
The Sequential Change in Left Ventricular Function among Various Cardiovascular Diseases: A 12-Year Study

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Methods
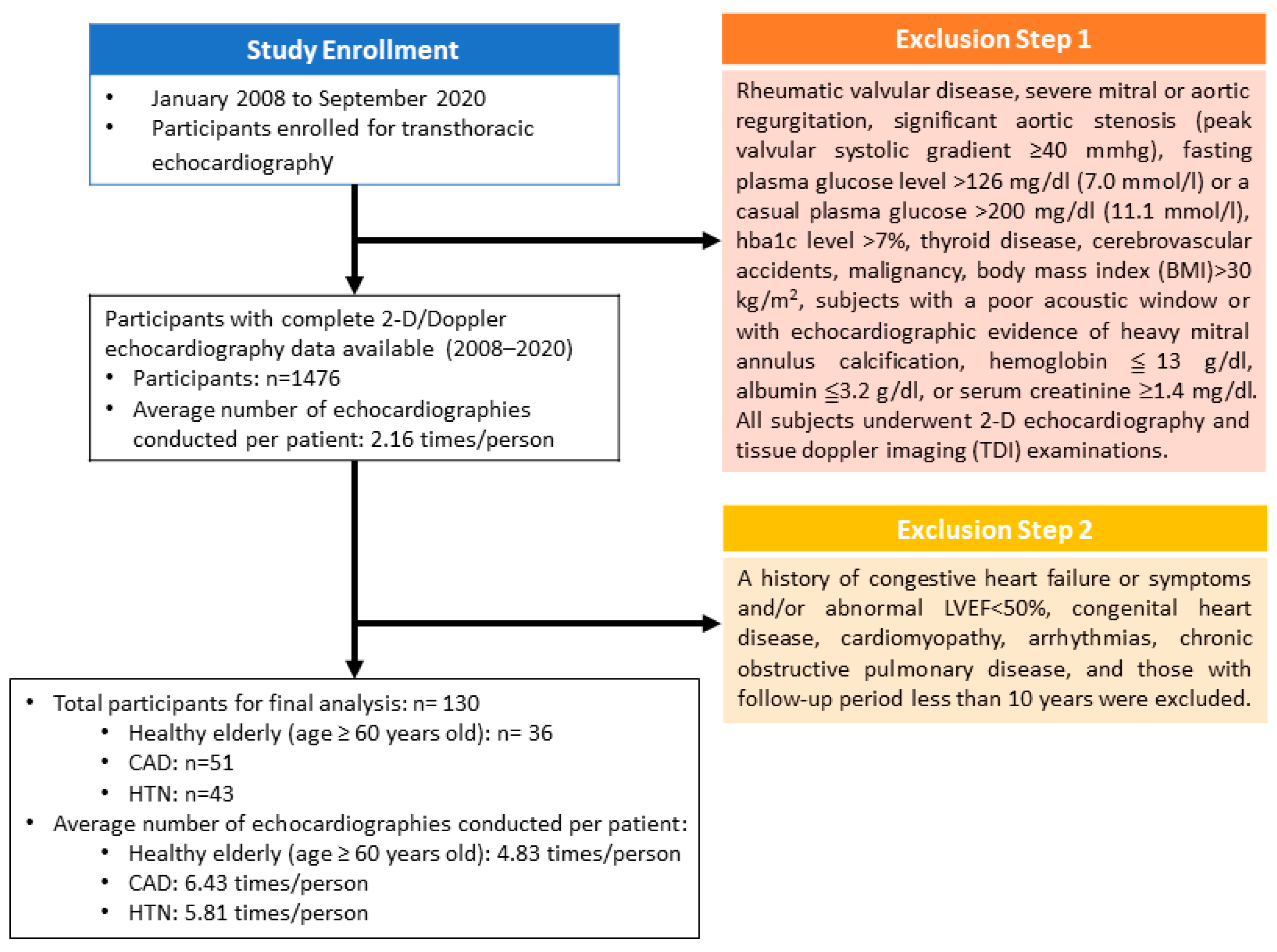
2.1. Study Setting and Participants
2.2. Study Algorithms
2.3. Grouping
2.4. Two-Dimensional Echocardiography and Tissue Doppler Imaging
2.5. Score Calculation by the Novel Integrated Score Index
2.6. Statistical Analyses
3. Results
Basic Characteristics and Demographics of Echocardiography
4. Discussion
4.1. The Main Findings of This Study
4.2. The Clinical Parameters for Detecting LV Diastolic Function with Aging
4.3. The Change in LV Diastolic Function with Aging
4.4. The Aging Effects on the Diastolic Function between the Elderly and HTN Groups
4.5. The Aging Effects on the Diastolic Function between the CAD and HTN Groups
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xu, B.; Daimon, M. Cardiac aging phenomenon and its clinical features by echocardiography. J. Echocardiogr. 2016, 14, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Sorop, O.; Heinonen, I.; van Kranenburg, M.; van de Wouw, J.; de Beer, V.J.; Nguyen, I.T.N.; Octavia, Y.; van Duin, R.W.B.; Stam, K.; van Geuns, R.J.; et al. Multiple common comorbidities produce left ventricular diastolic dysfunction associated with coronary microvascular dysfunction, oxidative stress, and myocardial stiffening. Cardiovasc. Res. 2018, 114, 954–964. [Google Scholar] [CrossRef] [PubMed]
- Upadhya, B.; Kitzman, D.W. Heart failure with preserved ejection fraction: New approaches to diagnosis and management. Clin. Cardiol. 2020, 43, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Kuznetsova, T.; Thijs, L.; Knez, J.; Cauwenberghs, N.; Petit, T.; Gu, Y.M.; Zhang, Z.; Staessen, J.A. Longitudinal changes in left ventricular diastolic function in a general population. Circ. Cardiovasc. Imaging 2015, 8, e002882. [Google Scholar] [CrossRef] [Green Version]
- Cassar, A.; Holmes, D.R., Jr.; Rihal, C.S.; Gersh, B.J. Chronic coronary artery disease: Diagnosis and management. Mayo Clin. Proc. 2009, 84, 1130–1146. [Google Scholar] [CrossRef] [Green Version]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef]
- Saraste, A.; Knuuti, J. ESC 2019 guidelines for the diagnosis and management of chronic coronary syndromes : Recommendations for cardiovascular imaging. Herz 2020, 45, 409–420. [Google Scholar] [CrossRef]
- Gerc, V.; Buksa, M. Similarity and difference between American (JNC 7) and European (2003 ESH/ESC) guidelines for management of hypertension. Med. Arh. 2005, 59, 396–399. [Google Scholar]
