
Respiratory Muscle Training Can Improve Cognition, Lung Function, and Diaphragmatic Thickness Fraction in Male and Non-Obese Patients with Chronic Obstructive Pulmonary Disease: A Prospective Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Protocol of Intervention
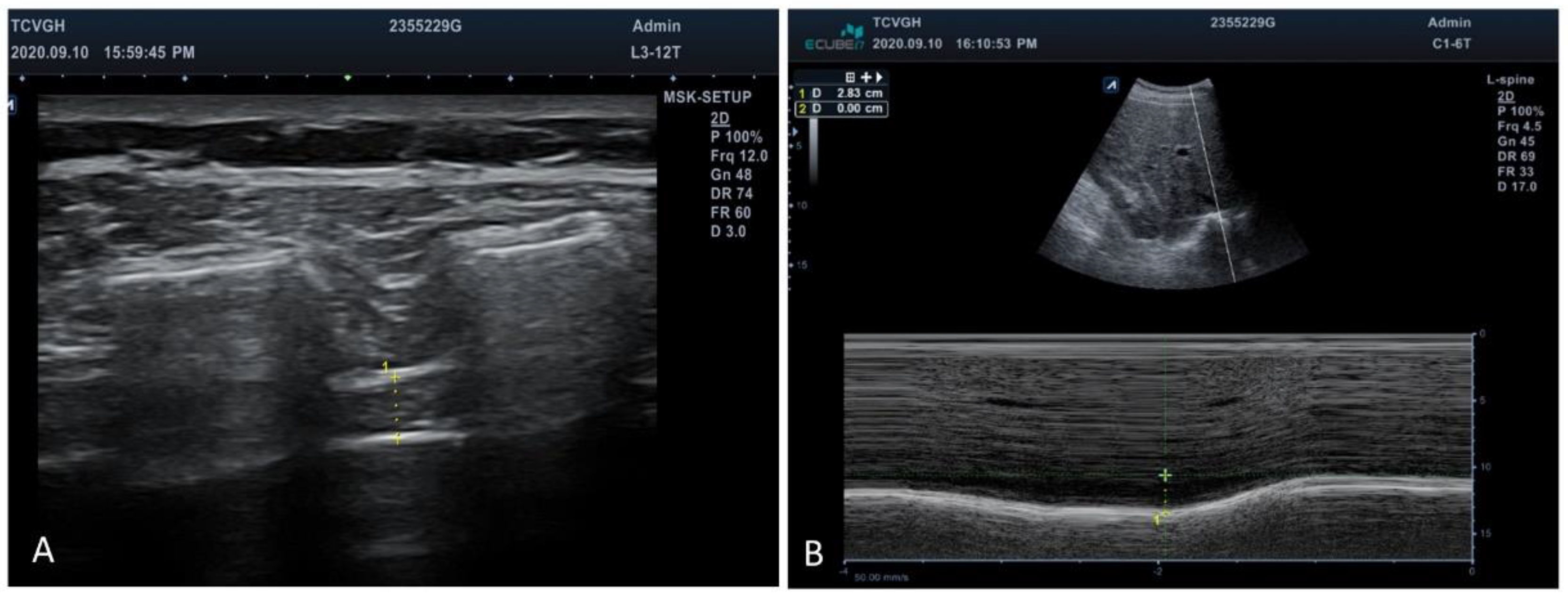
2.3. Parameter Measures
2.4. Statistical Analysis
3. Results
3.1. Patients’ Clinical and Demographic Characteristics
3.2. Differences between before and after RMT Program
3.3. Differences between the Full RMT Training and Single RMT Training Group
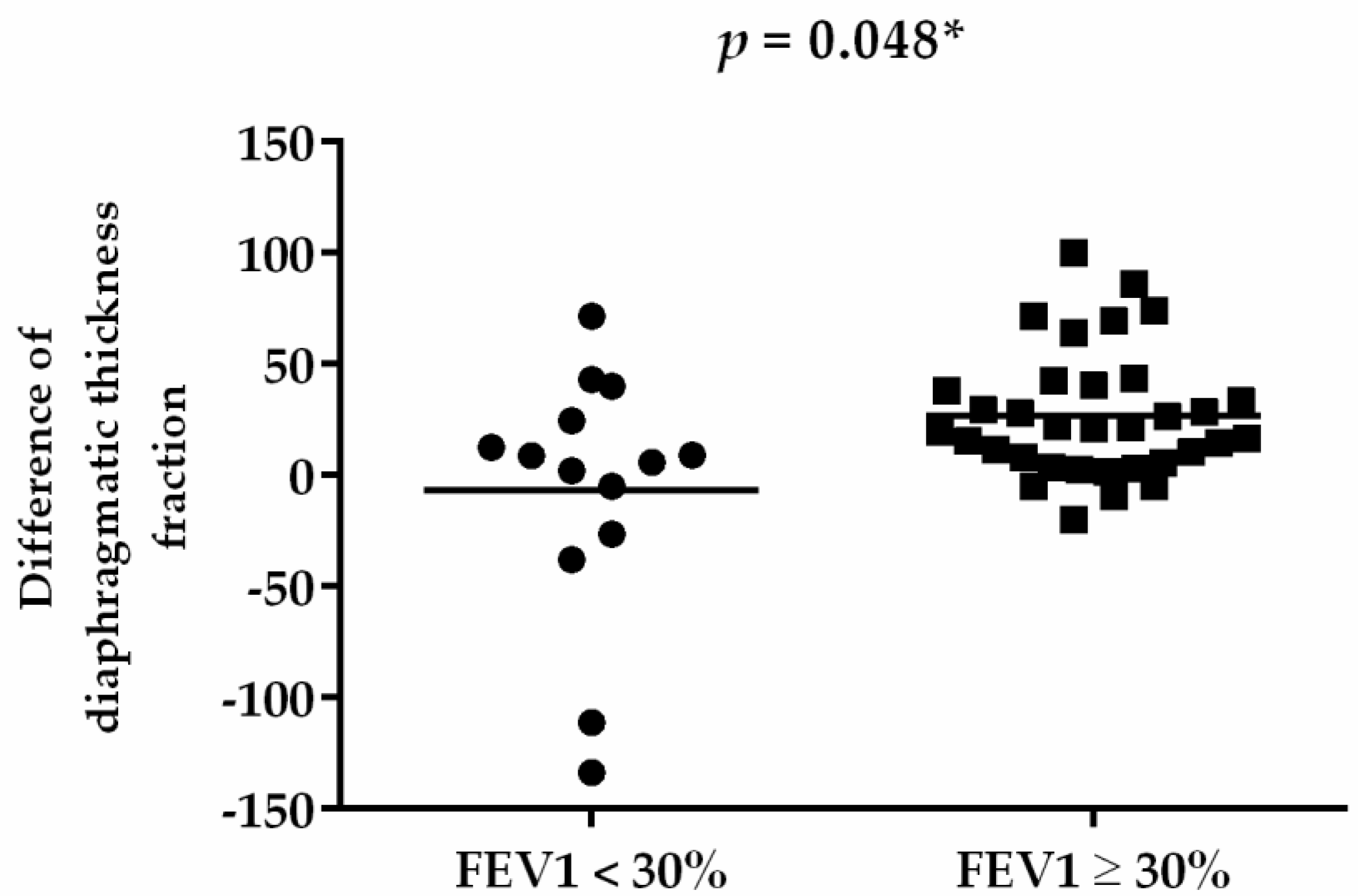
3.4. Differences of RMT Training Effect between FEV1 < 30% and FEV1 ≥ 30% among Patients with COPD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rabe, K.F.; Watz, H. Chronic obstructive pulmonary disease. Lancet 2017, 389, 1931–1940. [Google Scholar] [CrossRef]
- Ruvuna, L.; Sood, A. Epidemiology of Chronic Obstructive Pulmonary Disease. Clin. Chest Med. 2020, 41, 315–327. [Google Scholar] [CrossRef]
- McCarthy, B.; Casey, D.; Devane, D.; Murphy, K.; Murphy, E.; Lacasse, Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2015, 2, CD003793. [Google Scholar] [CrossRef]
- Beaumont, M.; Forget, P.; Couturaud, F.; Reychler, G. Effects of inspiratory muscle training in COPD patients: A systematic review and meta-analysis. Clin. Respir. J. 2018, 12, 2178–2188. [Google Scholar] [CrossRef]
- Hill, K.; Cecins, N.M.; Eastwood, P.R.; Jenkins, S.C. Inspiratory muscle training for patients with chronic obstructive pulmonary disease: A practical guide for clinicians. Arch. Phys. Med. Rehabil. 2010, 91, 1466–1470. [Google Scholar] [CrossRef]
- Frangogiannis, N.G.; Dewald, O.; Xia, Y.; Ren, G.; Haudek, S.; Leucker, T.; Kraemer, D.; Taffet, G.; Rollins, B.J.; Entman, M.L. Critical role of monocyte chemoattractant protein-1/CC chemokine ligand 2 in the pathogenesis of ischemic cardiomyopathy. Circulation 2007, 115, 584–592. [Google Scholar] [CrossRef]
- Chigira, Y.; Miyazaki, I.; Izumi, M.; Oda, T. Effects of expiratory muscle training on the frail elderly’s respiratory function. J. Phys. Ther. Sci. 2018, 30, 286–288. [Google Scholar] [CrossRef][Green Version]
