
Newly Diagnosed Type 2 Diabetes Care between Family Physicians, Endocrinologists, and Other Internists in Taiwan: A Retrospective Population-Based Cohort Study

 and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Source of Data
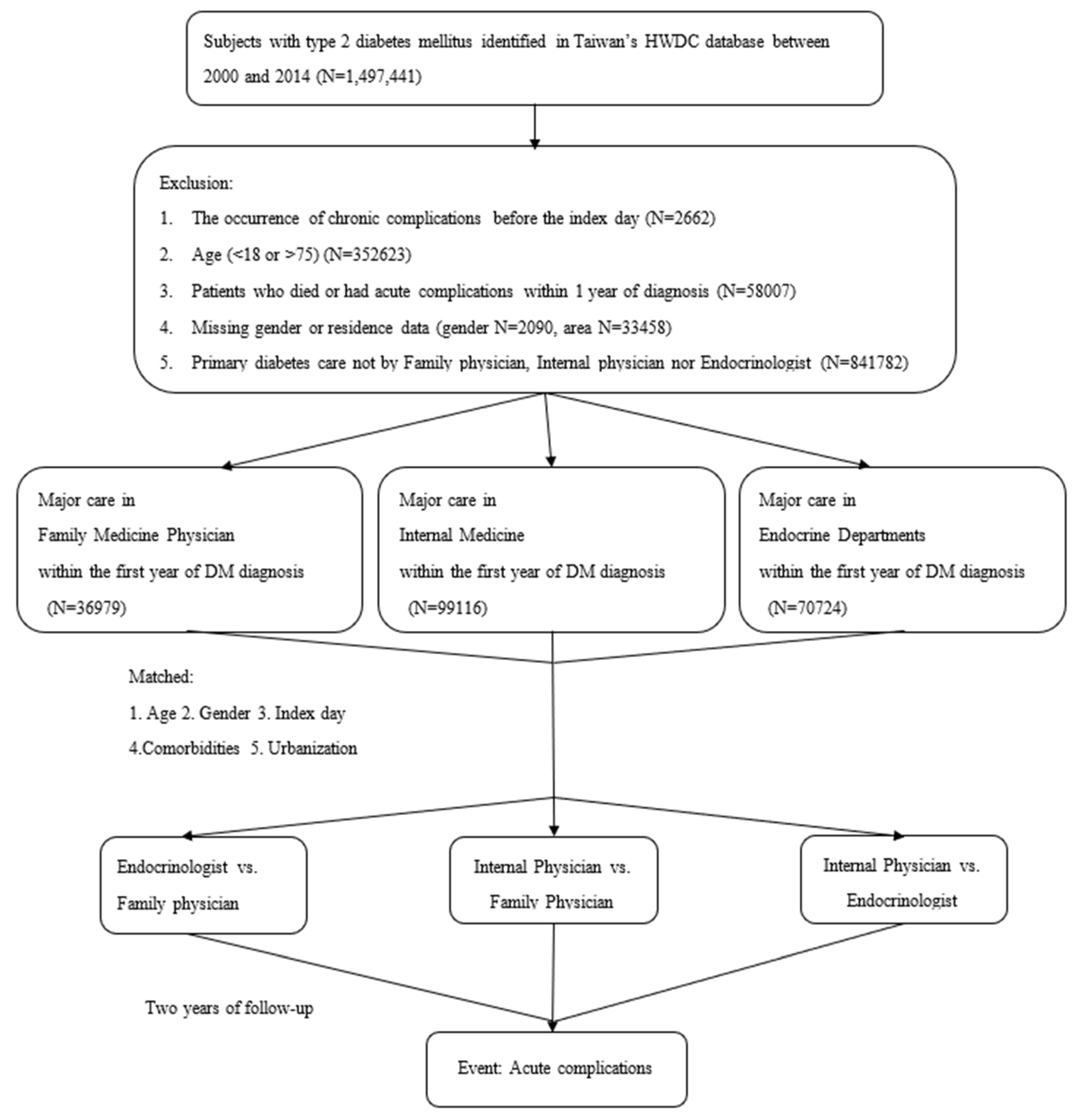
2.2. Study Design and Study Population
2.3. Outcome Indicators in Two-Year Follow-Up
2.4. Statistical Analysis and Comorbidity Risk Analysis
3. Results
3.1. Participants
3.2. Process Indicators
3.3. Total Diabetes-Related Costs
3.4. Prediction of the Occurrence of Acute Complications
3.5. Incidence of Acute Complications
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethical Approval
References
- Gregg, E.W.; Li, Y.; Wang, J.; Rios Burrows, N.; Ali, M.K.; Rolka, D.; Williams, D.E.; Geiss, L. Changes in Diabetes-Related Complications in the United States, 1990–2010. N. Engl. J. Med. 2014, 370, 1514–1523. [Google Scholar] [CrossRef] [PubMed]
- Fleming, B.B.; Greenfield, S.; Engelgau, M.M.; Pogach, L.M.; Clauser, S.B.; Parrott, M.A.; DQIP Group. The Diabetes Quality Improvement Project: Moving science into health policy to gain an edge on the diabetes epidemic. Diabetes Care 2001, 24, 1815–1820. [Google Scholar] [CrossRef] [PubMed]
- Association, A.D. 1. Improving Care and Promoting Health in Populations: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44 (Suppl. 1), S7–S14. [Google Scholar]
- Spann, S.J.; Nutting, P.A.; Galliher, J.M.; Peterson, K.A.; Pavlik, V.N.; Dickinson, L.M.; Volk, R.J. Management of Type 2 Diabetes in the Primary Care Setting: A Practice-Based Research Network Study. Ann. Fam. Med. 2006, 4, 23–31. [Google Scholar] [CrossRef]
- Saydah, S.H.; Fradkin, J.; Cowie, C.C. Poor Control of Risk Factors for Vascular Disease among Adults with Previously Diagnosed Diabetes. JAMA J. Am. Med. Assoc. 2004, 291, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Braga, M.F.B.; Casanova, A.; Teoh, H.; Gerstein, H.C.; Fitchett, D.H.; Honos, G.; McFarlane, P.A.; Ur, E.; Yale, J.-F.; Langer, A.; et al. Poor achievement of guidelines-recommended targets in type 2 diabetes: Findings from a contemporary prospective cohort study. Int. J. Clin. Pract. 2012, 66, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-J.; Lu, F.-H.; Yang, Y.-C.; Wu, J.-S.; Wu, T.-J.; Chen, M.-S.; Chuang, L.-M.; Tai, T.-Y. Epidemiologic study of type 2 diabetes in Taiwan. Diabetes Res. Clin. Pr. 2000, 50, S49–S59. [Google Scholar] [CrossRef]
- Tseng, F.-Y. Quality of medical care for noninsulin-dependent diabetic patients in a community teaching hospital in Taiwan. J. Formos. Med. Assoc. 1996, 95, 414–416. [Google Scholar]