- Green, L. JNC 7 express: New thinking in hypertension treatment. Am. Fam. Physician 2003, 68, 228. [Google Scholar]
- Sanders, M.; Fiscella, K.; Hill, E.; Ogedegbe, O.; Cassells, A.; Tobin, J.N.; Williams, S.; Veazie, P. Motivation to move fast, motivation to wait and see: The association of prevention and promotion focus with clinicians’ implementation of the JNC-7 hypertension treatment guidelines. J. Clin. Hypertens. 2021, 23, 1752–1757. [Google Scholar] [CrossRef]
- Flack, J.M.; Adekola, B. Blood pressure and the new ACC/AHA hypertension guidelines. Trends Cardiovasc. Med. 2020, 30, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F.; Appleton, C.P.; Gillebert, T.C.; Marino, P.N.; Oh, J.K.; Smiseth, O.A.; Waggoner, A.D.; Flachskampf, F.A.; Pellikka, P.A.; Evangelista, A. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. J. Am. Soc. Echocardiogr. 2009, 22, 107–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gottdiener, J.S.; Bednarz, J.; Devereux, R.; Gardin, J.; Klein, A.; Manning, W.J.; Morehead, A.; Kitzman, D.; Oh, J.; Quinones, M.; et al. American Society of Echocardiography recommendations for use of echocardiography in clinical trials. J. Am. Soc. Echocardiogr. 2004, 17, 1086–1119. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef] [Green Version]
- Chang, S.N.; Juang, J.J.; Tsai, C.T.; Ko, J.T.; Lien, W.P. A Novel Integrated Score Index of Echocardiographic Indices for the Evaluation of Left Ventricular Diastolic Function. PLoS ONE 2015, 10, e0142175. [Google Scholar] [CrossRef]
- Shek, D.T.; Ma, C.M. Longitudinal data analyses using linear mixed models in SPSS: Concepts, procedures and illustrations. ScientificWorldJournal 2011, 11, 42–76. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.; Wang, Z.; Chang, Y.I. Sequential adaptive variables and subject selection for GEE methods. Biometrics 2020, 76, 496–507. [Google Scholar] [CrossRef]
- Caraballo, C.; Desai, N.R.; Mulder, H.; Alhanti, B.; Wilson, F.P.; Fiuzat, M.; Felker, G.M.; Piña, I.L.; O’Connor, C.M.; Lindenfeld, J.; et al. Clinical Implications of the New York Heart Association Classification. J. Am. Heart Assoc. 2019, 8, e014240. [Google Scholar] [CrossRef]
- Hoshida, S.; Shinoda, Y.; Ikeoka, K.; Fukuoka, H.; Inui, H.; Watanabe, T. Age- and sex-related differences in diastolic function and cardiac dimensions in a hypertensive population. ESC Heart Fail. 2016, 3, 270–277. [Google Scholar] [CrossRef] [Green Version]