- Kim, J.; Davenport, P.; Sapienza, C. Effect of expiratory muscle strength training on elderly cough function. Arch. Gerontol. Geriatr. 2009, 48, 361–366. [Google Scholar] [CrossRef]
- Xu, W.; Li, R.; Guan, L.; Wang, K.; Hu, Y.; Xu, L.; Zhou, L.; Chen, R.; Chen, X. Combination of inspiratory and expiratory muscle training in same respiratory cycle versus different cycles in COPD patients: A randomized trial. Respir. Res. 2018, 19, 225. [Google Scholar] [CrossRef]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 270–279. [Google Scholar] [CrossRef]
- Zaudig, M. A new systematic method of measurement and diagnosis of “mild cognitive impairment” and dementia according to ICD-10 and DSM-III-R criteria. Int. Psychogeriatr. 1992, 4 (Suppl. S2), 203–219. [Google Scholar] [CrossRef]
- Kakkera, K.; Padala, K.P.; Kodali, M.; Padala, P.R. Association of chronic obstructive pulmonary disease with mild cognitive impairment and dementia. Curr. Opin. Pulm. Med. 2018, 24, 173–178. [Google Scholar] [CrossRef]
- Singh, B.; Mielke, M.M.; Parsaik, A.K.; Cha, R.H.; Roberts, R.O.; Scanlon, P.D.; Geda, Y.E.; Christianson, T.J.; Pankratz, V.S.; Petersen, R.C. A prospective study of chronic obstructive pulmonary disease and the risk for mild cognitive impairment. JAMA Neurol. 2014, 71, 581–588. [Google Scholar] [CrossRef]
- Singh, B.; Parsaik, A.K.; Mielke, M.M.; Roberts, R.O.; Scanlon, P.D.; Geda, Y.E.; Pankratz, V.S.; Christianson, T.; Yawn, B.P.; Petersen, R.C. Chronic obstructive pulmonary disease and association with mild cognitive impairment: The Mayo Clinic Study of Aging. Mayo Clin. Proc. 2013, 88, 1222–1230. [Google Scholar] [CrossRef]
- Ranzini, L.; Schiavi, M.; Pierobon, A.; Granata, N.; Giardini, A. From Mild Cognitive Impairment (MCI) to Dementia in Chronic Obstructive Pulmonary Disease. Implications for Clinical Practice and Disease Management: A Mini-Review. Front. Psychol. 2020, 11, 337. [Google Scholar] [CrossRef]
- Anstey, K.J.; Windsor, T.D.; Jorm, A.F.; Christensen, H.; Rodgers, B. Association of pulmonary function with cognitive performance in early, middle and late adulthood. Gerontology 2004, 50, 230–234. [Google Scholar] [CrossRef]
- de la Torre, J.C. Critical threshold cerebral hypoperfusion causes Alzheimer’s disease? Acta Neuropathol. 1999, 98, 1–8. [Google Scholar] [CrossRef]
