ventilation monitoring, mean ± SD | ||||
| Inspiratory tidal volume, mL/kg | 554.92 ± 84.93 | 422.41 ± 336.91 | <0.001 | * |
| Expiratory tidal volume, mL/kg | 555.55 ± 80.85 | 507.98 ± 156.23 | <0.001 | * |
| Peak pressure, cmH2O | 21.05 ± 2.85 | 211.52 ± 273.68 | <0.001 | * |
| Mean pressure, cmH2O | 8.75 ± 1.33 | 13.37 ± 7.38 | <0.001 | * |
| Expiratory minute ventilation, L/min | 7.26 ± 1.72 | 10.49 ± 4.13 | <0.001 | * |
| Compliance, mL/cmH2O | 60.04 ± 29.42 | 28.78 ± 35.06 | <0.001 | * |
| Resistance, mL/cmH2O | 13.68 ± 5.43 | 28.95 ± 33.67 | <0.001 | * |
| Arterial blood gas test, ABG, mean ± SD | ||||
| SpO2, % | 99.36 ± 31.84 | 63.59 ± 36.53 | <0.001 | * |
| pH | 7.03 ± 0.18 | 7.04 ± 0.18 | 0.947 | |
| PCO2, mmHg | 37.33 ± 8.15 | 32.03 ± 11.89 | <0.001 | * |
| HCO3, mmol/L | 23.57 ± 4.06 | 29.36 ± 11.29 | <0.001 | * |
| PO2, mmHg | 162.86 ± 96.22 | 72.75 ± 102.14 | <0.001 | * |
| SAO2, % | 154.74 ± 140.22 | 230.17 ± 172.74 | <0.001 | * |
| Base Excess, mmol/L | 2.99 ± 21.32 | 36.83 ± 49.32 | <0.001 | * |
| Others, mean ± SD | ||||
| Systolic blood pressure, mmHg | 124.55 ± 24.57 | 97.67 ± 33.42 | <0.001 | * |
| Diastolic blood pressure, mmHg | 66.50 ± 26.76 | 93.78 ± 41.28 | <0.001 | * |
| Heart rate, bpm | 82.42 ± 14.98 | 106.87 ± 28.78 | <0.001 | * |
| Model | Accuracy | Sensitivity | Specificity | Precision | F1 Score | ROC-AUC | PR-AUC |
|---|---|---|---|---|---|---|---|
| Artificial neural network | 85.2% | 67.5% | 91.7% | 75.7% | 71.4% | 84.0% | 76.0% |
| Decision tree | 87.7% | 66.2% | 93.6% | 79.7% | 72.4% | 84.0% | 79.0% |
| Logistic regression | 83.1% | 64.5% | 98.3% | 93.4% | 76.3% | 86.0% | 84.0% |
| Random forest | 86.8% | 67.5% | 91.7% | 75.7% | 71.4% | 84.0% | 76.0% |
| Support vector machine | 86.8% | 64.2% | 98.8% | 95.5% | 76.8% | 88.0% | 70.0% |
| XGBoost | 85.8% | 62.7% | 98.6% | 94.3% | 75.3% | 85.0% | 82.0% |
| Variable | Coefficient |
|---|---|
| Expiratory minute ventilation (L/min) | 0.397 |
| Expiratory tidal volume (mL/kg) | −0.010 |
| Ventilation rate set (30/min) | 0.094 |
| Heart rate (bpm) | 0.017 |
| Peak pressure (cmH2O) | 0.069 |
| pH | 0.667 |
| Age | 0.015 |
| Intercept | −11.430 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, W.-T.; Huang, H.-L.; Ko, P.-S.; Su, W.; Kao, C.-C.; Su, S.-L. A Simple Algorithm Using Ventilator Parameters to Predict Successfully Rapid Weaning Program in Cardiac Intensive Care Unit Patients. J. Pers. Med. 2022, 12, 501. https://doi.org/10.3390/jpm12030501
Chen W-T, Huang H-L, Ko P-S, Su W, Kao C-C, Su S-L. A Simple Algorithm Using Ventilator Parameters to Predict Successfully Rapid Weaning Program in Cardiac Intensive Care Unit Patients. Journal of Personalized Medicine. 2022; 12(3):501. https://doi.org/10.3390/jpm12030501
Chicago/Turabian StyleChen, Wei-Teing, Hai-Lun Huang, Pi-Shao Ko, Wen Su, Chung-Cheng Kao, and Sui-Lung Su. 2022. "A Simple Algorithm Using Ventilator Parameters to Predict Successfully Rapid Weaning Program in Cardiac Intensive Care Unit Patients" Journal of Personalized Medicine 12, no. 3: 501. https://doi.org/10.3390/jpm12030501
APA StyleChen, W.-T., Huang, H.-L., Ko, P.-S., Su, W., Kao, C.-C., & Su, S.-L. (2022). A Simple Algorithm Using Ventilator Parameters to Predict Successfully Rapid Weaning Program in Cardiac Intensive Care Unit Patients. Journal of Personalized Medicine, 12(3), 501. https://doi.org/10.3390/jpm12030501