- Tseng, F.-Y.; Lai, M.-S.; Syu, C.-Y.; Lin, C.-C. Professional accountability for diabetes care in Taiwan. Diabetes Res. Clin. Pr. 2006, 71, 192–201. [Google Scholar] [CrossRef]
- Pera, P.I. Living with diabetes: Quality of care and quality of life. Patient Prefer. Adherence 2011, 5, 65. [Google Scholar]
- Shani, M.; Taylor, T.R.; Vinker, S.; Lustman, A.; Erez, R.; Elhayany, A.; Lahad, A. Characteristics of Diabetics with Poor Glycemic Control Who Achieve Good Control. J. Am. Board Fam. Med. 2008, 21, 490–496. [Google Scholar] [CrossRef]
- Harrold, L.R.; Field, T.S.; Gurwitz, J.H. Knowledge, patterns of care, and outcomes of care for generalists and specialists. J. Gen. Intern. Med. 1999, 14, 499–511. [Google Scholar] [CrossRef]
- Ho, M.; Marger, M.; Beart, J.; Yip, I.; Shekelle, P. Is the Quality of Diabetes Care Better in a Diabetes Clinic or in a General Medicine Clinic? Diabetes Care 1997, 20, 472–475. [Google Scholar] [CrossRef] [PubMed]
- De Berardis, G.; Pellegrini, F.; Franciosi, M.; Belfiglio, M.; Di Nardo, B.; Greenfield, S.; Kaplan, S.H.; Rossi, M.C.; Sacco, M.; Tognoni, G.; et al. Quality of care and outcomes in type 2 diabetic patients: A comparison between general practice and diabetes clinics. Diabetes Care 2004, 27, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Greenfield, S.; Kaplan, S.H.; Kahn, R.; Ninomiya, J.; Griffith, J.L. Profiling care provided by different groups of physicians: Effects of patient case-mix (bias) and physician-level clustering on quality assessment results. Ann. Intern. Med. 2002, 136, 111–121. [Google Scholar] [CrossRef]
- Greenfield, S.; Rogers, W.; Mangotich, M.; Carney, M.F.; Tarlov, A.R. Outcomes of Patients with Hypertension and Non—insulin-dependentn Diabetes Mellitus Treated by Different Systems and Specialties: Results From the Medical Outcomes Study. JAMA 1995, 274, 1436–1444. [Google Scholar] [CrossRef]
- Tseng, F.-Y.; Lai, M.-S. Effects of Physician Specialty on Use of Antidiabetes Drugs, Process and Outcomes of Diabetes Care in a Medical Center. J. Formos. Med. Assoc. 2006, 105, 821–831. [Google Scholar] [CrossRef][Green Version]
- Liu, C.-C.; Chen, K.-R.; Chen, H.-F.; Huang, S.-L.; Chen, C.-C.; Lee, M.-D.; Ko, M.-C.; Li, C.-Y. Association of doctor specialty with diabetic patient risk of hospitalization due to diabetic ketoacidosis: A national population-based study in Taiwan. J. Eval. Clin. Pr. 2010, 17, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.-Y.; Su, C.-C.; Shao, S.-C.; Sung, S.-F.; Lin, S.-J.; Kao Yang, Y.-H.; Lai, E.C.-C. Taiwan’s National Health Insurance Research Database: Past and future. Clin. Epidemiol. 2019, 11, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Miller, D.R.; Safford, M.M.; Pogach, L.M. Who Has Diabetes?Best Estimates of Diabetes Prevalence in the Department of Veterans Affairs Based on Computerized Patient Data. Diabetes Care 2004, 27, b10–b21. [Google Scholar] [CrossRef]