- Koyama, A.; O’Brien, J.; Weuve, J.; Blacker, D.; Metti, A.L.; Yaffe, K. The role of peripheral inflammatory markers in dementia and Alzheimer’s disease: A meta-analysis. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 433–440. [Google Scholar] [CrossRef]
- Venturelli, M.; Scarsini, R.; Schena, F. Six-month walking program changes cognitive and ADL performance in patients with Alzheimer. Am. J. Alzheimers Dis. Other Demen. 2011, 26, 381–388. [Google Scholar] [CrossRef]
- Vreugdenhil, A.; Cannell, J.; Davies, A.; Razay, G. A community-based exercise programme to improve functional ability in people with Alzheimer’s disease: A randomized controlled trial. Scand. J. Caring Sci. 2012, 26, 12–19. [Google Scholar] [CrossRef]
- Van de Winckel, A.; Feys, H.; De Weerdt, W.; Dom, R. Cognitive and behavioural effects of music-based exercises in patients with dementia. Clin. Rehabil. 2004, 18, 253–260. [Google Scholar] [CrossRef]
- Ferreira, L.; Tanaka, K.; Santos-Galduroz, R.F.; Galduroz, J.C. Respiratory training as strategy to prevent cognitive decline in aging: A randomized controlled trial. Clin. Interv. Aging 2015, 10, 593–603. [Google Scholar] [CrossRef]
- Sarwal, A.; Walker, F.O.; Cartwright, M.S. Neuromuscular ultrasound for evaluation of the diaphragm. Muscle Nerve 2013, 47, 319–329. [Google Scholar] [CrossRef]
- Epelman, M.; Navarro, O.M.; Daneman, A.; Miller, S.F. M-mode sonography of diaphragmatic motion: Description of technique and experience in 278 pediatric patients. Pediatr. Radiol. 2005, 35, 661–667. [Google Scholar] [CrossRef]
- Halpin, D.M.G.; Criner, G.J.; Papi, A.; Singh, D.; Anzueto, A.; Martinez, F.J.; Agusti, A.A.; Vogelmeier, C.F. Global Initiative for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease. The 2020 GOLD Science Committee Report on COVID-19 and Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2021, 203, 24–36. [Google Scholar] [CrossRef]
- Burkhardt, R.; Pankow, W. The diagnosis of chronic obstructive pulmonary disease. Dtsch. Arztebl. Int. 2014, 111, 834–845, quiz 846. [Google Scholar] [CrossRef]
- Rasekaba, T.; Lee, A.L.; Naughton, M.T.; Williams, T.J.; Holland, A.E. The six-minute walk test: A useful metric for the cardiopulmonary patient. Intern. Med. J. 2009, 39, 495–501. [Google Scholar] [CrossRef]