- Ujjawal, A.; Gupta, M.; Ghosh, R.K.; Jain, V.; Bandyopadhyay, D.; Qamar, A.; Aronow, W.S.; Deedwania, P.; Kapadia, S.; Lavie, C.J. Aspirin for Primary Prevention of Coronary Artery Disease. Curr. Probl. Cardiol. 2021, 46, 100553. [Google Scholar] [CrossRef]
- Lockery, J.E.; Ernst, M.E.; Broder, J.C.; Orchard, S.G.; Murray, A.; Nelson, M.R.; Stocks, N.P.; Wolfe, R.; Reid, C.M.; Liew, D.; et al. Prescription Medication Use in Older Adults Without Major Cardiovascular Disease Enrolled in the Aspirin in Reducing Events in the Elderly (ASPREE) Clinical Trial. Pharmacotherapy 2020, 40, 1042–1053. [Google Scholar] [CrossRef] [PubMed]
- Ernst, M.E.; Fravel, M.A.; Webb, K.L.; Wetmore, J.B.; Wolfe, R.; Chowdhury, E.; Reid, C.M.; Woods, R.L.; Beilin, L.; Margolis, K.L.; et al. Long-Term Blood Pressure Variability and Kidney Function in Participants of the ASPREE Trial. Am. J. Hypertens. 2022, 35, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Slivnick, J.; Lampert, B.C. Hypertension and Heart Failure. Heart Fail. Clin. 2019, 15, 531–541. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Elderly | CAD | HTN | ||
|---|---|---|---|---|
| Cases (M/W) | n = 36 (12/24) | n =51 (42/9) | n = 43 (23/20) | |
| Diastolic Dysfunction Grade (normal/1/2/3) [12] | 28/3/5/0 | 7/6/38/0 | 4/10/29/0 | |
| Mean ± SD | Mean ± SD | Mean ± SD | p-Value | |
| Age (yrs) | 79.39 ± 9.51 | 68.31 ± 12.09 | 67.51 ± 5.92 | <0.001 |
| BMI (kg/m2) | 23.32 ± 2.67 | 25.17 ± 2.98 | 24.84 ± 2.98 | 0.01 |
| SBP (mmHg) | 132.75 ± 15.80 | 134.20 ± 14.70 | 138.93 ± 17.33 | 0.19 |
| DBP (mmHg) | 72.14 ± 8.01 | 77.22 ± 9.02 | 81.35 ± 9.27 | <0.001 |
| HR (beats/min) | 69.31 ± 9.56 | 68.55 ± 8.18 | 66.40 ± 8.26 | 0.29 |
| EDD (mm) | 4.43 ± 0.53 | 4.77 ± 0.59 | 4.77 ± 0.43 | 0.01 |
| LA (mm) | 3.39 ± 0.50 | 3.75 ± 0.55 | 3.47 ± 0.70 | 0.01 |
| IVS (mm) | 0.97 ± 0.23 | 1.03 ± 0.27 | 0.98 ± 0.16 | 0.39 |
| PW (mm) | 0.90 ± 0.18 | 0.94 ± 0.17 | 0.90 ± 0.15 | 0.48 |
| LVEF (%) | 61.75 ± 6.25 | 60.46 ± 8.23 | 62.54 ± 7.86 | 0.41 |
| E/A | 0.83 ± 0.25 | 0.96 ± 0.35 | 0.92 ± 0.25 | 0.11 |
| DT (ms) | 233.21 ± 45.42 | 233.06 ± 52.60 | 232.69 ± 49.93 | 1 |
| Sep e′/a′ | 0.65 ± 0.20 | 0.67 ± 0.22 | 0.65 ± 0.15 | 0.84 |
| Lat e′/a′ | 0.77 ± 0.31 | 0.80 ± 0.28 | 0.78 ± 0.24 | 0.89 |
| Sep E/e′ | 12.73 ± 4.22 | 12.73 ± 3.91 | 12.37 ± 3.93 | 0.89 |
| Lat E/e′ | 9.54 ± 2.82 | 9.32 ± 3.40 | 9.21 ± 3.00 | 0.9 |
| Score | 7.31 ± 2.97 | 6.82 ± 3.17 | 7.19 ± 2.88 | 0.73 |
| NYHA | 1.11 ± 0.32 | 1.08 ± 0.27 | 1.00 ± 0.00 | 0.1 |