- Lin, C.-C.; Lai, M.-S.; Syu, C.-Y.; Chang, S.-C.; Tseng, F.-Y. Accuracy of diabetes diagnosis in health insurance claims data in Taiwan. J. Formos. Med. Assoc. 2005, 104, 157–163. [Google Scholar]
- Haller, B.; Schmidt, G.; Ulm, K. Applying competing risks regression models: An overview. Lifetime Data Anal. 2012, 19, 33–58. [Google Scholar] [CrossRef] [PubMed]
- Association, A.D. 4. Comprehensive medical evaluation and assessment of comorbidities: Standards of medical care in diabetes-2021. Diabetes Care 2021, 44 (Suppl. 1), S40–S52. [Google Scholar] [CrossRef] [PubMed]
- Chau, Y.-L. Effects of Care-Seeking Behavior on Health Service Utilization: A Study Based on Patients with Diabetes in Taiwan; Asian University: Taichung City, Taiwan, 2005. [Google Scholar]



{kind=link}
{kind=link}
| FM n = 28,269 | IM n = 28,269 | p-Value | |
|---|---|---|---|
| Age | 56.43 ± 10.03 | 54.99 ± 10.22 | <0.001 |
| Gender—no. (%) | >0.999 | ||
| Female | 15,940 (56.39) | 15,940 (56.39) | |
| Male | 12,329 (43.61) | 12,329 (43.61) | |
| Urbanization—no. (%) | >0.999 | ||
| High | 11,309 (40.00) | 11,309 (40.00) | |
| Moderate | 12,454 (44.06) | 12,454 (44.06) | |
| Low | 4506 (15.94) | 4506 (15.94) | |
| Testing frequency (per year) | |||
| HbA1C | 3.19 ± 2.75 | 2.8 ± 2.84 | <0.001 |
| Lipid profile | 7.29 ± 7.09 | 6.97 ± 7.41 | <0.001 |
| ACR | 0.46 ± 1.13 | 0.68 ± 1.74 | <0.001 |
| Insulin (1 month) b | 0.3 ± 1.42 | 0.45 ± 1.78 | <0.001 |
| Cost c | 487.41 ± 590.97 | 507.67 ± 853.62 | 0.01 |
| Comorbidities—no. (%) | |||
| Myocardial infarct | 875 (3.1) | 912 (3.23) | 0.374 |
| Congestive heart failure | 1646 (5.82) | 1692 (5.99) | 0.412 |
| Peripheral vascular disease | 1188 (4.2) | 1227 (4.34) | 0.417 |
| Cerebrovascular disease | 2882 (10.19) | 2820 (9.98) | 0.387 |
| Dementia | 47 (0.17) | 40 (0.14) | 0.453 |
| Chronic lung disease | 5401 (19.11) | 5343 (18.9) | 0.534 |
| Connective tissue disease | 221 (0.78) | 203 (0.72) | 0.380 |
| Ulcer | 8469 (29.96) | 8431 (29.82) | 0.727 |
| Chronic liver disease | 7726 (27.33) | 7974 (28.21) | 0.02 |
| Hemiplegia | 15 (0.05) | 10 (0.04) | 0.317 |
| Moderate or severe kidney disease | 701 (2.48) | 688 (2.43) | 0.724 |
| Tumor, leukemia, lymphoma | 2537 (8.97) | 2518 (8.91) | 0.779 |
| Moderate or severe liver disease | 137 (0.48) | 138 (0.49) | 0.952 |