- Chuang, M.L. Combining Dynamic Hyperinflation with Dead Space Volume during Maximal Exercise in Patients with Chronic Obstructive Pulmonary Disease. J. Clin. Med. 2020, 9, 1127. [Google Scholar] [CrossRef]
- Boutou, A.K.; Zafeiridis, A.; Pitsiou, G.; Dipla, K.; Kioumis, I.; Stanopoulos, I. Cardiopulmonary exercise testing in chronic obstructive pulmonary disease: An update on its clinical value and applications. Clin. Physiol. Funct. Imaging 2020, 40, 197–206. [Google Scholar] [CrossRef]
- Guazzi, M.; Arena, R.; Halle, M.; Piepoli, M.F.; Myers, J.; Lavie, C.J. 2016 Focused Update: Clinical Recommendations for Cardiopulmonary Exercise Testing Data Assessment in Specific Patient Populations. Circulation 2016, 133, e694–e711. [Google Scholar] [CrossRef]
- Weiner, P.; Man, A.; Weiner, M.; Rabner, M.; Waizman, J.; Magadle, R.; Zamir, D.; Greiff, Y. The effect of incentive spirometry and inspiratory muscle training on pulmonary function after lung resection. J. Thorac. Cardiovasc. Surg. 1997, 113, 552–557. [Google Scholar] [CrossRef]
- Abodonya, A.M.; Abdelbasset, W.K.; Awad, E.A.; Elalfy, I.E.; Salem, H.A.; Elsayed, S.H. Inspiratory muscle training for recovered COVID-19 patients after weaning from mechanical ventilation: A pilot control clinical study. Medicine 2021, 100, e25339. [Google Scholar] [CrossRef]
- El-Deen, H.A.B.; Alanazi, F.S.; Ahmed, K.T. Effects of inspiratory muscle training on pulmonary functions and muscle strength in sedentary hemodialysis patients. J. Phys. Ther. Sci. 2018, 30, 424–427. [Google Scholar] [CrossRef][Green Version]
- Bostanci, O.; Mayda, H.; Yilmaz, C.; Kabadayi, M.; Yilmaz, A.K.; Ozdal, M. Inspiratory muscle training improves pulmonary functions and respiratory muscle strength in healthy male smokers. Respir. Physiol. Neurobiol. 2019, 264, 28–32. [Google Scholar] [CrossRef]
- Aydogan Arslan, S.; Ugurlu, K.; Sakizli Erdal, E.; Keskin, E.D.; Demirguc, A. Effects of Inspiratory Muscle Training on Respiratory Muscle Strength, Trunk Control, Balance and Functional Capacity in Stroke Patients: A single-blinded randomized controlled study. Top. Stroke Rehabil. 2022, 29, 40–48. [Google Scholar] [CrossRef]