| Hb (g/dL) | 12.72 ± 1.54 | 14.35 ± 1.64 | 13.38 ± 1.30 | 0.01 |
| Cr (mg/dL) | 0.84 ± 0.22 | 0.98 ± 0.20 | 0.88 ± 0.21 | 0.03 |
| K (mmol/L) | 4.15 ± 0.50 | 4.05 ± 0.39 | 4.32 ± 0.29 | 0.1 |
| eGFR (mL/min/1.73 m2) | 76.24 ± 21.17 | 79.89 ± 19.04 | 82.15 ± 15.19 | 0.64 |
| β-blocker | 0.19 ± 0.40 | 0.35 ± 0.48 | 0.35 ± 0.48 | 0.23 |
| CCB | 0.53 ± 0.51 | 0.39 ± 0.49 | 0.77 ± 0.43 | <0.001 |
| ACEI/ARB | 0.42 ± 0.50 | 0.57 ± 0.50 | 0.86 ± 0.35 | <0.001 |
| Spironolactone | 0.00 ± 0.00 | 0.08 ± 0.27 | 0.12 ± 0.32 | 0.12 |
| Elderly | CAD | HTN | ||||
|---|---|---|---|---|---|---|
| Change with Age (per Year) | p-value | Change with Age (per Year) | p-Value | Change with Age (per Year) | p-Value | |
| BMI (kg/m2) | 0.038 | <0.001 | −0.01 | 0.17 | −0.083 | 0.01 |
| SBP (mmHg) | 0.5 | <0.001 | 0.212 | <0.001 | 0.212 | 0.18 |
| DBP (mmHg) | −0.308 | <0.001 | −0.363 | <0.001 | −0.382 | <0.001 |
| HR (beats/min) | 0.153 | <0.001 | 0.002 | 0.97 | 0.345 | <0.001 |
| EDD (mm) | −0.006 | <0.001 | −0.007 | 0.01 | 0.005 | 0.24 |
| LA (mm) | 0.009 | 0.01 | −0.002 | 0.46 | 0.014 | 0.01 |
| IVS (mm) | 0.008 | <0.001 | 0.002 | 0.11 | 0.001 | 0.65 |
| PW (mm) | 0.004 | <0.001 | 0.002 | <0.001 | 0 | 0.85 |
| LVEF (%) | −0.191 | 0.01 | −0.111 | <0.001 | −0.13 | <0.001 |
| E/A | −0.003 | <0.001 | −0.012 | <0.001 | −0.011 | <0.001 |
| DT (ms) | 0.501 | <0.001 | 2.217 | <0.001 | 1.661 | <0.001 |
| Septal e′/a′ | −0.004 | <0.001 | −0.006 | <0.001 | −0.006 | <0.001 |
| Lateral e′/a′ | −0.005 | <0.001 | −0.011 | <0.001 | 0.004 | 0.05 |
| Septal E/e′ | 0.248 | <0.001 | 0.183 | <0.001 | 0.084 | 0.01 |
| Lateral E/e′ | 0.147 | <0.001 | 0.167 | <0.001 | 0.032 | 0.23 |
| Score | 0.2 | <0.001 | 0.152 | <0.001 | 0.057 | 0.02 |
| Elderly vs. CAD | Elderly vs. HTN | CAD vs. HTN | ||||
|---|---|---|---|---|---|---|
| The β-Value Is Based on the Ratio of Elderly/CAD | The β-Value Is Based on the Ratio of Elderly/HTN | The β-Value Is Based on the Ratio of CAD/HTN | ||||
| Interaction term (β-Value) | p-Value | Interaction term (β-Value) | p-Value | Interaction Term (β-Value) | p-Value | |
| BMI (kg/m2) | 0.005 | 0.88 | 0.041 | 0.37 | 0.036 | 0.37 |
| SBP (mmHg) | 0.411 | <0.001 | 0.462 | 0.02 | 0.050 | 0.76 |
| DBP (mmHg) | 0.075 | 0.59 | 0.078 | 0.62 | 0.003 | 0.97 |
| HR (beats/min) | 0.036 | 0.70 | −0.242 | 0.04 | −0.278 | <0.001 |
| EDD (mm) | 0.003 | 0.58 | −0.005 | 0.41 | −0.008 | 0.13 |
| LA (mm) | 0.008 | 0.11 | −0.002 | 0.79 | −0.011 | 0.15 |
| IVS (mm) | 0.005 | 0.03 | 0.008 | <0.001 | 0.003 | 0.08 |