| Malignant tumor, metastasis | 537 (1.90) | 555 (1.96) | 0.582 |
| AIDS | 0 | 0 | |
| Acute Complications—no. (%) | 401 (1.42) | 665 (2.35) | <0.001 |
| FM n = 23,407 | Endocrinologist n = 23,407 | p-Value | |
|---|---|---|---|
| Age | 55.48 ± 10.09 | 54.54 ± 10.11 | <0.001 |
| Gender—no. (%) | >0.999 | ||
| Female | 13,274 (56.71) | 13,274 (56.71) | |
| Male | 10,133 (43.29) | 10,133 (43.29) | |
| Urbanization—no. (%) | >0.999 | ||
| High | 10,455 (44.67) | 10,455 (44.67) | |
| Moderate | 9974 (42.61) | 9974 (42.61) | |
| Low | 2978 (12.72) | 2978 (12.72) | |
| Testing frequency (per year) | |||
| HbA1C | 3.23 ± 2.76 | 4.89 ± 3.52 | <0.001 |
| Lipid profile | 7.42 ± 7.13 | 10.58 ± 8.34 | <0.001 |
| ACR | 0.46 ± 1.13 | 1.27 ± 1.93 | <0.001 |
| Insulin (1 month) b | 0.28 ± 1.28 | 0.81 ± 2.44 | <0.001 |
| Cost c | 484.39 ± 574.26 | 927.85 ± 922.90 | <0.001 |
| Comorbidities—no. (%) | |||
| Myocardial infarct | 626 (2.67) | 647 (2.76) | 0.551 |
| Congestive heart failure | 1181 (5.05) | 1295 (5.53) | 0.019 |
| Peripheral vascular disease | 633 (2.7) | 684 (2.92) | 0.154 |
| Cerebrovascular disease | 2223 (9.5) | 2387 (10.2) | 0.011 |
| Dementia | 48 (0.21) | 54 (0.23) | 0.552 |
| Chronic lung disease | 3816 (16.3) | 3876 (16.56) | 0.454 |
| Connective tissue disease | 269 (1.15) | 287 (1.23) | 0.443 |
| Ulcer | 6038 (25.8) | 6106 (26.09) | 0.473 |
| Chronic liver disease | 5225 (22.32) | 5077 (21.69) | 0.099 |
| Hemiplegia | 3 (0.01) | 3 (0.01) | >0.999 |
| Moderate or severe kidney disease | 584 (2.49) | 523 (2.23) | 0.064 |
| Tumor, leukemia, lymphoma | 1949 (8.33) | 2023 (8.64) | 0.220 |
| Moderate or severe liver disease | 50 (0.21) | 50 (0.21) | >0.999 |
| Malignant tumor, metastasis | 212 (0.91) | 216 (0.92) | 0.846 |
| AIDS | 0 | 0 | |
| Acute Complications—no. (%) | 302 (1.29) | 479 (2.05) | <0.001 |
| Endocrinologist n = 43,693 | IM n = 43,693 | p-Value | |
|---|---|---|---|
| Age | 54.08 ± 10.56 | 53.59 ± 10.73 | <0.001 |
| Gender—no. (%) | >0.999 | ||
| Female | 25,508 (58.38) | 25,508 (58.38) | |
| Male | 18,185 (41.62) | 18,185 (41.62) | |
| Urbanization—no. (%) | >0.999 | ||
| High | 22,467 (51.42) | 22,467 (51.42) | |
| Moderate | 16,974 (38.85) | 16,974 (38.85) | |
| Low | 4252 (9.73) | 4252 (9.73) | |
| Testing frequency (per year) | |||
| HbA1C | 4.95 ± 3.61 | 2.84 ± 2.87 | <0.001 |
| Lipid profile | 10.69 ± 8.48 | 7.15 ± 7.53 | <0.001 |
| ACR | 1.25 ± 1.89 | 0.68 ± 1.71 | <0.001 |
| Insulin (1 month) b | 0.83 ± 2.43 | 0.43 ± 1.73 | <0.001 |
| Cost c | 932.27 ± 943.78 | 502.05 ± 839.06 | <0.001 |
| Comorbidities—no. (%) | |||
| Myocardial infarct | 806 (1.84) | 825 (1.89) | 0.635 |