- Findley, L.J.; Barth, J.T.; Powers, D.C.; Wilhoit, S.C.; Boyd, D.G.; Suratt, P.M. Cognitive impairment in patients with obstructive sleep apnea and associated hypoxemia. Chest 1986, 90, 686–690. [Google Scholar] [CrossRef]
- Areza-Fegyveres, R.; Kairalla, R.A.; Carvalho, C.R.R.; Nitrini, R. Cognition and chronic hypoxia in pulmonary diseases. Dement. Neuropsychol. 2010, 4, 14–22. [Google Scholar] [CrossRef]
- Weiner, P.; Magadle, R.; Beckerman, M.; Weiner, M.; Berar-Yanay, N. Comparison of specific expiratory, inspiratory, and combined muscle training programs in COPD. Chest 2003, 124, 1357–1364. [Google Scholar] [CrossRef]
- Weiner, P.; McConnell, A. Respiratory muscle training in chronic obstructive pulmonary disease: Inspiratory, expiratory, or both? Curr. Opin. Pulm. Med. 2005, 11, 140–144. [Google Scholar] [CrossRef]
- Chuang, M.L.; Hsieh, B.Y.; Lin, I.F. Resting Dead Space Fraction as Related to Clinical Characteristics, Lung Function, and Gas Exchange in Male Patients with Chronic Obstructive Pulmonary Disease. Int. J. Gen. Med. 2021, 14, 169–177. [Google Scholar] [CrossRef]
- Garcia, S.; Rocha, M.; Pinto, P.; Lopes, A.M.; Bárbara, C. Inspiratory muscle training in COPD patients. Rev. Port. Pneumol. 2008, 14, 177–194. [Google Scholar] [CrossRef]
- Petrovic, M.; Reiter, M.; Zipko, H.; Pohl, W.; Wanke, T. Effects of inspiratory muscle training on dynamic hyperinflation in patients with COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2012, 7, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Hill, K.; Jenkins, S.C.; Philippe, D.L.; Cecins, N.; Shepherd, K.L.; Green, D.J.; Hillman, D.R.; Eastwood, P.R. High-intensity inspiratory muscle training in COPD. Eur. Respir. J. 2006, 27, 1119–1128. [Google Scholar] [CrossRef] [PubMed]
- Beaumont, M.; Mialon, P.; Le Ber-Moy, C.; Lochon, C.; Peran, L.; Pichon, R.; Gut-Gobert, C.; Leroyer, C.; Morelot-Panzini, C.; Couturaud, F. Inspiratory muscle training during pulmonary rehabilitation in chronic obstructive pulmonary disease: A randomized trial. Chron. Respir. Dis. 2015, 12, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, R.I.N.; Azambuja, A.M.; Cureau, F.V.; Sbruzzi, G. Inspiratory Muscle Training in COPD. Respir. Care 2020, 65, 1189–1201. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, A.J. A meta-analysis of the accuracy of the mini-mental state examination in the detection of dementia and mild cognitive impairment. J. Psychiatr. Res. 2009, 43, 411–431. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Mean ± SD (n, %) |