| PW (mm) | 0.004 | 0.01 | 0.006 | <0.001 | 0.003 | 0.03 |
| LVEF (%) | −0.002 | 0.98 | 0.174 | 0.01 | 0.176 | 0.01 |
| E/A | 0.001 | 0.74 | 0.003 | 0.49 | 0.002 | 0.62 |
| DT (ms) | −0.721 | 0.08 | −0.708 | 0.20 | 0.013 | 0.98 |
| Sep e′/a′ | −0.003 | 0.25 | −0.002 | 0.48 | 0.001 | 0.65 |
| Lat e′/a′ | −0.003 | 0.51 | −0.002 | 0.73 | 0.001 | 0.69 |
| Sep E/e′ | 0.044 | 0.23 | 0.152 | <0.001 | 0.109 | 0.01 |
| Lat E/e′ | 0.006 | 0.87 | 0.147 | <0.001 | 0.142 | <0.001 |
| Score | 0.027 | 0.42 | 0.111 | 0.01 | 0.085 | 0.01 |
| NYHA | −0.004 | 0.40 | 0.010 | 0.03 | 0.014 | <0.001 |
| Hb (g/dL) | −0.020 | 0.37 | −0.021 | 0.53 | −0.001 | 0.98 |
| Cr (mg/dL) | −0.006 | 0.16 | −0.003 | 0.55 | 0.003 | 0.35 |
| K (mmol/L) | −0.033 | <0.001 | −0.014 | 0.08 | 0.018 | 0.01 |
| eGFR (mL/min/1.73 m2) | 0.932 | 0.03 | 0.571 | 0.22 | −0.361 | 0.17 |
| β-blocker | −0.019 | 0.45 | −0.007 | 0.83 | 0.012 | 0.63 |
| CCB | −0.088 | <0.001 | −0.076 | 0.04 | 0.012 | 0.69 |
| ACEI/ARB | −0.074 | 0.02 | −0.065 | 0.12 | 0.009 | 0.76 |
| Spironolactone | 0.025 | 0.61 | 0.026 | 0.63 | 0.001 | 0.98 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, S.-N.; Lin, J.-W.; Wang, Y.-C.; Wu, C.-K.; Cheng, J.-J.; Hwang, J.-J.; Lin, J.-L.; Chiang, F.-T.; Chen, Y.-S.; Hsu, R.-B.; et al. The Sequential Change in Left Ventricular Function among Various Cardiovascular Diseases: A 12-Year Study. J. Pers. Med. 2022, 12, 415. https://doi.org/10.3390/jpm12030415
Chang S-N, Lin J-W, Wang Y-C, Wu C-K, Cheng J-J, Hwang J-J, Lin J-L, Chiang F-T, Chen Y-S, Hsu R-B, et al. The Sequential Change in Left Ventricular Function among Various Cardiovascular Diseases: A 12-Year Study. Journal of Personalized Medicine. 2022; 12(3):415. https://doi.org/10.3390/jpm12030415
Chicago/Turabian StyleChang, Sheng-Nan, Jou-Wei Lin, Yi-Chih Wang, Cho-Kai Wu, Jun-Jack Cheng, Juey-Jen Hwang, Jiunn-Lee Lin, Fu-Tien Chiang, Yih-Sharng Chen, Ron-Bin Hsu, and et al. 2022. "The Sequential Change in Left Ventricular Function among Various Cardiovascular Diseases: A 12-Year Study" Journal of Personalized Medicine 12, no. 3: 415. https://doi.org/10.3390/jpm12030415
APA StyleChang, S.-N., Lin, J.-W., Wang, Y.-C., Wu, C.-K., Cheng, J.-J., Hwang, J.-J., Lin, J.-L., Chiang, F.-T., Chen, Y.-S., Hsu, R.-B., Chen, W., Chen, J.-J., & Lien, W.-P. (2022). The Sequential Change in Left Ventricular Function among Various Cardiovascular Diseases: A 12-Year Study. Journal of Personalized Medicine, 12(3), 415. https://doi.org/10.3390/jpm12030415