| Congestive heart failure | 2454 (5.62) | 2442 (5.59) | 0.860 |
| Peripheral vascular disease | 1688 (3.86) | 1636 (3.74) | 0.358 |
| Cerebrovascular disease | 4573 (10.47) | 4271 (9.78) | <0.001 |
| Dementia | 94 (0.22) | 75 (0.17) | 0.144 |
| Chronic lung disease | 7055 (16.15) | 6744 (15.43) | 0.004 |
| Connective tissue disease | 269 (0.62) | 258 (0.59) | 0.631 |
| Ulcer | 12,006 (27.48) | 11,980 (27.42) | 0.844 |
| Chronic liver disease | 10,059 (23.02) | 10,345 (23.68) | 0.022 |
| Hemiplegia | 56 (0.13) | 47 (0.11) | 0.375 |
| Moderate or severe kidney disease | 831 (1.90) | 986 (2.26) | <0.001 |
| Tumor, leukemia, lymphoma | 3420 (7.83) | 3443 (7.88) | 0.772 |
| Moderate or severe liver disease | 373 (0.85) | 392 (0.90) | 0.490 |
| Malignant tumor, metastasis | 597 (1.37) | 609 (1.39) | 0.728 |
| AIDS | 0 | 0 | |
| Acute Complications—no. (%) | 924 (2.11) | 936 (2.14) | 0.779 |
| Endocrine vs. FM | IM vs. FM | IM vs. Endocrine | ||||
|---|---|---|---|---|---|---|
| sHR d (95% CI) | p-Value | sHR (95% CI) | p-Value | sHR (95% CI) | p-Value | |
| Endocrine vs. FM | 1.57 (1.38–1.78) | <0.001 | ||||
| IM vs. FM | 1.26 (1.08–1.47) | 0.003 | ||||
| IM vs. Endocrine | 1.10 (1.00–1.21) | 0.046 | ||||
| Age | 1.00 (0.99–1.01) | 0.780 | 1.00 (1.00–1.01) | 0.210 | 1.00 (0.99–1.00) | 0.669 |
| Male vs. Female | 1.06 (0.93–1.20) | 0.383 | 1.01 (0.87–1.16) | 0.942 | 0.99 (0.90–1.09) | 0.784 |
| Urbanization | ||||||
| High | REF. | REF. | REF. | |||
| Moderate | 1.22 (1.06–1.39) | 0.006 | 0.99 (0.84–1.15) | 0.869 | 1.19 (1.08–1.31) | <0.001 |
| Low | 1.45 (1.22–1.72) | <0.001 | 1.41 (1.15–1.72) | <0.001 | 1.40 (1.21–1.63) | <0.001 |
| Testing frequency (per year) | ||||||
| HbA1C | 0.94 (0.91–0.97) | <0.001 | 0.97 (0.95–1.00) | 0.091 | 0.98 (0.96–0.99) | 0.01 |
| Lipid profile | 1.01 (1.00–1.02) | 0.140 | 1.01 (0.99–1.02) | 0.267 | 1.00 (0.99–1.01) | 0.832 |
| ACR | 1.08 (1.06–1.09) | <0.001 | 1.03 (0.99–1.07) | 0.133 | 1.05 (1.03–1.07) | <0.001 |
| Insulin (1 month) b | 1.07 (1.05–1.09) | <0.001 | 1.07 (1.05–1.08) | <0.001 | 1.07 (1.05–1.08) | <0.001 |
| Cost c | 1.00 (1.00–1.00) | <0.001 | 1.00 (1.00–1.00) | <0.001 | 1.00 (1.00–1.00) | <0.001 |
| Comorbidities | ||||||
| Myocardial infarct | 1.62 (1.27–2.07) | <0.001 | 1.36 (0.99–1.88) | 0.061 | 1.53 (1.22–1.93) | <0.001 |
| Congestive heart failure | 1.80 (1.48–2.19) | <0.001 | 1.48 (1.15–1.89) | 0.002 | 1.68 (1.44–1.97) | <0.001 |
| Peripheral vascular disease | 1.85 (1.50–2.29) | <0.001 | 1.56 (1.16–2.10) | 0.004 | 1.94 (1.65–2.29) | <0.001 |
| Cerebrovascular disease | 1.72 (1.46–2.02) | <0.001 | 1.79 (1.48–2.15) | <0.001 | 1.64 (1.45–1.86) | <0.001 |