|---|---|
| Age (years) | 67.23 ± 7.32 |
| Body mass index (kg/m2) | 23.02 ± 3.89 |
| Pulmonary function test | |
| FVC (%) | 78.77 ± 21.36 |
| FEV1 (%) | 41.08 ± 15.26 |
| FEV1/FVC (%) | 42.83 ± 14.19 |
| DLCO (%) | 78.05 ± 24.63 |
| DLCO/VA | 83.76 ± 25.82 |
| Clinical score | |
| CAT score | 14.17 ± 8.39 |
| mMRC score | 1.63 ± 0.98 |
| MMSE | 24.39 ± 2.50 |
| MIP (cmH2O) | 69.41 ± 28.02 |
| MEP (cmH2O) | 85.30 ± 18.07 |
| 6MWT | |
| 6MWT distance (m) | 328.25 ± 71.72 |
| SpO2 at rest (%) | 95.19 ± 4.98 |
| Nadir SpO2 in 6MWT | 92.69 ± 7.97 |
| Borg scale at rest | 1.17 ± 1.32 |
| Borg scale after 6MWT | 2.89 ± 1.83 |
| Sonography evaluation | |
| Diaphragmatic thickness fraction | 39.38 ± 28.50 |
| Diaphragmatic excursion (cm) | 3.00 ± 1.10 |
| CPET | |
| Vd/Vt | 32.80 ± 7.04 |
| VE/VCO2 slope | 36.81 ± 6.34 |
| FEV1 subgroup | |
| <30% | 14 (29.17%) |
| ≥30% | 34 (70.83%) |
| Respiratory training subgroup | |
| IMT | 20 (41.67%) |
| IMT + EMT | 28 (58.33%) |
| Characteristics | before RMT | after RMT | p Value |
|---|---|---|---|
| Pulmonary function test | |||
| FVC (%) | 78.25 ± 20.68 | 81.93 ± 19.14 | 0.318 |
| FEV1 (%) | 40.05 ± 15.09 | 43.75 ± 15.72 | 0.002 ** |
| FEV1/FVC (%) | 42.05 ± 14.27 | 41.81 ± 15.82 | 0.372 |
| DLCO (%) | 79.83 ± 26.93 | 80.33 ± 22.62 | 0.969 |
| DLCO/VA | 86.42 ± 31.44 | 84.67 ± 27.47 | 0.563 |
| Clinical score | |||
| CAT score | 14.17 ± 8.39 | 9.06 ± 6.06 | <0.001 ** |
| mMRC score | 1.63 ± 0.98 | 1.13 ± 0.67 | <0.001 ** |
| MMSE | 24.39 ± 2.50 | 26.00 ± 4.13 | 0.002 ** |
| MIP (cmH2O) | 64.08 ± 30.42 | 80.79 ± 36.93 | 0.001 ** |
| MEP (cmH2O) | 80.86 ± 23.48 | 99.81 ± 34.57 | 0.036 * |
| 6MWT | |||
| 6MWT distance (m) | 331.28 ± 70.05 | 338.80 ± 68.91 | 0.381 |
| SpO2 at rest (%) | 95.19 ± 4.98 | 96.67 ± 2.77 | 0.005 * |
| Nadir SpO2 in 6MWT | 92.69 ± 7.97 | 93.78 ± 4.11 | 0.466 |
| SpO2 change in 6MWT | 2.50 ± 5.82 | 2.89 ± 3.34 | 0.174 |
| Borg scale at rest | 1.17 ± 1.32 | 0.83 ± 0.97 | 0.167 |
| Borg scale after 6MWT | 2.89 ± 1.83 | 2.19 ± 1.65 | 0.020 * |
| Borg scale change in 6MWT | 1.72 ± 1.61 | 1.36 ± 1.22 | 0.232 |
| Sonography evaluation | |||
| Diaphragmatic thickness fraction | 39.38 ± 28.50 | 56.40 ± 28.16 | <0.001 ** |
| Diaphragmatic excursion | 3.00 ± 1.10 | 3.83 ± 1.31 | <0.001 ** |
| CPET | |||
| Vd/Vt | 32.83 ± 7.18 | 32.98 ± 6.54 | 0.576 |
| VE/VCO2 slope | 36.63 ± 6.41 | 36.51 ± 5.62 | 1.000 |
| IMT Only (n = 20) | IMT + EMT (n = 28) | p Value | |
|---|---|---|---|
| Pulmonary function test | |||
| FVC (%) | 83.11 ± 19.54 | 80.86 ± 19.20 | 0.722 |
| FEV1 (%) | 46.32 ± 16.93 | 41.43 ± 14.56 | 0.371 |
| FEV1/FVC (%) | 43.55 ± 18.88 | 40.24 ± 12.72 | 0.386 |
| DLCO (%) | 80.00 ± 27.95 | 72.29 ± 15.13 | 0.624 |
| DLCO/VA | 90.00 ± 28.66 | 83.36 ± 25.68 | 0.711 |
| Clinical score | |||
| CAT score | 7.75 ± 4.46 | 10.00 ± 6.91 | 0.396 |
| mMRC score | 1.20 ± 0.62 | 1.07 ± 0.72 | 0.667 |
| MMSE | 25.78 ± 5.47 | 26.14 ± 3.23 | 0.585 |
| MIP (cmH2O) | 75.25 ± 38.30 | 83.82 ± 37.69 | 0.714 |
| MEP (cmH2O) | 99.81 ± 34.57 | --- | |
| 6MWT | |||
| 6MWT distance (m) | 321.75 ± 73.09 | 351.92 ± 63.83 | 0.166 |
| SpO2 at rest (%) | 95.95 ± 2.67 | 96.16 ± 3.45 | 0.289 |
| Nadir SpO2 in 6MWT | 92.25 ± 4.89 | 92.72 ± 4.93 | 0.680 |
| SpO2 change in 6MWT | 3.70 ± 3.15 | 3.44 ± 3.88 | 0.549 |
| Borg scale at rest | 0.95 ± 0.89 | 0.64 ± 0.95 | 0.160 |
| Borg scale after 6MWT | 2.30 ± 1.98 | 2.60 ± 1.80 | 0.523 |
| Borg scale change in 6MWT | 1.35 ± 1.63 | 1.96 ± 1.43 | 0.076 |
| Sonography evaluation | |||
| Diaphragmatic thickness fraction | 50.74 ± 28.74 | 60.44 ± 27.55 | 0.098 |
| Diaphragmatic excursion (cm) | 4.00 ± 1.17 | 3.72 ± 1.40 | 0.523 |
| CPET | |||
| Vd/Vt | 31.70 ± 8.52 | 33.96 ± 4.40 | 0.230 |
| VE/VCO2 slope | 36.21 ± 5.75 | 36.75 ± 5.62 | 0.991 |
| FEV1 < 30% | FEV1 ≥ 30% | p Value | |
|---|---|---|---|
| Pulmonary function test | |||
| ΔFVC (%) | 3.33 ± 17.41 | 3.82 ± 18.62 | 0.821 |
| ΔFEV1 (%) | 3.00 ± 5.22 | 4.00 ± 7.32 | 0.666 |
| ΔFEV1/FVC (%) | −1.80 ± 13.23 | 0.43 ± 7.34 | 0.867 |
| ΔDLCO (%) | 9.33 ± 5.03 | −2.44 ± 20.28 | 0.195 |
| ΔDLCO/VA | 0.00 ± 6.08 | −2.33 ± 10.99 | 0.864 |
| Clinical score | |||
| ΔCAT score | −6.86 ± 7.49 | −4.38 ± 6.92 | 0.265 |