| Dementia | 2.00 (0.64–6.22) | 0.233 | 0.51 (0.07–3.67) | 0.508 | 1.35 (0.56–3.26) | 0.501 |
| Chronic lung disease | 0.91 (0.77–1.06) | 0.227 | 0.82 (0.67–1.01) | 0.065 | 0.96 (0.85–1.10) | 0.570 |
| Connective tissue disease | 1.63 (0.99–2.69) | 0.055 | 1.51 (0.89–2.57) | 0.126 | 1.46 (0.93–2.30) | 0.101 |
| Ulcer | 0.98 (0.85–1.12) | 0.720 | 0.94 (0.79–1.11) | 0.440 | 1.04 (0.94–1.16) | 0.439 |
| Chronic liver disease | 1.08 (0.94–1.24) | 0.289 | 0.99 (0.83–1.19) | 0.913 | 0.99 (0.89–1.12) | 0.914 |
| Hemiplegia | 1.05 (0.15–7.52) | 0.962 | - | 0.65 (0.16–2.64) | 0.549 | |
| Moderate or severe kidney disease | 1.29 (0.93–1.80) | 0.133 | 1.38 (0.94–2.02) | 0.096 | 1.09 (0.82–1.45) | 0.569 |
| Tumor, leukemia, lymphoma | 0.84 (0.64–1.10) | 0.200 | 1.01 (0.76–1.34) | 0.965 | 0.81 (0.66–1.00) | 0.048 |
| Moderate or severe liver disease | 1.04 (0.43–2.52) | 0.936 | 0.67 (0.09–4.78) | 0.687 | 2.23 (1.53–3.24) | <0.001 |
| Malignant tumor, metastasis | 1.44 (0.86–2.41) | 0.165 | 1.71 (0.88–3.33) | 0.115 | 1.99 (1.34–2.97) | <0.001 |
| AIDS | - | - | - | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chou, P.-L.; Chiang, I.-H.; Lin, C.-W.; Wang, H.-H.; Wang, H.-K.; Huang, C.-H.; Chang, C.-S.; Huang, R.-Y.; Lin, C.-Y. Newly Diagnosed Type 2 Diabetes Care between Family Physicians, Endocrinologists, and Other Internists in Taiwan: A Retrospective Population-Based Cohort Study. J. Pers. Med. 2022, 12, 461. https://doi.org/10.3390/jpm12030461
Chou P-L, Chiang I-H, Lin C-W, Wang H-H, Wang H-K, Huang C-H, Chang C-S, Huang R-Y, Lin C-Y. Newly Diagnosed Type 2 Diabetes Care between Family Physicians, Endocrinologists, and Other Internists in Taiwan: A Retrospective Population-Based Cohort Study. Journal of Personalized Medicine. 2022; 12(3):461. https://doi.org/10.3390/jpm12030461
Chicago/Turabian StyleChou, Pei-Lin, I-Hui Chiang, Chi-Wei Lin, His-Hao Wang, Hao-Kuang Wang, Chi-Hsien Huang, Chao-Sung Chang, Ru-Yi Huang, and Chung-Ying Lin. 2022. "Newly Diagnosed Type 2 Diabetes Care between Family Physicians, Endocrinologists, and Other Internists in Taiwan: A Retrospective Population-Based Cohort Study" Journal of Personalized Medicine 12, no. 3: 461. https://doi.org/10.3390/jpm12030461
APA StyleChou, P.-L., Chiang, I.-H., Lin, C.-W., Wang, H.-H., Wang, H.-K., Huang, C.-H., Chang, C.-S., Huang, R.-Y., & Lin, C.-Y. (2022). Newly Diagnosed Type 2 Diabetes Care between Family Physicians, Endocrinologists, and Other Internists in Taiwan: A Retrospective Population-Based Cohort Study. Journal of Personalized Medicine, 12(3), 461. https://doi.org/10.3390/jpm12030461