| ΔmMRC score | −0.86 ± 1.10 | −0.35 ± 0.69 | 0.074 |
| ΔMMSE | 2.00 ± 1.87 | 1.50 ± 2.48 | 1.000 |
| ΔMIP (cmH2O) | 8.33 ± 15.64 | 15.79 ± 23.35 | 0.549 |
| ΔMEP (cmH2O) | 18.80 ± 6.08 | 19.00 ± 23.27 | 1.000 |
| 6MWT | |||
| Δ6MWT distance (m) | 15.92 ± 65.42 | 4.21 ± 29.50 | 0.951 |
| ΔSpO2 at rest (%) | 1.86 ± 1.21 | 1.38 ± 4.03 | 0.152 |
| ΔNadir SpO2 in 6MWT | 1.57 ± 2.70 | 0.97 ± 7.20 | 0.302 |
| ΔBorg scale at rest | 0.29 ± 0.76 | −0.48 ± 1.43 | 0.122 |
| ΔBorg scale after 6MWT | −0.71 ± 1.70 | −0.69 ± 1.71 | 0.922 |
| Sonography evaluation | |||
| ΔDiaphragmatic thickness fraction | −6.84 ± 56.35 | 26.84 ± 28.55 | 0.048 * |
| ΔDiaphragmatic excursion (cm) | 1.09 ± 1.50 | 0.73 ± 1.14 | 0.734 |
| CPET | |||
| ΔVd/Vt | 0.46 ± 5.92 | 0.02 ± 4.94 | 0.565 |
| ΔVE/VCO2 slope | −0.38 ± 3.71 | −0.01 ± 5.18 | 0.678 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, Y.-Y.; Lin, S.-Y.; Hsu, C.-Y.; Fu, P.-K. Respiratory Muscle Training Can Improve Cognition, Lung Function, and Diaphragmatic Thickness Fraction in Male and Non-Obese Patients with Chronic Obstructive Pulmonary Disease: A Prospective Study. J. Pers. Med. 2022, 12, 475. https://doi.org/10.3390/jpm12030475
Cheng Y-Y, Lin S-Y, Hsu C-Y, Fu P-K. Respiratory Muscle Training Can Improve Cognition, Lung Function, and Diaphragmatic Thickness Fraction in Male and Non-Obese Patients with Chronic Obstructive Pulmonary Disease: A Prospective Study. Journal of Personalized Medicine. 2022; 12(3):475. https://doi.org/10.3390/jpm12030475
Chicago/Turabian StyleCheng, Yuan-Yang, Shih-Yi Lin, Chiann-Yi Hsu, and Pin-Kuei Fu. 2022. "Respiratory Muscle Training Can Improve Cognition, Lung Function, and Diaphragmatic Thickness Fraction in Male and Non-Obese Patients with Chronic Obstructive Pulmonary Disease: A Prospective Study" Journal of Personalized Medicine 12, no. 3: 475. https://doi.org/10.3390/jpm12030475
APA StyleCheng, Y.-Y., Lin, S.-Y., Hsu, C.-Y., & Fu, P.-K. (2022). Respiratory Muscle Training Can Improve Cognition, Lung Function, and Diaphragmatic Thickness Fraction in Male and Non-Obese Patients with Chronic Obstructive Pulmonary Disease: A Prospective Study. Journal of Personalized Medicine, 12(3), 475. https://doi.org/10.3390/jpm12030475